
Abstract
Background
As China undergoes a demographic transition towards an aging society, the prevalence and incidence of age-related disabilities, Alzheimer's disease, and various geriatric syndromes are steadily rising.
Objective
The China Healthy Aging Cohort Study (China-Aging) aims to investigate the prevalence and associated risk factors of disability and cognitive impairment, and to develop predictive models for these conditions by combining traditional risk factors with artificial intelligence-derived metrics (such as gait, speech, vision, etc.).
Methods
The China-Aging cohort consists of community-dwelling participants aged 60 years and older from Beijing, Hangzhou, Shenzhen, and Haikou. The baseline recruitment was from May 16, 2022 to March 19, 2025, with study participants primarily from urban areas. Follow-up assessment of the cohort will occur every 1–3 years from the baseline.
Results
Among 6283 participants who completed the baseline evaluation (mean age 70.6 years, SD 6.3), 3775 (60.1%) were women. The overall prevalence of disability, cognitive impairment, frailty, depression, and sarcopenia were 17.8%, 18.5%, 5.9%, 7.1%, and 5.7%, respectively. The prevalence of disability in the Beijing cohort was higher than in other cohorts (Beijing: 35.6%, Hangzhou: 6.5%, Shenzhen: 6.8%, Haikou: 10.9%) and the prevalence of cognitive impairment in the Haikou cohort was higher than in other cohorts (Beijing: 9.5%, Hangzhou: 7.9%, Shenzhen: 16.2%, Haikou: 45.5%).
Conclusions
The prevalence of disability and cognitive impairment is relatively high, and notable regional difference exists in China. China-Aging cohort provides crucial evidence for the precise prevention and management of disability, cognitive impairment, and other geriatric syndromes in promoting active and healthy aging.
Introduction
The global population aging has emerged as one of the most pressing demographic and public health challenges. In China, the demographic of aging is accelerating at a particularly rapid rate. According to the National Bureau of Statistics, the population of individuals aged 60 and above (60+) reached 310 million by 2024, accounting for 22.0% of the total population. 1 It is predicted that the number of individuals 60 + will reach 520 million by 2050, 2 which will bring a tremendous need for medical care and daily support. Therefore, improving the understanding of the factors affecting healthy aging has profound public health importance. 3
Disability and cognitive impairment are the major causes of dependence and loss of autonomy among older adults. 3 In China, the prevalence of disability among the population aged 60 and over was 20.5%, with an expectation of underreporting in rural regions. 4 For cognitive impairment, nationwide prevalence was reported to be 15.5%, affecting 38.77 million individuals. 5 In addition, the prevalence of geriatric syndromes—including frailty (4%-59.1%), depression (7.8%-46%), and sarcopenia (3.3%-17.5%)—is rising,6–8 all of which are associated with adverse health outcomes. 9 Therefore, identifying risk factors and biomarkers for the aforementioned health conditions in older adults are crucial for identifying high-risk populations and enabling targeted preventive interventions.
At present, the identification and screening of disabilities, cognitive impairment, and geriatric syndromes rely predominantly on evaluation scales. 10 Emerging technologies, including intelligent speech analysis, micro-expression recognition, and posture detection, offer promising alternatives for early detection and identification of disabilities, cognitive impairment, and certain geriatric syndromes. For instance, artificial intelligence (AI) systems capable of processing speech and analyzing micro-expressions have shown potential in effectively identifying the risk of emotional abnormalities and cognitive impairments. 11 Moreover, advanced posture recognition technology can aid in the early detection of apraxia and gait abnormalities, which are commonly seen in older adults with disabilities. 12 However, despite the potential of these intelligent technologies, their application remains fragmented, with limited standardization and generalizability. Prioritizing the development of comprehensive, multidimensional risk assessment technologies that are adaptable for use in both family and community settings is major concern.
Several longitudinal cohort studies covering different populations and regions have been conducted in China,13,14 but there remains a dearth of representative cohorts that incorporate intelligent technologies to assess the health issues from multiple dimensions including physical function and mental health. The China Healthy Aging Cohort Study (China-Aging) aims to address this gap. As a longitudinal survey of the Chinese older adults, it seeks to generate robust data on a large sample of older adults from four typical cities across north, central, and south regions of China. Specifically, the China-Aging cohort aims to investigate the prevalence and risk factors of disability and cognitive impairment. Furthermore, by leveraging AI technologies to assess functional performance in domains such as gait, cognitive, speech, vision, hearing, and comorbidities—combined with traditional risk factors—we aim to develop predictive models for disability and cognitive impairment. The findings from the China-Aging cohort will help identify risk factors for disability and cognitive impairment, facilitate the formulation of targeted prevention and intervention strategies, and ultimately may contribute to healthy aging in China.
Methods
Data source
The China-Aging cohort consisted of participants from four sub-cohorts: Beijing Disability Risk and Aging Monitoring Study (BEAM, Beijing cohort), the Hangzhou Brain Health and Psychological Survey (Hangzhou cohort), the Shenzhen Aging Cohort Study (SZ-aging, Shenzhen cohort), and the Hainan Community Cognition Cohort (Haikou cohort), four regions (Beijing, Hangzhou, Shenzhen, Haikou) located in the northern, middle and southern parts of China (Figure 1). The China-Aging study has been ethically approved by the Ethics Committee of Xuanwu Hospital (2024214001) and registered in ClinicalTrials.gov (NCT06472674).

Selected cities in China for sampling in China-Aging.
The Beijing cohort was established by Xuanwu Hospital of Capital Medical University, encompassing older adults from Baizhifang Community of Beijing city; and baseline data was collected from May 8, 2023 to January 29, 2024. The Hangzhou cohort was established by the First Affiliated Hospital of Zhejiang University School of Medicine, involving older adults from Liucuijingxiang Community, Jinzhiyuan Community, Xiaoyingxiang Community, Zhanongkou Community, Qinghefang Community, and Laodonglu Community of Hangzhou city; and the baseline data collection was from November 2, 2022 to January 25, 2024. The Shenzhen cohort was established by Shenzhen Center for Chronic Disease Control comprising older individuals residing in Dongjiaotou Community, Haile Community, Haiyue Community, Huaguoshandong Community, Luhu Community, and Shangtangdao Community of Shenzhen city; and the baseline data was collected from May 16, 2022 to October 10, 2023. The Shenzhen cohort protocol has been published previously. 15 The Haikou cohort was initiated by Hainan Medical University targeting community-dwelling older adults from Gongyuanhou Community, Haidian Community, Renmin Community, Baipoli Community, Yanfeng Community, Jiahua Community, Haiken Community, Binlian Community, Jindi Community, Binjiang Community, Fucheng Community, Balun Community, and Haigang Community of Haikou; and the baseline data collection was from December 1, 2022 to March 19, 2025.
