
Abstract
Background
Early neurovascular coupling (NVC) dysfunction in Alzheimer's disease (AD) remains poorly understood despite being a key pathological feature.
Objective
This study aimed to investigate NVC alterations across the AD continuum, including individuals with AD, mild cognitive impairment (MCI), and cognitively normal (CN) individuals, and to examine their associations with cognitive performance and plasma biomarkers.
Methods
This study included 23 CN participants, 80 MCI, and 33 AD patients. Neuronal activity was assessed using amplitude of low-frequency fluctuation (ALFF) and regional homogeneity (ReHo), which were derived from blood oxygen level-dependent functional magnetic resonance imaging signals, whereas cerebral blood flow (CBF) maps measured perfusion. Neurovascular coupling was quantified via the ALFF-CBF and ReHo-CBF. Group differences were evaluated using analysis of variance, and associations with cognitive scores and plasma biomarkers were analyzed.
Results
The AD group exhibited lower ALFF-CBF coupling values in the left anterior cingulate and middle cingulate gyri compared with the CN and MCI groups. Reduced coupling values were positively correlated with Mini-Mental State Examination scores. In cognitively impaired groups, left anterior cingulate coupling was negatively correlated with plasma glial fibrillary acidic protein (GFAP) levels. AD patients showed decreased ReHo-CBF coupling in the left inferior frontal and middle temporal gyri.
Conclusions
Neurovascular coupling dysfunction is significantly linked to cognitive impairment along the AD continuum. Reduced coupling values in key regions correlated with impaired cognition and higher plasma GFAP levels, underscoring vascular-metabolic and astroglial contributions. These findings support ALFF-CBF coupling as a promising non-invasive biomarker for early AD detection and disease monitoring.
Keywords
Introduction
Alzheimer's disease (AD) is a progressive neurodegenerative disorder and the leading cause of dementia. 1 Characteristic neuropathological features of AD include neurofibrillary tangles (NFTs) and amyloid-β (Aβ) plaques. The brains of individuals with AD show elevated levels of hyperphosphorylated tau protein, Aβ, and neuronal loss.2,3 Epidemiological, clinical, pathological, and experimental studies in recent decades indicate that early neurovascular dysfunction may be a critical factor in AD progression.4,5 There is increasing evidence that AD-related pathologies, including Aβ and tau, may contribute to neurovascular unit dysfunction, resulting in impaired neurovascular coupling (NVC). 6 However, these findings have primarily been observed in animal models; there is limited in vivo evidence from studies involving humans. 7 The relationship between plasma Aβ levels and neurovascular dysfunction remains poorly understood.
Recent advancements in in vivo imaging techniques have enhanced the broader understanding of pathophysiology across the AD continuum. Resting-state functional magnetic resonance imaging (rs-fMRI), which utilizes measures such as amplitude of low-frequency fluctuation (ALFF) and regional homogeneity (ReHo), has revealed abnormal neuronal activity in the default mode network regions.2,8,9 Arterial spin labeling (ASL), a non-invasive method for measuring cerebral blood flow (CBF) via magnetic tagging of blood water spins, eliminates the need for contrast agents. 10 Studies using ASL have revealed decreased perfusion in regions such as the posterior cingulate; precuneus; and occipital, temporal, and parietal cortices.11,12 NVC refers to the complex process through which neuronal activity induces an increase in blood flow to active brain regions. This mechanism relies on the release of vasoactive agents from neurons and astrocytes to ensure adequate oxygen and nutrient resources for neuronal function. Although the precise mechanisms underlying NVC are not fully understood, Liang et al. introduced a novel approach for characterizing NVC in 2013. 13 Recent studies indicate that NVC dysfunction may contribute to AD pathogenesis. 5 For instance, Li et al. reported that Aβ-positive individuals exhibited reduced NVC, particularly in the left medial and inferior temporal gyri; this reduction was associated with cognitive performance. 7
The present study aimed to investigate the relationship between regional neuronal activity and cerebral perfusion, as measured by rs-fMRI and ASL, across the AD continuum. Based on prior findings, we hypothesized that NVC would be disrupted across the AD spectrum. We also hypothesized that NVC would be correlated with cognitive performance and AD-associated plasma biomarkers.
Methods
Participants
This cross-sectional study included 153 individuals who were recruited from the community via advertisement. All participants underwent blood sampling, neuropsychological assessments, and MRI scans. Seventeen individuals were excluded due to poor image quality. Thus, only 136 participants were included in the analysis. AD dementia was diagnosed based on criteria established by the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association. 14 These criteria include: (1) a gradual onset of symptoms developing over several months or years, rather than a sudden onset over hours or days; (2) documented or observed evidence of progressive cognitive decline; (3) memory impairment as the initial and most prominent symptom, confirmed through clinical history and neuropsychological assessment; and (4) the absence of substantial concomitant conditions such as significant cerebrovascular disease, core features of dementia with Lewy bodies, prominent features of frontotemporal dementia, or evidence of another active neurological disorder. Mild cognitive impairment (MCI) was diagnosed using neuropsychological criteria proposed by Jak and Bondi. 15 Participants were classified as having MCI if they did not meet criteria for dementia and fulfilled at least one of the following conditions: (1) two test scores within a single cognitive domain (memory, language, or processing speed/executive function) were more than 1 standard deviation below the normative mean, adjusted for age and education; (2) one impaired score was observed in each of the three cognitive domains; or (3) a score of ≥9 was obtained on the Functional Activities Questionnaire. Cognitively normal (CN) individuals had a Clinical Dementia Rating of 0 and no history of cognitive decline.
The study protocol was approved by the ethics committee of Hainan General Hospital. Written informed consent was obtained from all participants or their legal guardians. Clinical data collected for each participant included age, sex, education level, and apolipoprotein E (APOE) genotype.
