
Abstract
Background
Dementia with Lewy bodies (DLB) is one of the main degenerative dementias after Alzheimer's disease and is characterized by neurovisual deficits. Volumetric MRI data on these deficits and their neuro-anatomical correlates are lacking.
Objective
We propose a volumetric analysis of the neuro-anatomical substrates of neurovisual deficits in DLB, as assessed by subtests of the Visual Object and Space Perception (VOSP) battery and the Rey-Osterrieth Complex Figure (ROCF).
Methods
Seventy patients with prodromal to mild DLB were included in the study, along with 23 healthy elderly subjects (NCT01876459). We used VOSP's incomplete letters (LET) for object perception, and dot counting (DOT) for space perception. The ROCF copy was used to assess visuoconstruction. Correlation analyses were performed in voxel-based morphometry (VBM).
Results
VBM analyses showed a positive correlation between LET performance and the left cerebellar hemisphere (p < 0.05, family-wise error). Positive correlations between LET performance and bilateral occipitotemporal cortex were also demonstrated (p < 0.001 uncorrected). VBM analyses showed a positive correlation between DOT performance and both occipitoparietal cortex and cerebellum (p < 0.001 uncorrected). ROCF performance was positively correlated with frontoparietal cortex (p < 0.001 uncorrected).
Conclusions
Visuoperceptive performance (i.e., on LET) was associated with the occipitotemporal cortex, corresponding to the “what” pathway, while performance involving visuospatial skills (i.e., on DOT and ROCF) was associated with the occipitoparietal cortex, corresponding to the “where” pathway. The cerebellum also appears to be involved, predominantly in visuoperception (LET). This exploratory work suggests the involvement of the cerebellum in the neurovisual impairment of DLB, alongside other regions classically involved in visuoperception.
Introduction
Dementia with Lewy bodies (DLB) is one of the main degenerative dementias after Alzheimer's disease (AD). 1 DLB is characterized by an accumulation of phosphorylated alpha-synuclein within Lewy bodies of diffuse localization. 2 Its prevalence is estimated at 0.7% of people over the age of 65, 3 and it accounts for 23% of cases in memory clinic patients according to a seed amplification assay (α-synuclein RT-QuIC). 4 The sex ratio of DLB is 1.2, with a slight female predominance. 5 The main clinical features of DLB include cognitive and vigilance fluctuations, recurrent visual hallucinations, rapid eye movement sleep behavior disorder (RBD) and parkinsonism. 6 Cognitive testing of DLB patients at prodromal and very mild stage 7 demonstrates prominent deficits in executive functions, including impaired retrieval in verbal episodic memory and working memory, and attention, including impaired short-term memory, with a slower processing speed than controls. Aside from this frontal-subcortical syndrome, studies have also highlighted impairments in visual recognition memory, visuoconstruction and weakened visuospatial abilities. These deficits worsen at a dementia stage, with a more severe frontal-subcortical syndrome, more impaired episodic memory and more impaired neurovisual functions, both for visuospatial and visuoperceptual abilities, as evaluated in space and object perception tasks. 8
Neurovisual functions include visuoperception, visuospatial abilities and visuoconstruction. Visuoperception consists in the integration of information derived from visual stimuli. This information relates to the characteristics of the stimuli (such as their shape, color or texture), as well as their organization in space. Research in monkeys 9 and in humans 10 has shown that these two types of information are processed by partially distinct networks. On the one hand, the ventral, occipito-temporal pathway is used to process the characteristics of objects (the “what” pathway): its impairment is responsible for object agnosia. On the other hand, the dorsal, occipito-parietal pathway processes information about the location of visual stimuli in space (the “where” pathway): its alteration is responsible for visuospatial impairment. Visuoconstruction consists in the production of simple or complex shapes, using drawing, puzzle solving or figure assembly. Research on focal brain-lesion subjects suggests that visuoconstructive abilities are supported by the parietal cortex: the left parietal cortex is involved in praxis abilities allowing the completion of complex construction actions, and the right parietal cortex is involved in spatial analysis. 11
We currently lack evidence regarding the neural correlates of visual deficits in DLB. A functional-MRI study has shown functional dysconnectivity in visuospatial regions during the intertask of a fragmented letters paradigm. 12 To our knowledge no study has been conducted with volumetric MRI data to specifically assess the neural bases of visuoperception and visuoconstruction deficits in patients with DLB.
We therefore conducted a volumetric analysis of the neural correlates of neurovisual impairment in DLB assessed by the Visual and Spatial Object Perception (VOSP) battery and the Rey-Osterrieth Complex Figure (ROCF). For perceptual tasks, we hypothesized an involvement of the occipitotemporal and occipito-parietal cortex, corresponding to the “what” and “where” pathways, respectively. For constructive tasks, we hypothesized an involvement of the bilateral parietal cortex.
Methods
Study design
We conducted a multicenter, observational cohort study, with prospective data collection. The study followed patients with DLB and elderly healthy control (HC) subjects. Our study compared the clinical, neuropsychological and brain imaging characteristics of the participants according to their group (DLB or HC). Our report follows the STROBE guidelines.
Setting
DLB patients and HC subjects were recruited in the memory clinics of two French hospitals: Strasbourg University Hospital (neurology and geriatrics departments) and Colmar Civil Hospitals (geriatrics department). The inclusions spanned the years 2013 to 2016. Patients were followed for 96 months. Data were collected between May and October 2023. This study was carried out within the scope of the AlphaLewyMA cohort (NCT01876459, 2013), was in accordance with the 1964 Helsinki Declaration and its later amendments and was approved by the Ethics Committee of East France (IV). Written informed consent was obtained from the patients and controls prior to their inclusion in the study.
Participants
Inclusion in the DLB group of the AlphaLewyMA cohort was proposed to patients over 50 years of age consulting one of the two centers and presenting signs suggestive of DLB. Patients had to fulfill the criteria for mild neurocognitive disorder or major neurocognitive disorder. 13 All patients were examined by trained clinicians with expertise in cognitive disorders. The diagnosis of DLB was then confirmed if patients fulfilled the DLB consortium's clinical current and formal diagnosis criteria,6,14,15 for dementia and prodromal stages respectively. To exclude AD copathology, all patients underwent a lumbar puncture. Four biomarkers were analyzed to assess AD in cerebrospinal fluid: amyloid-β (Aβ)42 (N > 600 ng/L), Aβ42/Aβ40 ratio (N > 5.0%), total tau (t-Tau, N < 500 ng/L) and phosphorylated tau (p-Tau, N < 75 ng/L). Aβ42 and the Aβ42/Aβ40 ratio were considered biomarkers of amyloidopathy, while t-Tau and p-Tau were considered biomarkers of tauopathy. AD pathology was defined as the presence of at least one pathological biomarker of amyloidopathy and at least one pathological biomarker of tauopathy. Only patients with pure Lewy body pathology were included in the DLB group, i.e., patients with DLB criteria but who did not fulfill the criteria for AD pathology.
Inclusion in the HC group of the AlphaLewyMA cohort was proposed to healthy volunteers without cognitive complaint. HC subjects were found via listing of controls of Strasbourg University Hospital's clinical investigation center or among patients’ relatives. HC subjects were matched to DLB patients on age and educational level.
Exclusion criteria for both groups included contraindications to MRI, evidence for psychiatric or alternative neurological explanation for cognitive impairment (for DLB group only), or non-stabilized or severe medical condition.