Beijing and Hangzhou cohorts included registered residents aged 60 years or older who had resided in the communities for more than one year, and excluded the older adults who could not complete the survey because of severe psychological and physiological disorders. Shenzhen cohort included registered residents aged 65 years or older who had resided in the communities for more than six months, and excluded the older adults who lived in long-term care institutions and had severe mental diseases. Haikou cohort included registered residents aged 60 years or older who had resided in the communities for more than six months, and excluded the older adults who lived in long-term care institutions and had severe psychological and physiological diseases. China-Aging was assembled from the above four cohorts, including registered residents aged ≥ 60 years in the community with more than six months of residence and excluding severe psychological or physiological disorders. At present, the merged China-Aging cohort includes 6283 individuals (Supplemental Figure 1).
Quality control and follow-up
Team members and interviewers of four sub-cohorts were all underwent comprehensive training encompassing research objectives, face-to-face interview technic, specific indicator's assessment (for example, MMSE measurement), standardized physical measurement procedures, utilization of intelligent software, biological sample collection and processing, etc
Follow-ups will be conducted every 1 to 3 years according to actual situations of fundings and human resources by each sub-cohort. For participants who cannot complete face-to-face interviews during the follow-up period, indicators regarding disabilities, cognitive impairments, and other geriatric syndromes will be collected via telephone interviews.
Measurement indicators
Questionnaire. The baseline questionnaire encompasses a broad spectrum of data, including participants’ demographic information, lifestyle habits, self-reported physician's diagnosed chronic medical history, physical health status, and sensory abilities, et al. Cognitive function was evaluated using Mini-Mental State Examination (MMSE). 16 Activities of daily living (ADL) were assessed using ADL scale (Barthel index) 17 except in Shenzhen cohort, where basic activities of daily living (BADL) and instrumental activities of daily living (IADL) were assessed using BADL scale (Katz scale) 18 and IADL scale (Lawton scale). 19 The Geriatric Depression Scale-15 (GDS-15) 20 was used to assess the presence of depression in the Beijing and Hangzhou cohorts, and Patient Health Questionnaire-2 (PHQ-2) 21 used in Shenzhen and Haikou cohorts. Frailty was evaluated using Frailty Phenotype (FP) 22 in Beijing and Haikou cohorts, and Frailty Scale (FS) for frailty in Shenzhen cohorts. 23 The strength, assistance in walking, rise from a chair, climb stairs, and falls (SARC-F) was used to assess sarcopenia in Beijing, Hangzhou and Haikou cohorts. 24 The Clinical Physical Resilience Assessment Scale (CHEES), which has been validated in the Chinese population, 25 was used to assess the elasticity of older individuals in Beijing, Hangzhou and Haikou cohorts. Short Physical Performance Battery (SPPB) was used for physical ability in Beijing, Shenzhen, and Haikou cohorts (Table 1). 26
Contents of the baseline data collected from China-Aging.
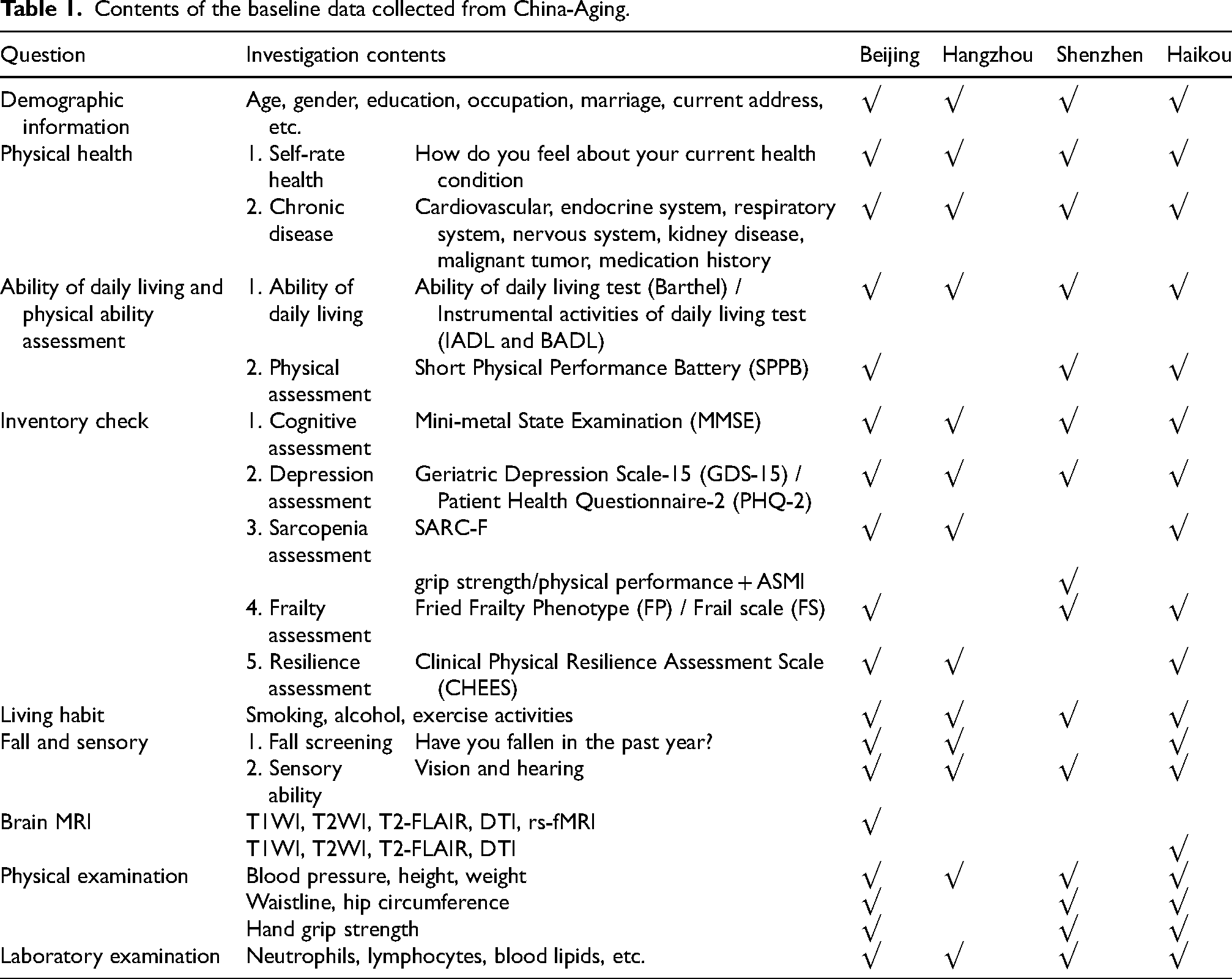
Physical measurements. Physical measurements included body height (in meter, m), weight (in kilogram, kg), waist circumference (in centimeter, cm), hip circumference (cm), hand grip strength (kg), and blood pressure (mmHg).
