
Abstract
Sex differences in dementia with Lewy bodies (DLB) remain understudied despite growing evidence in neurodegenerative diseases. In this retrospective multicentric study of 310 patients with probable DLB, we assessed whether sex-related clinical differences could be explained by Alzheimer's disease (AD) cerebrospinal fluid biomarkers. While, in univariate analysis, females had lower Mini-Mental State Examination (MMSE) scores and more frequent AD profiles, males presented more REM sleep disorders. Adjusting for AD biomarkers attenuated some differences (REM sleep disorder, MMSE), but not all like parkinsonism. These findings suggest that AD co-pathology partly contributes to sex differences in DLB, but additional mechanisms likely underlie the observed clinical variability.
Introduction
In this short report, we describe how sex-difference impacts symptoms in dementia with Lewy bodies (DLB). DLB is the second most prevalent cause of neurodegenerative cognitive disease; however, it is still under-diagnosed and under-explored, probably due to the high variability of its symptoms. Neuropathologically, DLB is characterized by neuronal inclusions of phosphorylated α-synuclein with varying distribution patterns and can be associated with Alzheimer's disease (AD) pathology (amyloid plaques and neurofibrillary tangles).1–4 This neuropathological variability as well as clinical comorbidities are considered as important factors of the clinical heterogeneity. However, while sex difference is increasingly explored in many neurodegenerative diseases, 5 sex differences remain surprisingly poorly explored in DLB. 2 In this context, taking advantage of our large multicentric DLB cohort from daily clinical practice, our aim was to evaluate the impact of the sex in the variability of the DLB phenotype.
Methods
Detailed methods have already been described in Aveneau et al. 1 All data were collected retrospectively from 2006 to 2021 from daily clinical practice in four centers (Expert Memory Centre Lariboisière Paris and Rouen, Expert Parkinson Center Avicenne Hospital, and the Rothschild Foundation Paris). The diagnosis of probable DLB was made according to the McKeith's 2017 revised criteria for dementia stage and 2020 for MCI stage. When the diagnosis was made before 2017, the diagnosis has been revised to according to the new criteria 1. Some patients had cerebrospinal fluid (CSF) biomarkers analysis for AD and were classified according to their profile (as a categorical variable, A + T+, A + T-, A-T+, A-T-). The cut-offs for determining abnormality were < 860 pg/mL for Aβ42, > 12 for the Aβ40/Aβ42 ratio, and > 22 pg/mL for pTau181 using the Elecsys® immunoassays.
We used Wilcoxon and chi-square models for univariate analysis to examine and compare the clinical characteristics of patients. We conducted separate binary logistic regression analyses for each cardinal symptom—REM sleep behavior disorder, cognitive fluctuations, visual hallucinations, and parkinsonian syndrome—as dichotomous outcomes variables, with age at diagnosis, follow-up duration (because of the difference between male and female), sex and CSF biomarker profile (categorized according to [specify, e.g., A+/T+/N + classification]) as predictors. For the Mini-Mental State Examination (MMSE) score, treated as a continuous outcome, we performed a linear regression analysis including the same predictors. The CSF biomarker profile was operationalized as a binary categorical variable, contrasting A + T + individuals with all other AT(N) profiles (i.e., A + T−, A−T−, and A−T+), according to the AT(N) classification framework. Interaction effects were evaluated for each clinical outcome by including terms in logistic regression models to test whether the association of age or amyloid biomarker status with the outcome differed according to sex. Only participants with non-missing values for all variables involved in the interaction were included in the analyses. A p-value less than 0.05 (two-tailed) was considered statistically significant. We performed analyses and generated graphics using R studio (version 4.3.2).
Results
We analyzed 310 patients (210 male and 100 female). The main characteristics of the population are summarized in Table 1. The mean age of DLB onset and diagnosis were significantly later in female than male (respectively 71.2 versus 69.2-year-old (yo), p = 0.04, 75.05 versus 72.80 yo, p = 0.01) with no significant difference in the time to diagnosis. There was no difference in terms of age at diagnosis or sex between patients with and without AD CSF biomarkers (data not shown). The average follow-up duration was 11.8 years for male and 5.9 years for female. This apparent difference is not statistically significant (p = 0.18). Using a univariate model, we observed that male had more REM sleep disorders than females did (55.9% versus 76.3%, p = 0.005) and female had lower MMSE than male (21.6 versus 20.2 p = 0.04). Concerning AD CSF biomarkers, at comparable age, females displayed more frequently AD biological CSF profile (A + T+) than male (p = 0.02).
