
Abstract
Background
Eye movement abnormalities have emerged as promising non-invasive candidate biomarkers for the early detection, progression monitoring, and differential diagnosis of Alzheimer's disease (AD), with preliminary clinical evidence supporting their translational potential. Current AD diagnostic methods are limited by subjectivity, high cost, and complexity—making non-invasive biomarkers critical, especially for mild cognitive impairment (MCI). The tight functional link between the eye and brain underscores eye movement abnormalities as a window into AD-related pathology.
Objective
This systematic review summarizes AD-associated multi-modal eye movement dysfunctions (focusing on saccades, fixation, and smooth pursuit), clarifies their pathological mechanisms, clinical value, and translational feasibility, providing a basis for constructing an AD biomarker system.
Methods
Literature searches were conducted in PubMed, Web of Science, and Google Scholar using (“Alzheimer's disease” OR “mild cognitive impairment” AND “eye movements” OR “saccades” OR “smooth pursuit” OR “fixation”) with a search cutoff date of September 30, 2025. Studies deemed irrelevant or lacking sufficient data were excluded.
Results
AD/MCI patients exhibit eye movement abnormalities: prolonged saccadic latency, increased antisaccade errors, reduced fixation stability, and attenuated smooth pursuit gain, which are closely linked to core AD pathologies, detectable in AD/MCI stages, and can, to a certain extent, distinguish AD from Parkinson's disease and frontotemporal dementia, and have value for MCI-to-AD conversion prediction.
Conclusions
Eye movement abnormalities hold promise as non-invasive biomarkers for AD, with potential for preclinical screening and differential diagnosis. To advance translation, future research should prioritize AI-driven multi-modal integration, standardized detection protocols, portable device development, and preclinical longitudinal validation.
Introduction
Alzheimer's disease (AD) is a neurodegenerative disease characterized by progressive memory loss and cognitive decline. Its typical neuropathological features include senile plaques formed by amyloid-β (Aβ) deposition, neurofibrillary tangles (NFTs) caused by hyperphosphorylation of tau protein, and significant loss of cholinergic neurons in the basal forebrain. 1 At present, the clinical diagnosis of AD still mainly relies on neuropsychological scale assessment combined with cerebrospinal fluid (CSF) detection or molecular imaging techniques, such as Aβ positron emission tomography (PET), tau-PET, magnetic resonance imaging (MRI) and other imaging techniques. However, these approaches exhibit distinct limitations when applied to early screening and popularization efforts, primarily due to strong subjectivity, insufficient specificity, and the practical challenges of high cost and complex operation.2,3 Therefore, the identification of objective, non-invasive biomarkers with high feasibility for widespread implementation has emerged as a critical research focus in the field of AD.
The eye and brain are highly analogous with respect to developmental origin, functional characteristics, cellular composition, neurotransmitter receptors, blood supply sources, and angiogenesis.4,5 These similarities suggest that aberrant eye movements could have an inherent link to abnormalities in brain network function, underscoring the eye's potential as a window into central nervous system pathology.6,7 It is reported that the regulation of eyeball movement depends on a fine neural network composed of frontal eye movement area (FEF), 8 parietal eye fields (PEF), 9 superior colliculus (SC), 10 cerebellum and brainstem nuclei. 11 It is worth noting that this network is the key area involved in the early stage of AD pathology. Studies have shown that AD-related Aβ and tau pathological deposition, cholinergic system degeneration, and neural network connection breakage can directly affect the efficiency and accuracy of eye movement control.12–15 Therefore, AD patients may have quantifiable eye movement abnormalities before clinical symptoms appear, and eye movement tracking technology is expected to become a powerful tool for early identification and course monitoring of AD.
Compared with traditional technologies such as neuroimaging, eye movement detection has the advantages of non-invasive, short time-consuming and low cost, and is more suitable for large-scale population screening and longitudinal monitoring. Existing studies have initially revealed that AD patients have characteristic changes in many types of eye movement tasks, including saccade 16 (such as prolonged latency, increased error rate), fixation stability 17 (such as increased drift), smooth pursuit 18 (such as decreased gain), and exploratory strategies. 19 However, most of the existing reviews focus on a single type of eye movement abnormalities, and there is a lack of integrated analysis of multi-modal eye movement indicators and a systematic exposition of their association with the pathological progression of AD.
This review aims to systematically review the research progress of AD-related eye movement dysfunction, focusing on the abnormal characteristics of various eye movement modes such as saccade, fixation, and smooth pursuit and their evolution with the progression of the disease, and to explore the neurobiological mechanisms such as Aβ/tau pathology, cholinergic defects, and neural network disruption. In addition, this paper will also compare the differences in eye movement patterns between AD and other neurodegenerative diseases (such as Parkinson's disease (PD) and frontotemporal dementia (FTD)) to evaluate the value of eye movement parameters in differential diagnosis, and provide a theoretical basis and application framework for the construction of AD biomarker system based on eye movement tracking. Notably, this review emphasizes MCI as a critical transitional stage, highlighting the unique value of eye movement parameters in predicting AD conversion and guiding early intervention.
To systematically retrieve literature on eye movements linked to AD, core search terms were defined as (“Alzheimer's disease” OR “Mild Cognitive Impairment”) AND (“eye movements” OR “saccades” OR “smooth pursuit” OR “fixation”). Searches were done in PubMed, Web of Science, and Google Scholar with a retrieval cutoff date of September 30, 2025. Duplicates were removed via EndNote; initial screening (titles/abstracts) excluded irrelevant studies. Full-text screening excluded inaccessible texts, insufficient data, or mismatched designs, yielding eligible studies for later use (Figure 1).