Neuropsychological assessments
Global cognitive function was assessed using the Mini-Mental State Examination (MMSE). Episodic memory was evaluated with the 30-min delayed free recall (AVLT-N5) and recognition task (AVLT-N7) components of the Auditory Verbal Learning Test. Executive function was measured using sections A and B of the Shape Trail Test. Language function was evaluated with the Verbal Fluency Test and Boston Naming Test. Each participant's raw test scores within each domain were standardized into z-scores based on the mean and standard deviation for the test. The z-scores from all tests within a domain were then averaged to calculate a mean z-score for that domain.
Plasma biomarkers
Venous blood samples (2 ml) were collected in ethylenediaminetetraacetic acid (EDTA) tubes, then centrifuged at 4°C for 15 min at 2500 g/min. The resulting plasma supernatants were isolated and stored at −80°C; each sample was thawed on ice prior to analysis. Levels of plasma glial fibrillary acidic protein (GFAP) and neurofilament light chain (NfL) were quantified using the Single Molecule Array (Simoa™) platform (Quanterix Corporation, Billerica, MA, USA), in accordance with the manufacturer's instructions. The assays utilized commercial kits: the Simoa™ GFAP Discovery Kit for GFAP and the Simoa™ NF-light® Advantage Kit for NfL. All measurements were performed in duplicate, and mean concentrations were reported. Values below the lower limit of quantification (LLOQ) were recorded as one-half of the LLOQ.
MRI data acquisition and processing
MRI examinations of all participants were performed using a 3T MAGNETOM Prisma scanner (Siemens Healthineers, Erlangen, Germany) equipped with a 64-channel head/neck receiver coil. The imaging protocol included a simultaneous multi-slice (SMS) echo planar imaging sequence for rs-fMRI, a three-dimensional (3D) MPRAGE T1-weighted sequence for anatomical imaging, and a 3D pseudo-continuous ASL (PCASL) sequence with multiple post-label delays for perfusion analysis. The scanning parameters were (1) for rs-fMRI: SMS factor = 2, repetition time (TR) = 2000 ms, echo time (TE) = 30 ms, matrix size = 94 × 94, field of view (FOV) = 224 × 224 mm2, number of slices = 64, slice thickness = 2.4 mm, and 480 volumes; (2) for MPRAGE T1-weighted imaging: TR = 2300 ms, TE = 2.26 ms, inversion time = 900 ms, flip angle = 8°, slice thickness = 1 mm, FOV = 256 × 256 mm2, and voxel size = 1 × 1 × 1 mm3; and (3) for PCASL perfusion imaging: TR = 4200 ms, TE = 37.78 ms, five post-label delays set at 500, 1000, 1500, 2000, and 2500 ms, slice thickness = 3 mm, FOV = 240 × 240 mm2, and voxel size = 2.5 × 2.5 × 3 mm3. Routine MR sequences, including T2-weighted imaging and T2-fluid-attenuated inversion recovery (T2-FLAIR), were also utilized to identify brain abnormalities.
fMRI preprocessing
Data preprocessing was performed using SPM12 (http://www.fil.ion.ucl.ac.uk/spm) and the Data Processing and Analysis of Brain Imaging toolbox (DPABI, Version 6.0, http://rfmri.org/dpabi). 16 Preprocessing steps included converting the images to NIFTI format and discarding the first 10 volumes. Slice timing correction and realignment were conducted to correct for head motion; participants with head motion exceeding 3.0 mm or 3.0° were excluded. Realigned images were spatially normalized to the Montreal Neurological Institute (MNI) template and transformed into Z-scores. To improve signal quality, normalized functional images were smoothed with a Gaussian kernel of 8 mm full width at half maximum (FWHM). Low-frequency fluctuations were retained by applying a bandpass filter within the 0.01–0.1 Hz range.
ALFF and ReHo calculation
ALFF and ReHo were computed using DPABI software (Version 6.0, http://rfmri.org/dpabi).16 ALFF was calculated by transforming the time series of each voxel into the frequency domain via fast Fourier transform. ALFF values were obtained by averaging the square root of the power spectrum across the frequency range of 0.01–0.08 Hz for each voxel.
For ReHo calculation, normalized images were bandpass filtered within the 0.01–0.08 Hz range prior to generation of the ReHo map. Voxel-wise ReHo values were calculated using Kendall's coefficient of concordance to measure the consistency between a voxel and its neighboring voxels. To minimize individual variability, each voxel's ReHo value was normalized via division by the global mean ReHo value. Spatial smoothing was subsequently applied using a Gaussian kernel of 8 mm FWHM.
CBF calculation
CBF maps were generated using control and label images from 3D ASL. SPM12 was employed to perform rigid body transformation, aligning MPRAGE T1-weighted images to reference ASL M0 images. Aligned MPRAGE T1-weighted images were then normalized to the MNI standard space. The same transformation parameters were applied to CBF images to achieve spatial alignment. Smoothing with a Gaussian kernel of 8 mm FWHM was applied to spatially normalized images to reduce noise. Gray matter and white matter templates in SPM12 were thresholded at 0.5 to create gray and white matter masks. A whole-brain mask was generated by combining the gray and white matter templates and applying a threshold of 0.5.
Brain region-based NVC analysis
The Anatomical Automatic Labeling (AAL) Atlas was used to divide the cerebrum into 90 distinct regions. For each brain region, correlation analyses between the regional synchronization of neuronal activity (ALFF maps, ReHo maps) and local cerebral perfusion (CBF maps) across voxels were conducted to quantitatively evaluate the NVC: ALFF-CBF and ReHo-CBF.