When measuring height, participants were required to remove their shoes, maintain an upright posture with their feet positioned together, and align their heads horizontally with the right-angle board. For weight measurement, the subject wore lightweight clothes without shoes. For waist and hip circumference measurements, a standardized tape measure was placed horizontally around the participant's abdomen and hip. The handheld dynamometers (WCS-10000/ EH101) were used to measure hand grip strength (HGS) in a standing position with an extended arm straight down to the side. Each participant was asked to exert their maximum effort twice, and their grip strength for both hands was recorded in kilograms every time. Before the blood pressure measure using Omron ™ HEM-4021/ HEM7121, the participants were advised to avoid smoking, alcohol consumption, caffeinated beverage intake, and physical activity for a period of thirty minutes and remain at rest for five minutes. Blood pressure in the subject's right upper arm was measured twice in a sitting position, maintaining an interval of one to two minutes between each measurement, and a mean value was taken for analysis (Table 1).
Laboratory examination. Blood samples were collected from the elbow vein by trained nurses via standard blood collection methods after participants had fasted for at least 8 h. All the samples were subjected to testing in local laboratories, all of which successfully fulfilled standardization and capability plans. To ensure the accuracy and stability of the measurements, internal and external quality control programs are routinely used. Clinical laboratory tests provide valuable information regarding routine blood test, hepatic function, kidney function, lipid profiles, et al. (Table 1).
Imaging examination. A subset of Beijing and Haikou cohort were invited for brain structural and functional measurements using brain magnetic resonance imaging (MRI). The participants were imaged using 3.0 T MRI scanner. T1-weighted imaging (T1WI), T2-weighted imaging (T2WI), T2-fluid attenuated inversion recovery (T2-FLAIR), diffusion tractography imaging (DTI), and resting-state functional magnetic resonance imaging (rs-fMRI) were conducted in Beijing cohort. T1W1, T2WI, T2-FLAIR, and DTI were conducted in Haikou cohort.
Measurements of cognition, disability, and other geriatric syndromes. The MMSE was applied to measure the cognitive function, with a total score of 30. 16 For various educational levels, namely, illiteracy, primary school, middle school and higher, the cognitive impairment was classified as MMSE score of ≤ 19, ≤ 22, and ≤ 26, respectively. 27
Disability was measured using the Barthel index (eating, bathing, grooming, dressing, bowel control, bladder control, toileting, transferring from bed to chair, ambulation, and stair climbing) in Beijing, Hangzhou, and Haikou cohorts; and Katz scale (eating, dressing, bowel control and bladder control, toileting, bathing, transferring from bed to chair) in Shenzhen cohort. Participants were considered disabled if they were unable to perform any item without difficulty, regardless of the instrument measuring disability.28,29
Frailty was assessed with the FP (slowness, weakness, weight loss, inactivity, and exhaustion) among Beijing and Haikou cohorts, and FS (fatigue, resistance, ambulation, illnesses, and loss of weight) among Shenzhen cohort. FP and FS have been validated for frailty assessment among older community dwellers.30,31 Participants exhibiting three or more phenotypes were defined as frailty. 22
Depression was evaluated using GDS-15 among the Beijing and Hangzhou cohorts, and PHQ-2 among the Shenzhen and Haikou cohorts. The GDS-15 contain 15 items, with the scores of ≥ 5 indicating depression. 32 The PHQ-2 contain two questions assessing the frequency of depressive symptoms, with each answer values from 0 (never or not at all) to 3 (almost every day) on the scales and according to most published studies, the scores of ≥ 3 indicates depression. 33
Sarcopenia was evaluated using SARC-F in the Beijing, Hangzhou, and Haikou cohorts. The SARC-F was a simple and quick way to assess the risk of sarcopenia. It consists of five components: walking aids, falls prevention, getting up from a chair, climbing stairs, and strength training. Each item values from zero to two. An individual with a score of four points or higher is considered as having the risk of sarcopenia. 24 In Shenzhen cohort, individuals with low hand grip strength (< 28 kg for male; < 18 kg for female) or physical performance (SPPB ≤ 9) combined with low appendicular skeletal muscle mass index (ASMI) (< 7.0 kg/m2 for male; < 5.7 kg/m2 for female) were defined as sarcopenia according to the Asian Working Group for Sarcopenia (AWGS) guidelines. 34
Artificial intelligence applications
An Android application was custom-developed for functional performance screening. This application comprises six modules: gait detection, cognitive impairment recognition, speech disturbance detection, vision test, hearing test, and comorbidity test (Figure 2). Each module incorporates specific algorithms, including established deep learning models, such as YOLOv5, AlphaPose, and OpenFace (Figure 2).