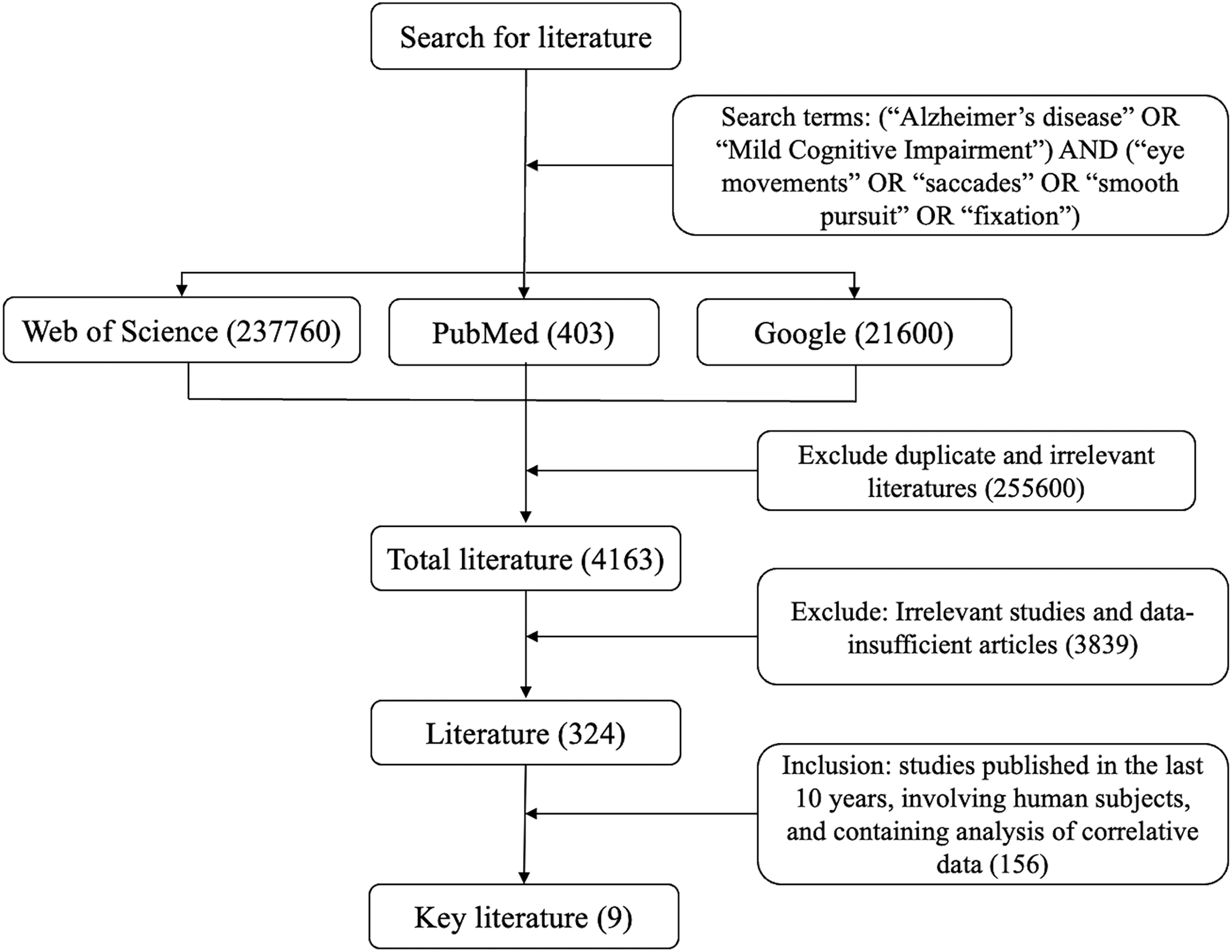
Schematic diagram of literature retrieval and screening process.
Eye movement dysfunctions in AD patients
AD-related eye movement impairments include saccades, smooth pursuit, and fixation. 20 These abnormalities are closely associated with the stages of AD. The NIA-AA 2011 Clinical Diagnostic Criteria, combined with the DSM-5 staging system, were adopted to categorize AD into three stages: preclinical AD, MCI due to AD, and AD dementia, with the latter further subdivided into mild, moderate, and severe sub-stages in some studies.21–23
Characteristics and pathological mechanisms of saccadic dysfunction in ad patients
Saccadic movement is the fastest type of eye movement in the human body, whose primary function is to rapidly shift the foveal fixation to the target region. 24 Its role is to enable the macular region—the retina's area of highest visual and color sensitivity—to rapidly capture targets, while regulating the neural network consisting of the FEF, PEF, SC, and brainstem eye movement nuclei. 25 This eye movement is closely linked to the brain's attentional mechanisms and serves as one of the most sensitive indicators for screening cognitive impairment.26–28 Saccadic dysfunction in patients with AD is characterized by multiple types, early onset, and gradual progression. 26 It encompasses prosaccades, antisaccades, and microsaccades, with all these abnormalities exhibiting a distinct exacerbation pattern as the disease advances.
Prosaccade dysfunction in AD patients
Prosaccade denotes a type of saccadic eye movement wherein the eyes rapidly shift from a fixation point to a suddenly appearing peripheral target, aligning their direction with the target's location. 29 The prosaccade task typically requires participants to first maintain fixation on a central point. Upon presentation of a peripheral target stimulus, they must execute an immediate saccade toward the target, with no deliberate inhibition or redirection. 23 This eye movement is regarded as a fundamental, automatic eye movement response, commonly utilized in clinical and neuroscientific research to evaluate the integrity of visual attention, sensorimotor integration, and eye movement control. 30 It has been reported that prosaccadic abnormalities progressively worsen with the clinical progression of AD, with distinct disease-discriminating features observed at each stage.27,31,32 In the preclinical stage of AD, patients typically exhibit no objective cognitive impairment, 28 with their prosaccadic function remaining largely intact. 26 There are reports indicating that upon progressing to the MCI stage of AD, saccadic abnormalities may emerge, including prolonged saccadic latency and an increased incidence of saccadic undershoot. 33 Clinical observations and relevant research have shown that as AD progresses to the dementia stage, the previously identified saccadic abnormalities are further exacerbated. 28 Specifically, this stage is characterized by a significant prolongation of saccadic latency, a marked reduction in peak velocity, and an increased incidence of both saccadic undershoot and saccadic overshoot2,3,32,34 (Table 1), with the indicator mainly used for assessing disease severity rather than early prediction.
Prosaccade abnormalities in AD.
