
Abstract
Background
Metformin has been proposed to have neuroprotective benefits, but its effects on AD-related brain changes remain unclear and may be influenced by apolipoprotein E ε4 (APOE4) genotype, a major genetic risk factor for AD.
Objective
To examine the association between metformin use and in vivo AD pathologies and to evaluate whether APOE4 status moderates these associations in older adults with type 2 diabetes mellitus (T2DM).
Methods
This cross-sectional study used baseline data from 76 non-demented older adults with T2DM (aged 55–90 years), who were enrolled in the Korean Brain Aging Study for Early Diagnosis and Prediction of Alzheimer's Disease (KBASE). The participants underwent comprehensive clinical and neuropsychological assessment and multimodal neuroimaging, including global amyloid- β (Aβ) retention ([11C] PiB-PET), inferior temporal tau deposition ([18F] AV-1451 PET), AD-signature cortical thickness (AD-CT), and white matter hyperintensity (WMH) volume. Global cognition was assessed using the Consortium to Establish a Registry for Alzheimer's Disease (CERAD) neuropsychological battery.
Results
Among 76 participants, 55 (72%) were metformin users and 21 (28%) were non-users. Metformin use was significantly associated with greater AD-CT, but not with Aβ, tau, or WMH volume. A significant interaction between metformin use and APOE4 status was observed with respect to AD-CT. In APOE4-stratified analyses, metformin use was significantly associated with greater AD-CT and better global cognition among APOE4 non-carriers, but not among carriers.
Conclusions
Our findings indicate that metformin use is associated with greater AD-CT—independently of amyloid or tau pathology—particularly among APOE4 non-carriers, and this structural preservation is accompanied by better cognitive outcomes.
Introduction
Type 2 diabetes mellitus (T2DM) has been associated with an increased risk of overall dementia and Alzheimer's disease (AD).1,2 T2DM typically presents with gradual onset and a longer duration, exposing individuals to prolonged hyperglycemia and metabolic abnormalities that may increase their risk of AD and related cognitive decline.2,3 Accumulating evidence also indicates that AD and T2DM share numerous pathophysiological mechanisms, including oxidative stress, impaired insulin signaling, mitochondrial dysfunction, neuroinflammation, and metabolic syndrome. 4
Metformin, an insulin-sensitizing biguanide agent, stands as the most prescribed first-line drug for glycemic control in T2DM. 5 In recent years, several epidemiological and clinical studies have demonstrated that metformin use is associated with a reduced risk of all-cause dementia or AD dementia beyond its anti-diabetic effect,6–9 while some studies did not find such an association.10,11
However, the pathological mechanisms underlying the association between metformin use and reduced AD or overall dementia risk are not yet clearly understood. Several preclinical studies have reported that metformin regulates or inhibits inflammation, oxidative stress, and cell death pathways in the brain, contributing to neuroprotection.12–17 Regarding AD-specific proteins, some animal studies reported that metformin attenuates amyloid- β (Aβ) 18 and tau pathology,18,19 while others showed that metformin even facilitates the generation of Aβ.20,21 A series of human clinical studies also investigated the association between metformin use and in vivo brain changes using neuroimaging or fluid biomarkers, resulting in controversial findings: Although one study showed an association between metformin use and relatively preserved brain structure, 22 others did not find such a positive association 23 or even reported the association between metformin use and more atrophy in AD-related brain regions. 24 In addition to AD-specific pathologies, white matter hyperintensities (WMH)—a marker of cerebrovascular burden commonly observed in older adults with T2DM 25 —frequently co-occur with AD pathology and contribute to AD-related cognitive decline. 26 While one study suggested that long-term metformin use may reduce overall cerebral small vessel disease burden, direct evidence focusing on WMH volume as an outcome is still limited. 27 While a limited number of studies have explored the association between metformin and Aβ or tau measured by fluid biomarkers,23,28,29 no study has examined the relationship using PET imaging for Aβ or tau deposition in the brain yet.
Interestingly, recent evidence suggests that genetic factors, particularly apolipoprotein E ε4 (APOE4) status, may influence metformin's neuroprotective effects. Wu et al. 30 reported that metformin use was associated with memory preservation only in APOE4 non-carriers, while no benefit was observed in APOE4 carriers. Moreover, in the same study, among individuals with established AD dementia, metformin use was paradoxically associated with faster memory decline in the APOE4-positive group. Taken together, these findings suggest that the relationship between metformin use and AD-related brain changes may be modulated by genetic factors, particularly the presence of the APOE4 allele.
In light of this, we investigated the relationship between metformin use and in vivo AD pathologies- including Aβ deposition, tau deposition, AD-related neurodegeneration, and white matter changes-measured by multi-modal neuroimaging modalities, in non-demented older adults with T2DM, focusing primarily on the moderating effect of the APOE4 allele on this relationship.
Methods
Participants
This study was part of the Korean Brain Aging Study for the Early Diagnosis and Prediction of Alzheimer's Disease (KBASE), which was initiated in 2014 and aimed to explore new biomarkers for AD, and to examine the impact of a range of life experiences and bodily changes on the brain in relation to AD. 31 Participants were recruited through four recruitment sites (two public centers for dementia prevention and memory clinics at two university hospitals) in Seoul, South Korea. 31 For this study, we included 76 older adults (aged 55–90 years) with T2DM who had no diagnosis of dementia, including 48 cognitively normal (CN) individuals and 28 with amnestic mild cognitive impairment (MCI). CN participants were individuals with a global Clinical Dementia Rating (CDR) score of 0 and without a diagnosis of MCI or dementia. All participants with MCI met the current consensus criteria for amnestic MCI 32 : 1) a memory complaint confirmed by an informant; 2) objective memory impairment; 3) preserved global cognitive function; 4) independence in functional activities; and 5) absence of dementia. The exclusion criteria were as follows: 1) presence of major psychiatric illnesses, including schizophrenia, major depressive disorder, bipolar disorder, and alcohol-related disorders; 2) significant neurological or general medical conditions or diseases that could affect mental function; 3) illiteracy; 4) the presence of significant visual/hearing difficulties and/or severe communication or behavioral problems that would make clinical examinations or brain scans difficult; and 5) current use of an investigational drug. The study protocol was approved by the Institutional Review Boards of Seoul National University Hospital (C-1401-027-547) and SNU-SMG Boramae Center (26-2015-60), both located in Seoul, South Korea. The study was conducted in accordance with the recommendations of the latest version of the Declaration of Helsinki. All subjects provided written informed consent.
