
Abstract
Background
Alzheimer's disease (AD) has been reported to be associated with changes in inflammatory levels, although further research is needed. This study focused on identifying specific inflammatory biomarkers in peripheral blood that could differentiate patients with AD from healthy control subjects.
Objective
The primary objective was to determine whether a selection of peripheral blood inflammatory biomarkers could serve as a diagnostic tool for AD.
Methods
A multicenter study was conducted, comparing 39 patients with AD to 27 healthy controls. AD diagnosis was confirmed through a comprehensive evaluation, including the Mini-Mental State Examination and analysis of cerebrospinal fluid or positron emission tomography. Thirteen inflammatory markers were measured, and logistic regression analysis was used to assess their discriminatory potential. The relationship between the APOE genotype and biomarker levels was also examined.
Results
The analysis revealed that interleukin-8 (IL-8), platelet-derived growth factor (PDGF-AB/BB), and interleukin-12p40 (IL-12p40) were the most significant markers. IL-8 levels showed a strong correlation with disease status, being notably lower in AD patients compared to controls. Furthermore, the levels of these three markers were associated with the patient's amyloid-positive status of the APOE genotype.
Conclusions
These results suggest that reduced levels of IL-8 in the blood could be a promising biomarker for the diagnosis of AD. Additionally, inflammatory biomarkers such as IL-8 and IL-12p40 may be linked to the amyloid pathology of the APOE genotype in AD patients.
Introduction
Alzheimer's disease (AD) is a progressive neurodegenerative disease and the leading cause of dementia in older adults, manifesting cognitive impairment and a decline in functional abilities. 1 Pathophysiological senile plaques formed by amyloid-β (Aβ) peptides, and neurofibrillary tangles of aggregates of hyperphosphorylated tau have long been suggested as the main causes of AD, although it is evident that AD is a complex disease involving multiple mechanisms, including inflammation.2,3
In the last two decades, significant efforts have been made to discover new non-invasive markers with discriminatory capacity for AD. Neuroinflammation-related markers have gained special prominence, particularly following the seminal work of Ray et al. in 2007. 4 This study identified 18 signaling proteins in plasma that could discriminate between AD and control subjects, including cytokines, chemokines, and growth factors.
Cytokines, including interleukins and chemokines, mediate neuroinflammation responses,5–7 wherein microglia and astrocytes play a crucial role in modulating pro- and anti-inflammatory molecules. 8 In AD, there is evidence linking neuropathological hallmarks to cytokine-mediated glia activity.9–11 Evidence indicates that cytokine dysregulation can occur before or during the earliest clinical stages, such as mild cognitive impairment (MCI), which often precedes full AD. Longitudinal cerebrospinal fluid studies in at-risk, symptom-free individuals have reported significant associations between specific cytokines (e.g., Interleukin (IL)-18, IL10RB, CD40) and established AD biomarkers (Aβ42, phosphorylated tau (p-tau)), suggesting that inflammatory changes may precede dementia onset. 12 Similarly, meta-analyses and systematic reviews have found elevated peripheral and central cytokine levels, including IL-1β, IL-6, Tumor necrosis factor-alpha (TNF-α), and IL-18, in MCI and early AD compared to controls, supporting the concept that inflammation is an early event in AD pathogenesis.13–16 However, results are not fully consistent: some studies report pronounced cytokine elevations in early AD, whereas others observe only modest or non-specific changes in preclinical stages.17,18 Methodological differences, patient heterogeneity, and the influence of comorbidities likely contribute to these discrepancies.15,18,19 Overall, these findings suggest that cytokine imbalance may precede the clinical onset of AD, 20 highlighting the potential impact of peripheral cytokines on disease progression. 21
In this study, we assessed a panel of inflammatory proteins in the blood of sex- and age-matched cognitively unimpaired older adults (normal controls (NC)) and individuals diagnosed with AD using Mini-Mental State Examination (MMSE), Aβ, and tau markers in cerebrospinal fluid (CSF) and/or Aβ PET. Our objective was to identify novel circulating markers that could differentiate between cases and controls as well as potential targets for disease-modifying therapies.
Methods
Study participants
Participants aged 65 and older were recruited in 2023 from three Spanish clinical centers (Hospital de la Magdalena, Hospital Arnau de Vilanova, and FISABIO). Inclusion and exclusion criteria, disseminated to participating hospitals, guided recruitment. Independent, specialized neurologists at each site assessed all diagnoses based on clinical history, cognitive evaluation, cerebrospinal fluid biomarkers, and/or Aβ PET imaging. Exclusion criteria included psychiatric disorders and cognitive impairments attributable to other systemic or central nervous system conditions. No systemic inflammatory diseases were reported in either the NC or AD group.
Control subjects were recruited concurrently from the same geographical area (Comunitat Valenciana, Spain), directly from participating hospitals or the Biobank for Biomedical and Public Health Research of the Comunitat Valenciana (Biobank IBSP-CV) (belonging to the FISABIO Foundation). The inclusion criteria for participant recruitment required: individuals aged over 65 years, who reported no subjective memory or cognitive complaints, and no history of psychiatric or cognitive disease.
In addition to age and sex, the following parameters were collected: educational level (no studies, elementary school, middle school, or bachelor's degree), tobacco use (smokers or non-smokers), alcohol consumption frequency (times per week), number of spoken languages, body mass index (BMI), and physical activity (PA, categorized as sedentary or meeting regular exercise criteria, defined as at least 150 min of moderate-intensity or 75 min of vigorous-intensity aerobic exercise per week).
Ethical considerations
The study protocol was approved by the Ethics Committees of Universitat Jaume I (ethical approval number CEISH/44/2022), and the FISABIO Foundation (ethical approval number CEI-SP 20230127/03). Neurologists provided written information and explained the study protocol to the controls, patients and/or caregivers.
Informed consent was obtained from all participants or their guardians in cases where the patient's capacity to consent was compromised. This study was conducted in accordance with the Declaration of Helsinki.
Clinical examination
Prior to the test day, cognitive assessments were conducted by independent Neurology teams at participating hospitals. Body weight was measured to the nearest 0.1 kg, body height was measured barefoot to the nearest 0.01 m, and BMI was calculated. CSF sampling and Aβ-PET analysis were performed as part of routine clinical practice and utilized to determine the final diagnosis. All cases diagnosed with AD exhibited an abnormal tau/Aβ42 ratio.
CSF acquisition and processing
CSF (2.5 mL) was collected via lumbar puncture (L3/L4 or L4/L5). Samples were immediately centrifuged (2000×g, 10 min, 4°C), aliquoted, and stored at −80°C.
CSF (Aβ42), total tau (t-tau), and phosphorylated tau at threonine 181 (p-tau181) were quantified using commercial electrochemiluminescence immunoassays (ECLIA; Roche Diagnostics cobas e411; kit references: 08821941190, 08846685190, and 08846715190) according to manufacturer's instructions. All analyses, conducted as part of standard diagnostic procedures, maintained an analytical coefficient of variation below 10%.
Amyloid PET image acquisition and processing
Amyloid PET imaging used [18F] flutemetamol (185 MBq intravenous bolus) on a Siemens Biograph PET/CT. Images were acquired 90–110 min post-injection.
A qualified nuclear medicine specialist at Hospital General de Castellón performed qualitative visual assessment of tracer uptake. Images were reoriented along the orbitomeatal axis; the Rainbow color scale was used, with the pons as a 90% maximum intensity reference. Grey matter uptake was evaluated in frontal, posterior cingulate/precuneus, lateral temporal, parietal, and striatum regions. Aβ status was determined qualitatively.
Blood collection and biochemical procedures
Fasted blood was collected via venipuncture (8:00–10:00 AM) to minimize diurnal fluctuations. After 15–30 min coagulation at room temperature, samples were centrifuged for serum. Serum aliquots were stored at −80°C for biochemical analyses, avoiding freeze-thaw. Previously, an apolipoprotein E gene (APOE) genotyping aliquot was collected in EDTA tubes.
Biochemical analyses were performed by a blinded laboratory analyst at Hospital Doctor Peset, Valencia, Spain. Serum samples were analyzed using a commercially available Cytokine Human 48-plex panel (MILLIPLEX® Human Cytokine/Chemokine/Growth Factor Panel A-Immunology Multiplex Assay) for the following analytes: epidermal growth factor (EGF), granulocyte-macrophage colony-stimulating factor (GM-CSF), IL-3, IL-4, IL-5, IL-6, IL-8, IL-12p40, IL-15, IP-10, PDGF-BB, sCD40L (reference: HCYTA-60K-12 Human Cyto Panel A), and RANTES (reference: HCYTA-60K-01 Human Cyto Panel A). Samples were randomized across the plate and analyzed in duplicate, according to the manufacturer's recommendations, using the antibody bead mix with biotinylated detection antibody, followed by streptavidin-phycoerythrin. The assay was performed on a Luminex platform (Milliplex), and data was collected for 100 beads per cytokine from each well. Cytokine concentrations were calculated using Milliplex Analyst software, employing a five-parameter curve-fitting algorithm for standard curve fittings. Values below the limit of detection were excluded from statistical analysis. All analyses were conducted in a single batch to minimize inter-assay variability.
APOE genotyping
APOE genotyping was performed on genomic DNA from peripheral blood lymphocytes, as previously described. 22 APOE exon 4, including c.388 and c.526 positions, was amplified (306 bp amplicon) using forward (5'-cggaactggaggaacaactg-3’) and reverse (5'-ggatggcgctgaggaggccgcgctc-3’) primers.