Statistical analysis
Demographic data were analyzed using IBM SPSS Statistics Version 21 (IBM, Armonk, NY, USA); p-values < 0.05 were considered statistically significant. Continuous variables were presented as mean ± standard deviation, whereas categorical variables were reported as numbers. Age, education, MMSE score, memory, executive function, language, GFAP level, and NfL level were analyzed by analysis of variance. The Chi-square test was utilized to assess differences in sex and APOE4 status.
Using the AAL Atlas (90 regions, excluding the cerebellum), the cerebrum was parcellated into anatomically defined regions of interest. For each region, voxel-wise Pearson correlations between spontaneous neuronal activity (as measured by ALFF and ReHo maps) and local cerebral blood flow (CBF maps) were calculated across voxels within that region, resulting in regional ALFF-CBF and ReHo-CBF coupling coefficients. These regional coefficients were considered indices of NVC. Group comparisons of these regional NVC values were conducted among the CN, MCI, and AD groups using one-way analysis of variance. To control for multiple comparisons across regions, Bonferroni correction was applied (corrected significance threshold p < 0.00056, 0.05/90). When significant group effects were observed, post hoc pairwise comparisons were performed using the Bonferroni correction to adjust for multiple comparisons. Partial correlation analysis was performed to evaluate relationships among the ALFF-CBF, neuropsychological performance, and AD biomarkers, with adjustments for age, sex, and education. To address potential confounding factors, APOE4 status was included as a covariate in additional analyses.
Results
Demographic and clinical characteristics
This study included 133 participants, comprising 23 CN individuals, 80 participants with MCI, and 33 AD dementia patients. Table 1 provides a summary of the demographic and clinical characteristics of each group. Sex (p = 0.303) and APOE4 status (p = 0.125) did not significantly differ across the groups. Plasma Aβ42/40 levels demonstrated an increasing trend from CN to MCI to AD, although the groupwise differences were not statistically significant. Cognitive performance was lowest in the AD dementia group, intermediate in the MCI group, and highest in the CN group.
Demographic and clinical characteristics of the study population.
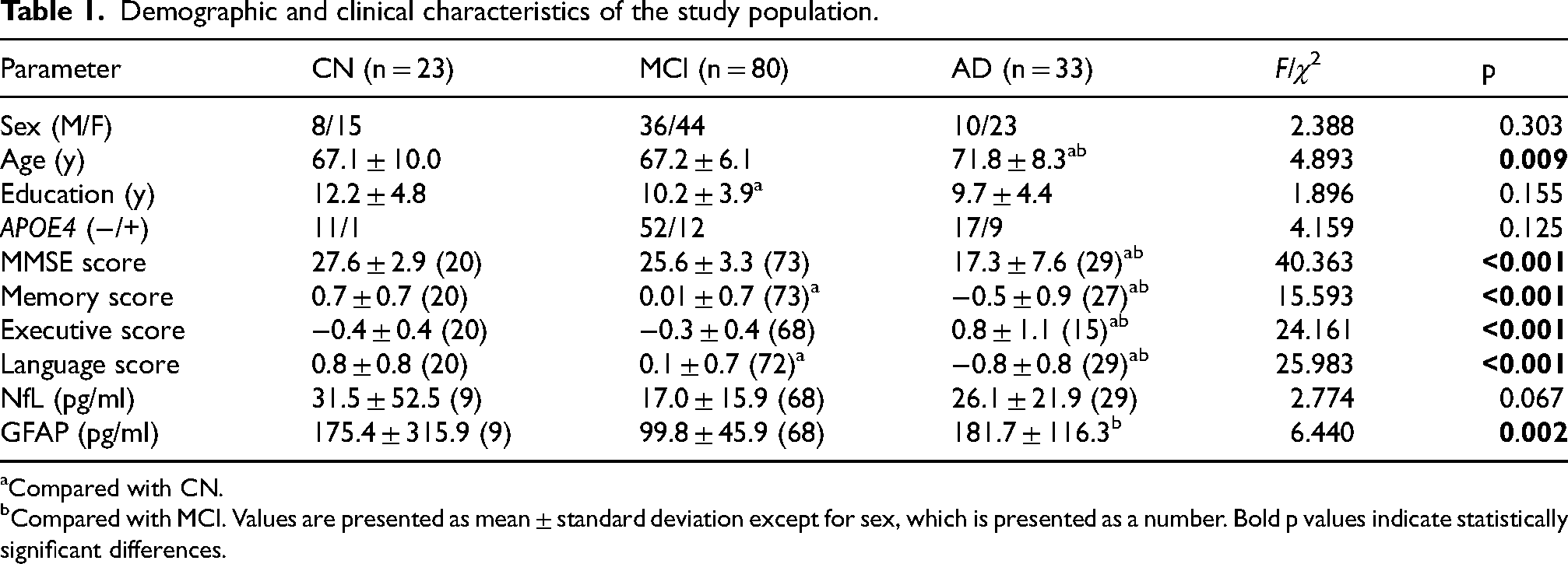
Compared with CN.
Compared with MCI. Values are presented as mean ± standard deviation except for sex, which is presented as a number. Bold p values indicate statistically significant differences.
Groupwise differences in NVC values at the regional level
NVC values, represented by ALFF-CBF and ReHo-CBF coefficients, were analyzed and compared among the three groups using the AAL atlas. ALFF-CBF maps revealed significant between-group differences in nine brain regions (Figure 1): the triangular part of the left inferior frontal gyrus, left anterior cingulate gyrus, left middle cingulate gyrus, right middle cingulate gyrus, left inferior occipital gyrus, left paracentral lobule, right paracentral lobule, right pallidum, and left superior temporal gyrus (p < 0.05, uncorrected). However, after applying Bonferroni correction for multiple comparisons across 90 regions (p < 0.00056), only the left anterior cingulate gyrus remained statistically significant.