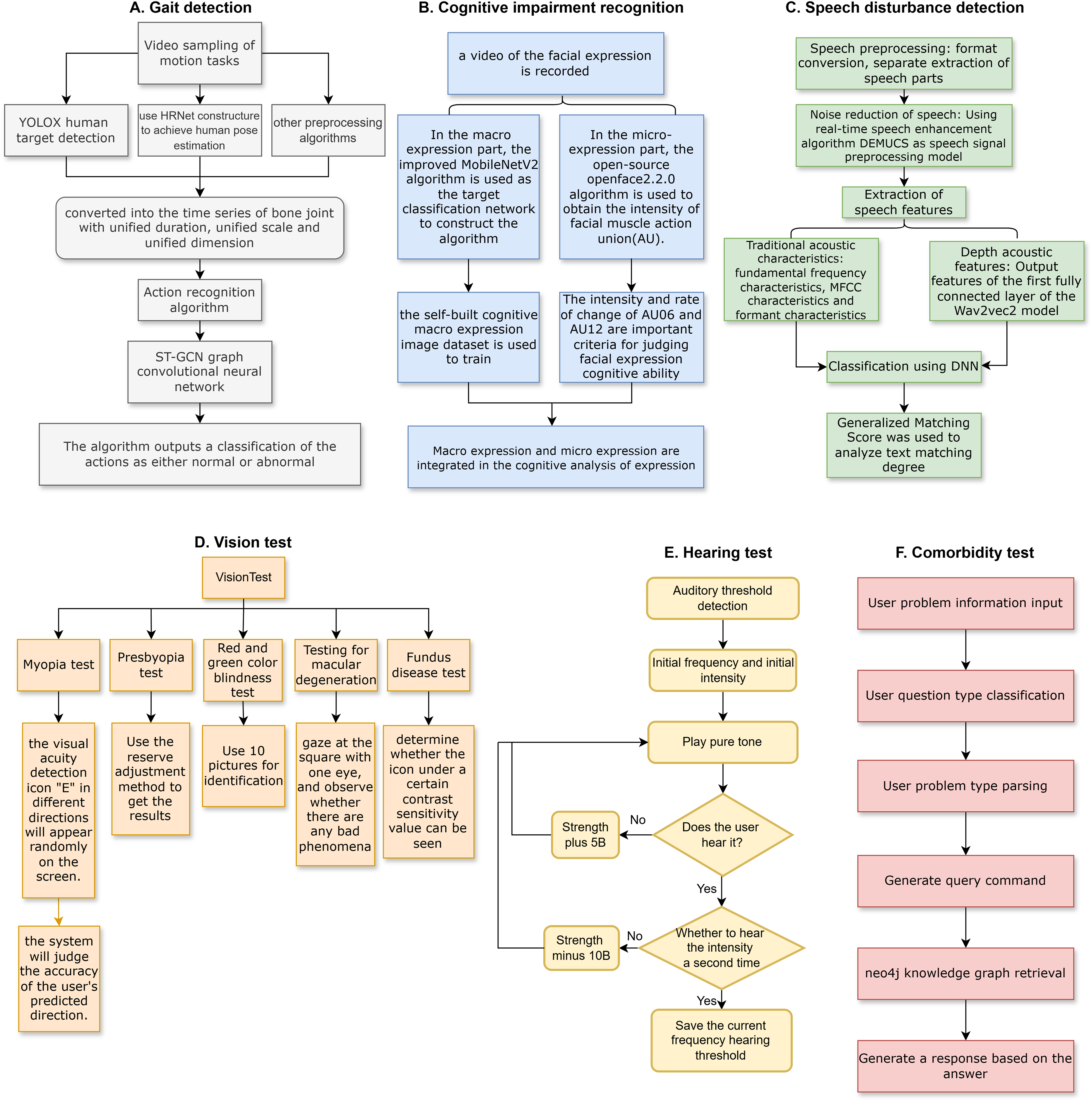
Summary of data collected in the artificial intelligence application.
Gait detection: Within the gait recording module, the application prompts participants to perform three prescribed movements: walking, sit-to-stand transitions, and turning in place. Stationary cameras then capture video of their movements. Subsequently, video frames are extracted, and YOLOv5 is employed for object detection, followed by HRNet for pose estimation. The resulting skeletal joint time series are transformed to ensure uniform duration, scale, and dimensionality. Finally, the core action recognition algorithm, the open-source SkeletonGCL based on ST-GCN, is applied to analyze this sequence. This algorithm utilizes graph convolution methods to extract key spatiotemporal features, which are then input into a classifier to determine normal or abnormal action classification results (Figure 2A).
Cognitive impairment recognition: For the cognitive impairment recognition part, the app first shows the older adults a funny video and records a video of the facial expression. The recorded video is a sequence of pictures that frame humorous punchlines. Then a set of algorithms based on macro and micro-expression analysis are used to parse the image sequences. In the macro expression part, the improved MobileNetV2 algorithm is used as the target classification network to construct the algorithm, and the self-built cognitive macro expression image dataset is used to train and test the model. In the micro-expression part, the open-source openface2.2.0 algorithm is used to obtain the intensity of facial muscle movement units. In this process, AU06 and AU12 are the most important parameters. When their own intensity and change rate reach a certain threshold, the facial expression is considered normal (Figure 2B).
Speech disturbance detection: For the speech assessment module, the app provides several speech tasks, such as narrative retelling, and records participants’ audio data. In the process of data acquisition and preprocessing, real-time speech enhancement algorithm DEMUCS is used as the speech signal preprocessing model. Instead of training the de-noising model, the trained model provided by the government is directly used for noise removal. The speech after de-noising by using this algorithm basically only includes the speaker's speech and is very clear. Using advanced automatic speech recognition technology and quantitative analysis methods, the subject's speech data is transformed into analyzable feature quantities. These features are divided into traditional typical acoustic features and deep acoustic features. The typical acoustic features include fundamental frequency features, MFCC features and formant characteristics, etc. The deep acoustic features are semantic features extracted from speech signals through Wav2vec2 model, and the features are averaged and pooled in time series. These two features are combined for classification. Finally, a one-dimensional Deep Neural Network (1D DNN) is trained and employed for inference using all extracted audio features, yielding an AI model for screening purposes. The ultimate output is an assessment of the participant's language function as normal or abnormal (Figure 2C).
Vision test: The vision test module is divided into five sub-modules: myopia testing, presbyopia testing, red-green color blindness testing, macular disease screening, and fundus disease screening. Myopia is assessed by having participants identify the orientation of a software-generated ‘E’ chart to measure visual acuity. Presbyopia is evaluated through binocular comparison tests conducted at varying distances to assess presbyopia. Red-green color blindness is assessed using ten red-green color vision test plates. Macular disease is evaluated by having users observe a specialized grid for macular degeneration monocularly and monitoring their responses to identify potential macular issues. Fundus disease is assessed based on the participant's ability to perceive icons of varying fundus sensitivity, indicating potential fundus pathologies. All these assessments are conducted interactively within the application (Figure 2D).