PCR utilized Firepol DNA polymerase (SolisBioDyne) and 10 μM primers, with 1 μL of 100% DMSO facilitating amplification of the GC-rich target. Thermal cycling (ProFlex PCR system, Applied Biosystems) involved initial denaturation (95°C, 2 min), 35 cycles of denaturation (95°C, 30 s), annealing (57°C, 30 s), and extension (72°C, 30 s), followed by a final extension (72°C, 7 min). Unincorporated primers and nucleotides were removed with an Illustra ExoProStar 1-STEP Kit (Cytiva) before bidirectional Sanger sequencing to determine c.388T > C and c.526C > T polymorphisms.
Statistical analyses
The sample size was calculated using an a priori power analysis performed with G-Power to ensure adequate statistical power to detect a meaningful effect. The estimated effect size (Cohen's d = 0.88) was derived from empirical estimates based on preliminary group means and standard deviations, calculated using the effect size determination function implemented in G-Power. Assuming a one-tailed independent samples t-test, a desired power of 0.95, and a significance level (α) of 0.05, the required sample size was 29 participants per group, resulting in a total sample size of 58. Data were extracted from individual files and imported into Jeffreys’ Amazing Statistical Package (JASP; https://jasp-stats.org/) and GraphPad Prism 10.1.1. for statistical analysis and visualization. Outliers were identified using a robust regression and outlier method (ROUT, Q = 0.1%). Prior to each statistical analysis, the normality of the dependent variable's distribution was assessed using the Kolmogorov-Smirnov (KS) test, and homogeneity of variances was evaluated using Levene's test.
Descriptive statistics were used to characterize both groups. To account for multiple testing across the 13 biomarkers analyzed, p-values were adjusted using the two-stage linear step-up procedure of Benjamini, Krieger, and Yekutieli, controlling the false discovery rate (FDR) at Q = 5%. Unless otherwise stated, statistical significance was determined based on FDR-adjusted p-values. A significance level of α < 0.05 was adopted for all statistical tests. To compare the proportions of control and AD subjects with and without the ε4 allele, Fisher's exact test was applied to a contingency table. Binary logistic regression (BLR) models were utilized to examine the association between AD status (AD/NC), amyloid positivity, APOE (ε4/no ε4) status, and protein levels. Each model was fitted using the maximum likelihood estimation method. The discriminatory capacity of each protein was subsequently assessed using receiver operating characteristic (ROC), the area under the curve (AUC), and their associated likelihood ratio test p-values. Effect sizes were reported as odds ratios (OR) with 95% confidence intervals (95% CI), which were calculated by exponentiating the β coefficients (Exp(β)). To evaluate the association between inflammatory markers and AD diagnosis, multivariable logistic regression models were constructed. Model parsimony was prioritized; thus, variables were excluded if they did not significantly improve model fit (as assessed by ΔDeviance) or materially alter the primary effect estimates. All models were tested for interaction terms to ensure an additive relationship between predictors. Adjusted marginal effects were calculated to estimate the predicted probability of AD across standardized protein levels.
All quantitative variables were also depicted using raincloud plots, which combined a cloud of points, box plot, and one-sided violin plot. The cloud of jittered points represents individual observations. The box plot illustrates the median (thick line), interquartile range (box), and the minimum and maximum values (error bars). The one-sided violin (density) plot displays data distribution.
Results
Sociodemographic data
A comprehensive analysis of sociodemographic factors was conducted to characterize the study cohort (Table 1). The final case-control study included 39 AD patients and 27 age-matched NC. All participants self-identified as White of European descent. The mean age of the participants across both groups was 74.8 ± 0.8 years. The age range for the first group was 63.0−84.0 years, and for the second group, it was 66.0−83.0 years. No statistically significant difference in age was observed between the groups (p = 0.98). Women were overrepresented in patients (64.1%), aligning with the previously described sex-biased vulnerability in AD.23–25 In the NC group the percentage of women was 66.7%, demonstrating perfect pairing between the distribution of both two groups, with no statistically significant differences observed (p = 0.8). Furthermore, and as anticipated, BMI was significantly lower in patients (p = 0.008).
Sociodemographic factors of the study cohort.
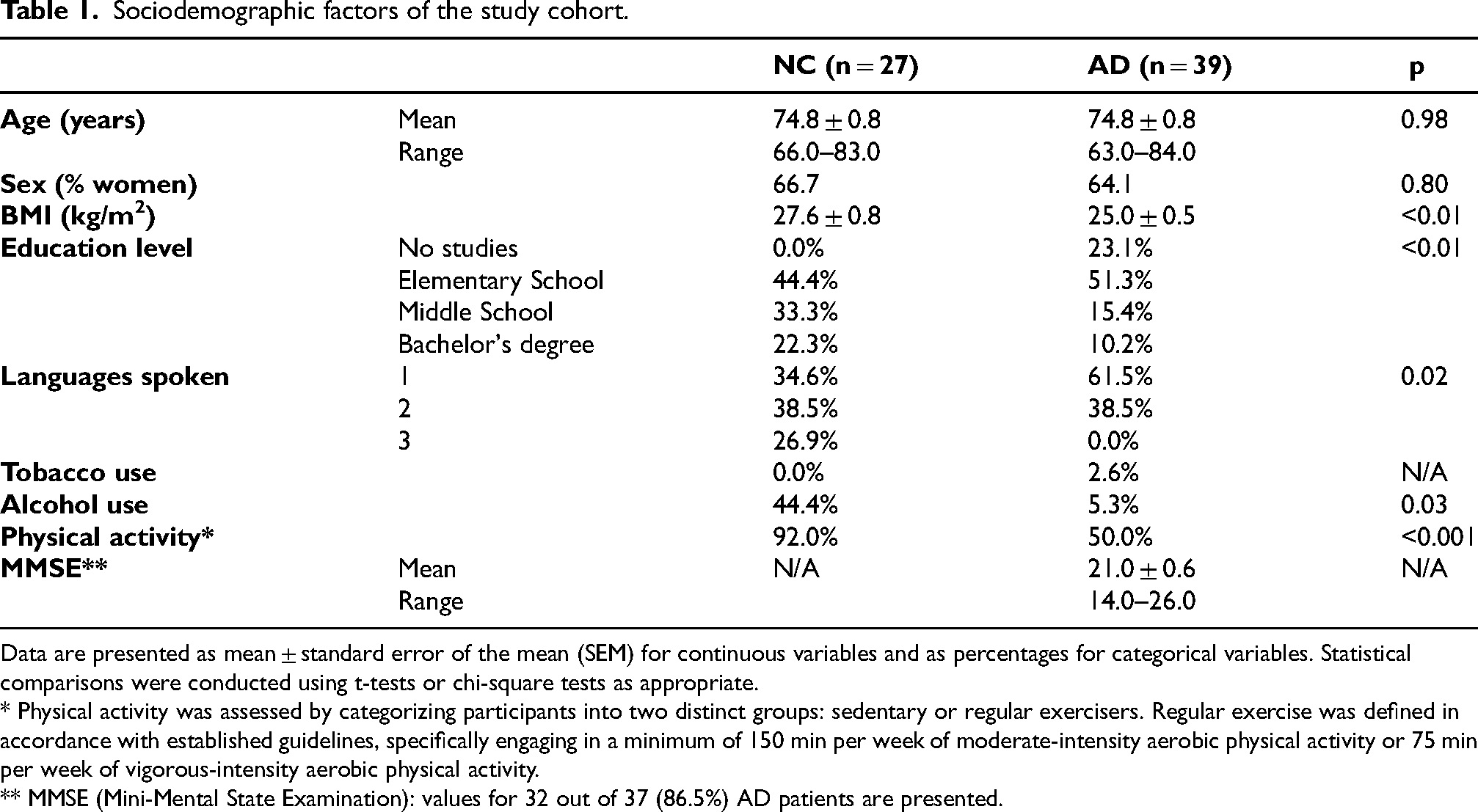
Data are presented as mean ± standard error of the mean (SEM) for continuous variables and as percentages for categorical variables. Statistical comparisons were conducted using t-tests or chi-square tests as appropriate.
* Physical activity was assessed by categorizing participants into two distinct groups: sedentary or regular exercisers. Regular exercise was defined in accordance with established guidelines, specifically engaging in a minimum of 150 min per week of moderate-intensity aerobic physical activity or 75 min per week of vigorous-intensity aerobic physical activity.
** MMSE (Mini-Mental State Examination): values for 32 out of 37 (86.5%) AD patients are presented.
Regarding cognitive reserve factors, educational level was inversely associated with AD prevalence. Indeed, assigning values from zero to three (zero: no education, one: elementary school, two: middle school, and three: bachelor's degree), the score was significantly higher (p = 0.007) in the NC group than in the AD patients (1.78 versus 1.13; a decrease of 36.5%). Additionally, differences in language proficiency were observed between groups, with a higher proportion of AD patients being monolingual (61.5%), whereas a greater percentage of NC reported speaking two or more languages (65.4%). This between-group difference reached statistical significance (p = 0.02). However, these findings should be interpreted with caution, as multilingualism may be associated with other unmeasured factors such as educational attainment and socio-economic status, which were not accounted for in the present study.