We retrospectively screened all DLB patients and HC subjects in the AlphaLewyMA cohort for eligibility. Inclusion in the final analysis required a Mini-Mental State Examination (MMSE) score of at least 20/30, to avoid test failures being due to comprehension difficulties related to global cognitive impairment, rather than to specific impairment of neurovisual functions. Inclusion in the final analysis also required a 3D brain MRI with sufficient image quality, no missing data at the 6 VOSP subtests, and a delay between MRI and neuropsychological testing of less than two years.
Variables
At the inclusion visit, clinical data were collected, including demographics, medical history, concomitant medication and physical examination. A three-dimensional high-resolution brain MRI was acquired for each DLB patient and HC subject at inclusion. Neuropsychological examinations were performed periodically at prespecified follow-up visits.
Data sources/measurement
Parkinsonism was assessed using the Movement Disorder Society Unified Parkinson's Disease Rating Scale (MDS-UPDRS part 3) 16 and was defined by at least one spontaneous feature of bradykinesia, rigidity or rest tremor. The 4-item Mayo Clinic Fluctuation Scale 17 was used to assess fluctuations. We evaluated hallucinations using the Parkinson's Disease-Associated Psychotic Symptoms Questionnaire. 18 Clinical rapid eye movement sleep behavior disorder (RBD) was identified using the Stavanger Sleep Questionnaire. 19 Orthostatic hypotension was diagnosed if the subject's blood pressure dropped by at least 20 mmHg (systolic) or 10 mmHg (diastolic) within 3 min of orthostatism. Other neurovegetative phenomena were determined using semi-quantitative questionnaires. Functional independence was evaluated with a simplified version of the Instrumental Activities of Daily Living scale. 20
Assessment of neurovisual abilities
All quantitative variables obtained from neuropsychological testing were managed as continuous variables.
Global cognitive function
Global cognitive function was evaluated using the French version of the MMSE, 21 with a maximal score of 30 and a pathological cutoff of 26.
Visuoperceptual and visuospatial abilities
Visuoperceptual and visuospatial abilities were evaluated using 6 subtests from the VOSP battery. 22 Five percent cutoff scores are derived from the VOSP scoring sheet. The screening subtest (SCR) was used to check participants’ ability to perform the other subtests. We used the incomplete letters subtest (LET) to assess object perception, whereas the dot counting (DOT), position discrimination (POS), number location (LOC) and cube analysis subtests (CUB) were used to assess space perception.
Visuoconstruction
The “copy” condition of the ROCF 23 was used to evaluated visuoconstruction performance. Five percent cutoff scores are derived from the ROCF manual. 24
Neuroimaging study
We used voxel-based morphometry (VBM) to determine the neural correlates of neurovisual performances in DLB patients. We tested the correlations between the gray matter (GM) volume at a voxel level and the scores at the ROCF and at each of the 6 VOSP subtests, mapping the regions of atrophy for these different tests. Each patient underwent a 3 T MRI scan at inclusion (Verio 32-channel Tim Siemens scanner; Siemens, Erlangen, Germany), and 3-dimensional T1-weighted images were used in the VBM analysis (image matrix = 256 × 256, slice thickness = 1 mm, repetition time = 1900 ms, echo time = 2.52 ms, flip angle = 9°). All 3D-T1 images were then pre-processed using MATLAB software with SPM12 and CAT12 toolboxes. Weighted overall image quality rating (IQR) was assessed for each participant's image. We excluded scans with an IQR below 60. Each 3D-T1 image was segmented using SPM12 tissue probability maps and registered in 6 classes: GM, white matter (WM), cerebrospinal fluid (CSF), bones, soft tissues and air. Segmented images were corrected for bias. Spatial registration was performed using geodesic shooting. Individual total intracranial volumes (TIV) were calculated as the sum of GM + WM + CSF and was later used as a covariate to correct for different brain sizes. We checked for sample homogeneity using quadratic mean z-scores of the modulated normalized GM segments before smoothing. We used an 8-mm kernel for smoothing.
Statistical analysis
Behavioral analysis
For descriptive analysis of clinical data, we performed statistical tests according to a frequentist design. The difference between two groups was considered statistically significant if p-value was <0.05. Quantitative variables were compared using a Mann-Whitney test or a Welch's t-test as appropriate. Qualitative variables were compared using Pearson's Chi-squared test or Fisher's exact test. Missing data were considered missing at random. We used pvalue.io online software to perform descriptive statistical analysis.
VBM analysis
We used a general linear model to investigate statistical correlations between local GM volume and scores on visuoperception, visuospatial and visuoconstruction tests. Raw scores of the ROCF and the 6 VOSP subtests were successively tested in the DLB patient group. We used t-contrast to test correlations, considering that decreased raw scores in VOSP and ROCF tests would be associated with decreased GM volumes. We used TIV, age and MMSE as nuisance covariates. Since the inclusion of years of education as a fourth covariate did not meaningfully impact the results, we chose not to incorporate it. We analyzed the results using two different statistical significance levels, either corrected for multiple comparisons using family-wise error (FWE) at p < 0.05, or uncorrected at p < 0.001. We used a cluster extent of 20 voxels. The results were visualized using the xjView toolbox. In a second step, we completed the analyses using a specific mask generated with the NeuroQuery tool 25 and including the control subjects, due to the lack of statistically significant results without controls. The “visual perception” mask was used for the LET and SCR subtests, while the “space perception” mask was used for DOT, LOC, POS, CUB and ROCF. We included age and TIV as covariates in the analyses. We also kept the MMSE as a covariate in these analyses, assuming a continuum between normal and pathological aging.
Results
Participants
Of the 105 DLB patients in the AlphaLewyMA cohort, 94 had available 3D brain MRI. We excluded one patient due to insufficient MRI quality (IQR < 60), 20 patients due to a delay of more than 2 years between brain MRI and neuropsychological tests and three patients due to MMSE <20. The remaining 70 DLB patients were included in the final analysis. Of the 28 HC subjects in the AlphaLewyMA cohort, 24 had available 3D brain MRI. We excluded one subject due to a delay of more than 2 years between brain MRI and neuropsychological tests. The remaining 23 HC subjects were included in the analysis.
Descriptive data
We describe participants’ characteristics in Table 1. DLB patients and HC subjects were comparable regarding age, sex, educational level and handedness. Among the DLB group, 59 patients (84%) had fluctuations, 42 (60%) had visual hallucinations, 42 (61%) had RBD, and 52 (74%) presented with at least one spontaneous feature of parkinsonism (p < 0.001 for each criterion versus HC). The mean IADL-4 score was significantly lower in the DLB group versus the HC group (p < 0.01). Of the patients in the DLB group, 24 (34%) were at the dementia stage. History of depression was found in 34 (53%) patients (p < 0.001 versus HC group).
Clinical characteristics of dementia with Lewy bodies patients and healthy control subjects.