Clinical and neuropsychological assessment
All participants underwent standardized clinical assessments by trained psychiatrists using the KBASE clinical assessment protocol, which incorporated the Korean version of the Consortium to Establish a Registry for Alzheimer's Disease assessment packet (CERAD-K).32,33 All participants were systematically assessed for T2DM and other vascular risk factors (VRFs) (e.g., hypertension, dyslipidemia, coronary heart disease, transient ischemic attack, and stroke) based on data collected by trained nurses during systematic interviews of participants and their reliable informants and a review of medical records. Metformin use was defined as the use of metformin at the baseline evaluation. T2DM was deemed present if participants had been diagnosed at a clinic or were taking anti-diabetic medication(s) for T2DM at the time of recruitment. A vascular risk score (VRS) reflecting the vascular burden other than T2DM was calculated based on the number of vascular risk factors excluding T2DM. 34
All participants also received a neuropsychological assessment based on the CERAD neuropsychological battery, which consists of several subsets including verbal fluency (VF), Boston Naming Test (BNT), Mini-Mental State Examination, word list memory (WLM), construction praxis (CP), word list recall (WLR), word list recognition (WLRc), construction recall (CR), Trail Making Test, Part B (TMT-B) and Stroop Color-Word Test (SCWT). The total score (TS) for the CERAD neuropsychological battery was calculated by summing the scores of 6 tests (VF, BNT, WLM, CP, WLR, and WLRc) as proposed by Chandler et al. 35 CR and the TMT were not included because they were not part of the original CERAD battery developed in 1986, and thus were not incorporated into the validated TS. Individual cognitive tests were also grouped into four cognitive domains: memory (WLM, WLR, WLRc, CR), language (BNT), visuospatial function (CP), and executive function (VF, TMT-B and SCWT). Raw scores of each individual test were transformed to z-scores using normative data.32,33 and the summary score for each cognitive domain was the average of the z-scores of component tests (for memory and executive function) or the z-score itself of a single component test (for language and visuospatial function).
Laboratory tests for blood samples
Overnight fasting blood samples were collected in the morning (8–9 a.m.) by venipuncture. Fasting serum insulin level was measured with chemiluminescent immunoassay method (ADVIOA Centaur XP, Siemens, Washington DC, USA). Fasting blood glucose (FBS) level was measured using the glucose hexokinase method. Glycated hemoglobin (HbA1c) was measured using standard protocols (BIO-RAD, Hercules, CA, USA). Homeostasis model assessment (HOMA) was used to estimate insulin resistance (IR). HOMA-IR was calculated with the formula: fasting plasma glucose (mmol/L) times fasting serum insulin (mU/L) divided by 22.5. Genomic DNA was extracted from whole blood, and APOE genotyping was performed as described previously. 36 APOE4 status was coded if at least 1 ε4 allele was present.
Measurement of Aβ deposition
At the time of clinical evaluation, participants underwent simultaneous three-dimensional (3D) [11C] Pittsburgh compound B (PiB)-positron emission tomography (PET) and 3D T1-weighted MRI scans using a 3.0T Biograph mMR (PET-MR) scanner (Siemens; Washington DC, USA). The details of PiB-PET acquisition and preprocessing were previously described. 37 An automatic anatomical labeling algorithm 38 and a region combining method 39 were applied to determine regions of interest (ROIs) to characterize the PiB retention level in the frontal, lateral parietal, posterior cingulate-precuneus, and lateral temporal regions. A global Aβ retention value was the mean standardized uptake value ratio (SUVR) for all voxels of the four ROIs, calculated by dividing the mean uptake value of a reference region.
Measurement of cerebral tau deposition
A subset of subjects (n = 30) underwent [18F] AV-1451 PET scans using a Biograph TruePoint 40 PET/CT scanner (Siemens), on average 2.45 years (SD 0.35) after clinical evaluation and PiB-PET imaging in accordance with the manufacturer's guidelines. The details of AV-1451 PET imaging acquisition and preprocessing were described previously. 37 AV-1451 PET SUVR images based on the mean uptake over 80 min post-injection were normalized by the mean uptake in the inferior cerebellar gray matter, following the published code. We used tau deposition in the inferior temporal (IFT) ROI as a proxy for AD-related neocortical tau deposition, as previously reported. 40 The IFT gyrus is an early site of tau spread into the neocortex during Braak stage III, 41 and an association of this spread from the medial temporal lobe to the neocortex with early cognitive impairment has been reported. 40 We used a size-weighted average of partial volume-corrected SUVR in the IFT ROI for our analyses.
Measurement of AD-related neurodegeneration
For measurement of AD-signature region cortical thickness (AD-CT), all T1 MR images were obtained using the aforementioned PET-MR machine at the time of clinical evaluation The details of MRI acquisition and preprocessing were previously described. 37 The AD-CT was calculated as the average cortical thickness of the AD-signature regions, including the medial temporal (entorhinal and parahippocampal), middle temporal, angular gyri, posterior cingulate, and precuneus.42,43
Measurement of white matter hyperintensities
All participants underwent MRI scans with fluid-attenuated inversion recovery using the aforementioned PET-MR scanner at the time of clinical evaluation. White matter hyperintensities (WMH) volume was quantified using a validated automatic procedure as described previously.44,45 The final WMH volume was extracted in the native space for each participant.