Concerning lifestyle habits, only one subject in the entire cohort was a smoker (an AD patient). In contrast, the NC group exhibited significantly higher alcohol consumption habits than patients (44.4% versus 5.3%; p = 0.03). This discrepancy may be attributed to the increased dependence of AD patients. Moreover, control subjects had substantially higher PA levels than patients (92.0% versus 50.0%; p < 0.001), likely due to similar reasons.
Finally, regarding the MMSE, AD patients exhibited a mean score of 21.0 ± 0.6, with values ranging from 14.0 to 26.0. This performance level indicates a predominantly mild-to-moderate severity of global cognitive impairment, consistent with the clinical spectrum of AD in its early-to-intermediate stages.
APOE genotyping
Statistical analysis of the APOE genotypic distribution revealed significant differences between cohorts. The APOE ε3/ε3 genotype was predominant in NC subjects (23/27, 85.2%), whereas APOE ε3/ε4 was the most frequent genotype in AD patients (24/39, 61.5%) (Figure 1A). Consistent with established reports of APOE ε4 enrichment in AD patients, 25 a significantly higher proportion of AD patients carried at least one copy of the APOE ε4 (28/39, 71.8%) compared to NC subjects (3/27, 11.1%). Fisher's exact test confirmed a highly significant association (p < 0.0001; OR = 0.05, 95% CI: 0.014–0.19) (Figure 1(b)).
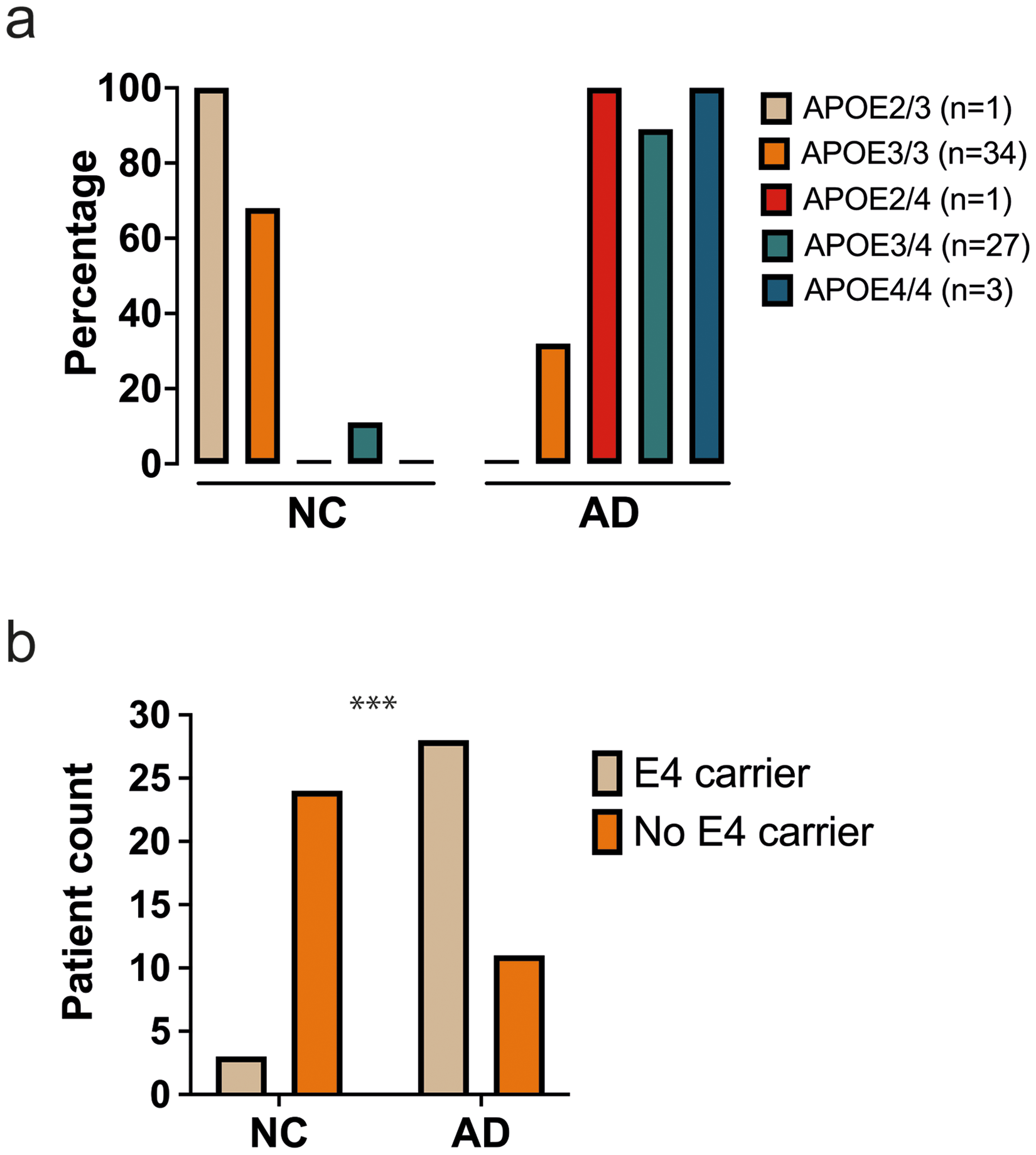
APOE genotypic distribution within the study cohort. Bar graphs were used to present the allelic frequency distribution and total number of cases of each APOE variant across both groups (a), while depicting the number of control and AD individuals carrying at least one ε4 allele (b). Statistical analyses were performed using Fisher's exact test with a significance threshold set at α = 0.05. ***p ≤ 0.001.
Serum concentrations of markers
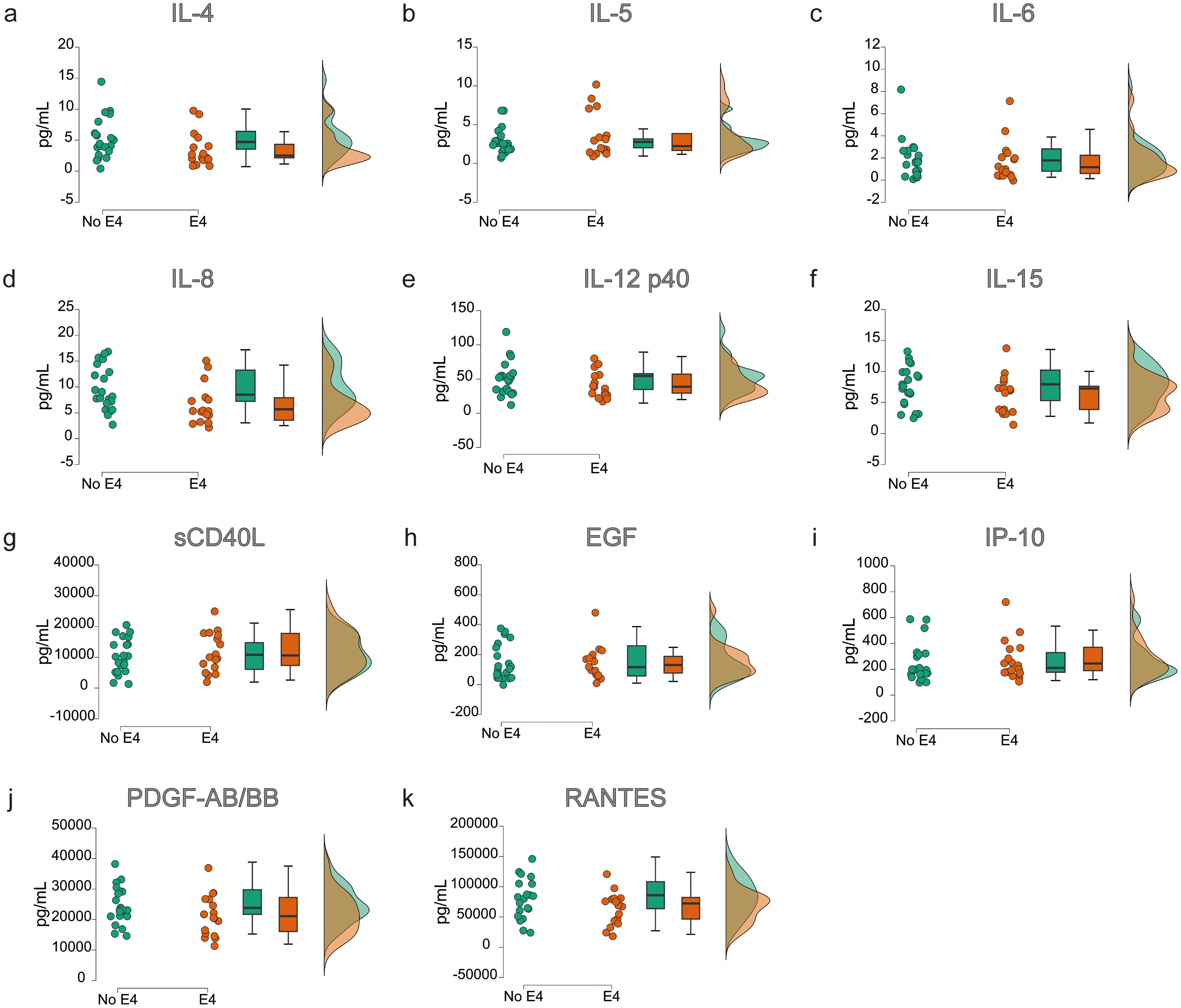
Protein concentrations were evaluated in the serum of NC and AD patients (Figure 2). IL-4, IL-5, IL-6, IL-8, IL-12p40, IL-15, IP-10, EGF, PDGF-AB/BB, sCD40L, and RANTES were detectable within the assay's dynamic range in serum, while IL-3 and GM-CSF were undetectable and thus excluded from the study. In the patient group, serum concentrations of all inflammatory were lower than those of the controls (except for IP-10 and sCD40L), although only the reductions in IL-8 (p = 0.002), IL-12p40 (p = 0.006), and PDGF-AB/BB (p = 0.01) were statistically significant.