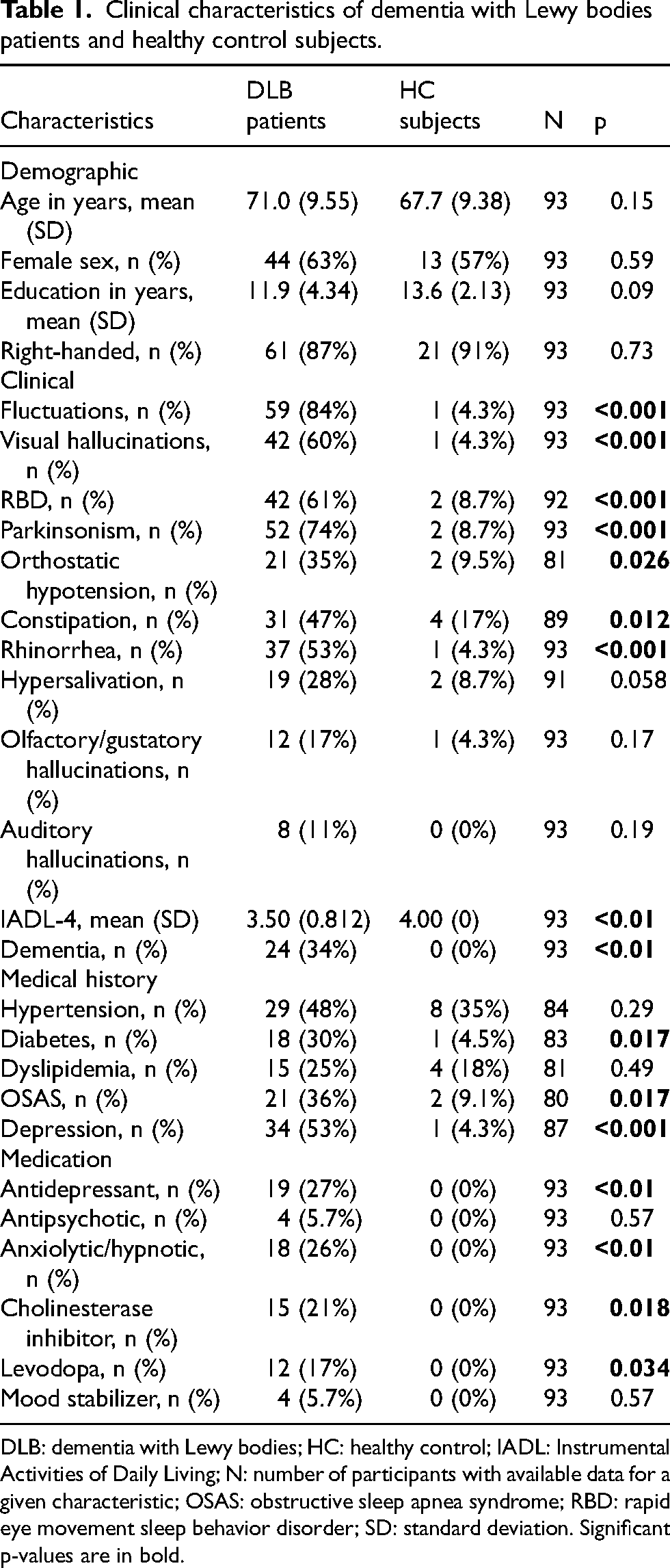
DLB: dementia with Lewy bodies; HC: healthy control; IADL: Instrumental Activities of Daily Living; N: number of participants with available data for a given characteristic; OSAS: obstructive sleep apnea syndrome; RBD: rapid eye movement sleep behavior disorder; SD: standard deviation. Significant p-values are in bold.
Behavioral results
Participants’ scores at neuropsychological tests are reported in Table 2. DLB patients had a significantly lower MMSE score (26.4) compared to HC subjects (29.3) (p < 0.001).
Neuropsychological tests of dementia with Lewy bodies patients and healthy control subjects.
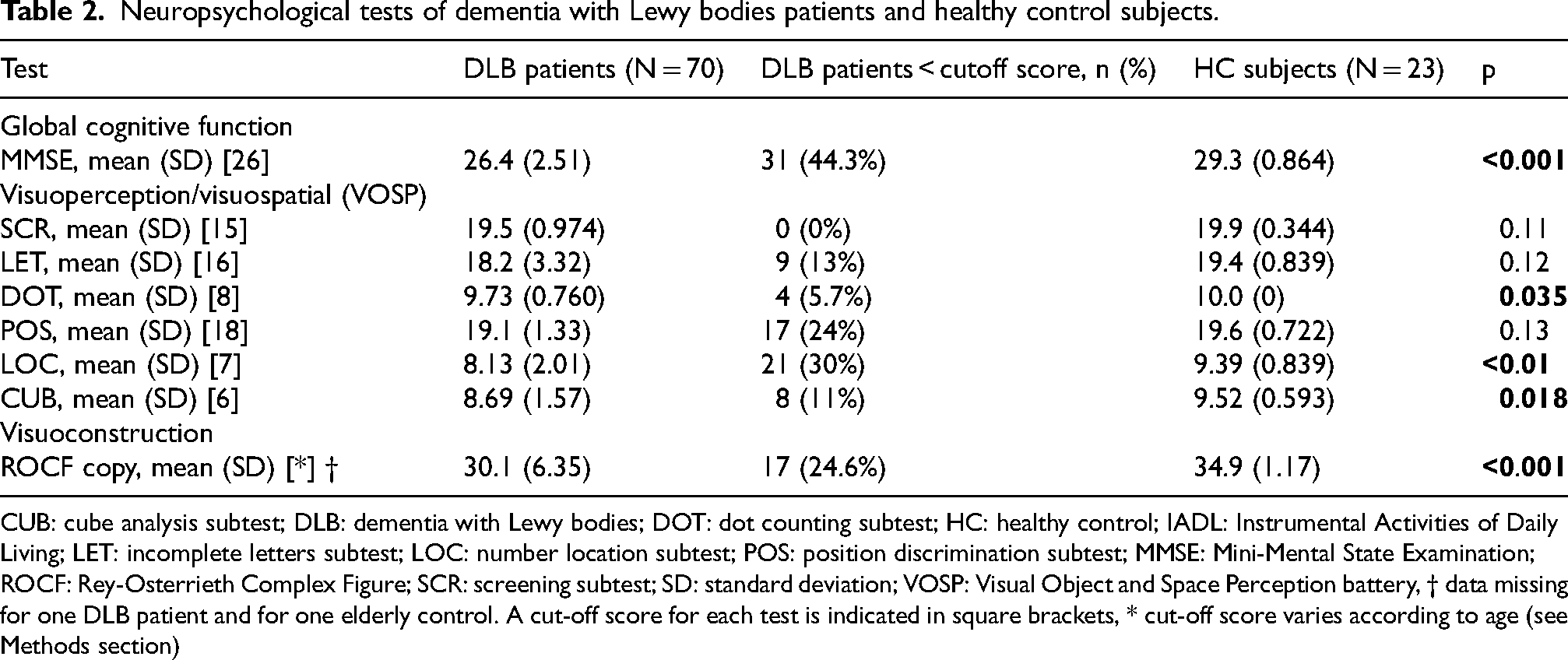
CUB: cube analysis subtest; DLB: dementia with Lewy bodies; DOT: dot counting subtest; HC: healthy control; IADL: Instrumental Activities of Daily Living; LET: incomplete letters subtest; LOC: number location subtest; POS: position discrimination subtest; MMSE: Mini-Mental State Examination; ROCF: Rey-Osterrieth Complex Figure; SCR: screening subtest; SD: standard deviation; VOSP: Visual Object and Space Perception battery, † data missing for one DLB patient and for one elderly control. A cut-off score for each test is indicated in square brackets, * cut-off score varies according to age (see Methods section)
Considering the VOSP, all participants performed over the SCR cutoff score. Performance at the LET was altered in 9 DLB patients, although the difference in mean LET scores was not statistically significant between DLB patients and HC subjects. The performance was significantly lower in the DLB group at three of the space perception subtests, namely DOT, LOC and CUB (p = 0.035, p < 0.01, p = 0.018, respectively). No statistically significant difference was found for the POS.