Statistical analysis
To compare metformin users and non-users in terms of the variables in Table 1, group differences in continuous variables were examined using Student t-test, and categorical variables were compared using χ2 tests. Prior to evaluating the moderating effect of the APOE4 allele on the association of metformin use with neuroimaging biomarkers, we conducted exploratory general linear model (GLM) analyses, treating each neuroimaging biomarker as the dependent variable and metformin use as an independent variable (Table 2). Covariates included age, sex, APOE4 status, cognitive status (CN versus MCI), VRS, HbA1c levels, and the use of other classes of diabetes medications. Among four neuroimaging biomarkers (i.e., global Aβ retention, IF tau deposition, AD-CT, and WMH volume), only those with p values < 0.2 in the exploratory GLM analyses were selected for the subsequent interaction analyses. We then conducted GLM analysis using the selected neuroimaging biomarker as the dependent variable, with the metformin use × APOE4 status interaction term and the main effect of metformin use as independent variables, while adjusting for the same covariates (Table 3). Additional subgroup analyses were performed according to APOE4 status to assess the main effects of metformin use on the selected neuroimaging marker in APOE4-positive and APOE4-negative individuals. Bonferroni correction method was applied to account for multiple comparisons, with a significant threshold of p < 0.025 (i.e., 0.05 divided by the number of subgroup analyses = 2). For exploratory purposes, we also investigated the association between metformin use and global cognition in APOE4-positive and APOE4-negative subgroups, additionally adjusting for years of education given its potential influence on cognitive outcome. Additionally, we also explored whether other potential confounders-age, sex, cognitive status, HbA1c, and use of other classes of anti-diabetes medications-moderated the relationship between metformin use and the selected neuroimaging biomarker. To test these interactions, we separately included a two-way interaction term between metformin use and each confounder, along with main effects, in the GLM (Table 4). All analyses were conducted using R statistical software (version 4.3.0; R Foundation for Statistical Computing, Vienna, Austria). Unless otherwise specified, two-tailed p values < 0.05 were considered statistically significant.
Demographic and clinical characteristics of participants by metformin use.
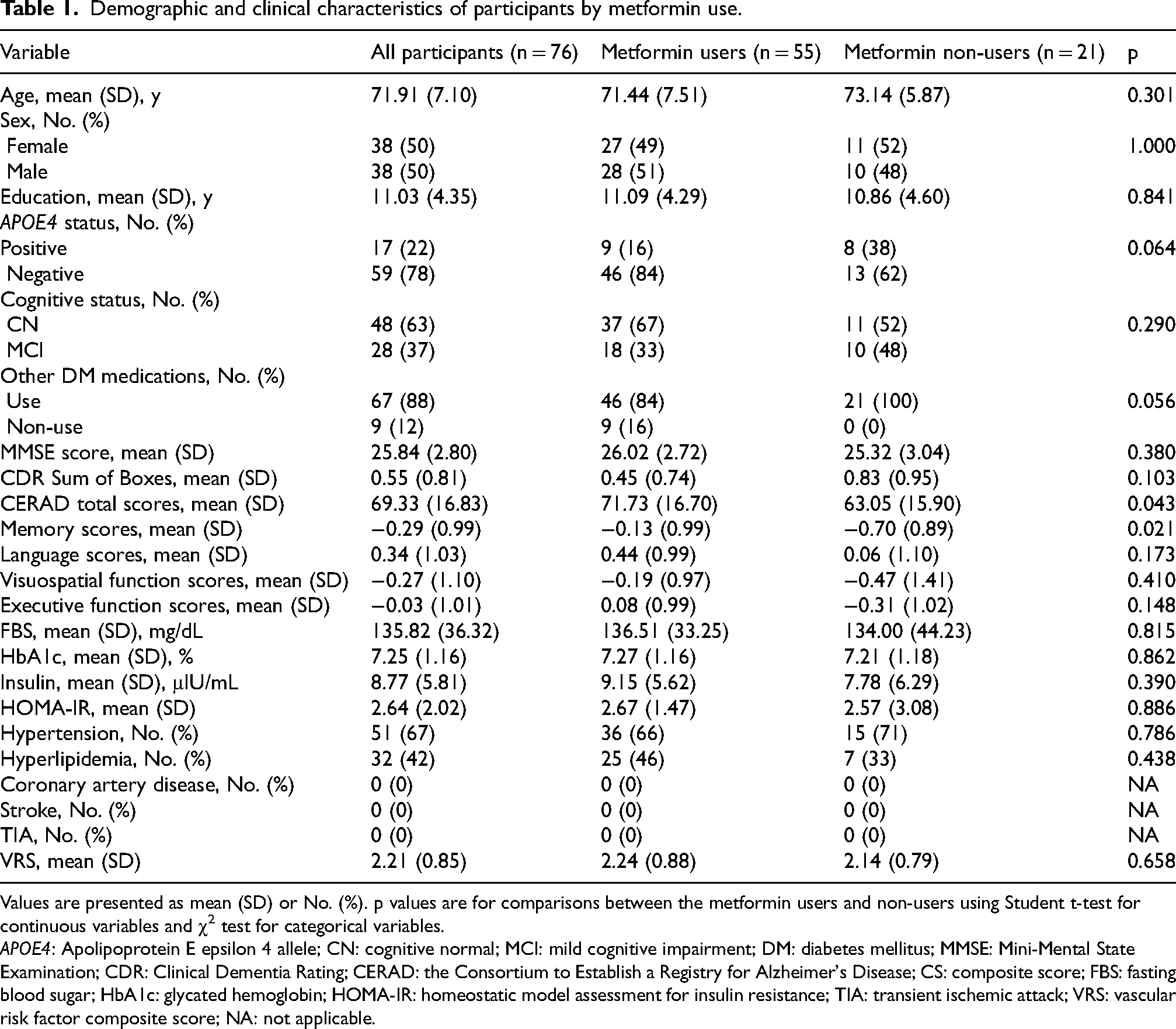
Values are presented as mean (SD) or No. (%). p values are for comparisons between the metformin users and non-users using Student t-test for continuous variables and χ2 test for categorical variables.