Patient sample characteristics.
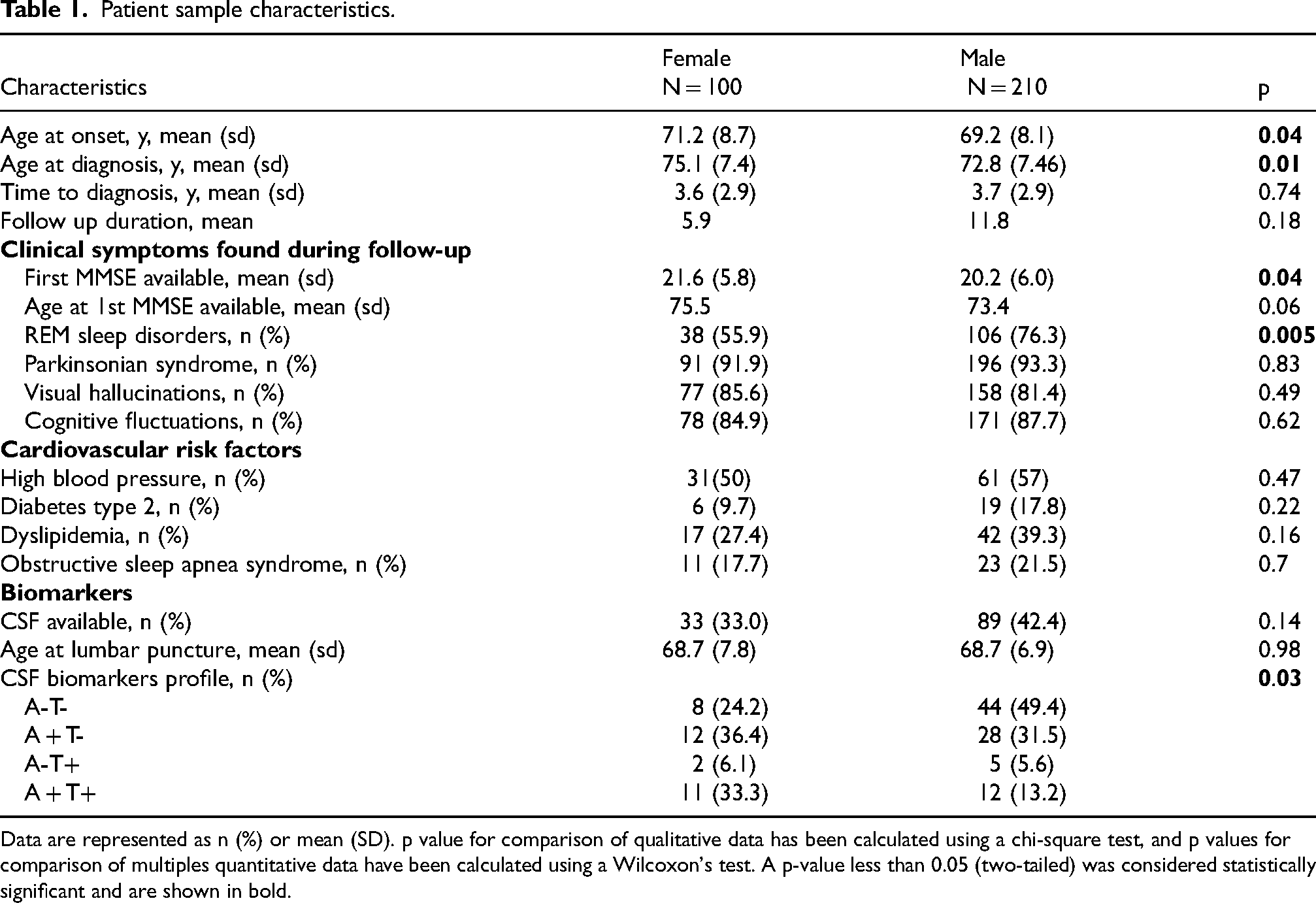
Data are represented as n (%) or mean (SD). p value for comparison of qualitative data has been calculated using a chi-square test, and p values for comparison of multiples quantitative data have been calculated using a Wilcoxon's test. A p-value less than 0.05 (two-tailed) was considered statistically significant and are shown in bold.