Regarding the ROCF, copy performance was significantly lower in the DLB group (p < 0.001), with 24.6% of DLB patients scoring below the fifth percentile adjusted for age.
Neuroimaging results
We performed an initial VBM analysis comparing the 70 DLB patients with the 23 HC subjects (t-contrast HC-DLB). Our results showed that DLB patients presented with diffuse atrophy, including the temporal cortex (p < 0.05, FWE corrected), as well as the occipital, parietal and prefrontal cortices (p < 0.001 uncorrected, Supplemental Figure 1).
VOSP
VBM analysis was performed on all 70 DLB patients for each of the 6 VOSP subtests, with no missing data. Our analysis revealed a positive correlation between LET performance and the left cerebellar hemisphere (p < 0.05 FWE, Figure 1A). Positive correlations between LET performance and bilateral occipitotemporal cortex were also found (p < 0.001 uncorrected, Figure 1B and Table 3). For DOT performance, VBM analysis showed a positive correlation with the occipito-parietal cortex, as well as with the left cerebellum (p < 0.001 uncorrected, Figure 2 and Table 4). A significant cluster was obtained in the right fusiform gyrus for LOC, and in the right middle frontal gyrus for POS (p < 0.001 uncorrected for both tests, Supplemental Table 1). Positive correlations were also obtained between SCR performance and bilateral temporal cortex and right cerebellum (p < 0.001 uncorrected, Supplemental Table 1). No cluster emerged for CUB performance at the prespecified statistical thresholds.
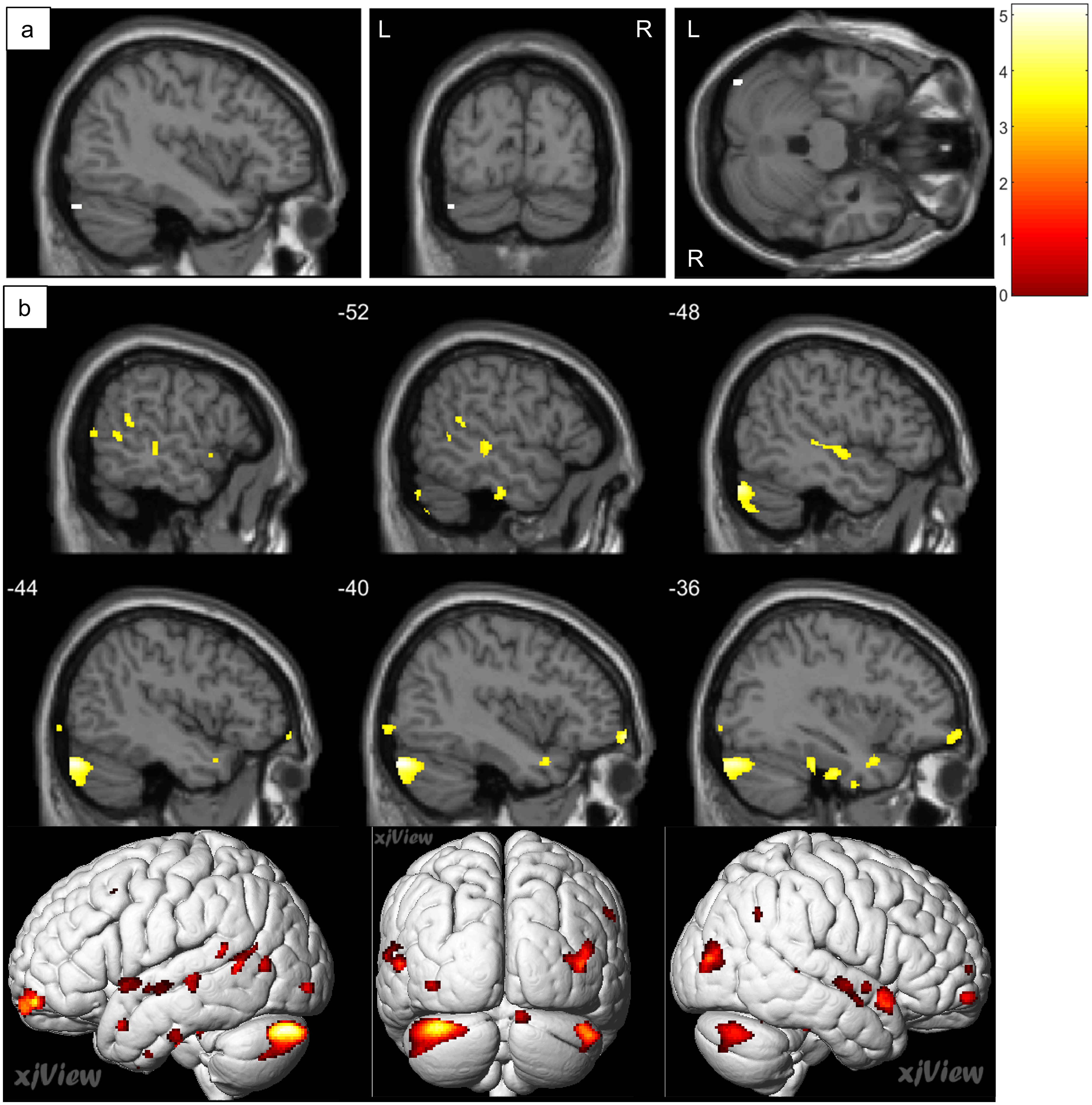
Brain regions correlated with the incomplete letters subtest (LET) in dementia with Lewy bodies patients. Positive correlation was found between LET scores and a cluster in the posterior part of the left cerebellar hemisphere (a) (p < 0.05, family-wise error corrected). Positive correlations were found between LET scores and bilateral occipitotemporal cortex and left cerebellar hemisphere (b) (p < 0.001 uncorrected), using total intracranial volume, Mini-Mental State Examination score, and age as nuisance covariates.