APOE4: Apolipoprotein E epsilon 4 allele; CN: cognitive normal; MCI: mild cognitive impairment; DM: diabetes mellitus; MMSE: Mini-Mental State Examination; CDR: Clinical Dementia Rating; CERAD: the Consortium to Establish a Registry for Alzheimer's Disease; CS: composite score; FBS: fasting blood sugar; HbA1c: glycated hemoglobin; HOMA-IR: homeostatic model assessment for insulin resistance; TIA: transient ischemic attack; VRS: vascular risk factor composite score; NA: not applicable.
Associations between metformin use and Alzheimer's disease-related neuroimaging biomarkers.
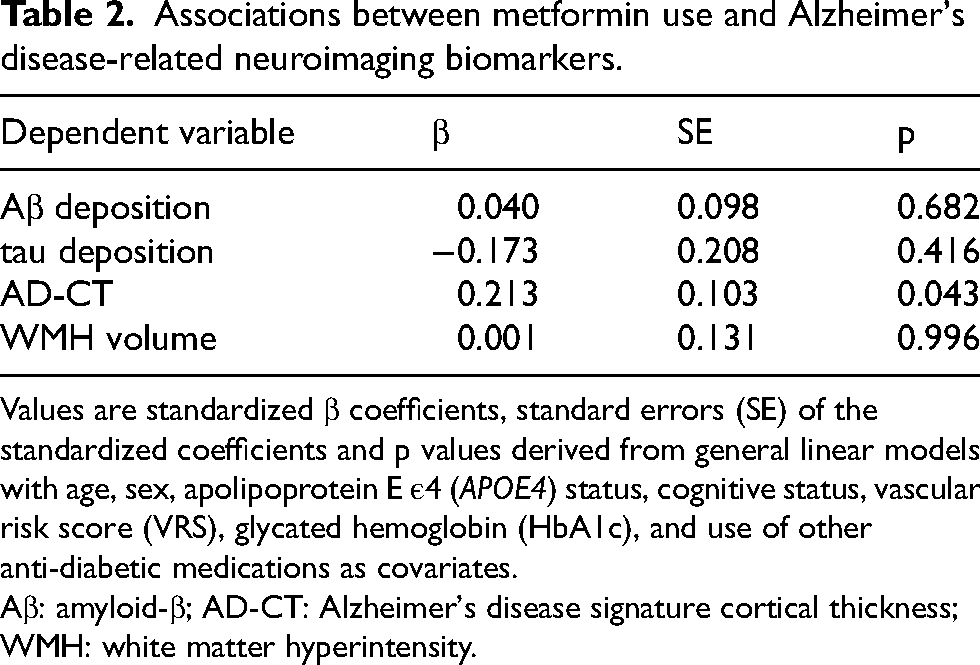
Values are standardized β coefficients, standard errors (SE) of the standardized coefficients and p values derived from general linear models with age, sex, apolipoprotein E ε4 (APOE4) status, cognitive status, vascular risk score (VRS), glycated hemoglobin (HbA1c), and use of other anti-diabetic medications as covariates.
Aβ: amyloid-β; AD-CT: Alzheimer's disease signature cortical thickness; WMH: white matter hyperintensity.
Moderation effects of APOE4 status on the association between metformin use and AD-CT.
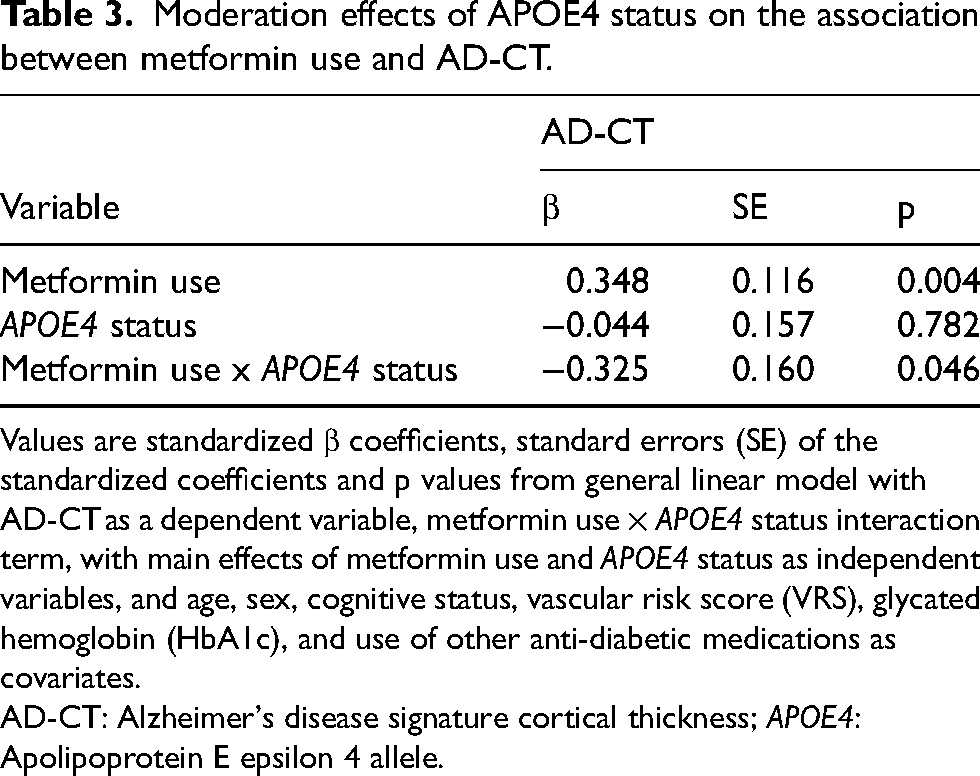
Values are standardized β coefficients, standard errors (SE) of the standardized coefficients and p values from general linear model with AD-CT as a dependent variable, metformin use × APOE4 status interaction term, with main effects of metformin use and APOE4 status as independent variables, and age, sex, cognitive status, vascular risk score (VRS), glycated hemoglobin (HbA1c), and use of other anti-diabetic medications as covariates.