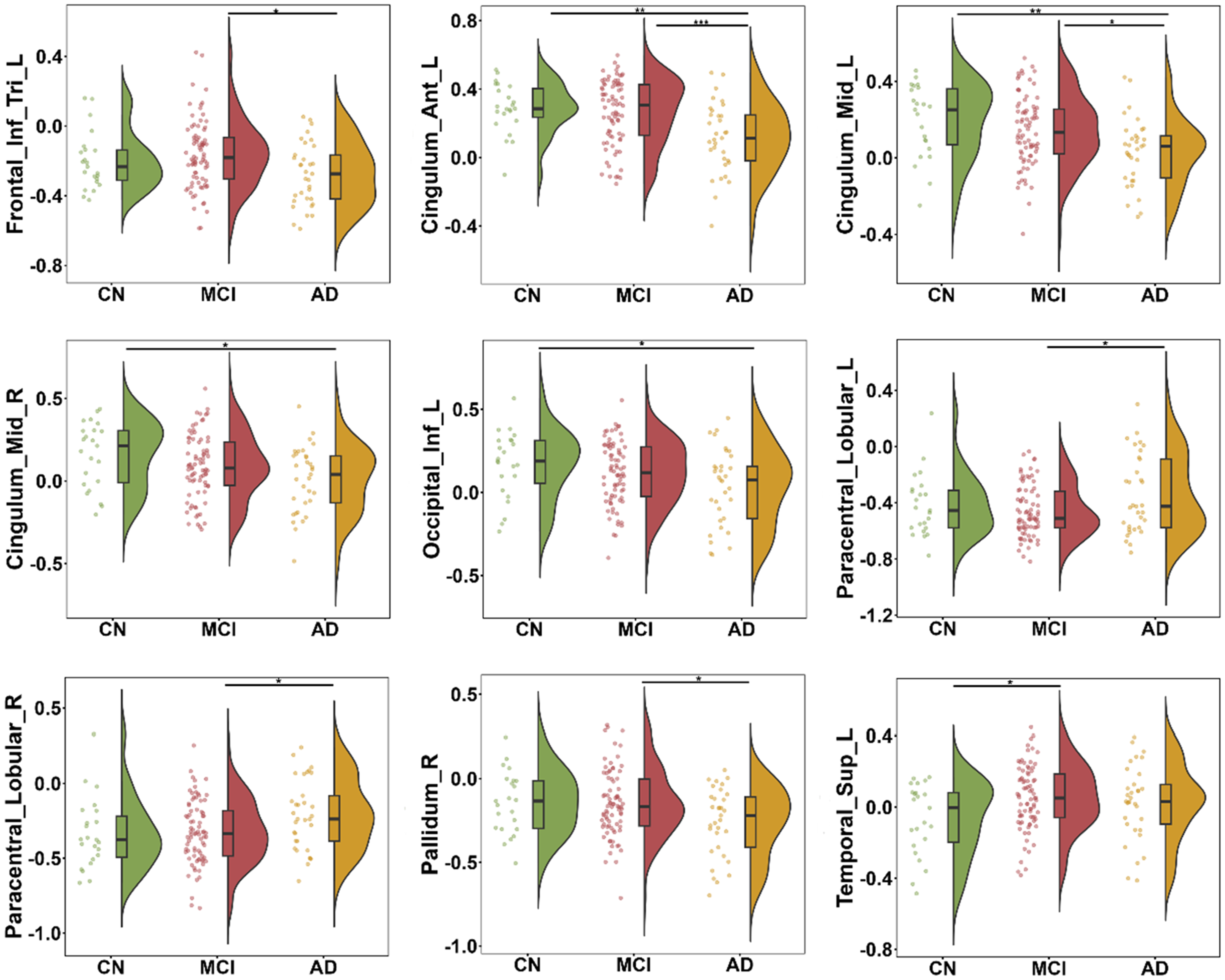
Differences in regional ALFF-CBF coupling values among the three groups. Nine brain regions showed significant differences across the CN, MCI, and AD dementia groups (one-way ANOVA, p < 0.05, uncorrected). Lines between groups indicate significant post hoc differences identified using Bonferroni-adjusted pairwise comparisons. *p < 0.05; **p < 0.01; ***p < 0.001. CN: cognitively normal; MCI: mild cognitive impairment; AD: Alzheimer's disease.
Post hoc pairwise comparisons among the three groups were then conducted within these nine regions, and Bonferroni correction was applied. Based on corrected post hoc results, the AD group exhibited lower coupling values than the MCI group in the triangular part of the left inferior frontal gyrus and the right pallidum but showed higher coupling values in the bilateral paracentral lobules. Compared with the CN and MCI groups, the AD group displayed lower coupling values in the left anterior cingulate gyrus and left middle cingulate gyrus. The AD group also had lower coupling values than the CN group in the right middle cingulate gyrus and left inferior occipital gyrus. Additionally, the MCI group demonstrated significantly higher coupling values in the left superior temporal gyrus relative to the CN group.
After Bonferroni correction had been applied, significant differences in ReHo-CBF coefficients were observed in two brain regions across the groups: the triangular part of the left inferior frontal gyrus and the left middle temporal gyrus, as illustrated in Supplemental Figure 1.