Hearing test: In the hearing assessment module, the application determines participants’ hearing thresholds by presenting pure-tone audio at varying intensities and frequencies and querying their audibility. Specifically, an initial sound intensity and frequency are set. Based on the participant's response (audible or inaudible), the sound intensity is adjusted using a 10 dB down, 5 dB up step size. This process establishes the participant's hearing threshold at that frequency. Subsequently, the audio frequency is adjusted, and the procedure is repeated. Finally, an audiogram, representing hearing thresholds across frequencies, is generated, providing the participant's hearing levels in decibels (Figure 2E).
Comorbidity test: In the comorbidity assessment module, the application engages in a brief spoken interaction with participants. Participants are prompted to answer a series of health-related questions, and the application automatically records the question-and-answer dialogue via voice input. Subsequently, the input question results are subjected to classification analysis, generating query instructions. Finally, a Neo4j knowledge graph is utilized to query disease outcomes, yielding potential comorbidity risks for the participant (Figure 2F).
Statistical analyses
Continuous variables are expressed as mean (SD) and categorical variables as frequencies (%). One-way analyses of variance were performed for comparisons of continuous variables. The Chi-squared test was used for comparisons of categorical variables. Logistic regression models were employed to analyze risk factors for disability and cognitive impairment. All statistical analyses were conducted using R software version 4.2.1. A two-tailed value of p < 0.05 was deemed statistically significant.
Results
Table 2 showed the baseline characteristics of 6283 participants enrolled in China-Aging cohort. The mean age of the total participants was 70.6 ± 6.3 years (69.9 ± 6.1 years in Beijing; 72.1 ± 7.6 years in Hangzhou; 70.5 ± 4.6 years in Shenzhen; and 70.7 ± 7.2 years in Haikou; p < 0.001), 60.1% females (63.1% in Beijing; 60.6% in Hangzhou; 56.0% in Shenzhen; 60.2% in Haikou; p < 0.001). There was variation on age and sex among the four sub-cohorts.
Baseline characteristics of the participants in China-Aging.
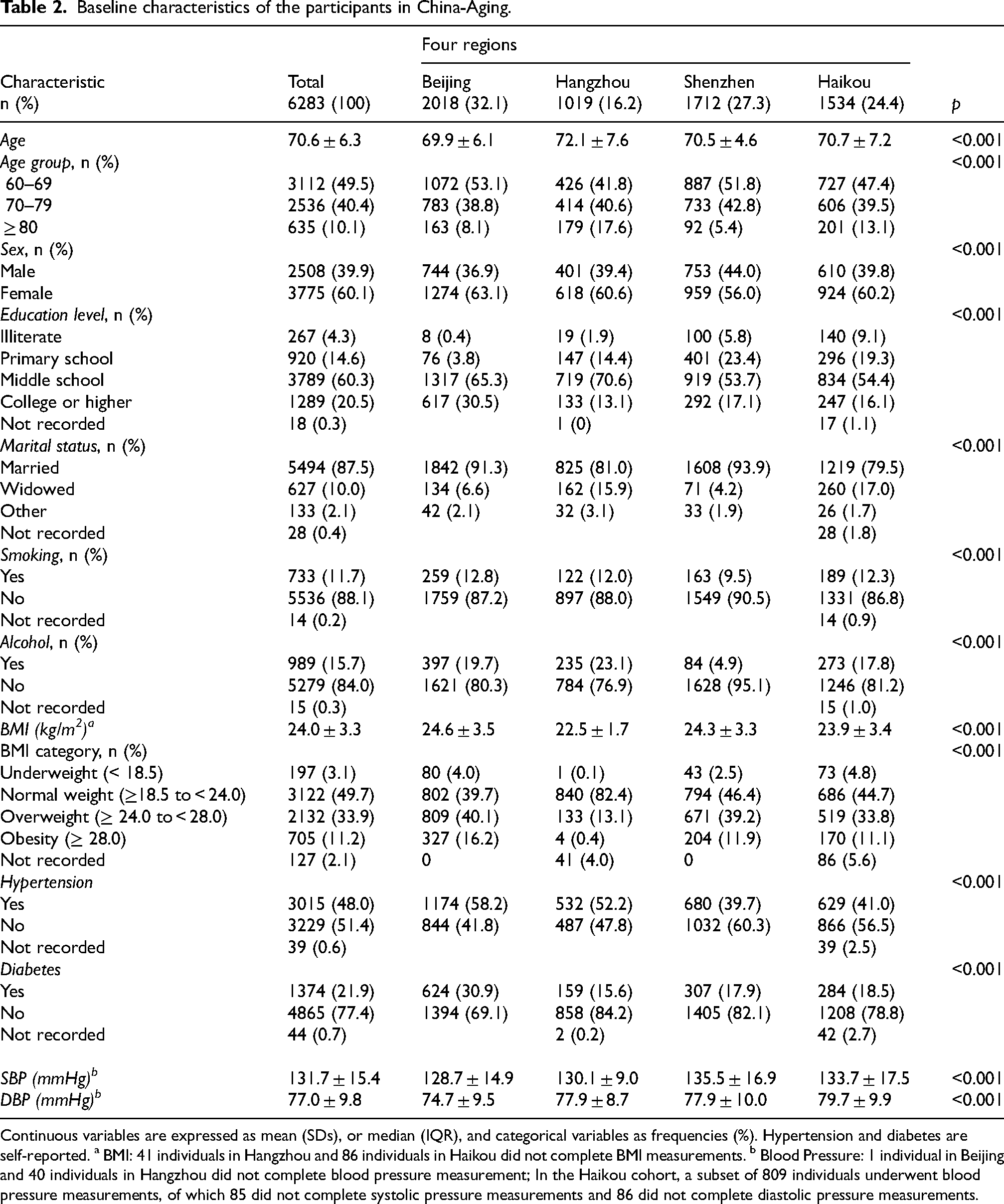
Continuous variables are expressed as mean (SDs), or median (IQR), and categorical variables as frequencies (%). Hypertension and diabetes are self-reported. a BMI: 41 individuals in Hangzhou and 86 individuals in Haikou did not complete BMI measurements. b Blood Pressure: 1 individual in Beijing and 40 individuals in Hangzhou did not complete blood pressure measurement; In the Haikou cohort, a subset of 809 individuals underwent blood pressure measurements, of which 85 did not complete systolic pressure measurements and 86 did not complete diastolic pressure measurements.