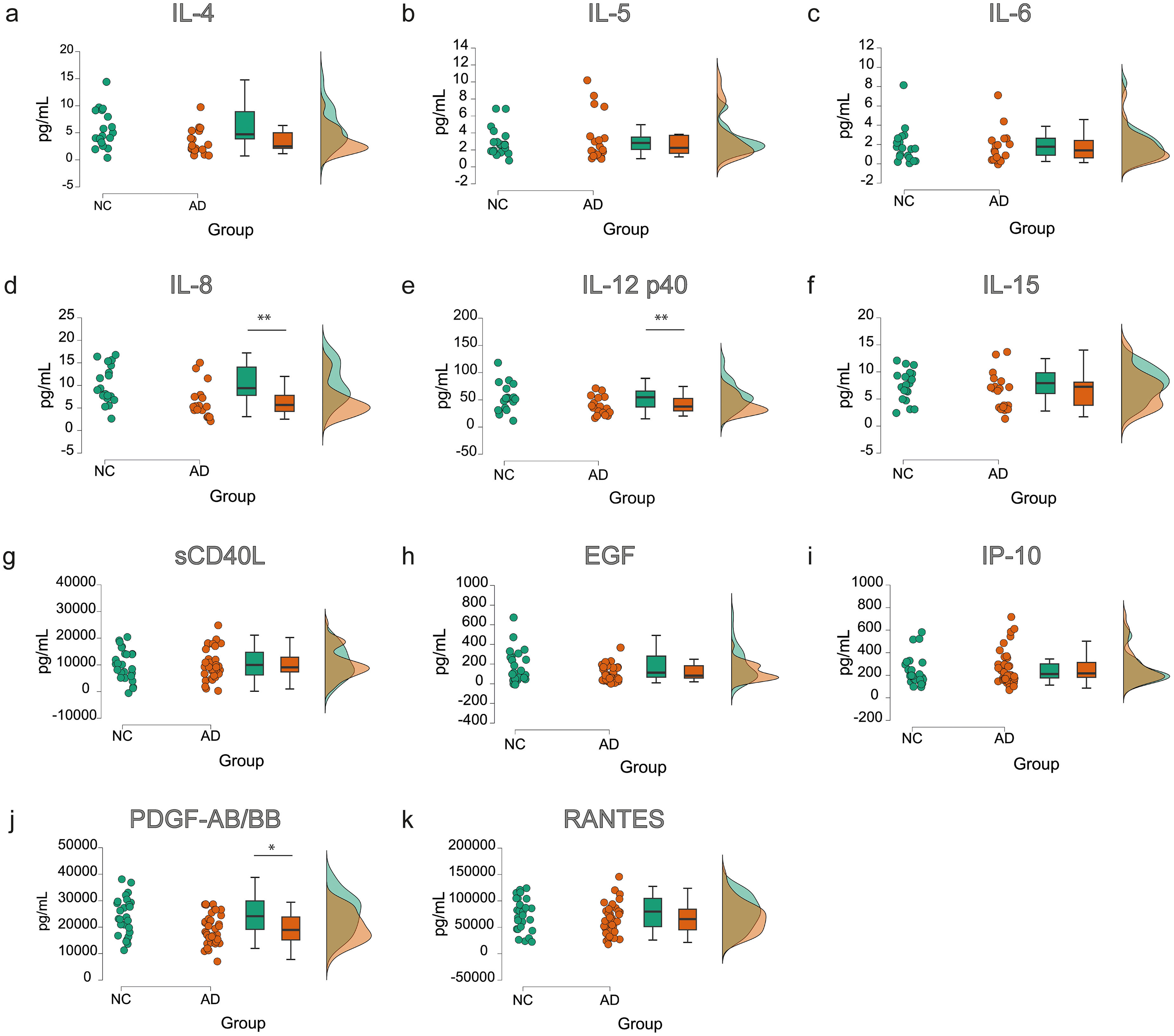
Protein concentrations of the different evaluated markers in NC and AD subjects. Violin plots were used to visualize the data distribution and compare concentrations between the two groups. Results revealed statistically significant differences in the levels of IL-8 (d, **), IL-12p40 (e, **), and PDGF-AB/BB (j, *) between groups. A significance level of 0.05 was set, and independent sample t-tests were performed. *p < 0.05; **p ≤ 0.01.
BLR analyses were conducted to evaluate the independent association of each protein with the presence of AD. IL-8 was significantly associated with an increased probability of AD (OR = 0.83; 95% CI: 0.73–0.93; p = 0.008). Its ROC curve yielded an AUC of 0.77 ± 0.06 (CI: 0.64–0.89, p = 0.003), demonstrating good discriminatory capacity for AD. Similarly, IL-12p40 showed a significant association with a higher probability of AD (OR = 0.97; 95% CI: 0.95–0.99; p = 0.02). The ROC curve for IL-12p40 exhibited an AUC of 0.74 ± 0.07 (CI: 0.61–0.87, p = 0.008), also indicating good discriminatory capacity. Finally, PDGF-AB/BB was significantly associated with an increased probability of AD (OR = 0.99; 95% CI: 0.99–1.00; p = 0.02). The ROC curve for PDGF-AB/BB demonstrated an AUC of 0.69 ± 0.07 (CI: 0.56–0.82, p = 0.03), suggesting, as the others, a good discriminatory capacity (Figure 3).
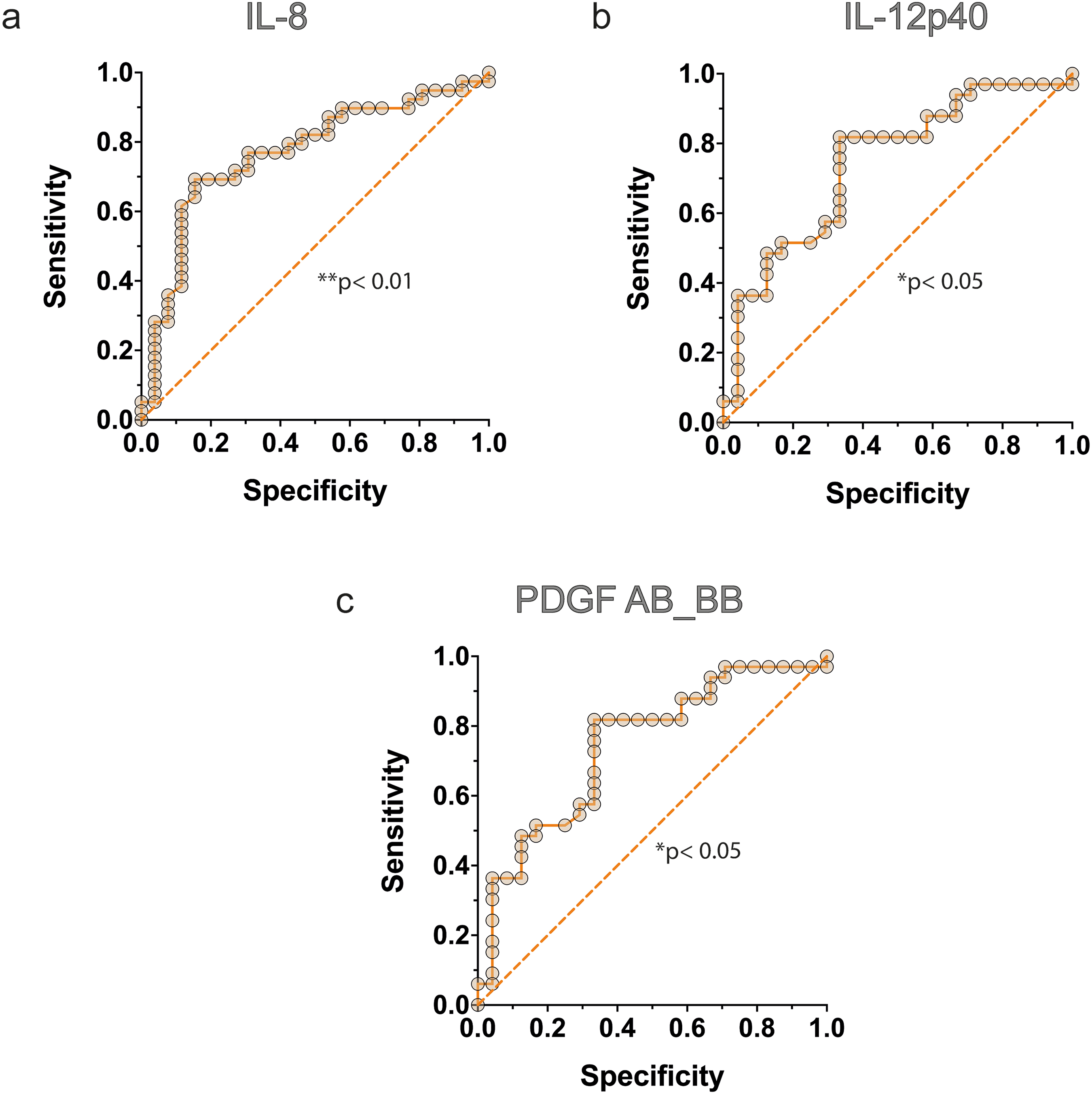
Logistic regression analysis AD cases from NC. The model includes the biomarkers IL-8, PDGF-AB/BB, and IL-12p40 as predictors. Each marker contributes significantly to the classification, as indicated by their respective p-values (*p<0.05; **p < 0.01).