Analyses of correlations between cognitive performance and ALFF-CBF coupling values
As shown in Figure 2, coupling values in the left anterior cingulate gyrus, left middle cingulate gyrus, right middle cingulate gyrus, and right pallidum were positively correlated with MMSE scores (r = 0.30, p = 0.002; r = 0.27, p = 0.005; r = 0.23, p = 0.016; r = 0.26, p = 0.006, respectively) across the three groups. Conversely, coupling values in the right paracentral lobule were negatively correlated with MMSE scores (r = −0.22, p = 0.022). After correction for multiple comparisons (Bonferroni correction, 0.05/13 = 0.004), the association between the left anterior cingulate gyrus and MMSE score remained statistically significant. Supplemental Figure 2 depicts the relationship between ReHo-CBF coupling values and global cognition.
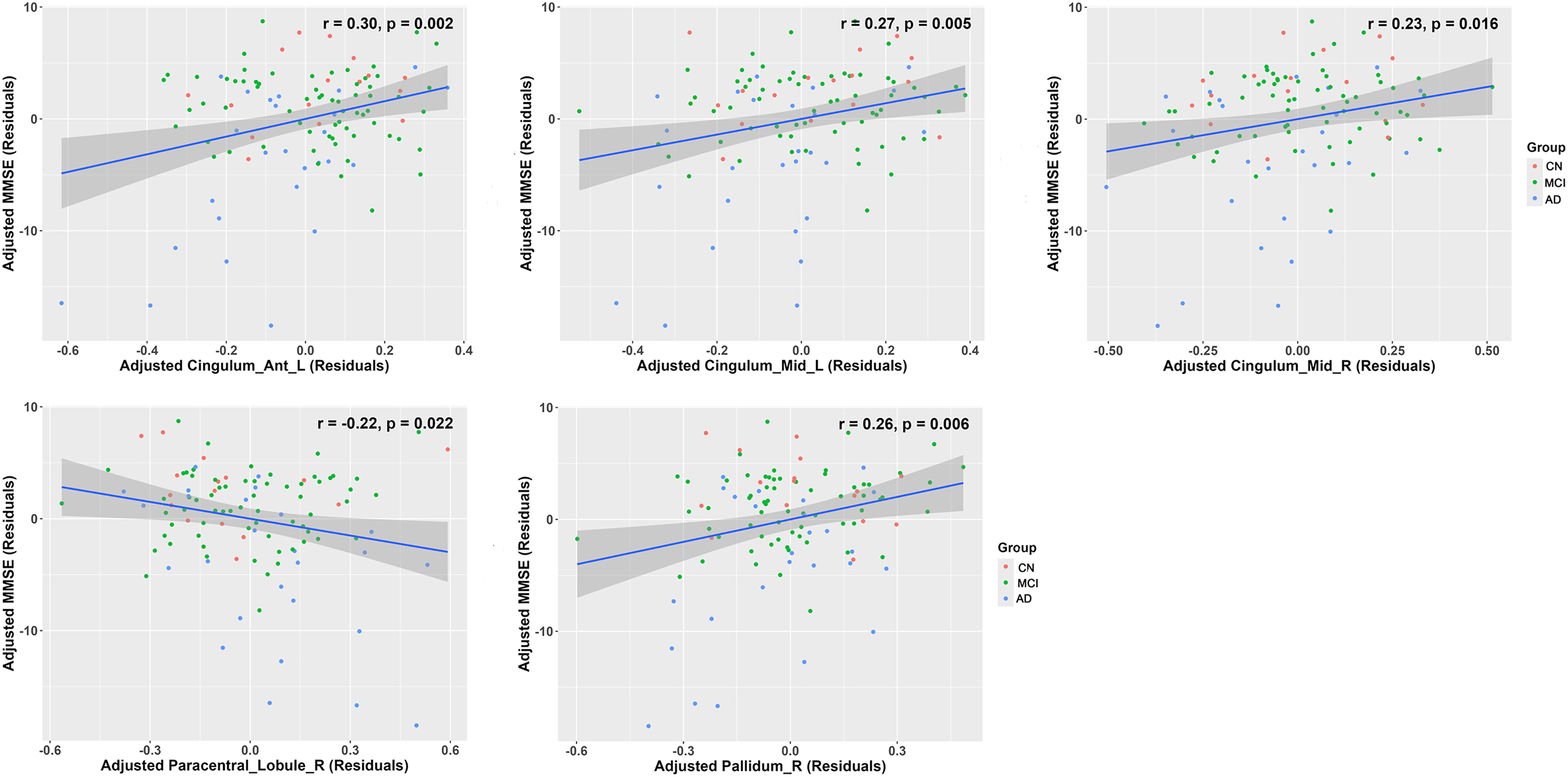
Partial correlation analyses between regional ALFF-CBF coupling values and MMSE scores across all participants, adjusted for age, sex, and education level. MMSE scores were positively correlated with coupling values in the left anterior cingulate gyrus, left middle cingulate gyrus, right middle cingulate gyrus, and right pallidum (r = 0.30, p = 0.002; r = 0.27, p = 0.005; r = 0.23, p = 0.016; r = 0.26, p = 0.006, respectively) across the three groups. Coupling values in the right paracentral lobule were negatively correlated with MMSE scores (r = −0.22, p = 0.022). MMSE: Mini-Mental State Examination; CN: cognitively normal; MCI: mild cognitive impairment; AD: Alzheimer's disease.
Analyses of correlations between coupling values and memory/language functions were performed after adjustments for age, sex, and education level. As shown in Figure 3, coupling values in the left anterior cingulate gyrus and right pallidum were positively correlated with memory function (r = 0.23, p = 0.021; r = 0.21, p = 0.034, respectively) across the three groups. Regarding language scores, coupling values in the left inferior occipital gyrus and right paracentral lobule showed positive and negative correlations, respectively (r = −0.20, p = 0.039; r = −0.21, p = 0.029).