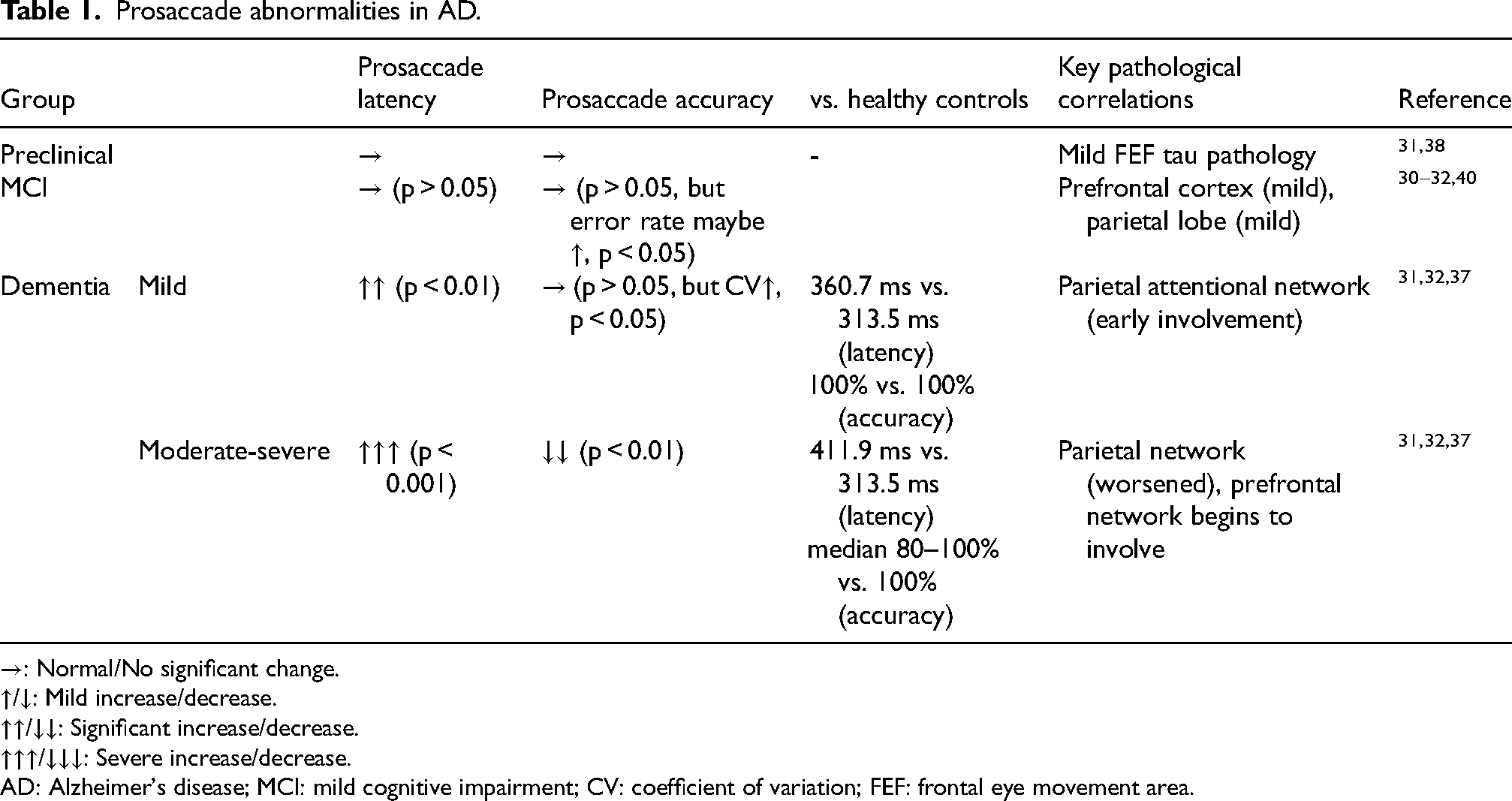
→: Normal/No significant change.
↑/↓: Mild increase/decrease.
↑↑/↓↓: Significant increase/decrease.
↑↑↑/↓↓↓: Severe increase/decrease.
AD: Alzheimer's disease; MCI: mild cognitive impairment; CV: coefficient of variation; FEF: frontal eye movement area.
Compared with other neurodegenerative diseases, the prosaccade abnormalities of AD are mainly characterized by progressive and significant prolongation of latency, reflecting impaired information processing speed. 27 PD patients usually have normal latency but significant undershoot due to dopaminergic damage in the basal ganglia; FTD patients may show normal latency but more severe undershoot. These differences provide a reference for clinical identification.35,36
The pathological basis of prosaccade abnormalities is related to the structural damage of PEF and SC. In the course of AD, pathological changes in these brain regions, including tau protein deposition, 37 Aβ deposition, 38 cholinergic system degeneration 39 and decreased synaptic density,are closely involved in prosaccade dysfunction. Specifically, tau deposition in PEF impairs spatial information processing and sensorimotor integration, directly leading to increased saccadic undershoot and variability in amplitude. 38 Additionally, neuroinflammation may further participate in and accelerate this pathological process.
Prosaccade detection can be used as a potential auxiliary biomarker for AD diagnosis, but its application has certain limitations. The sensitivity of preclinical stage is insufficient, and the specificity of MCI stage is limited, which overlaps with PD, FTD and other diseases. In the stage of mild to moderate dementia, the combined application of multiple indicators may help to assess the severity of the disease, but it still needs to be combined with multi-modal indicators such as CSF detection and imaging for comprehensive judgment.
Antisaccade dysfunction in AD patients
The antisaccade task requires participants to suppress the instinctive impulse to look at a sudden visual stimulus (prosaccade) and instead perform an eye movement pointing in the opposite direction. Successful completion of this task requires complete inhibition control, working memory, and attentional flexibility. 41 Studies 31 have shown that AD patients show increased error rate (i.e., difficulty in inhibiting the impulse of reflexive stimuli) and decreased correction ability (i.e., difficulty in autonomous correction after finding errors) in this task, and these defects are aggravated with disease progression. In the preclinical AD stage, patients may show a slight increase in error rate in complex tasks, while simple task performance is often normal, and this mild abnormality has no statistical significance for predicting AD risk. As the disease progressed to the MCI stage, the error rate further showed a moderate increase, the correction rate decreased, and the correction latency prolonged.28,40 This stage's antisaccade error rate is a core predictive marker for AD conversion: when combined with prosaccade latency, the predictive efficacy is superior, which is far more valuable than the preclinical stage's trivial changes and the dementia stage's severe error ratethat only reflects the loss of inhibitory control function. In the AD dementia stage, the abnormality is more significant, the error rate continues to increase, the correction ability decreases significantly, and finally the patient may completely lose the reverse saccade ability 42 (Table 2).