AD-CT: Alzheimer's disease signature cortical thickness; APOE4: Apolipoprotein E epsilon 4 allele.
Subgroup analysis of associations between metformin use and AD-CT by APOE4 status.
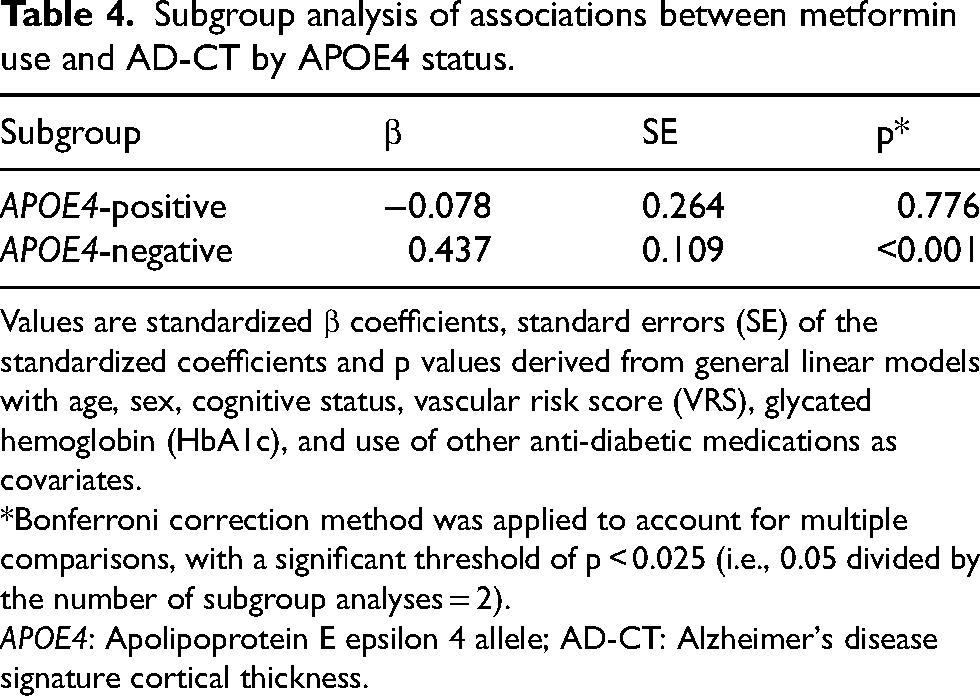
Values are standardized β coefficients, standard errors (SE) of the standardized coefficients and p values derived from general linear models with age, sex, cognitive status, vascular risk score (VRS), glycated hemoglobin (HbA1c), and use of other anti-diabetic medications as covariates.
*Bonferroni correction method was applied to account for multiple comparisons, with a significant threshold of p < 0.025 (i.e., 0.05 divided by the number of subgroup analyses = 2).
APOE4: Apolipoprotein E epsilon 4 allele; AD-CT: Alzheimer's disease signature cortical thickness.
Results
Subject characteristics
The demographic and clinical characteristics of the participants are presented in Table 1. Among the 76 participants, 55 (72%) were metformin users, and 21 (28%) were non-users. The proportion of participants with either CN or MCI status did not significantly differ between the two groups. Additionally, there were no significant differences in APOE4 status, FBS, HbA1c, insulin levels, presence of other VRFs, or VRS between the groups. For cognitive measures, metformin users showed significantly higher CERAD total scores and Memory scores compared to non-users (p = 0.016 and p = 0.021, respectively). There were no significant differences in MMSE scores, CDR sum of boxes, Language, Visuospatial function, and Executive function scores.
Associations between metformin use and neuroimaging biomarkers: exploratory analyses