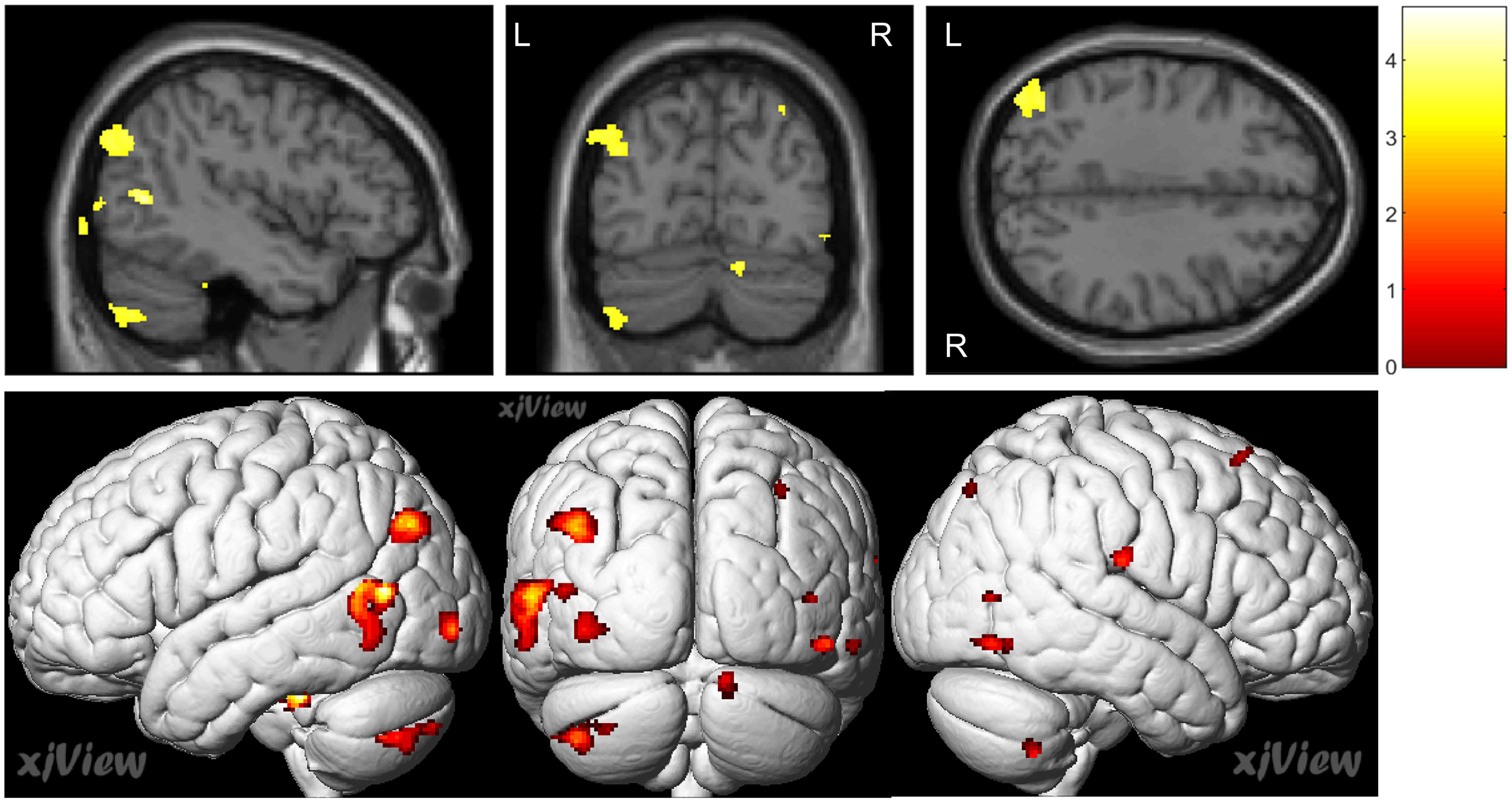
Brain regions correlated with the dot counting subtest (DOT) in dementia with Lewy bodies patients. Positive correlations were found between DOT scores and occipito-parietal cortex and left cerebellar hemisphere (p < 0.001 uncorrected), using total intracranial volume, Mini-Mental State Examination score and age as nuisance covariates.
Brain regions positively correlated with the scores on the incomplete letters subtest (significant at p < 0.05, family-wise error corrected, or p < 0.001, uncorrected) for the dementia with Lewy bodies group, using total intracranial volume, Mini-Mental State Examination score and age as nuisance covariates.
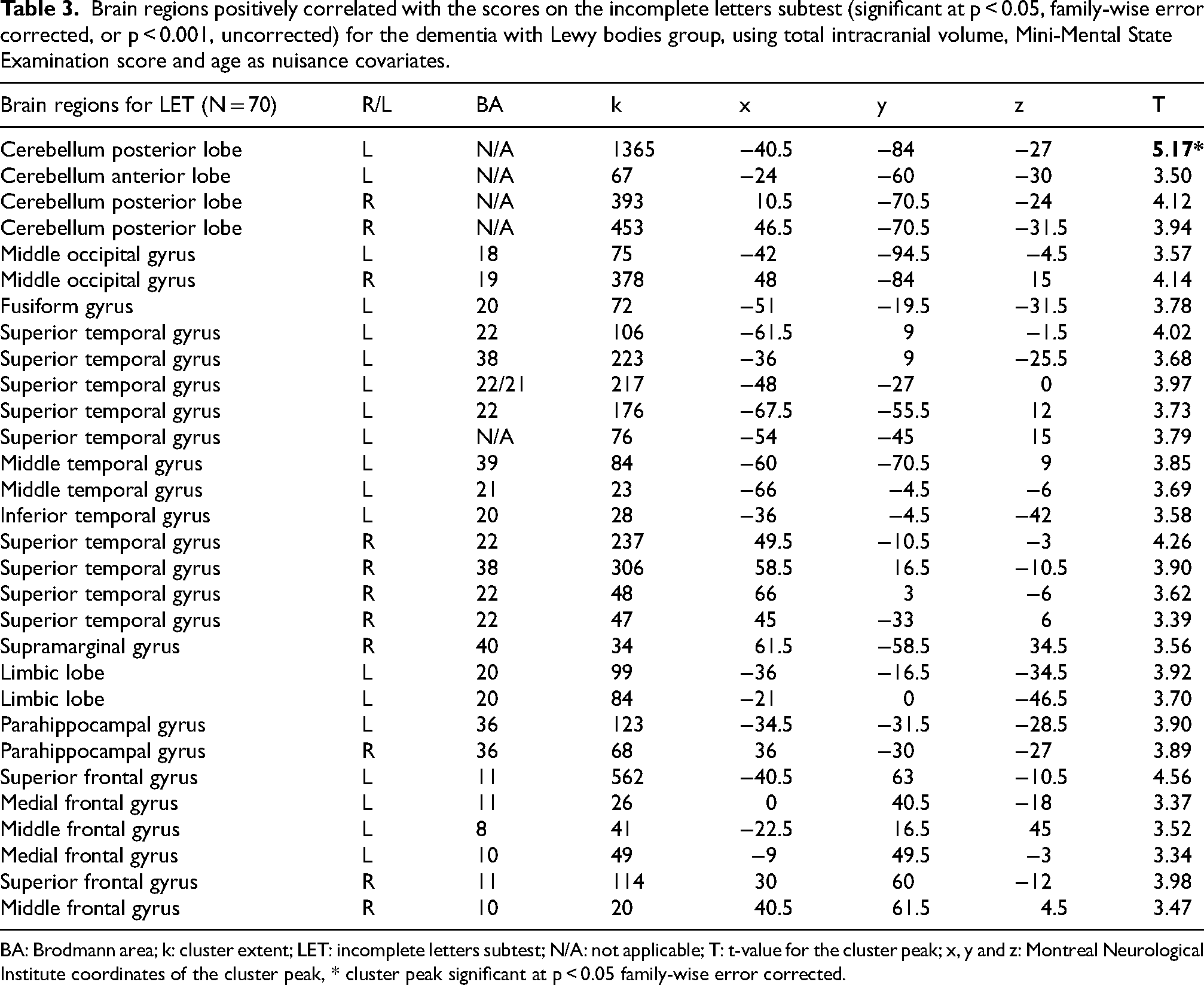
BA: Brodmann area; k: cluster extent; LET: incomplete letters subtest; N/A: not applicable; T: t-value for the cluster peak; x, y and z: Montreal Neurological Institute coordinates of the cluster peak, * cluster peak significant at p < 0.05 family-wise error corrected.
Brain regions positively correlated with the scores on the dot counting subtest (significant at p < 0.001, uncorrected) for the dementia with Lewy bodies group, using total intracranial volume, Mini-Mental State Examination score and age as nuisance covariates.