In additional analysis, the subjects were divided into carriers and non-carriers of APOE ε4, regardless of group affiliation, and inflammatory markers were compared again (Figure 4). Most tested proteins exhibited lower levels in the APOE ε4 carrier group (n = 31) than in the non-carriers (n = 35), with some differences reaching nominal statistical significance; however, these associations did not remain significant after FDR correction. Among these, IL-4 (p = 0.12) and IL-8 (p = 0.11) showed the most pronounced trends toward differential expression between groups. BLR analyses suggested a tendency for IL-4 levels to be associated with a higher probability of APOE ε4 carrier status (OR = 0.82; 95% CI: 0.66–0.99). Consistently, the ROC curve for IL-4 exhibited an AUC of 0.67 ± 0.07 (CI: 0.53–0.81), indicating a modest discriminatory performance. Similarly, IL-8 showed a comparable trend toward association with APOE ε4 carrier status (OR = 0.87; 95% CI: 0.77–0.98), with an AUC of 0.69 ± 0.07 (CI: 0.56–0.82) in ROC analysis, suggesting limited but non-negligible discriminative capacity (Figure 5).
Protein concentrations of the different evaluated markers in APOE ε4 carriers and non-carriers. Violin plots were used to visualize the data distribution and compare concentrations between the two groups. Results revealed no statistically significant differences; however, a trend toward reduced IL-4 (a) and IL-8 (d) levels was observed in AD compared with NC.
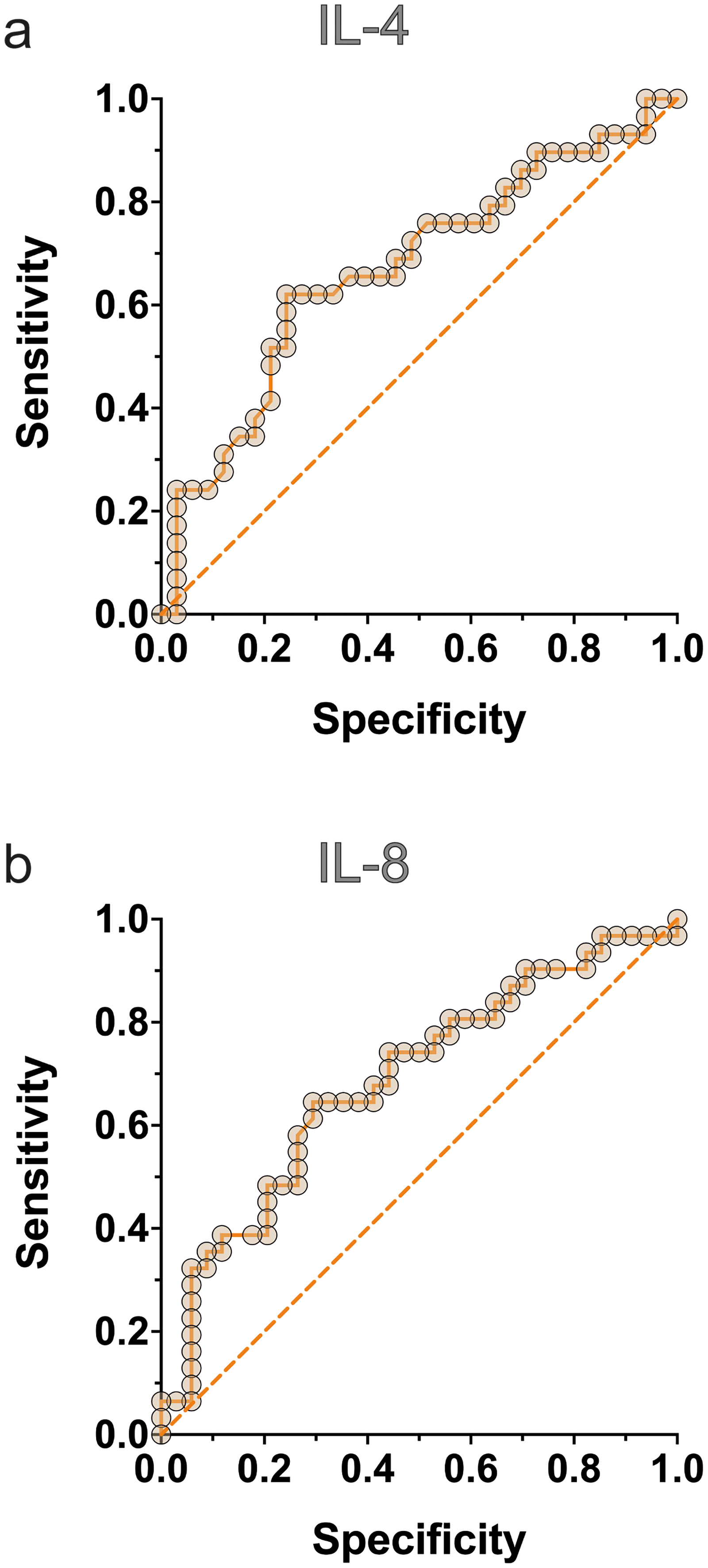
Logistic regression analysis assessing the association between APOE genotype and inflammatory biomarkers. The model includes IL-4 and IL-8 as predictors, both of which show a trend toward contribution to APOE genotype classification.
Finally, the three proteins with significant differences between AD patients and NC (IL-8, IL12p40, and PDGF-AB-BB) were compared for amyloid positivity (determined by CSF (n = 13) and/or PET (n = 26) in APOE ε4 patients) (Figure 6). Amyloid-positive and APOE ε4 patients (n = 30) showed significantly lower levels of all three proteins when compared to amyloid-negative cases (n = 27) (IL8: p = 0.01; IL12: p = 0.01). BLR analyses were also performed to evaluate the independent association of each protein with amyloid positivity in APOE ε4 patients. IL-8 was significantly associated with an increased probability of amyloid positivity in APOE ε4 patients (OR = 0.83; 95% CI: 0.70–0.95; p = 0.04). Its ROC curve yielded an AUC of 0.73 ± 0.07 (CI: 0.59–0.87, p = 0.02), demonstrating good discriminatory capacity. Similarly, IL-12p40 showed a significant association with amyloid positivity (OR = 0.95; 95% CI: 0.91–0.98; p = 0.008) in APOE ε4 patients. The ROC curve for IL-12p40 exhibited an AUC of 0.76 ± 0.07 (CI: 0.62–0.90, p = 0.02), also indicating good discriminatory capacity. Finally, PDGF-AB/BB showed a significantly association with amyloid positivity that did not remain statistically significant after FDR correction (p = 0.07). BLR analysis suggested a tendency for PDGF-AB/BB to be associated with amyloid positivity (OR = 0.99; 95% CI: 0.99–1.00;) in APOE ε4 patients. Consequently, the ROC curve demonstrated an AUC of 0.67 ± 0.07 (CI: 0.52–0.81), indicating a modest discriminatory capacity (Figure 7).