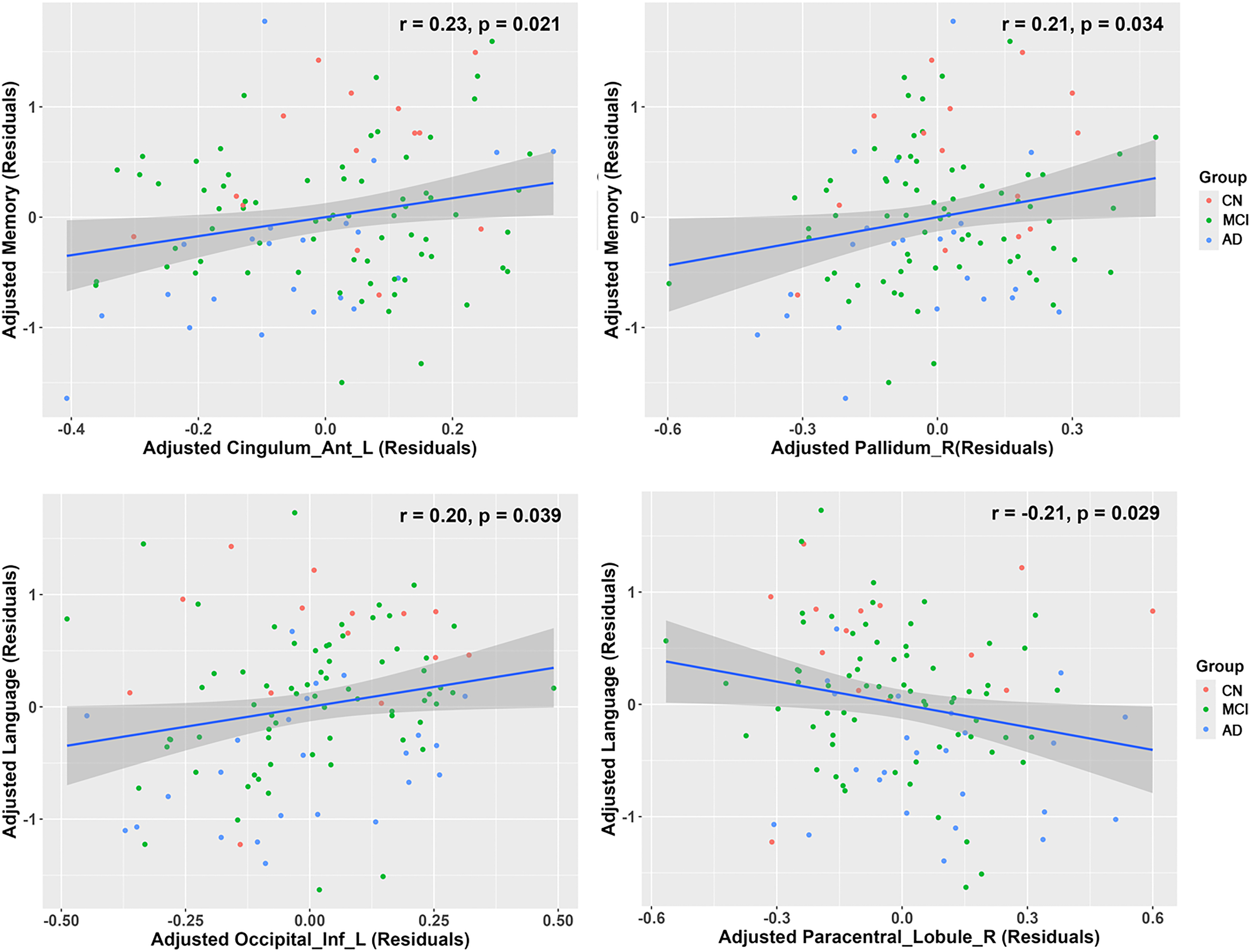
Analyses of correlations between coupling values and memory/language function, adjusted for age, sex, and education level. Coupling values in the left anterior cingulate gyrus and right pallidum were positively correlated with memory function (r = 0.23, p = 0.021; r = 0.21, p = 0.034, respectively) across the three groups. Coupling values in the left inferior occipital gyrus and right paracentral lobule were positively and negatively correlated with language scores, respectively (r = −0.20, p = 0.039; r = −0.21, p = 0.029). CN: cognitively normal; MCI: mild cognitive impairment; AD: Alzheimer's disease.
Analyses of correlations between plasma AD biomarkers and ALFF-CBF coupling values
Figure 4 shows correlations between coupling values and plasma GFAP values after adjustments for age and sex. Across the cognitively impaired groups, coupling values in the left anterior cingulate gyrus were negatively correlated with plasma GFAP levels (r = −0.40, p < 0.001). This association remained statistically significant after additional adjustments for education and APOE4 status.