Antisaccade abnormalities in AD.
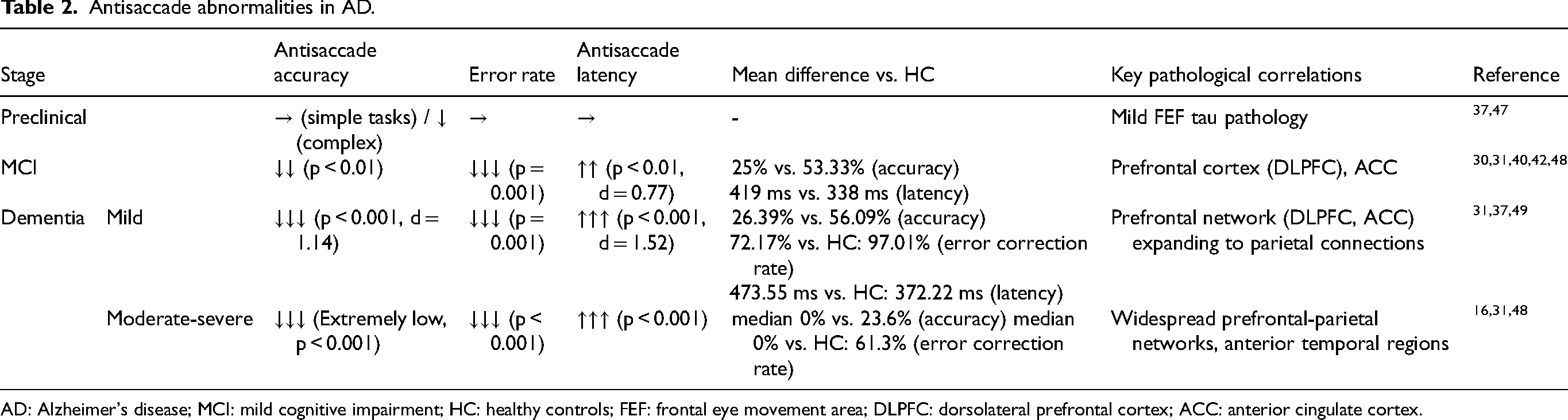
AD: Alzheimer's disease; MCI: mild cognitive impairment; HC: healthy controls; FEF: frontal eye movement area; DLPFC: dorsolateral prefrontal cortex; ACC: anterior cingulate cortex.
Compared with other neurodegenerative diseases, the abnormal pattern of AD in the antisaccade task may be of differential significance. Studies have shown that the increase of error rate in PD patients is usually mild, and the correction ability is relatively retained. FTD patients may show more serious error rate and correction ability defects, reflecting different pathological mechanisms and neural basis. 43
The dysfunction of antisaccade is related to the neuropathological changes of AD, mainly involving the damage of FEF and cholinergic system.27,44 The pathological deposition of tau in the FEF region and the loss of cholinergic neurons in the basal forebrain may be related to the decrease of inhibitory control function, 45 but the specific pathophysiological mechanism still needs further study. Neuroimaging studies have linked prolonged corrected antisaccade latency to decreased metabolism in the right dorsolateral prefrontal cortex (DLPFC), a region critical for working memory and task monitoring during antisaccade execution. 46
The antisaccade task stands as a promising biomarker for AD and a sensitive behavioral measure to identify progressive deficits in inhibitory control and error monitoring in affected individuals. Key behavioral signatures include markedly elevated error rates, particularly uncorrected errors—compromised error correction capacity, and prolonged latency of correct responses, with performance worsening sequentially from the MCI stage to AD dementia. Critically, antisaccade impairment emerges in the prodromal phase, conferring predictive value for MCI-to-AD conversion. For differential diagnosis, a defining feature distinguishes AD from bvFTD: AD patients exhibit near-complete loss of error correction, whereas bvFTD patients retain relatively intact correction abilities. Its clinical utility is nonetheless limited in moderate-to-severe dementia due to inadequate patient cooperation, necessitating future studies to validate its real-world applicability and explore combinatorial use with other biomarkers.
Fixation dysfunction in AD patients
The fixation movement disorder of AD patients can occur in the early stage of the disease and deteriorate systematically with the progression of the disease. Fixation is not the complete stillness of the eyeball, but an active control process involving physiological drift, tremor and microsaccades.16,50,51 Its core function is to maintain the stability of visual images in the macular fovea of the retina to support higher-order cognitive processing. This process depends on coordinated regulation of neural networks including the parietal cortex, SC, brainstem integrators, and prefrontal cortex, with the prefrontal cortex critical for suppressing irrelevant saccades via cognitive control.31,35,51,52
In the preclinical stage, although AD patients have no significant clinical symptoms, there have been subtle changes in fixation stability, manifested as a slight increase in drift velocity and an increase in the frequency of small square wave beats. As the disease progresses to the MCI stage, the fixation instability is further aggravated, the variability of fixation position is significantly increased, and the fixation maintenance ability begins to decline. 16 Patients show increased saccade intrusion rate and shortened fixation duration in tasks that require ignoring distractors. In the stage of AD dementia, the fixation function is seriously impaired, and patients often cannot maintain stable fixation, showing a purposeless “wandering fixation” mode, and the visual positioning function is basically lost 16 Table 3.
Fixation abnormalities and neural mechanisms in AD.