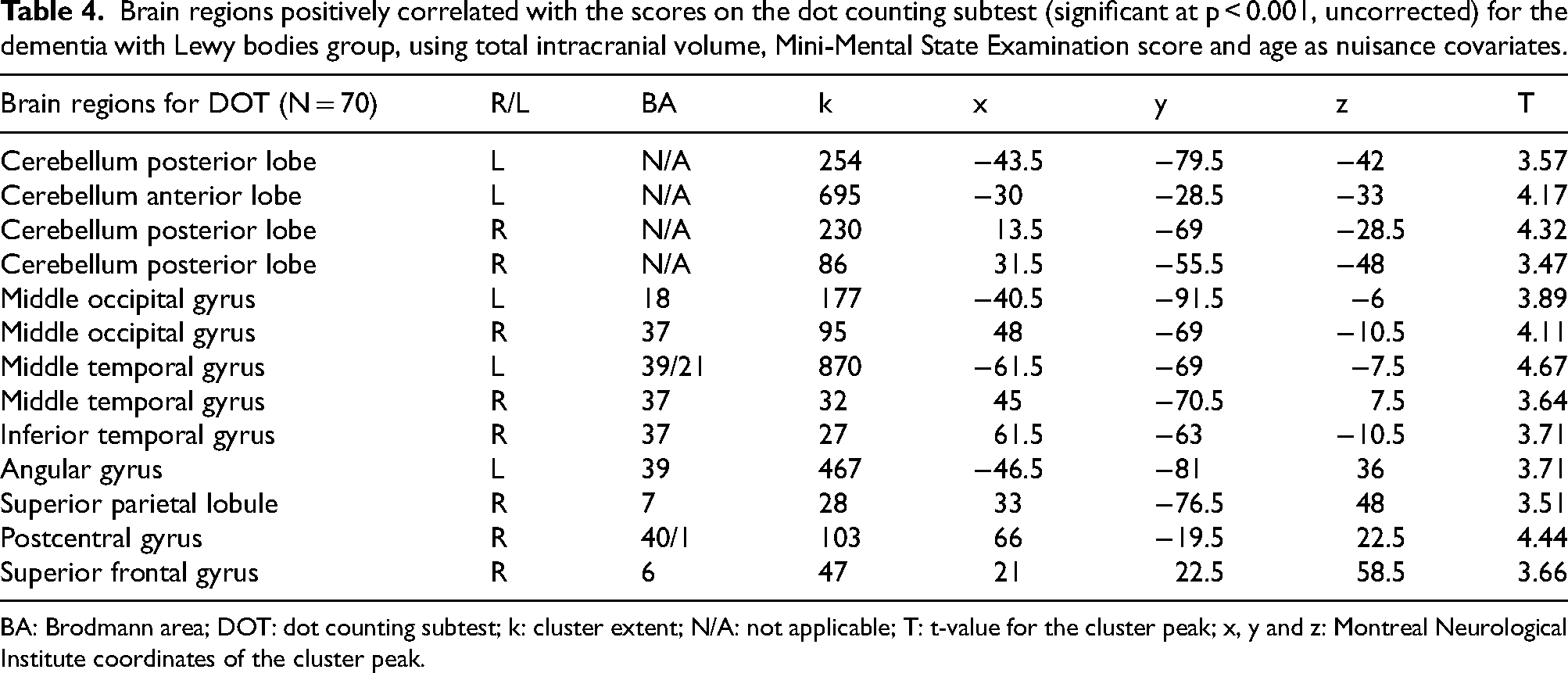
BA: Brodmann area; DOT: dot counting subtest; k: cluster extent; N/A: not applicable; T: t-value for the cluster peak; x, y and z: Montreal Neurological Institute coordinates of the cluster peak.
ROCF
VBM analysis was performed on 69 DLB patients for ROCF, as one patient had missing data. ROCF copy performance was positively correlated with right prefrontal cortex and bilateral parietal cortex (p < 0.001 uncorrected, Figure 3 and Table 5).
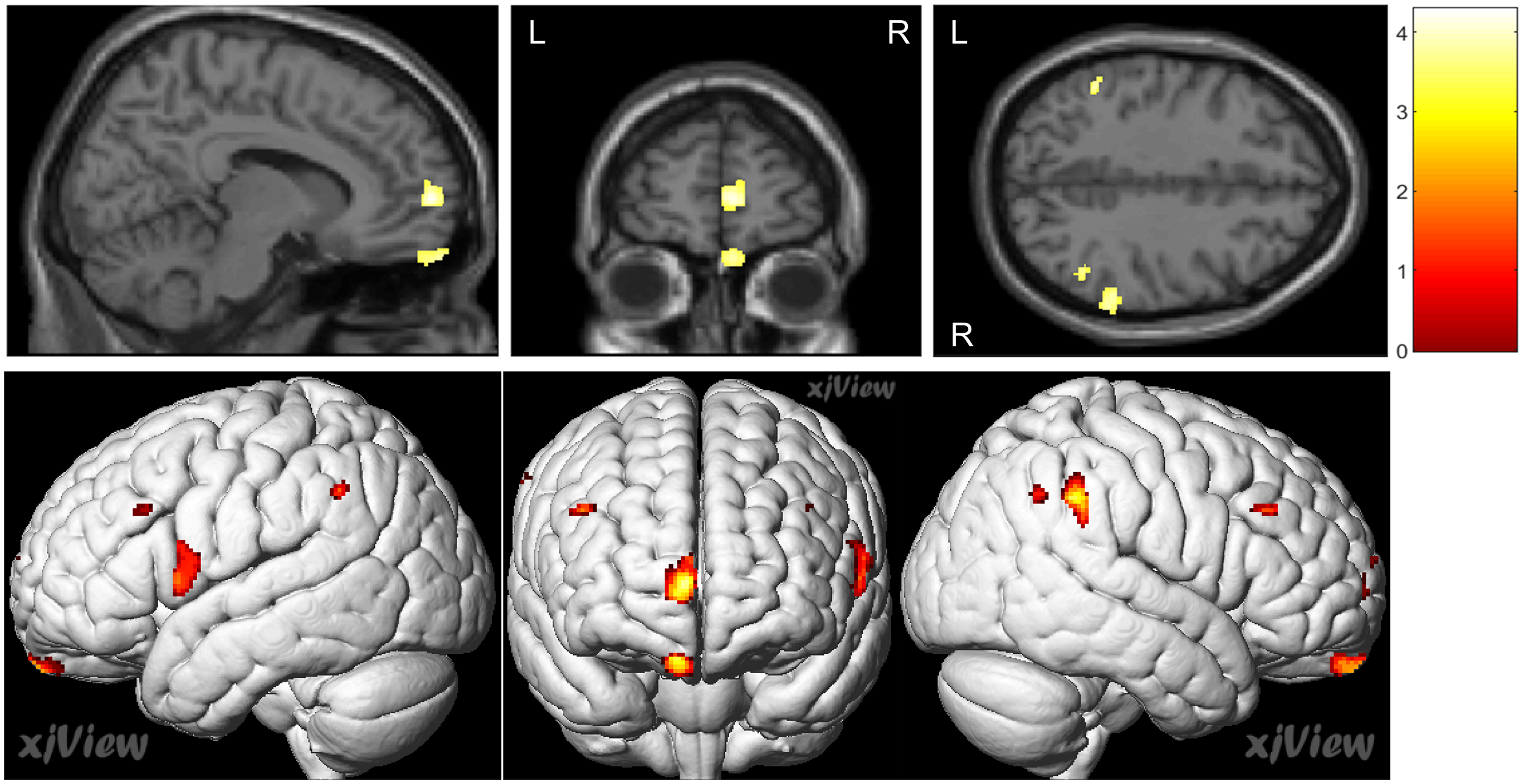
Brain regions correlated with the Rey-Osterrieth Complex Figure (ROCF) copy in dementia with Lewy bodies patients. Positive correlations were found between ROCF copy scores and biparietal and right prefrontal cortex (uncorrected p < 0.001), using total intracranial volume, Mini-Mental State Examination score and age as nuisance covariates.