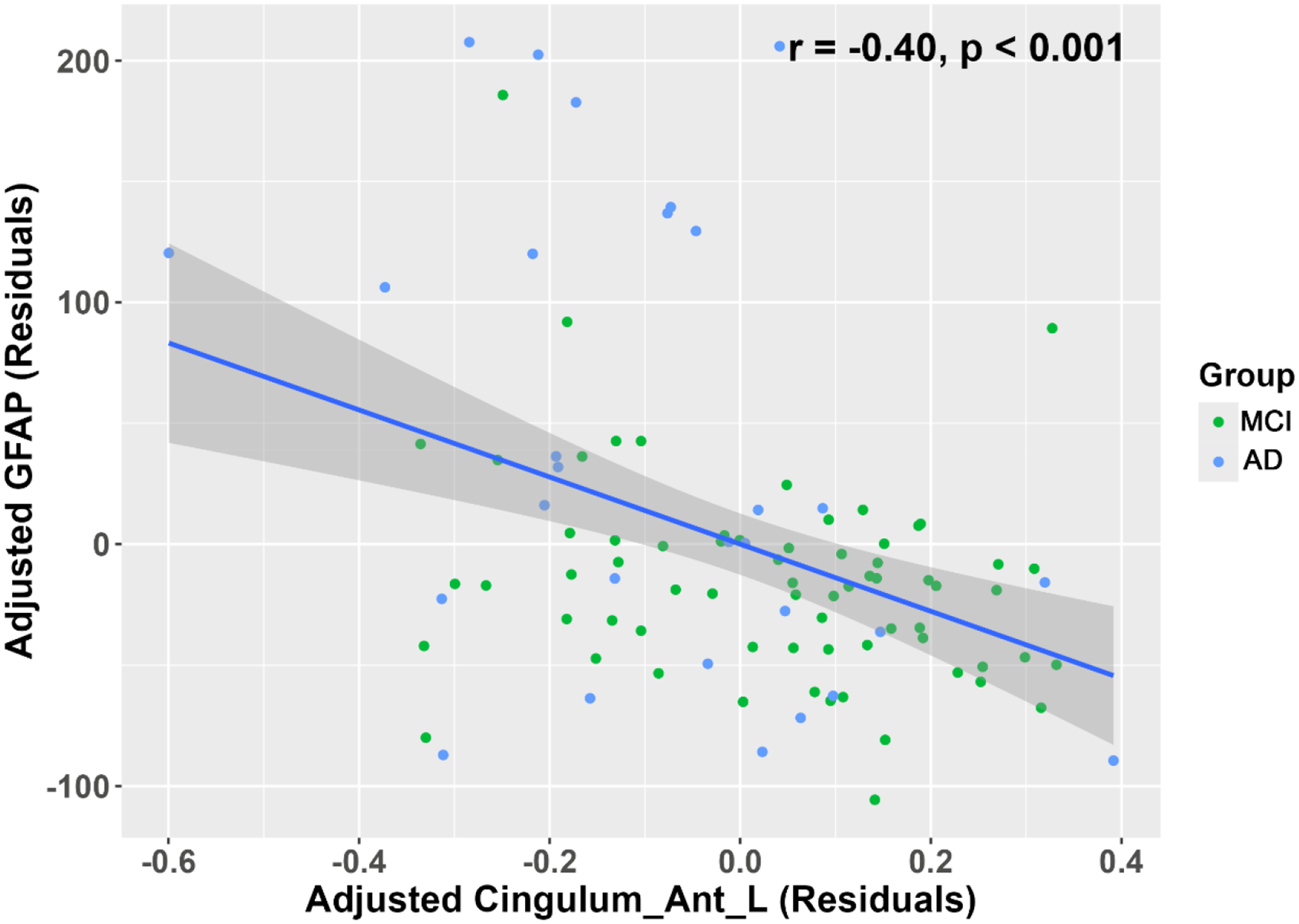
Analyses of correlations between coupling values and plasma GFAP levels, adjusted for age and sex. Coupling values in the left anterior cingulate gyrus were negatively correlated with plasma GFAP levels (r = −0.40, p < 0.001) across the cognitively impaired groups.
Discussion
This study examined changes in NVC, represented by the ALFF-CBF and ReHo-CBF coupling coefficients, across the AD continuum. The AD group exhibited significantly lower coupling values in several regions, including the triangular parts of the bilateral inferior frontal gyrus, the left anterior cingulate gyrus, left middle cingulate gyrus, and right middle cingulate gyrus. Our key findings were that an altered CBF/ALFF ratio was associated with worse global cognitive performance, reduced memory function, and a higher burden of neuroinflammation. Although several regions showed uncorrected significance, only the left ACC remained statistically significant after applying Bonferroni correction for multiple comparisons. Thus, findings from other regions should be interpreted with caution and considered exploratory.
We observed a significant reduction in NVC values in the left anterior cingulate cortex (ACC) among AD patients relative to CN individuals and participants with MCI, and this region was the only one to remain significant after strict Bonferroni correction, underscoring the robustness of this finding. This finding is consistent with increasing evidence that emphasizes early ACC involvement in AD pathology. The ACC plays important roles in cognitive processes such as attention, decision-making, and emotional regulation; ACC dysfunction has been strongly associated with the onset of cognitive decline in AD.17,18 In the present study, coupling values in the ACC were significantly correlated with MMSE scores and memory function, indicating a strong relationship between altered coupling values and cognitive performance. Previous studies have shown that the ACC is among the earliest brain regions to undergo functional and structural changes in AD,19,20 particularly with respect to NVC and CBF. 21 Our finding of decreased NVC within the ACC may reflect neurovascular dysfunction. This disruption could result from Aβ accumulation, which impairs vascular regulation and NVC in early stages of AD. 22 Additionally, tau pathology in the ACC has been documented in early stages of AD, highlighting this region's susceptibility to pathological changes during AD onset. 18 Further longitudinal studies are needed to determine whether the decline in NVC begins during the MCI stage. Such research should track changes among individuals with MCI over time to clarify whether NVC deterioration within the ACC occurs in early stages of AD.
Intriguingly, the MCI group exhibited significantly higher ALFF-CBF values in the left superior temporal gyrus compared with the CN group, offering novel insights into the pathophysiological mechanisms underlying MCI. The superior temporal gyrus is a key region involved in auditory processing and higher-order cognitive functions, including language and memory. 23 Elevated NVC in this region may reflect compensatory mechanisms aimed at preserving cognitive performance during early stages of neurodegeneration. Previous studies have shown that the hippocampus and adjacent structures (e.g., entorhinal cortex, subiculum, and superior temporal gyrus) are among the earliest brain regions to exhibit pathological changes and neuronal degeneration.24,25 Increased neural activity in response to cognitive demands during MCI may drive heightened metabolic and vascular responses, which are reflected in higher NVC values. However, this compensatory phenomenon may decline during disease progression, consistent with the lower coupling displayed by AD patients in the present study. Further research is needed to determine whether increased coupling in the superior temporal gyrus can serve as a biomarker for early-stage neurovascular dysregulation in MCI.