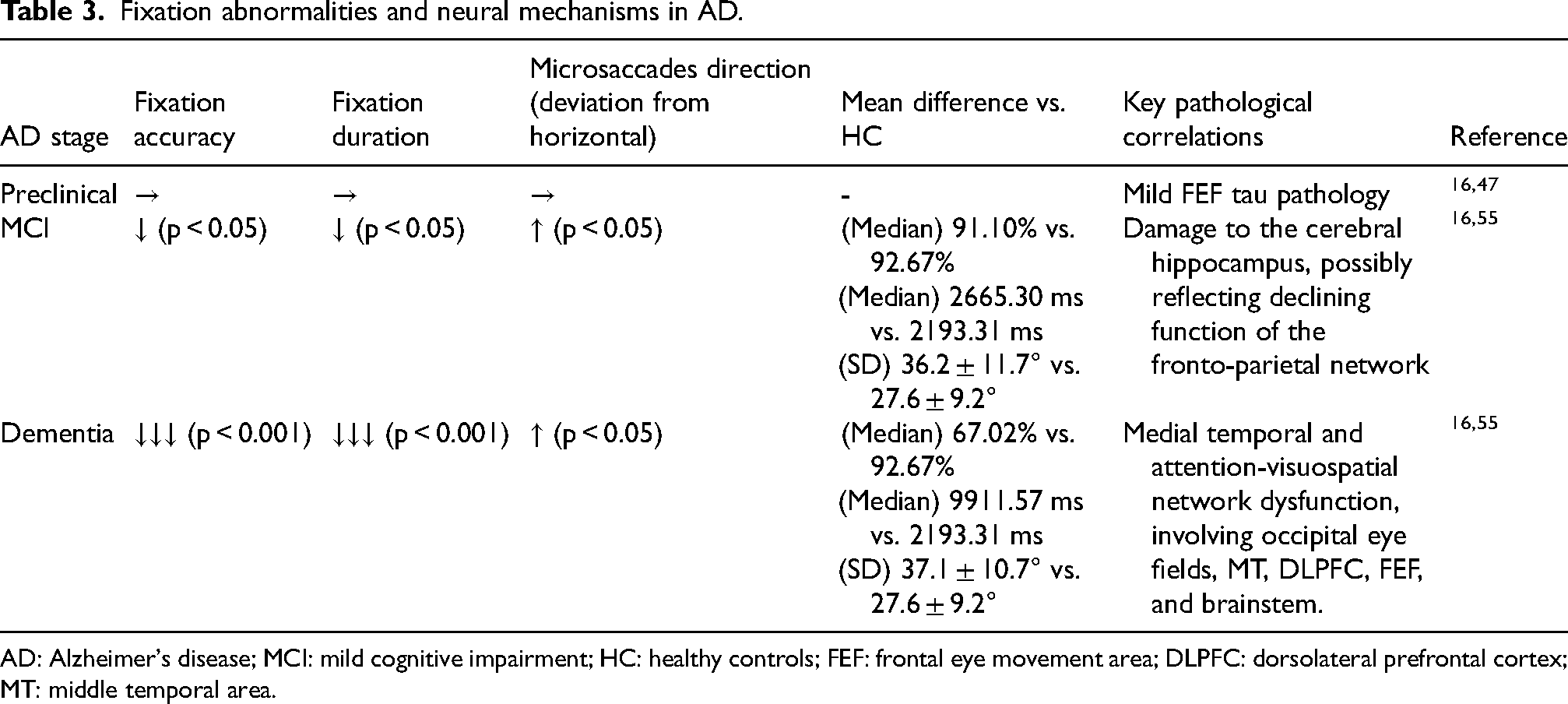
AD: Alzheimer's disease; MCI: mild cognitive impairment; HC: healthy controls; FEF: frontal eye movement area; DLPFC: dorsolateral prefrontal cortex; MT: middle temporal area.
The neural correlates of this impairment are linked to distinct pathological processes. The degradation of basic fixation stability is primarily associated with posterior cortical dysfunction, particularly in parietal regions essential for spatial processing31,53—exacerbated by tau and Aβ deposition that weakens position signal coding. Concurrently, the failure to actively suppress distracting glances implicates a breakdown of inhibitory control mechanisms governed by the prefrontal cortex.29,46 Neuroimaging evidence corroborates altered activation within these frontoparietal networks during fixation tasks in AD. 16
Although fixation parameters provide promising objective biomarkers for the early identification of AD, their clinical translation remains hampered by inherent challenges. Notably, fixation indices are susceptible to confounding factors such as aging-related physiological changes and comorbid eye disorders, which may compromise diagnostic specificity. To address this limitation, multi-modal integration strategies, including combining gaze metrics with CSF biomarkers or structural MRI data, are warranted to enhance diagnostic accuracy. Future research should focus on standardizing detection protocols to ensure cross-center reproducibility, establishing large-scale longitudinal databases to clarify the trajectory of fixation abnormalities throughout AD progression, and exploring the utility of fixation parameters for efficacy assessment in clinical trials of anti-AD therapeutics. These efforts will facilitate the successful translation of this non-invasive detection approach into routine clinical practice.
Microsaccades, small reflexive eye movements during fixation, may also demonstrate altered properties in AD. Studies have shown that the microsaccade parameters of AD patients may change with disease progression, including abnormalities in frequency, amplitude stability, and direction control16,18 (Table 3).
A comparative perspective aids differential diagnosis. The eye movement profile of AD, characterized by progressive fixation instability, contrasts with patterns seen in other disorders. PD, for instance, often features saccadic hypometria alongside movement-related fixation issues.29,43,54 Notably, patients with semantic dementia, a frontotemporal lobar degeneration subtype, frequently retain normal eye movement function, providing a key distinguishing feature from AD.46,53
The pathophysiology underlying microsaccadic changes in AD is not fully elucidated but likely involves the degradation of cortical networks responsible for predictive visual control. Pathology in visual and posterior parietal association cortices may disrupt the fine-tuning of these movements.31,53
As a potential biomarker, microsaccades are still in the research phase. In early AD, their sensitivity is insufficient, and they are susceptible to confounders (such as eye diseases, mental disorders), which limits ability as an independent diagnostic marker. Future research should focus on standardized detection protocols and explore combinatorial applications with CSF or imaging biomarkers to improve effectiveness in early AD diagnosis and disease monitoring.