Brain regions positively correlated with the scores on the Rey-Osterrieth Complex Figure copy (significant at p < 0.001, uncorrected) for the dementia with Lewy bodies group, using total intracranial volume, Mini-Mental State Examination score and age as nuisance covariates.
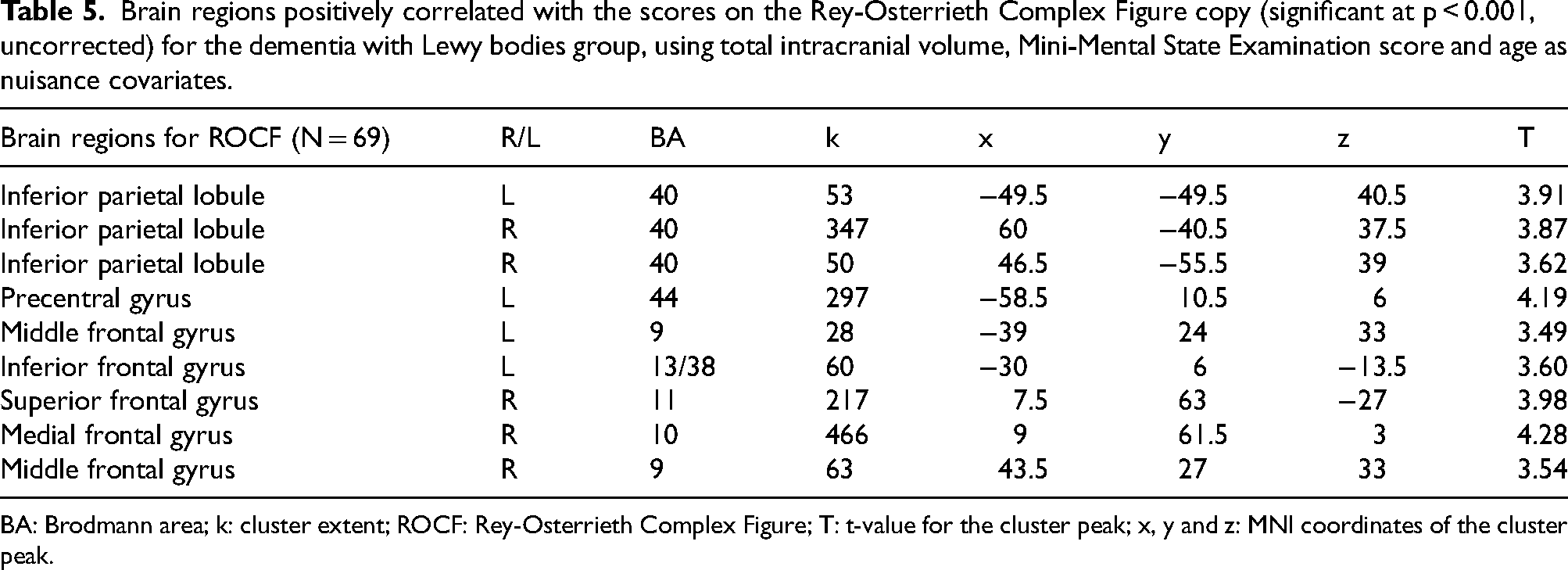
BA: Brodmann area; k: cluster extent; ROCF: Rey-Osterrieth Complex Figure; T: t-value for the cluster peak; x, y and z: MNI coordinates of the cluster peak.
Supplemental analysis
The results of complementary analyses combining patient and control data and using a mask based on functional MRI data (NeuroQuery) are shown in Supplemental Figure 2 and in Supplemental Table 2. For LET performance, the VBM analysis confirmed a positive correlation with bilateral cerebellar hemispheres, as well as occipitotemporal cortex (p < 0.05, false discovery rate corrected). We found a positive correlation between DOT performance and left occipitotemporal cortex (p < 0.001 uncorrected). ROCF performance was positively correlated with right frontoparietal cortex (p < 0.001 uncorrected).
Discussion
We characterized neurovisual impairment in DLB patients compared with control subjects. We sought to correlate these tests with GM atrophy in VBM. In line with our hypotheses, object perception performance (LET) was associated with involvement of the occipitotemporal cortex, corresponding to the “what” associative visual pathway, while performance involving visuospatial skills (DOT, ROCF) was associated with involvement of the occipito-parietal cortex, corresponding to the “where” associative visual pathway. In our research, cerebellar involvement appeared preponderant in object perception (LET, p < 0.05 FWE) and was also associated with visuospatial skills (DOT, p < 0.001 uncorrected), suggesting cerebellar involvement in neurovisual impairment in DLB. Regarding the other tasks, the results obtained with SCR were similar to those observed with LET (temporal cortex and cerebellum), which is consistent with the visuoperceptual nature of the task, even though the SCR subtest was primarily designed as a screening test rather than to evaluate visuoperception. However, no correlation was found with the expected regions of the visual pathway when testing POS and LOC, and no correlation at all was found with the CUB. The results of our supplementary analyses are consistent with our main analysis. The use of control subject data and a neuroimaging mask increased statistical power.