Exploratory GLM analyses revealed that the p-value for the association between metformin use and AD-CT was < 0.2 (i.e., 0.043), whereas p-values for the associations between metformin use and other neuroimaging biomarkers-global Aβ retention, IF tau deposition, and WMH volume-were > 0.2 (Table 2 and Figure 1). Therefore, AD-CT was selected for subsequent moderation analysis based on APOE4 status.
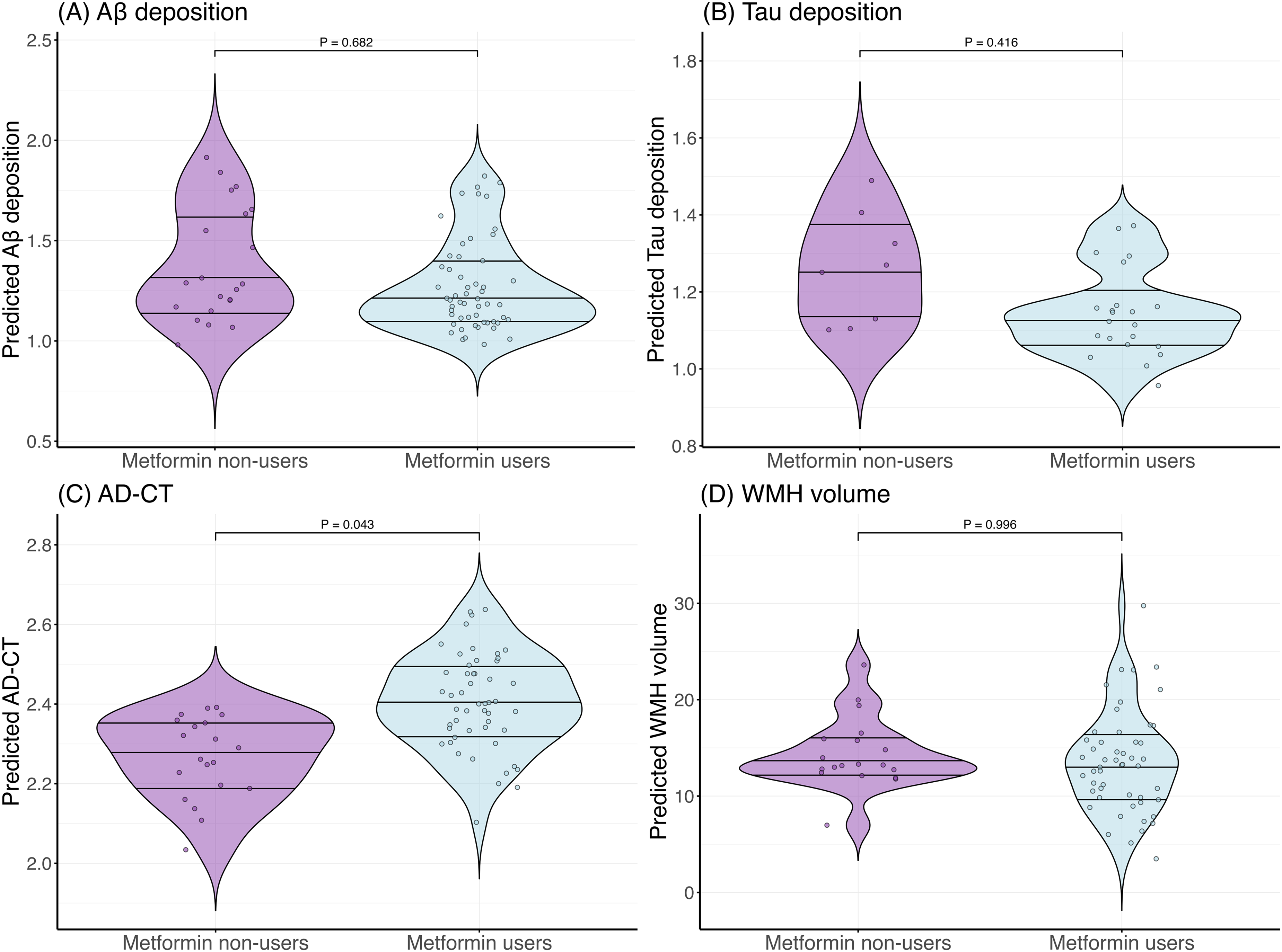
Associations of metformin use with Alzheimer's disease-related neuroimaging biomarkers. Violin plots demonstrate differences in Alzheimer's disease-related neuroimaging biomarkers between the metformin users and non-users. Each violin plot displays the data distribution; horizontal lines represent the 25th, 50th (median), and 75th percentiles. (A) Amyloid-β (Aβ) deposition; (B) Tau deposition; (C) Alzheimer's disease–signature cortical thickness (AD-CT); (D) White matter hyperintensity (WMH) volume. p values were derived from general linear models adjusted for age, sex, apolipoprotein E ε4 (APOE4) status, cognitive status, vascular risk score (VRS), glycated hemoglobin (HbA1c), and other diabetes medication use.
Moderation of APOE4 status on the association between metformin use and neurodegeneration
GLM analysis using AD-CT as the dependent variable revealed a significant interaction between APOE4 status and metformin use (Table 3). Subgroup analyses showed that metformin use was significantly associated with higher AD-CT in APOE4-negative individuals (β = 0.437, p < 0.001), but not in APOE4-positive individuals (β = −0.078, p = 0.780) (Table 4, and Figure 2A, B). Additional exploratory analyses also revealed a significant association between metformin use and global cognition in APOE4-negative individuals (β = 0.170, p = 0.038), but not in APOE4-positive individuals (β = 0.101, p = 0.586) (Figure 2C, D).