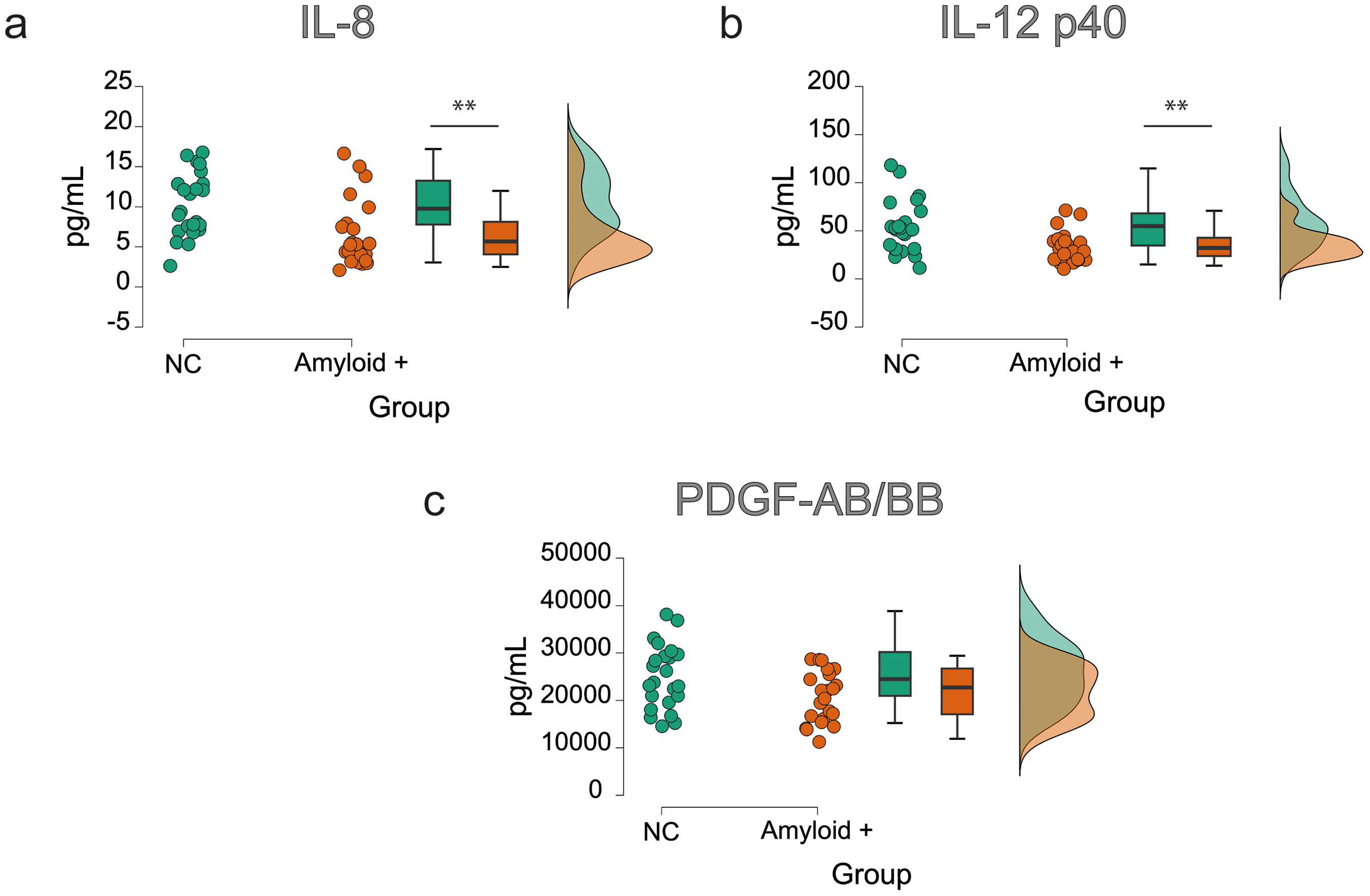
Protein concentrations of IL-8, IL-12p40, and PDGF-AB/BB in nc compared to APOE ε4 amyloid-positive cases. Violin plots were used to visualize the data distribution and compare concentrations between the two groups. Results revealed statistically significant differences in the levels of IL-8 (a, **), IL-12p40 (b, **), and a tendency in PDGF-AB/BB (c) between groups. A significance level of 0.05 was set, and independent sample t-tests were performed. **p ≤ 0.01.
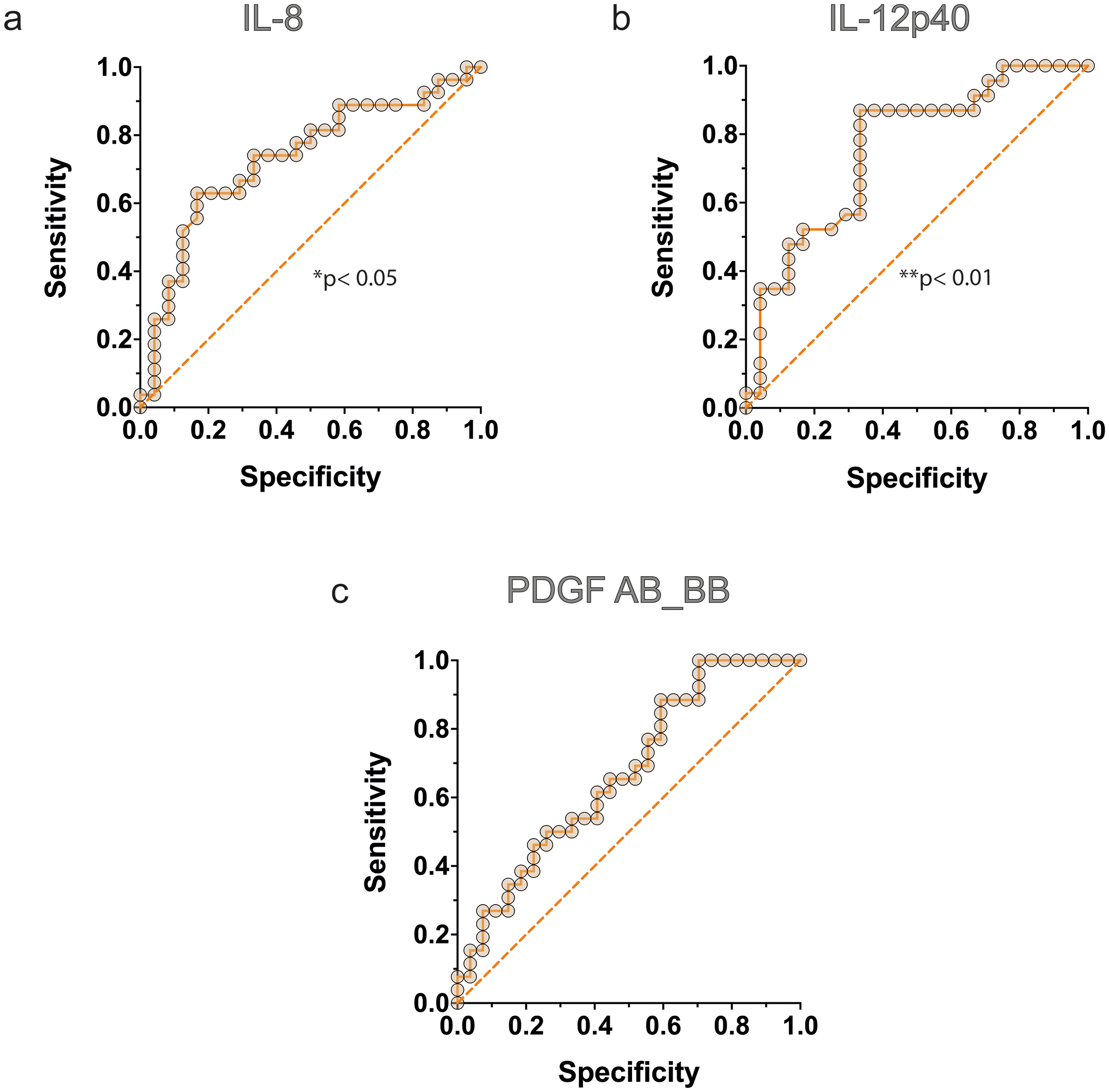
Logistic regression analysis assessing the association between APOE ε4 amyloid pathology and inflammatory biomarkers. The model includes the biomarkers IL-8, PDGF-AB/BB, and IL-12p40 as predictors. IL-8 and IL-12p40 show statistically robust contributions to the classification (*p < 0.05; **p < 0.01), whereas PDGF-AB/BB displays a trend toward contribution.
After analysis of IL-8, IL12p40, and PDGF-AB/BB levels, we studied the different ratios related to the analyzed conditions of the cohort, observing decreasing AD/NC ratios of 0.63, 0.61 and 0.81, respectively (Figure 8(a)). Upon stratification by APOE ε4 carrier status, the carrier-to-non-carrier ratios were observed to be 0.72 for IL-8, 0.78 for IL-12p40, and 0.87 for PDGF-AB/BB (Figure 8(b)). Finally, the comparison between amyloid-positive APOE ε4 subjects versus NC subjects showed ratios of 0.65 for IL-8, 0.61 for IL12p40, and 0.83 for PDGF-AB/BB (Figure 8(c)).