Our behavioral results are consistent with data available in the literature regarding neurovisual disorders in DLB. Concerning visuoperception and visuospatial abilities assessed by VOSP, several studies have shown that DLB patients perform significantly worse than healthy controls.26–28 This difference in comparison with control subjects is more difficult to demonstrate in the prodromal to mild stages, as only a minority of patients obtain scores below the pathological cutoffs. 7 In our study, the LET performance was not impaired overall in the DLB group because mostly prodromal patients were involved. However, there was significant variability in performance within this group, with nine of the patients having pathological scores. Therefore, it is unclear whether these correlations are driven by these nine patients, or if they rather reflect normal process. In terms of visuoconstruction, which is a cognitive hallmark of the disease, DLB patients show pathological results on the ROCF copy task, and their performance is significantly altered compared to controls. 28 In prodromal to mild DLB patients, this difference with controls is less marked, although DLB patients already have pathological z-scores, suggesting weakened visuoconstructive ability. 7 It is worth noting that ROCF copying does not only involve neurovisual processes, but also organizational and planning skills, which could provide a twofold explanation for the impaired performance of DLB patients on this task, as these patients experience impairment in both neurovisual and executive functions. 6
Performance on the LET and SCR was positively correlated with temporal cortex, and also with occipital cortex for the LET. These cortices are part of the visual associative “what” pathway, which is involved in the identification of the characteristics of objects, 10 in line with our hypothesis. In this way, the bilateral middle occipital gyrus stands out significantly for LET, a structure involved in typographic character identification. 29 Although the distribution of temporal clusters was bilateral for LET and SCR, a left predominance could be noted. This is consistent with the fact that letter representation areas are located in the left occipitotemporal cortex. 30 The DOT subtest as well as the ROCF copy correlated positively with the parietal cortex, which is part of the “where” visual associative pathway. 10 It is noteworthy that the parietal clusters for DOT were located in the right hemisphere in our study, which is consistent with data showing right-hemisphere dominance in visuospatial attention in humans. 31 With regard to the ROCF copy, we also found positive correlations with the right inferior parietal lobule, a structure involved in spatiotemporal integration. 32 The left angular gyrus correlated with the DOT subtest, which is likely related to counting, given that the angular gyrus is involved in number processing. 33 The involvement of the premotor cortex and left parietal cortex may account for the praxis required for drawing in the ROCF. 34 In the DOT, the temporal cortex is also involved despite the visuospatial nature of the task. This may reflect the concomitant involvement of visuoperceptual processes. In contrast to our assumptions, we did not find any involvement of associative visual pathways in the POS, LOC and CUB. As these tasks have more complex instructions, they may be disrupted by deficits that are not solely visuospatial. Another explanation for the lack of correlation in VBM for these three subtests could be that our DLB patients are in a mild stage. At this stage, DLB is a functional rather than an atrophic disease, with limited neuronal destruction. 35 The involvement of the prefrontal cortex in ROCF is likely to be of an executive origin, linked to organizational aspects. 36 Finally, the LET, SCR and DOT correlated positively with the cerebellum, which shows substantial connectivity with prefrontal regions, as illustrated by the phenomenon of cognitive dysmetria. 37
Our results are in line with those of other studies pointing out the involvement of the cerebellum in perceptual processes. A consensus paper suggested that the role of the cerebellum goes beyond the sole control and coordination of movements, and that it is involved in the control of several sensory processes. 38 The cerebellum acts as an anatomical relay between visual and motor cortical areas, modulating guidance to movement directed at a visual stimulus, and is thus part of the dorsal “where” pathway. 39 Hence, data from studies of patients with cerebellar lesions suggest that the cerebellum is involved in the processing of visual movement information. 40 MRI functional data have shown activation of particular regions of the cerebellum during visuospatial tasks that involved determining the direction of a stimulus in the presence of visual noise. 41 In a functional MRI study in healthy volunteers, the perception of configuration changes during a visuospatial task was correlated with activation of the left cerebellum and hippocampus. 42 However, there is less evidence that the cerebellum could be involved in the ventral “what” pathway. 38 A functional MRI study showed strong resting-state connectivity between lobules 1–6 and the vermis on the one hand, and the cerebral visual network on the other. 43 Other functional MRI data from patients with Parkinson's disease (PD) tested using the Montreal Cognitive Assessment showed a correlation between lobule VII of the cerebellum and visuospatial/executive and attentional networks. 44 A VBM study also showed correlations between the cerebellum and visual hallucinations in patients with PD. 45 These data suggest the involvement of cerebellar lobule VIII and Crus 1, which are associated with the dorsal attention network 46 and cortical visual processing, 47 respectively. Thus, we hypothesize that in our results, the cerebellum could be involved in two different ways, depending on the neurovisual process engaged. For the spatial perception task (DOT), the cerebellum would be involved as a modulator of the dorsal “where” pathway. In the object perception task (LET), the cerebellum would allocate cognitive resources and promote visual attention. The involvement of the cerebellum in DLB does not appear to be restricted to visuoperceptive functions. A recent VBM study in DLB patients suggested the involvement of the left cerebellum in the Digit Symbol Substitution Test, a task involving both visuoperceptual and attentional processes. 48 Cerebellar atrophy was already highlighted in a VBM study of global atrophy in DLB. 49 These imaging findings appear to be supported by pathological data, as pathological alpha-synuclein was reported in Purkinje cell axons from DLB and PD patients. 50
Our study has some limitations. As our analysis was cross-sectional, the temporal relationship between GM loss and the onset of neurovisual symptoms is unknown. The causal nature of the cerebellum's role in visual perception is therefore hypothetical. As the diagnosis of DLB is based on clinical criteria, not all our patients had a FP-CIT SPECT performed, leading to discussion of a possible diagnostic bias. However, formal clinical criteria suffer from a lack of sensitivity but are highly specific. Our DLB patients had to fulfill the 2005 diagnostic criteria, which are more stringent than the new 2017 criteria, intended to be more sensitive. Thus, a clinical diagnosis of DLB is considered 98% accurate. 51 In addition, our diagnoses were confirmed by longitudinal follow-up for up to 10 years in the AlphaLewyMA cohort. We chose to add healthy controls in order to improve the contrast between subjects with normal performance and patients. Nevertheless, we believe that the correlation between performance and brain volume is related to specific alterations in the neurovisual pathways of DLB patients. Highlighting the visual pathways in normal aging would have required a substantially larger sample size. 52 The “what” and “where” pathways did not significantly emerge after FWE correction. This may have been due to limited atrophy in prodromal to mild DLB. Functional MRI studies might have shown more significant correlations. Although we had an a priori hypothesis, we chose to perform whole-brain VBM to avoid restricting the analysis to regions known to be involved in neurovisual pathways. This design may have resulted in a lack of statistical power. The use of masks in complementary analyses improved the power of the study, but did not allow more clusters to reach the significance threshold after FWE correction. A region of interest analysis should be done as a complementary study. Our VOSP subtests battery was comprehensive for the space perception aspect, but we only had one test designed for object perception (LET). Indeed, the silhouette, progressive silhouette and object decision subtests 22 were not part of the AlphaLewyMA protocol. It would be interesting to carry out further neuroimaging studies on these subtests to assess whether the obtained results would be similar to those for LET.
In conclusion, our study investigated the anatomical correlates of neurovisual impairment in DLB patients using VBM and neuropsychological tests widely adopted in clinical practice. This paper suggests an involvement of the cerebellum in the neurovisual deficits of DLB alongside other regions classically involved in visuoperceptive functions, such as the occipito-temporal ventral and occipito-parietal dorsal pathways. Our study is limited by the inclusion of patients at prodromal to mild stages who ultimately had little neurovisual impairment, and our results remain exploratory. However, this study highlights the processes involved in early neurovisual impairment in DLB and could be complemented by functional MRI analysis to better characterize the involvement of the cerebellum in visuoperceptive processes in DLB patients.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251389634 - Supplemental material for Neural correlates of neurovisual deficits in prodromal and mild dementia with Lewy bodies: A voxel-based morphometry study
Supplemental material, sj-docx-1-alz-10.1177_13872877251389634 for Neural correlates of neurovisual deficits in prodromal and mild dementia with Lewy bodies: A voxel-based morphometry study by Augustin Moreau, Alice Tisserand, Léa Sanna, Anne Botzung, Frédéric Blanc and Nathalie Philippi in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors are grateful to the patients, their caregivers and the healthy controls who participated in this study. The authors thank all the professionals involved in the recruitment and assessment of the patients. The authors thank Nick Barton for language editing.
Ethical considerations
This study was carried out within the scope of the AlphaLewyMA cohort (NCT01876459, 2013), was in accordance with the 1964 Helsinki Declaration and its later amendments and was approved by the Ethics Committee of East France (IV).
Consent to participate
Written informed consent was obtained from the patients and controls prior to their inclusion in the study.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was performed using data from the AlphaLewyMA cohort (![]() ), which received public grants from an interregional clinical research hospital project (PHRC) (IDRCB 2012-A00992-41).
), which received public grants from an interregional clinical research hospital project (PHRC) (IDRCB 2012-A00992-41).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Anonymized data not provided in the article because of space limitations will be made available by request from any qualified investigator for purposes of replicating procedures and results.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.