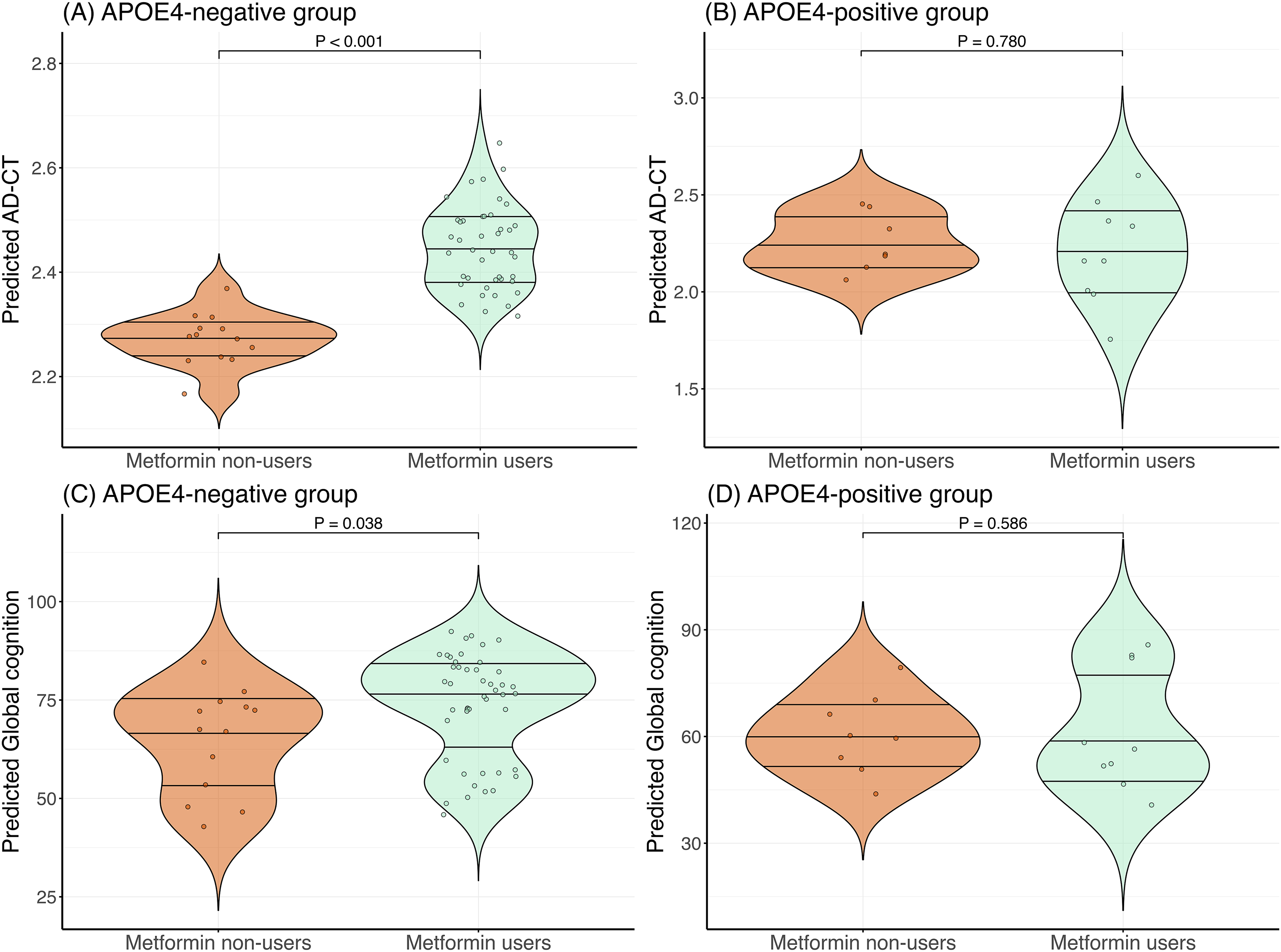
Associations of metformin use with AD-CT and global cognition stratified by APOE4 status. Violin plots demonstrate differences in Alzheimer's disease signature cortical thickness (AD-CT) scores and global cognition scores between metformin users and non-users stratified by apolipoprotein E ε4 (APOE4) status. Each violin plot displays the data distribution; horizontal lines represent the 25th, 50th (median), and 75th percentiles. (A) AD-CT in APOE4-negative group; (B) AD-CT in APOE4-positive group; (C) Global cognition in APOE4-negative group; (D) Global cognition in APOE4-positive group. p values were calculated using general linear models, adjusted for age, sex, cognitive status, vascular risk score (VRS), glycated hemoglobin (HbA1c), and other diabetes medication use. Models for global cognition (C and D) were additionally adjusted for years of education.
Moderation of other potential confounders
We also explored the potential moderation effects of age, sex, cognitive status, HbA1c, and use of other anti-diabetic medications on the relationship between metformin use and AD-CT. None of these variables showed significant interaction effects with metformin use (Table 5).
Moderation effects of other covariates on association between metformin use and AD-CT.
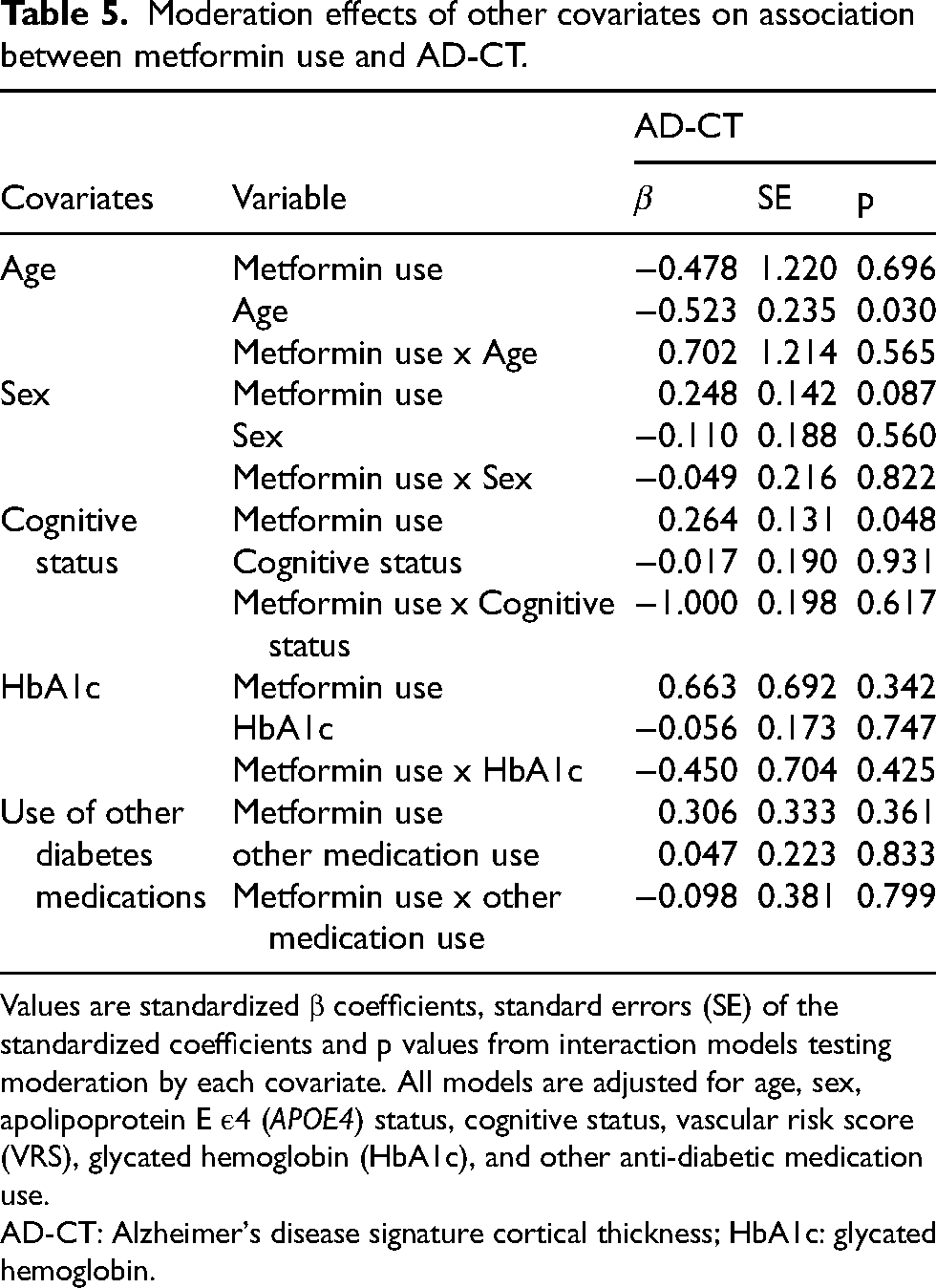
Values are standardized β coefficients, standard errors (SE) of the standardized coefficients and p values from interaction models testing moderation by each covariate. All models are adjusted for age, sex, apolipoprotein E ε4 (APOE4) status, cognitive status, vascular risk score (VRS), glycated hemoglobin (HbA1c), and other anti-diabetic medication use.