Compared with the participants in the other three regions, the Haikou cohort had a higher proportion of participants with a lower level of education (primary school education or less) (28.4%), and a higher proportion of widowed subjects (17.0%). The body mass index (BMI) of Beijing cohort participants was higher than that from the other three regions (24.6 ± 3.5 kg/m2 in Beijing; 22.5 ± 1.7 kg/m2 in Hangzhou; 24.3 ± 3.3 kg/m2 in Shenzhen; and 23.9 ± 3.4 kg/m2 in Haikou; p < 0.001). In addition, the systolic blood pressure (SBP) of Shenzhen cohort participants was higher than that from the other three regions (128.7 ± 14.9 mmHg in Beijing; 130.1 ± 9.0 mmHg in Hangzhou; 135.5 ± 16.9 mmHg in Shenzhen; and 133.7 ± 17.5 mmHg in Haikou; p < 0.001), but the diastolic blood (DBP) of Haikou cohort participants was higher than that from the other three regions (74.7 ± 9.5 mmHg in Beijing; 77.9 ± 8.7 mmHg in Hangzhou; 77.9 ± 10.0 mmHg in Shenzhen; and 79.7 ± 9.9 mmHg in Haikou; p < 0.001). In terms of lifestyle, 88.1% of the participants were non-smokers (87.2% in Beijing, 88.0% in Hangzhou, 90.5% in Shenzhen; and 86.8% in Haikou, p < 0.001), and 84.0% did not consume alcohol (80.3% in Beijing, 76.9% in Hangzhou, 95.1% in Shenzhen; and 81.2% in Haikou, p < 0.001). In terms of self-reported chronic diseases, 48.0% of the participants had hypertension (58.2% in Beijing, 52.2% in Hangzhou, 39.7% in Shenzhen; and 41.0% in Haikou, p < 0.001), and 21.9% had diabetes (30.9% in Beijing, 15.6% in Hangzhou, 17.9% in Shenzhen; and 18.5% in Haikou, p < 0.001).
Table 3 showed the prevalence of geriatric syndromes. The prevalence of disability, cognitive impairment, frailty, depression, and sarcopenia was 17.8%, 18.5%, 5.9%, 7.1%, and 5.7% respectively. In the Beijing cohort, the prevalence of disability, cognitive impairment, frailty, depression, and sarcopenia was 35.6%, 9.5%, 8.4%, 10.8%, and 1.8%, respectively. In the Hangzhou cohort, assessments were conducted for disability, cognition, depression, and sarcopenia; however, frailty was not evaluated. The prevalence of disability, cognitive impairment, depression, and sarcopenia in the Hangzhou cohort was 6.5%, 7.9%, 7.8%, and 2.6%, respectively. In the Shenzhen cohort, the prevalence of disability, cognitive impairment, frailty, depression, and sarcopenia was 6.8%, 16.2%, 2.4%, 0.6%, and 14.1%, respectively. In the Haikou cohort, the prevalence of disability, cognitive impairment, frailty, depression, and sarcopenia was 10.9%, 45.5%, 7.8%, 8.9%, and 4.5%. Compared with other regions, the prevalence of disability (p < 0.001), frailty (p < 0.001), and depression (p < 0.001) was higher in Beijing, the prevalence of cognitive impairment (p < 0.001) was higher in Haikou, and the prevalence of sarcopenia (p < 0.001) was higher in Shenzhen.
Prevalence of geriatric syndrome in China-Aging.
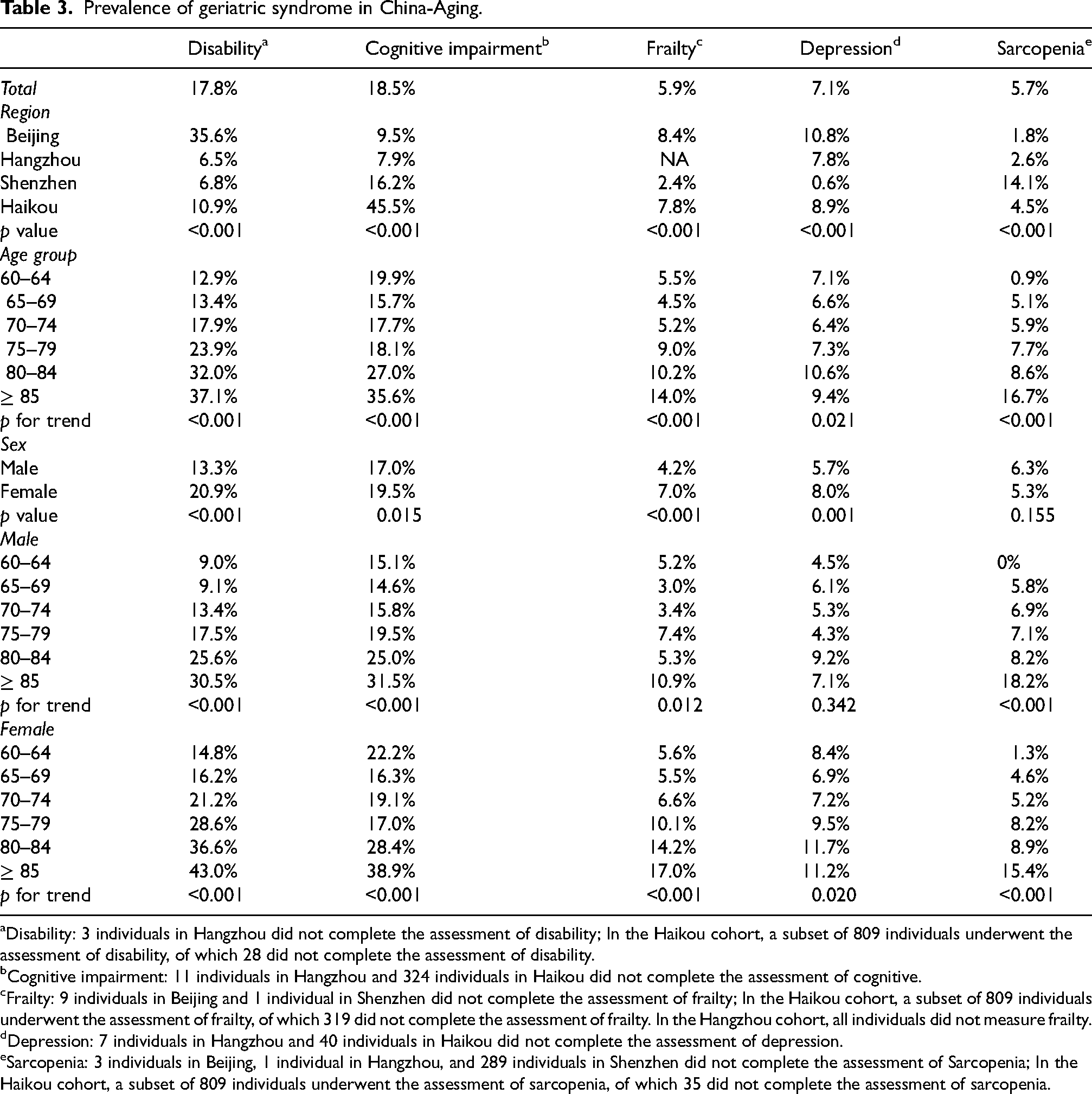
Disability: 3 individuals in Hangzhou did not complete the assessment of disability; In the Haikou cohort, a subset of 809 individuals underwent the assessment of disability, of which 28 did not complete the assessment of disability.