Smooth pursuit dysfunction in AD patients
Smooth pursuit eye movements (SPEM), which allow the eyes to closely follow a moving target, are frequently impaired in patients with AD.31,53 These abnormalities emerge early in disease progression, correlate closely with cognitive decline, and have drawn attention for their potential role in AD's early assessment, though their diagnostic specificity is not uniformly high across studies.31,46,53
The core deficits in AD involve a reduction in pursuit gain and an increase in tracking error. 53 Empirical data show that AD patients exhibit significantly greater horizontal pursuit error compared to healthy controls (e.g., an increase of 2.92°). 46 Prolonged vertical pursuit latency has also been documented. 53 These abnormalities worsen as the disease advances. In the preclinical stage, no definitive, specific SPEM changes have been validated-subtle, non-diagnostic alterations may occur but lack predictive value for AD conversion.53,55 By the MCI stage, subtle deficits emerge: gain may decrease modestly, and tracking error begins to rise, though these changes are often less pronounced than saccadic or fixation abnormalities.31,46 The AD dementia stage brings severe SPEM dysfunction: tracking error increases substantially, gain further declines, and initial acceleration is severely compromised.46,53 This progressive pattern reflects the spread of neurodegenerative changes along visuomotor pathways, particularly involving posterior cortical and cerebellar-brainstem networks31,53 (Table 4).
SPEM changes in AD progression.
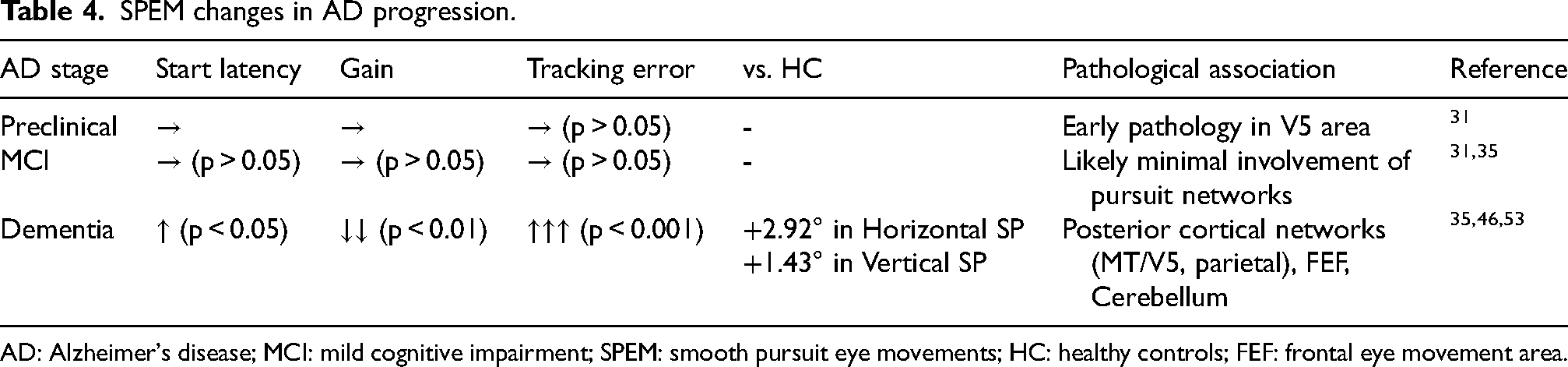
AD: Alzheimer's disease; MCI: mild cognitive impairment; SPEM: smooth pursuit eye movements; HC: healthy controls; FEF: frontal eye movement area.
Notably, SPEM impairment patterns differ across neurodegenerative diseases, conferring limited differential diagnostic value.46,53,54 PD patients exhibit reduced SPEM gain and increased saccadic intrusions, distinct from AD's prominent tracking error elevation. 54 bvFTD is characterized by decreased horizontal tracking gain (0.19 lower than controls, p = 0.031) but minimal tracking error increase, whereas AD shows marked error elevation across horizontal and vertical axes.46,53 These differences may assist in clinical differentiation but are not definitive in isolation 46 (Table 5).
Comparison of eye movement features in AD, PD, and FTD.
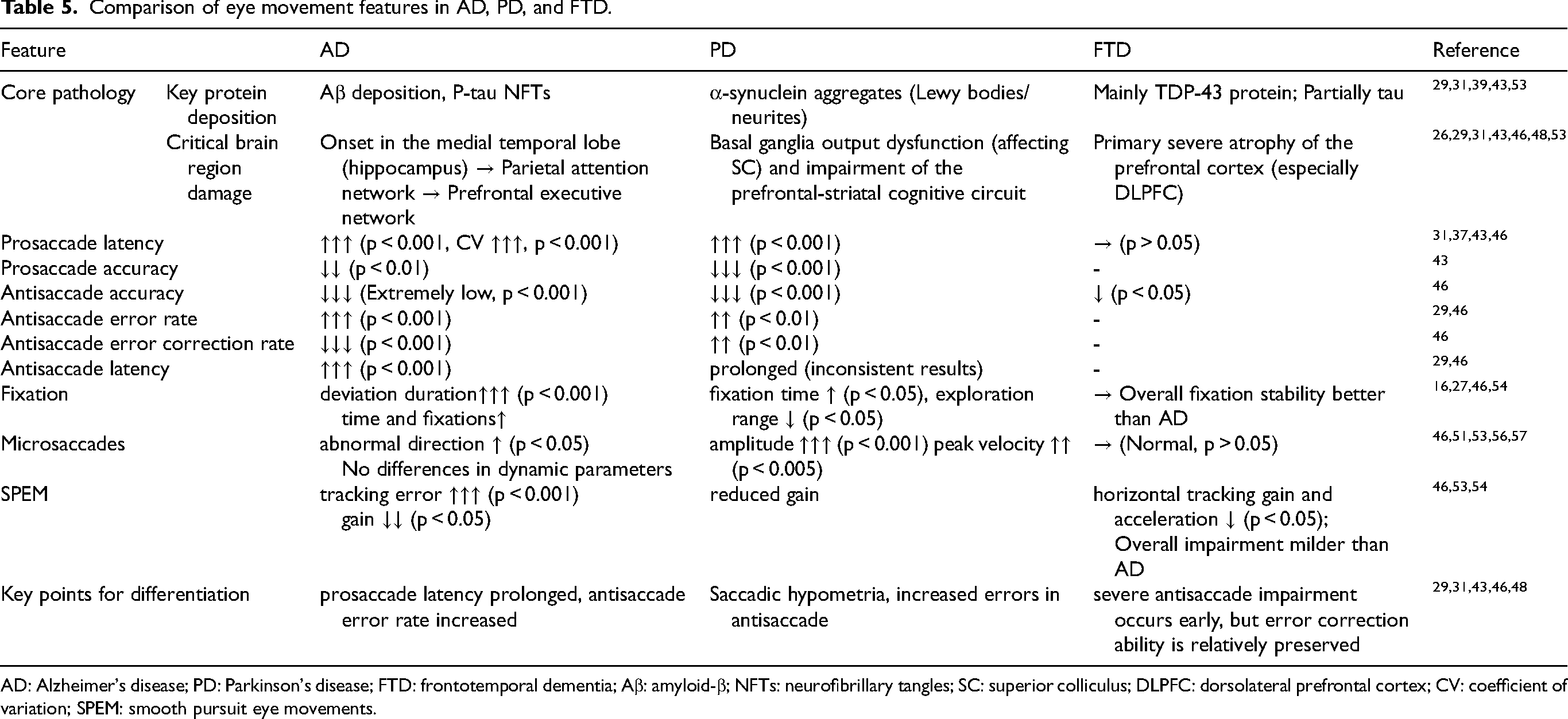
AD: Alzheimer's disease; PD: Parkinson's disease; FTD: frontotemporal dementia; Aβ: amyloid-β; NFTs: neurofibrillary tangles; SC: superior colliculus; DLPFC: dorsolateral prefrontal cortex; CV: coefficient of variation; SPEM: smooth pursuit eye movements.
The neural control of SPEM depends on a network encompassing visual cortical areas (e.g., MT/V5), the frontal eye fields, cerebellum, and brainstem nuclei.29,53 In AD, the observed decline in pursuit gain and acceleration is associated with dysfunction within this network, particularly involving frontal eye fields, medial temporal visual areas, and the cerebellum. 53 Widespread cortical neurodegeneration likely disrupts the neural circuits responsible for visual motion prediction and velocity matching. 31