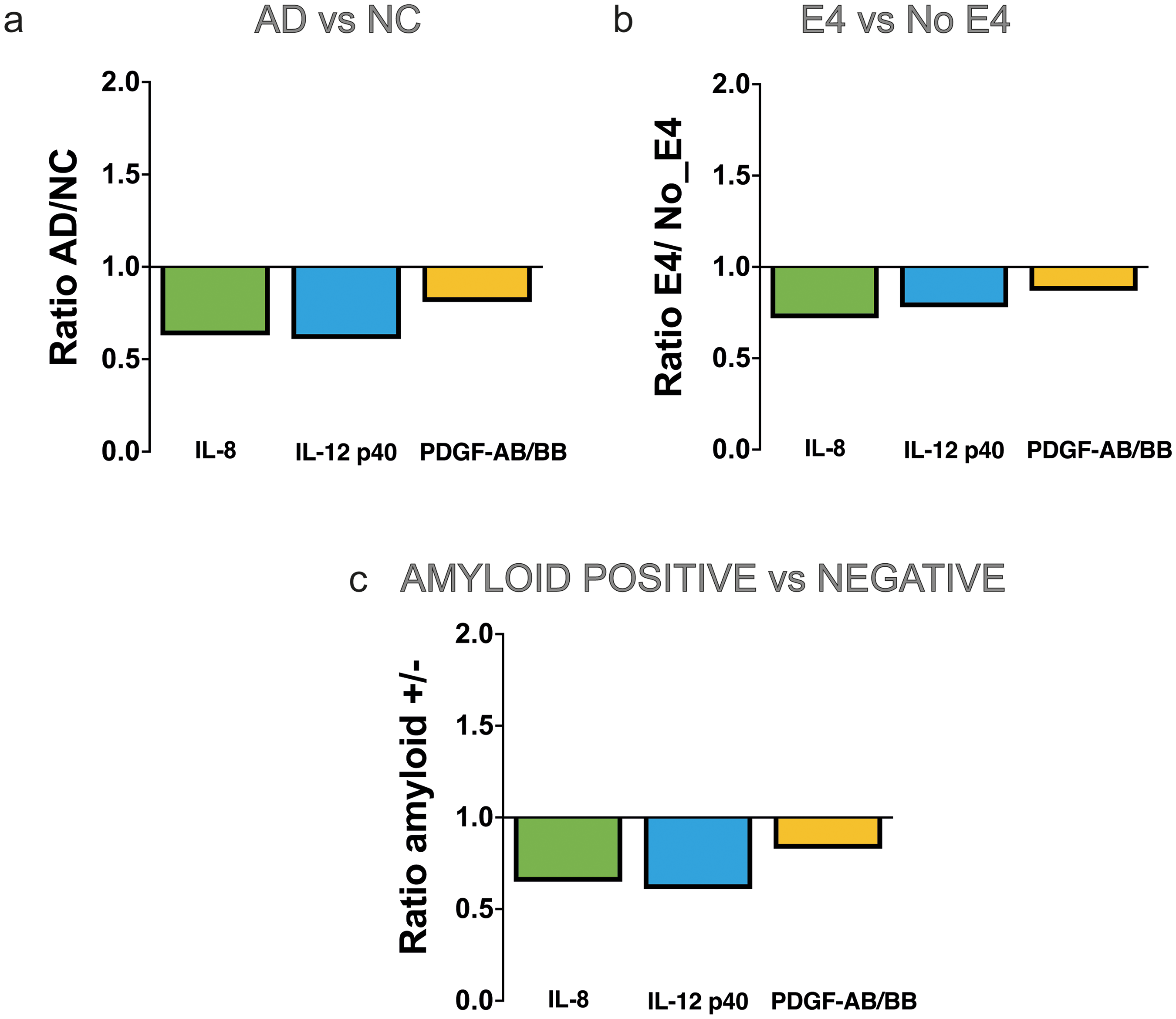
Protein concentration ratios for IL-8, IL-12p40, and PDGF-AB/BB. Bar graphs illustrate these ratios when comparing AD to NC groups (a), APOE ε4 carriers to non-carriers (b), and amyloid-positive to NC (c).
Regarding the potential crosstalk between our neuroinflammation and established AD hallmarks, correlation analyses revealed distinct patterns (Figure 9). While all IL-8, IL-12p40 and PDGF-AB/BB remained independent of CSF Aβ42 levels (Figure 9(a)–(c)), IL-8 displayed a modest yet significant positive association with p-tau (r = 0.34, p = 0.045) and total Tau (r = 0.37, p = 0.046). These data indicate that IL-8 levels may track more closely with tau-mediated axonal damage than with amyloid pathology. Notably, IL-12p40 and PDGF-AB/BB did not show any significant relationship with the biomarkers evaluated, further highlighting the specific involvement of IL-8 in this neurodegenerative process.
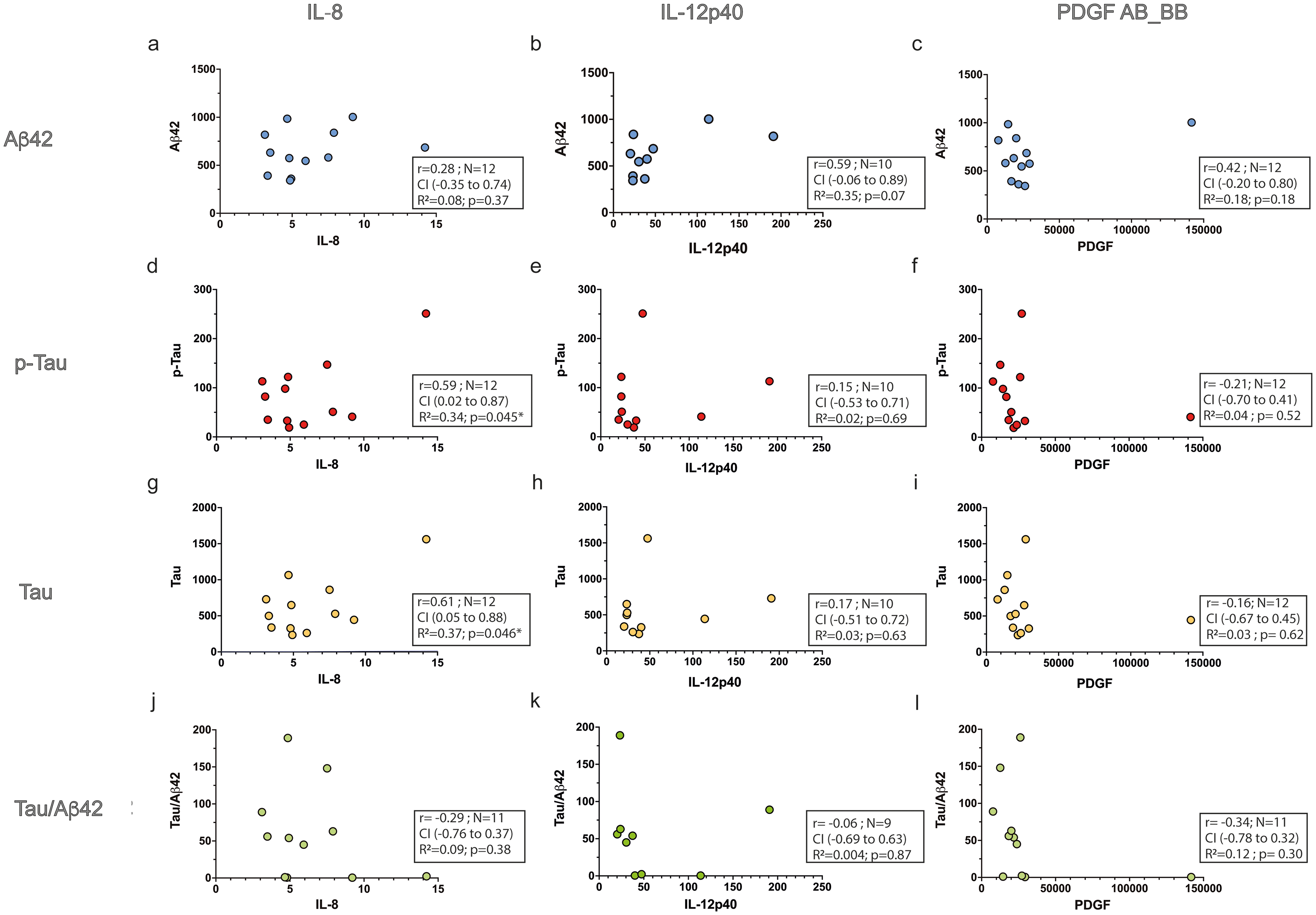
Correlations between IL-8, IL-12p40, and PDGF-AB/BB and core AD biomarkers. Scatter plots depict the relationships between serum concentrations of IL-8, IL-12p40, and PDGF-AB/BB and AD-related biomarkers. Panels (a–c) show correlations with Aβ42, panels (d–f) with phosphorylated tau (p-Tau), panels (g–i) with total tau (Tau), and panels (j–l) with the Tau/Aβ42 ratio. Each dot represents an individual subject. Spearman's correlation coefficients (r), p values, and sample sizes (N) are indicated within each panel. No significant associations were observed for Aβ42, whereas significant positive correlations were detected between IL-8 and both p-Tau and Tau.
Finally, to account for potential confounding, multivariable logistic regression models were expanded to include BMI and PA as covariates; notably, IL-8 was the only inflammatory marker to exhibit a persistent association with AD status under these adjusted conditions (data not shown). In the fully adjusted model, both IL-8 levels and PA remained independently associated with AD diagnosis. Specifically, PA demonstrated a robust inverse association with AD, while higher standardized IL-8 levels were associated with a lower predicted probability of AD.
Although the inclusion of BMI provided a modest improvement in model fit (ΔDeviance=3.51, p = 0.061), its independent association did not reach statistical significance. No significant interactions were observed between IL-8, BMI, and PA, supporting an additive model. Other sociodemographic factors, including education, smoking status, and alcohol consumption, were excluded from the final model to preserve parsimony and ensure model stability, as they either showed high imbalance across groups or did not materially alter the primary effect estimates (data not shown).
Discussion
While Aβ plaques and tau neurofibrillary tangles remain quintessential hallmarks of AD, over the past two decades the inflammatory component, both central and peripheral, has gained prominence among the events related to AD pathogenesis. A substantial body of work has underscored the significance of peripheral immune alterations, particularly proinflammatory signaling, in AD development. Indeed, peripheral inflammation has been identified as a potential risk factor for AD and vascular dementia.26,27 Cross-sectional analyses and cohort studies have consistently shown that cognitively normal individuals with elevated circulatory inflammatory markers face an increased risk of future MCI, AD dementia, and all-cause dementia.28–32 These findings highlight the critical need to clarify how disease stage, underlying pathology, and specific inflammatory molecules may influence the relationship between inflammatory proteins and AD progression.