Cognitive impairment: 11 individuals in Hangzhou and 324 individuals in Haikou did not complete the assessment of cognitive.
Frailty: 9 individuals in Beijing and 1 individual in Shenzhen did not complete the assessment of frailty; In the Haikou cohort, a subset of 809 individuals underwent the assessment of frailty, of which 319 did not complete the assessment of frailty. In the Hangzhou cohort, all individuals did not measure frailty.
Depression: 7 individuals in Hangzhou and 40 individuals in Haikou did not complete the assessment of depression.
Sarcopenia: 3 individuals in Beijing, 1 individual in Hangzhou, and 289 individuals in Shenzhen did not complete the assessment of Sarcopenia; In the Haikou cohort, a subset of 809 individuals underwent the assessment of sarcopenia, of which 35 did not complete the assessment of sarcopenia.
We further explored the prevalence of geriatric syndromes by age and sex (Table 3). The prevalence of disability, cognitive impairment, frailty, depression, and sarcopenia increases with age. Specifically, the prevalence of disability increased from 12.9% in people aged 60–64 years to 37.1% in people aged ≥85 years (p for trend <0.001). The corresponding rates increased from 19.9% to 35.6% for cognitive impairment (p for trend <0.001), 5.5% to 14.0% for frailty (p for trend <0.001), 7.1% to 9.4% for depression (p for trend =0.021), and 0.9% to 16.7% for sarcopenia (p for trend <0.001). The prevalence of disability (13.3% versus 20.9%, p < 0.001), cognitive impairment (17.0% versus 19.5%, p = 0.015), frailty (4.2% versus 7.0%, p < 0.001) and depression (5.7% versus 8.0%, p = 0.001) was lower in males than in females. There was no significant difference in the prevalence of sarcopenia between males and females (6.3% versus 5.3%, p = 0.155). In the sex-stratified analysis, similar patterns were observed across different age groups, except that no significant increase in the prevalence of depression with age was observed in males (p = 0.342).
We focused on the characteristics of disability and cognitive impairment. Participants with disability were more likely to be over 70 years old (62.7%), female (70.2%), and with the history of hypertension (56.6%) and diabetes (31.3%) (Supplemental Table 1). Participants with cognitive impairment were more likely to be over 80 years old (15.8%), female (63.4%), widowed (15.7%), and with a lower education level (primary school education or less) (20.9%) (Supplemental Table 2).
Compared to individuals aged 60–69 years, those in the 70–79 years and ≥80 years groups had higher risks of disability (adjusted OR 1.73, 95% CI 1.48–2.03; adjusted OR 4.20, 95% CI 3.33–5.29, respectively) in the multivariate analysis. Females demonstrated a 97% increased risk compared to males (adjusted OR 1.97, 95% CI 1.68–2.31). Compared with individuals with normal weight, individuals with underweight (adjusted OR 2.81, 95% CI 1.92–4.11), overweight (adjusted OR 1.50, 95% CI 1.28–1.77), and obese (adjusted OR 2.36, 95% CI 1.91–2.92) had higher risks of disability. Additionally, hypertension (adjusted OR 1.19, 95% CI 1.02–1.38) and diabetes (adjusted OR 1.64, 95% CI 1.39–1.92) were significantly associated with disability risk (Supplemental Table 3). Compared to individuals aged 60–69 years, those in the ≥80 years group had a higher risk of cognitive impairment (adjusted OR 2.03, 95% CI 1.64–2.52). Compared with individuals who were illiterate, individuals with college or higher education (adjusted OR 0.47, 95% CI 0.32–0.67) had lower risks of cognitive impairment. Individuals who were widowed showed a higher risk of cognitive impairment compared to those who were married (adjusted OR 1.65, 95% CI 1.34–2.03). Additionally, compared with individuals with normal weight, those who were underweight (adjusted OR 1.74, 95% CI 1.24–2.45) had a higher risk of cognitive impairment (Supplemental Table 4).
Discussion
China-Aging cohort collected multidimensional information of community-dwelling older adults, comprising traditional questionnaire, physical, functional and scale measurements, and dynamic data based on advanced AI approach, which provides an important perspective for a comprehensive analysis of health status of the older individuals.
Baseline data from the China-Aging cohort revealed significant variations in certain geriatric syndromes across different regions. In these geriatric syndromes, we focused on disability and cognitive impairment. We found that the prevalence of disability in the Beijing cohort and the prevalence of cognitive impairment in the Haikou cohort was higher than in other regions, potentially due to the following reasons. Sex, BMI, hypertension, and diabetes were identified as risk factors for disability in China-Aging. The higher proportion of females, the higher proportion of individuals with overweight and obesity, and the higher proportion of hypertension and diabetes in the Beijing cohort may explain the higher prevalence of disability in this region. Additionally, we found that educational attainment, marital status, and BMI are risk factors for cognitive impairment. The Haikou cohort had a lower proportion of individuals with high educational attainment, and a higher proportion of individuals who were widowed and underweight. These characteristics may collectively contribute to the higher prevalence of cognitive impairment in the Haikou cohort. China-Aging study involves a range of geriatric syndromes and provides insight into aging-related issues in similar regions with comparable economic levels and population structures.