Given the unequal distribution of AD CSF biomarker profiles between sexes, we used a multivariate model adjusted for sex, age at diagnosis, follow up duration and CSF AD biomarker status (A + T+, when available) to assess whether sex-related differences in clinical presentation remained significant. After adjustment, sex differences in the frequency of REM sleep disorders and MMSE between sexes were no longer significant, and we observed that males were more likely than females to present with parkinsonian syndromes (OR = 6.35, p = 0.043). No other significant clinical differences were observed. No significant interaction between sex and amyloid biomarker status or age was observed.
Discussion
In this study exploring a deeply phenotyped DLB cohort including CSF biomarkers, we observed a few sex differences in DLB clinical and biological phenotype. First, this has no impact on the time to diagnosis in our cohort between male and female), even though DLB onset and diagnosis occur significantly later in females. These results differ from some previous studies that reported a longer diagnostic delay in women, 5 which could be explained by the exclusive inclusion of tertiary expert centers, where atypical presentations may be more frequently recognized and diagnosed leading to a probable lower rate of misdiagnosis DLB female patients. Regarding the main clinical symptoms, results show that males have significantly more REM sleep disorders than females and females lower MMSE and more AD profile, than male in univariate analysis. After adjustment for lumbar puncture data, sex, age and follow-up duration, this significance disappears. Furthermore, we observe that males have more parkinsonian syndrome than female, which was not described in univariate analysis.
To first compare our univariate analysis, Chiu et al. 2 reported in a wide review, earlier occurrences of visual hallucinations in females, even though this is not found in a serious study with autopsy. 6 They also reported identical results like older onset in females, more REM sleep disorders and parkinsonism in male, with a large consensus.6–8
Furthermore, previous work has shown that both AD biomarkers and sex can influence the DLB phenotype.3,4 Both studies examined AD biomarkers and sex separately, without exploring their combined effects on the DLB phenotype.
In contrast, our study investigated sex-related clinical differences across the whole DLB cohort simultaneously adjusting for CSF biomarkers. This helped us see how sex and AD biomarkers each affect clinical outcomes. While adjusting for biomarkers did modify the interpretation of sex differences highlighting the importance of accounting for co-pathologies, our results do not entirely support the idea that co-pathology alone explains these differences. Indeed, CSF biomarkers (A + T+) influenced the frequency of REM sleep disorders and MMSE scores, but parkinsonian syndrome persisted after adjustment, suggesting that additional factors contribute to the clinical variability. Overall, these findings extend previous observations by providing a more nuanced understanding of sex-related heterogeneity in DLB.
Based on daily clinical practice including retrospective data collection is a potential source of bias. Some patients had a delay between CSF biomarkers analyze and the diagnosis then we cannot rule out the emergence of an amyloid co-pathology in some patients during this period. The reduced sample size in the biomarker sub-analysis may have limited the statistical power to confirm sex differences in REM sleep disorders after adjustment. Furthermore, the result about MMSE must be interpreted with caution because of the time elapsed between the onset of symptoms and the first MMSE available, which is highly variable (up to ten years).
To provide further explanations of these differences, a large prospective cohort including all biomarkers (AD biomarkers, neurofilament light chain, alpha-synuclein) should be conducted to improve phenotyping and help define target populations for new therapeutic strategies. Additionally, the use of a pre-clinical model to study these differences would be particularly valuable in understanding the pathophysiological mechanisms underlying this sex difference.
Footnotes
Acknowledgements
The authors thank all patients and their families.
Ethical considerations
The study was approved by local ethics committees of all participating centers.
Consent to participate
Patients provided informed consent for data use.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.