As a potential auxiliary biomarker, SPEM assessment offers a promising direction for early screening and differential diagnosis in AD. It is suitable for large-scale population screening and could enhance diagnostic accuracy when integrated into a multimodal strategy alongside other biomarkers. However, current evidence is insufficient to support its use as a standalone diagnostic marker in routine clinical practice. Future work must prioritize the development of standardized testing protocols, the establishment of normative data from large samples, and longitudinal studies to clarify its prognostic value.
MCI-related potential eye movement biomarkers
MCI serves as a critical transitional stage between normal cognition and AD dementia, characterized by distinct eye movement abnormalities.26,30 These abnormalities exhibit predictive value for AD conversion, rendering them promising candidate non-invasive biomarkers to guide early intervention.31,40,48 The clinically relevant candidate eye movement biomarker panel for MCI centers on three core metrics: antisaccade error rate, prosaccade latency, and fixation stability-their combination yields superior diagnostic performance compared to single neuropsychological scales such as the Mini-Mental State Examination.40,46,48
Eye movement abnormalities in MCI reflect functional decline rather than overt loss of function.31,40 Key manifestations include prolonged prosaccade latency (p = 0.024), 30 increased antisaccade error rate (p < 0.001), 40 and elevated lateral fixation deviation (MCI group 16.00 times vs. healthy controls 13.00 times, p < 0.05). 16 Core eye movement functions-such as saccade execution and basic error correction-remain relatively preserved in MCI.30,31 In contrast, AD dementia is marked by severe functional disruption: loss of saccade direction control, inability to sustain effective smooth pursuit, and near-complete impairment of error correction.16,31 This shift from functional decline to overt dysfunction mirrors the gradual accumulation of AD-related pathology, enabling eye movement metrics to support both cross-sectional diagnosis and longitudinal disease monitoring31,40
The pathological specificity of MCI stage eye movement abnormalities enhances their clinical utility.31,51,53 These changes are closely linked to early tau deposition in the prefrontal cortex (particularly the DLPFC) and parietal cortex,31,48 as well as cholinergic system dysfunction. 38 Eye movement abnormalities in MCI are distinguishable from benign age-related physiological changes. For example, MCI patients exhibit oblique microsaccade direction (36.2 ± 11.7° deviation from horizontal) while healthy controls show horizontal dominance (27.6 ± 9.2°, p = 0.011) 51 -age-related changes lack such directional bias and pathological relevance.51,55 This distinction allows MCI eye movement parameters to identify individuals at high risk of progressing to AD, facilitating targeted early interventions.40,48 Multimodal integration of eye movement metrics optimizes diagnostic performance: antisaccade error rate offers high sensitivity, 40 prosaccade latency provides good specificity, and their combination yields an AUC of 0.77 (Gap paradigm) 40 which outperforms single eye movement indicators or traditional neuropsychological tests 40 (Table 6).
Summary of eye movement parameters in MCI.