In the China-Aging study, the prevalence of disability and cognitive impairment tends to increase with age, with similar patterns observed across different genders. One possible explanation is that physiological functions continue to decline with advancing age in older individuals. Older adults are more susceptible to chronic conditions such as hypertension and diabetes, which can contribute to the development of geriatric syndromes. Additionally, we found that the prevalence of disability and cognitive impairment among older women is higher than that among men in China, which is consistent with previous research findings.4,35 The following reasons may explain the higher prevalence in females compared to males. In China, men tend to have higher educational attainment and economic status, and they are generally more proactive in managing their own healthcare.36–38 These factors may make men less susceptible to disability and cognitive impairment than women. Furthermore, the higher prevalence of cognitive impairment among older women might also be attributed to a reduction in estrogen and related hormones after menopause. 5
China-Aging cohort is a longitudinal community cohort that covers a large proportion of the older population in four cities across China from north to south. It is aimed to provide reliable real-world evidence for health aging and healthcare interventions by exploring scientific issues related to aging in China. Previous large aging cohorts in China, such as the China Health and Retirement Longitudinal Study (CHARLS) and the Chinese Longitudinal Healthy Longevity Survey (CLHLS),13,14 focused primarily on investigating factors that increase the longevity and quality of life of older individuals, with more emphasize on social science research. Compared with CHARLS and CLHLS, our cohort focuses more on biochemical indicators, imaging information, and AI-based early detection, which greatly supplements the previous general population-based data.
Furthermore, China-Aging was the first large-scale community cohort study in China to employ artificial intelligence for the identification of geriatric syndromes. Most research on aging cohorts predominantly emphasized biological variables and scale measurements for disability and various geriatric syndromes. However, the high variability of biological indicators and the subjectivity of these scales make the classification of disability in older adults prone to inaccuracies. Consequently, given the multifactorial nature of disability, the use of artificial intelligence and data science has been considered for identifying and predicting these complex geriatric syndromes in China-Aging. With the help of artificial intelligence, it is possible to establish relationships among different variables, such as kinematic, expressive, linguistic, visual, and auditory, leading to a more elaborate detection and classification of disabilities and geriatric syndromes. This cohort will provide evidence on how the data collected using scientific and intelligent approaches, combined with traditional data, facilitate the precise prevention and control of disability and cognitive impairment risk among older individuals, and ultimately reducing the incidence of disability and cognitive impairment.
This prospective cohort study has several advantages. First, it combines four regional sub-cohorts with different economic levels and geographic locations in China. This study provides an opportunity to describe the epidemiological characteristics of the most common health problems among older individuals. Second, it established a foundation for facilitating the holistic health development of the older adults through the collection of multidimensional data. Third, we have implemented artificial intelligence to identify and predict disabilities and cognitive impairment in older individuals, facilitating early detection and precise intervention. However, several limitations must be considered. First, community data were mainly derived from four cities with limited geographical representation, which may restrict the generalizability of the findings to rural areas in China. However, considering the diverse socio-economic structures in Beijing, Shenzhen, Hangzhou, and Haikou, our study can partly reflect the health status of older adults in China. Second, some participants may have higher mobility, leading to loss to follow-up; this could potentially introduce bias in our cohort. In modern society, with advanced transportation infrastructure, participants from more developed regions, such as Beijing, often engage in frequent inter-regional travel. This is relevant in our China-Aging cohort, where the study participants are predominantly retired older individuals with ample free time. During follow-up periods, participants traveling for tourism in other regions may become unavailable for assessments, potentially reducing follow-up rates. Furthermore, participants who are generally healthier and have higher socioeconomic status tend to be more mobile, potentially leading to systematic bias between those retained and those lost to follow-up. To mitigate these risks, we have implemented several preventive strategies: 1) we will proactively inform participants of the follow-up schedule well in advance and communicate with them to reserve a suitable time; 2) we will establish an incentive program, offering benefits to participants who complete the follow-up survey to enhance their participation and minimize loss to follow-up.
Baseline data from the China-Aging cohort reveal notable disparities in the prevalence of geriatric syndromes across regions with varying economic levels, underscoring the necessity of incorporating regional heterogeneity into the design of future aging-related policies in China. Furthermore, ongoing follow-up of the China-Aging cohort, along with subsequent research leveraging this cohort data, will advance the identification of risk factors for geriatric syndromes such as disability and cognitive impairment among community-dwelling older adults in China. These evidence-based insights may help to inform the development of targeted preventive strategies.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251360028 - Supplemental material for Cohort profile: China healthy aging cohort study (China-Aging)
Supplemental material, sj-docx-1-alz-10.1177_13872877251360028 for Cohort profile: China healthy aging cohort study (China-Aging) by Jie Chang, YueWu, Yiwei Zhao, Xue Gao, Yiwen Xing, Zhibin Wang, Qi Qin, Wenqing Ni, Yangwei Ying, Xiaoyan Liu, Lumin Leng, Hong Zhou, Lina Ma, Yansu Guo, Guoping Peng, Yong You, Jindong Ding Petersen, Jian Xu and Yi Tang in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
All authors thank the Beijing Disability Risk and Aging Monitoring Study (BEAM) team, the Shenzhen Aging Cohort (SZ-Aging) team; the Hainan Community Cognition Cohort (Haikou cohort) team, and the Hangzhou Brain Health and Psychological Survey (Hangzhou cohort) team for providing and sharing the data for China Healthy Aging Cohort Study (China-Aging). We thank all participants and volunteers involved in this study.
Ethical considerations
China-Aging was performed in line with the principles of the Declaration of Helsinki, approved by the Ethics Committee of Xuanwu Hospital (2024214001).
Consent to participate
Informed consent was obtained from all participants.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China (2022YFC3602600), National Natural Science Foundation of China (82220108009), Beijing Outstanding Young Scientist Program (JWZQ20240101023), STI2030-Major Projects (2021ZD0201801), National Natural Science Foundation of China (82273631), National Natural Science Foundation of China (8206050221), National Natural Science Foundation of China (82360673), Hainan Provincial Department of Science and Technology Fund (ZDYF2024SHFZ064), Hainan Medical University “Leading Talent” Scientific Research Fund (XRC2022005), and Shenzhen Medical Key Discipline Construction Fund (SZXK065).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.