In the present prospective multicenter case-control study, we comprehensively analyzed a panel of systemic inflammatory markers to determine their variations in AD patients and normal controls, with further stratification by APOE genotype and Aβ positivity. A key strength of our study lies in the rigorous matching of patients and NC in terms of age and sex ratio, minimizing heterogeneity and enabling more accurate conclusions regarding the circulating biomarkers under study. Moreover, patients with AD were enriched in the APOE ε4 allele compared to NC, confirming the classical association of this genotype with the disease 25 and reinforcing the representativeness of our study population. Our findings are consistent with an inverse association between education level and multilingualism and AD prevalence. However, rather than implying a protective effect, these observations should be interpreted as correlational and may reflect the influence of cognitive reserve–related factors or other unmeasured confounders, such as socio-economic status, which were not explicitly assessed in the present study.
To elucidate the role of inflammation in AD, we conducted a comprehensive analysis of up to 13 proteins associated with the inflammatory response in the serum of patients and normal controls using a Milliplex™ panel. While two of them were undetectable in either group, two others showed no difference between groups, and the remaining nine exhibited lower levels in patients than in controls. Notably, this study identifies an inverse association between serum levels of three of these proteins (IL-8, IL-12p40, and PDGF-AB/BB) and the presence of AD. Specifically, all of them were significantly associated with an increased probability of AD as their respective ROC curves yielded AUC values of 0.77 ± 0.06, 0.74 ± 0.07, and 0.69 ± 0.07, all demonstrating good discriminatory capacity.
IL-8, a chemokine produced by macrophages in response to proinflammatory mediators such as amyloid, may play a critical role in recruiting activated microglia to sites of AD brain damage. 33 While previous studies have reported significantly elevated IL-8 levels in the CSF of AD patients compared to controls, 34 plasma levels in late-onset AD have shown inconsistent findings, with some studies reporting no difference between patients and controls in European populations. 35 A meta-analysis, limited by the small number of studies examining IL-8, did not find conclusive evidence of its involvement in AD. 36 However, other studies have demonstrated increased IL-8 levels in AD, 37 underscoring the heterogeneity of the existing literature. Notably, very few studies have directly examined IL-8 in relation to core AD biomarkers, such as amyloid pathology, which limits the interpretation of IL-8 alterations in the context of underlying disease mechanisms. In this regard, our findings add novel evidence by specifically linking peripheral IL-8 with amyloid biomarkers. Consistent with our results, Kim et al. observed significant lower IL-8 concentrations in patients with MCI or AD compared to controls. 38 Furthermore, Shen et al. reported diminished peripheral IL-8 levels in AD patients compared to those with MCI. 39 The present findings indicate that circulating IL-8 levels are inversely associated with AD status, independent of BMI and PA. While this observation may seem counterintuitive given previous reports of increased inflammation in dementia, several mechanistic hypotheses could account for lower detectable IL-8 in peripheral blood. These include peripheral sequestration of cytokines in affected tissues, receptor desensitization or downregulation in chronic disease states, and compensatory anti-inflammatory regulatory processes. Importantly, the association of IL-8 with AD remained robust across multiple multivariable models, despite substantial heterogeneity in comorbidities and pharmacological treatments, suggesting that the observed relationship is not solely driven by medication effects or lifestyle factors. Nevertheless, residual confounding cannot be fully excluded, and these findings should be interpreted with caution. Future studies in larger and more homogeneous cohorts, ideally with longitudinal follow-up and detailed stratification by comorbidities and medication classes, will be essential to disentangle disease-related inflammatory changes from compensatory or treatment-related effects and to clarify the mechanistic role of IL-8 in AD pathogenesis.
Regarding IL-12, a pleiotropic and heterodimeric cytokine implicated in bacterial infections and autoimmune diseases,40,41 we observed lower serum levels of IL-12p40 in AD patients. In this sense, previous research has demonstrated a correlation between IL-12 levels and AD severity, with elevated levels in mild to moderate AD and decreased levels in severe AD. 42 In this regard, Yang and co-workers in a study analyzing nine cytokines found that higher levels of IL-12p70 were associated with slower cognitive decline in AD. 43 Additionally, Swardfager et al. reported increased IL-12 levels in the blood of patients with mild and moderate AD, 36 whereas severe AD was associated with suppressed plasma IL-12 levels. 42 These findings align with our results and suggest a potential role of IL-12 in AD progression.
Finally, PDGF is a potent mitogen for several cellular types, including vascular smooth muscle cells and brain glial cells, and is a primary mitogen in platelet-derived human serum.44–46 As observed in our study, Ray et al. identified PDGF-BB as a pivotal protein in a plasma signature differentiating AD from controls. 4 Their study revealed a lower PDGF-BB expression in AD subjects than in controls. The inhibitory effect of Aβ on the neuroprotective PDGF-BB system and the loss of its receptor in AD further emphasize its potential significance in disease pathogenesis.47,48
Our study provides further insights into the relationship between these proteins and key AD risk factors. Our findings suggest a trend in which decreased levels of both IL-8 and IL-4 align with a higher likelihood of being an APOE ε4 carrier, indicating a potential inverse association between these cytokines and genetic risk status.
Furthermore, we observed that IL-8 and IL-4 were all significantly associated with an increased probability of amyloid positivity in APOE ε4 carriers. Their respective AUCs underscore their discriminatory potential for amyloid-positive cases, consistent with established diagnostic criteria for AD. These findings extend beyond mere diagnostic markers, suggesting that these inflammatory proteins are not only associated with AD status but also with underlying genetic risk (APOE ε4) and core neuropathology (amyloid positivity).
A notable finding in our study was the independent diagnostic value of IL-8, which persisted even after adjusting for key lifestyle and metabolic factors such as PA and BMI. While PA demonstrated a robust inverse association with AD—consistent with its well-documented neuroprotective effects—the persistence of the IL-8 effect suggests that this cytokine captures a distinct facet of the disease's immunological endophenotype. The lack of significant interaction between IL-8 and PA further supports an additive model, implying that the inflammatory signaling represented by IL-8 and the benefits of physical activity may operate through partially independent pathways. Although BMI provided a modest improvement to the model's fit, its influence was attenuated in the fully adjusted analysis, reinforcing the idea that IL-8 serves as a more direct proxy for the systemic inflammatory state associated with AD. These results emphasize the importance of accounting for lifestyle covariates in biomarker research to ensure that observed associations reflect underlying pathophysiology rather than residual confounding.
Beyond the established utility of traditional biomarkers, it is important to note that while p-tau shows superior diagnostic accuracy for AD pathology, IL-8 offers distinct value by capturing the patient's immunological endophenotype. Unlike p-tau, IL-8 reflects the neuroinflammatory component, which is crucial for stratifying patients for immunomodulatory interventions. Additionally, the multiplex assay provides a cost-effective, comprehensive inflammatory profile from a single sample. Finally, IL-8 pre-analytical requirements (fasted morning serum) align with standard clinical biochemistry workflows, ensuring feasible implementation. Nevertheless, the present study has several methodological limitations that should be acknowledged. Although the statistical analyses yielded consistent results, the modest sample size may limit the robustness and generalizability of the logistic regression models and ROC curve analyses. The cross-sectional case–control design precludes any causal or temporal inferences regarding the observed biomarker associations. There are currently no universally established reference ranges for the cytokines analyzed using MILLIPLEX multiplex assays; absolute concentrations are assay-specific and not directly comparable across analytical platforms. Therefore, results should be interpreted in terms of relative differences and discriminative performance rather than absolute biomarker thresholds. The absence of an independent replication or validation cohort further constrains the interpretation of these findings in the context of biomarker discovery. In addition, all subjects were recruited from a single geographic region (the Valencian Community), which may limit generalizability. Key cognitive-reserve and lifestyle variables, including education, multilingualism, and socio-economic status, were incompletely captured, and formal adjustment was not possible. These limitations emphasize that the results should be interpreted within the context of these demographic and lifestyle constraints, highlighting the need for confirmation in larger, more diverse, and longitudinal cohorts.
In conclusion, our study supports the relevance of systemic inflammation in AD and identifies a peripheral inflammatory signature defined by reduced serum levels of IL-8, IL-12p40, and PDGF-AB/BB. These markers, particularly IL-8, are not only associated with AD diagnosis but also with key pathological features, including APOE ε4 carrier status and amyloid positivity, while retaining independent diagnostic value after adjustment for lifestyle and metabolic factors. Collectively, these findings suggest that selected circulating inflammatory proteins reflect an immunological endophenotype of AD that complements established biomarkers and may aid patient stratification. Nevertheless, larger and longitudinal studies are required to validate these associations and to clarify the prognostic and mechanistic relevance of systemic inflammatory alterations in AD progression.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to the patients and their caregivers, as well as to the control group participants, for their invaluable contributions to this study. We also acknowledge the institutional support of the Hospital de La Magdalena, the Hospital Arnau de Vilanova, the Hospital General Universitario de Castellón, and the FISABIO-Public Health Unit of the IBSP-CV Biobank (PT23/00034), which is part of the ISCIII Biomodels and Biobanks Platform and the Valencian Biobanking Network. Furthermore, we are deeply grateful for the generous donation of Paula Batet and Pau Torres, which made this research possible.
ORCID iDs
Ethical considerations
The study protocol was approved by the Ethics Committees of Universitat Jaume I (ethical approval number CEISH/44/2022), and the FISABIO Foundation (ethical approval number CEI-SP 20230127/03).
Consent to participate
Neurologists provided written information and explained the study protocol to the controls, patients and/or caregivers. Written informed consent was obtained from all participants or their guardians in cases where the patient's capacity to consent was compromised. This study was conducted in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the program UniSalut (grant number UJISABIO22_PI01).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.