AD-CT: Alzheimer's disease signature cortical thickness; HbA1c: glycated hemoglobin.
Discussion
In this study of older adults with T2DM, we found that metformin use was associated with greater AD-CT. Notably, the beneficial association was significant only in the APOE4-negative individuals, and not in APOE4-positive individuals. In contrast to AD-CT, we did not find any significant association between metformin use and other AD neuroimaging biomarkers.
Our findings regarding the relative preservation of AD-related brain regions in metformin users align with the findings from prior studies. For instance, Pomilio et al. 24 reported that among patients with both MCI due to AD and T2DM, those treated with metformin exhibited greater cortical thickness and hippocampal volume compared to non-users. Similarly, Nabizadeh et al. 22 demonstrated that metformin treatment in non-demented T2DM patients was linked to greater cortical thickness across several regions, including the bilateral parietal lobes, left cingulate, and right frontal cortex.
However, we did not find any differences in Aβ or tau burden, as assessed by PET imaging, between metformin users and non-users. This aligns with prior small-scale trials of metformin in AD dementia patients,28,29 which showed no significant alterations in Aβ or tau biomarkers in CSF or plasma, despite trends toward cognitive benefits. Preclinical studies have likewise found that metformin treatment improved cognitive deficits in sporadic AD mouse models without altering Aβ levels, 46 while other studies even suggested that metformin may increase Aβ accumulation.20,21
The observation that metformin use was linked to greater AD-CT but not to reduction in Aβ and tau pathology supports the hypothesis that metformin's neuroprotective effects may be mediated by mechanisms independent of AD-specific protein accumulation. Several such mechanisms could be considered. Although glycemic control is a potential pathway,47,48 we observed no group differences in glycemic markers (e.g., fasting glucose, HbA1c, insulin, or HOMA-IR). Furthermore, the association between metformin use and AD-CT remained significant after adjusting for HbA1c, and interaction tests revealed no moderation by HbA1c. Similarly, controlling for vascular risk had no impact on the results, and WMH volume did not differ across groups, suggesting vascular mechanisms are unlikely to be primary mediators. Alternative neuroprotective pathways may include metformin's ability to suppress neuroinflammation and microglial activation via AMPK-mediated inhibition of the NF-κB pathway.14,49 Additionally, metformin enhances mitochondrial function, reduces oxidative stress, and promotes neuronal survival through its effects on antioxidant enzymes and anti-apoptotic signaling.12,50,51
The main finding of this study is that the positive association between metformin use and AD-CT was evident only in APOE4-negative individuals. Additional exploratory analyses also revealed that global cognition was significantly associated with metformin use in APOE4-negative individuals, but not in APOE4 carriers. These findings are in line with a large observational study by Wu et al., 30 which similarly found that metformin was linked to higher cognitive function only in APOE4 non-carriers. This suggests that while metformin's neuroprotective effects on cortical structure and cognition may be more prominent in APOE4-negative individuals, they may be attenuated in APOE4 carriers, potentially due to APOE4's deleterious influence on neurodegeneration. APOE4 has been implicated in impaired insulin signaling through disrupted insulin receptor recycling, 52 increased neuroinflammatory responses via microglial activation and cytokine release, 53 and elevated oxidative stress due to decreased antioxidant defenses. 54 Such mechanisms may limit the extent to which metformin's neuroprotective effects can manifest in APOE4 carriers. In contrast to APOE4 status, no significant interactions were found between metformin use and other variables (age, sex, cognitive status, HbA1c, or other anti-diabetic medication use), suggesting these factors do not moderate its neuroprotective effects.
Several limitations warrant consideration. First, the cross-sectional design precludes causal inferences. Second, the relatively small sample size—particularly for participants with tau PET scans—may have limited statistical power. Larger studies are needed to validate whether metformin influences tau pathology. Third, there was approximately a two-year gap between the baseline clinical evaluation for metformin use and the tau PET scan. Nevertheless, because metformin is typically prescribed as a long-term maintenance therapy for T2DM, this interval is unlikely to have substantially affected our findings. Consistent with this, metformin use status at the time of tau PET was largely unchanged from baseline, with only one participant switching from use to non-use. Lastly, we lacked detailed information on metformin duration and dosage, which may have impacted the observed associations.
In conclusion, our findings suggest that metformin use in non-demented older adults with T2DM is associated with greater cortical thickness in AD-related regions, which may underlie better cognitive outcome, particularly among APOE4 non-carriers. In contrast, such neuroprotective effects were not apparent in APOE4 carriers, potentially due to APOE4-related neurobiological vulnerabilities.
Footnotes
Acknowledgements
The authors thank all members and participants of the KBASE Research.
ORCID iDs
Ethical considerations
The study protocol was approved by the Institutional Review Board of Seoul National University Hospital (C-1401-027-547) and conducted in accordance with the recommendations of the current version of the Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from all participants or their caregivers.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Ministry of Science, ICT, and Future Planning, Republic of Korea (Grant No: NRF-2014M3C7A1046042, NRF-2020R1G1A1099652 & RS-2022-00165636)) and grants of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (Grant No: HI18C0630, HI19C0149 & HU23C0140), a grant from Seoul National University, and a grant from the National Institute on Aging, United States of America (U01AG072177). The funding source had no role in the study design, data collection, data analysis, data interpretation, writing of the manuscript, or decision to submit it for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analyzed during the present study are not publicly available, owing to ethics considerations and privacy restrictions. Data might be obtained from the corresponding author after approval by the Institutional Review Board of the Seoul National University Hospital, South Korea.