Additionally, this study showed increased ALFF-CBF coupling values in the right paracentral lobule, a language-related region. The paracentral lobule is part of the frontoparietal network, which is involved in decision-making, action modification, and the integration of external information with mental representations. 26 Previous research has revealed increased functional connectivity within the paracentral lobule in AD patients, which aligns with our findings. 27 Increased coupling values in the right paracentral lobule may reflect a compensatory mechanism. We also found that coupling values in the paracentral lobule were associated with language function.
The present study identified a significant negative correlation between NVC values in the left ACC and plasma GFAP levels across the cognitively impaired groups. This finding suggests that GFAP-associated pathological processes disrupt neurovascular function in this region, thereby exacerbating neurodegenerative changes. GFAP, a marker of astrocyte activation, has recently been recognized as an important biomarker for AD biological diagnosis. 28 Elevated GFAP levels reflect astrocytic responses to neurodegeneration, including neuroinflammation and blood-brain barrier dysfunction, both of which contribute to neurodegenerative disease progression.29,30 Astrocytes play a crucial role in maintaining NVC by regulating cerebral blood flow and supporting neuronal metabolic demands. The left anterior cingulate cortex, a key component of the default mode network, plays key roles in cognitive control and emotional regulation. Impaired NVC in this region could compromise its functional integrity, contributing to the cognitive deficits observed in MCI and AD. Elevated GFAP levels may indicate astrocytic dysfunction that impairs astrocyte-neuron-vascular communication or promoting inflammation-related vascular damage. This astrocytic pathology could therefore represent a mechanistic link between neuroinflammation and neurovascular dysfunction in AD. Moreover, recent evidence suggests that astrocyte activation, as indexed by GFAP, not only reflects a response to Aβ and tau pathology but may also actively contribute to neurodegeneration through altered metabolic support and inflammatory signaling. These results highlight the potential utility of GFAP as a biomarker for neurovascular dysfunction and cognitive impairment in neurodegenerative diseases. Further longitudinal studies integrating plasma GFAP measurements with neuroimaging of NVC and cognitive assessments are warranted to elucidate the temporal dynamics and causal relationships of astrocyte activation and neurovascular impairment in AD progression.
To our knowledge, this is the first study to explore the relationship between compromised NVC and plasma biomarkers via neuroimaging. However, the study had some limitations. First, the modest sample size may have diminished the statistical power of the analyses, considering that some correlations did not remain statistically significant after Bonferroni correction. Larger-scale studies are needed to validate our findings. Second, the absence of PET data in this study hindered direct assessments of amyloid and tau pathologies. Third, the cross-sectional design precluded establishment of a temporal relationship between CBF/ALFF ratios and AD pathology. Fourth, although the CBF/ALFF ratio serves as an indirect measure of NVC, it does not allow precise assessments of the neurovascular unit. Finally, the diagnostic criteria used for AD and MCI were based on previously established frameworks, including the NINCDS-ADRDA criteria for AD 14 and the neuropsychological approach proposed by Jak and Bondi for MCI, 15 rather than the recently updated 2024 Alzheimer's Association Workgroup criteria. This may affect the classification of patients and could limit the generalizability of the findings. Future studies should consider adopting the latest diagnostic standards to enhance consistency across studies and improve clinical applicability.
Conclusion
This study demonstrated that NVC is impaired in AD patients; it showed a decreasing trend across CN individuals, MCI participants, and AD patients. The observed reduction in CBF–ALFF coupling values, particularly in the left anterior and middle cingulate gyri, may reflect impaired coordination between neuronal activity and cerebral perfusion. These alterations were associated with both lower cognitive performance and higher plasma GFAP levels, suggesting a potential relationship between vascular-metabolic dysregulation and astroglial activation. Abnormalities in NVC can serve as non-invasive biomarkers for early detection of AD and offer new insights into pathological mechanisms the neurovascular mechanisms underlying AD pathophysiology.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251375476 - Supplemental material for Neurovascular coupling dysfunction associated with cognition and glial fibrillary acidic protein along the Alzheimer's disease continuum
Supplemental material, sj-docx-1-alz-10.1177_13872877251375476 for Neurovascular coupling dysfunction associated with cognition and glial fibrillary acidic protein along the Alzheimer's disease continuum by Huijuan Chen, Yihao Guo, Zhanrong Zhang, Weiyuan Huang, Kun Zhang, Haodong Qin, Feiyun Wu, Tao Liu and Feng Chen in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors thank all study participants for their efforts.
Ethical considerations
The study protocol was approved by the ethics committee of Hainan General Hospital. The study complied with the World Medical Association Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from all participants or their legal guardians.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Key Science and Technology Project of Hainan Province (ZDYF2024SHFZ058, ZDYF2023SHFZ096), the National Natural Science Foundation of China (82271977, 82160327), the Hainan Academician Innovation Platform Scientific Research Project (YSPTZX202514), the Hainan Province ‘Nanhai Risi Star’ Healthcare Talent Platform Project (NHXXWJW-2023003), the Hainan Provincial Natural Science Foundation of China (825RC870), the Hainan Province Clinical Medical Center, and the Innovation Platform for Academicians of Hainan Province.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author when the appropriate data sharing agreements are consented.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.