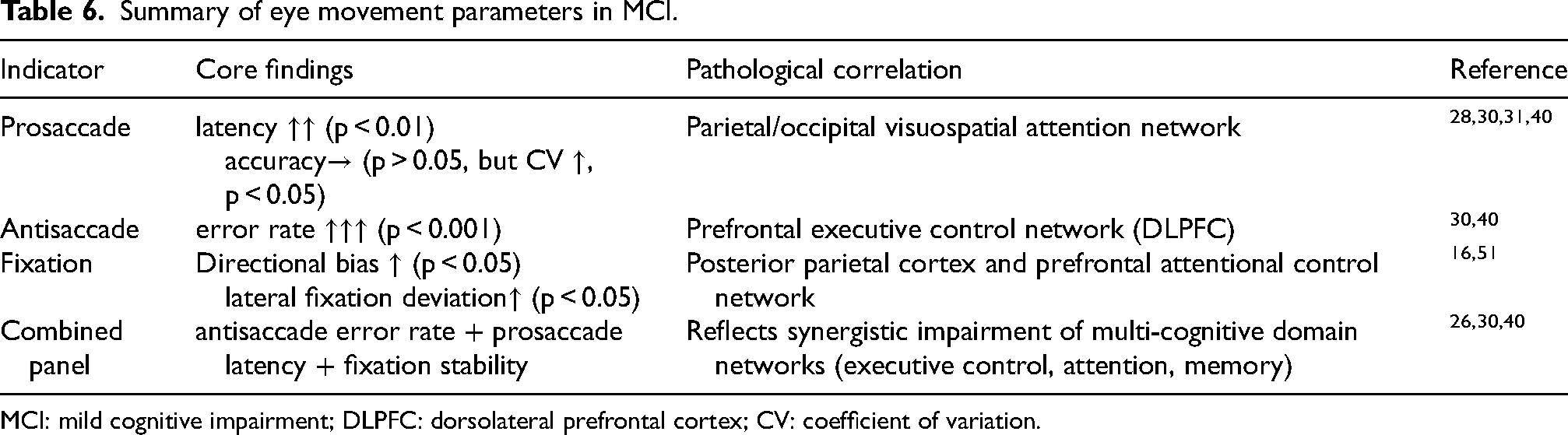
MCI: mild cognitive impairment; DLPFC: dorsolateral prefrontal cortex; CV: coefficient of variation.
Currently, the clinical translation of potential eye movement biomarkers faces challenges. Their diagnostic specificity may be influenced by age, attention, and comorbidities. Future research must focus on standardizing testing protocols, establishing normative data from large samples, and validating their predictive value for MCI-to-AD conversion through longitudinal studies.
Discussion and conclusion
Eye movement research holds great promise for early AD detection and monitoring. Yet the field faces limitations that hinder its clinical translation. These hurdles include sample selection bias, methodological heterogeneity, sparse longitudinal data, and variability in technical equipment. This systematic review pulls together evidence proving multi-modal eye movement abnormalities as reliable non-invasive biomarkers across the entire AD disease spectrum. Three key findings emerge from this synthesis. AD patients show eye movement deficits specific to disease stage. MCI features prolonged prosaccade latency, elevation in antisaccade error rate, and fixation stability decline. AD dementia worsens these anomalies: prosaccade latency becomes further prolonged, and antisaccade error rate rises to a higher level. These abnormalities tie mechanistically to Aβ/tau deposition, NFTs, and frontoparietal network disconnection. Eye movement parameters also aid differential diagnosis: AD differs from PD in progressive prosaccade latency prolongation (opposed to PD's multi-step saccade pattern) and from FTD in poor antisaccade error correction (versus FTD's retained correction capacity).
Besides pathological mechanisms involving Aβ, tau, and the cholinergic system,38,47 several neural circuits or networks are also implicated in the abnormal eye movements in AD. Eye movements rely on an extensive, hierarchical distributed neural network, 58 a complex system in human that requires the integration of sensory, motor, attentional, and executive processes.58–60 To date, no direct studies have identified a common or specific neural circuit impairment that underlying the diverse eye movement abnormalities observed in AD patients. Neuroimaging evidence has linked impaired smooth pursuit and prolonged saccade latency in AD patients to hypometabolism within the precuneus and middle temporal areas. 46 Additionally, poor performance on the antisaccade task in patients with MCI has been associated with reduced cortical thickness in the superior frontal gyrus, precuneus, and the angular gyrus. 42
Although abnormalities in eye movement parameters (e.g., antisaccade error rate) have been consistently observed in patients with MCI/AD,27,30,31,48,53 heterogeneity across multiple parameters persists, which limits the generalizability of these findings. Such heterogeneity is largely attributable to methodological variations in sample size, task design, patient population stratification, eye tracker models, and experimental equipment. For instance, one study reported significantly prolonged prosaccade latency in patients with MCI relative to healthy controls, 30 whereas another found no such difference in amnestic MCI (aMCI) in its primary analysis. 32 A key source of this discrepancy may lie in interstudy differences in patient populations. Indeed, several studies have reported that antisaccade impairments are prominent in aMCI but minimal in non-amnestic MCI (naMCI). 48 This suggests that failure to stratify MCI into its clinical subgroups may lead to differential detection of latency delays, with aMCI-enriched samples being more likely to reveal such delays. Beyond patient population characteristics, experimental paradigms also play a critical role in driving these heterogeneous results. For example, the overlap task employed requires greater cortical (parietal) engagement compared with the gap task, and this heightened cortical demand may render the overlap task more sensitive to early AD-related deficits.30,32 Most studies find no significant eye movement abnormalities in preclinical AD, while one study shows that prodromal AD patients exhibit poorer antisaccade accuracy than healthy controls in complex tasks. 48 These eye movement changes might stem from different pathological load in preclinical AD, the prodromal AD is defined as a later preclinical phase. 61
Eye movement abnormalities have emerged as promising non-invasive candidate biomarkers for the early detection, progression monitoring, and differential AD diagnosis, with accumulating preclinical and preliminary clinical evidence supporting their translational potential.26,51,53 Nevertheless, their clinical translation is hindered by interconnected challenges, including marked methodological heterogeneity, sample selection bias, sparse longitudinal data, inadequate disease specificity, high costs of specialized eye-tracking tools, and regulatory/clinical acceptance barriers.
The clinical translation and feasibility of eye movement measures need further research. Unifying equipment and task paradigms, eliminating confounding effects from aging and ocular comorbidities, and integrating with existing diagnostic workflows and multimodal biomarker frameworks can further enhance the standardization and clinical reliability of oculomotor candidate biomarkers.
Future research requires multicenter collaborations to validate results across diverse populations,62,63 developing AI-driven multimodal fusion models for extracting pathological signals,62,64 creating portable smart systems tailored for primary care settings, 62 and verifying ties between eye movement abnormalities and AD-specific neural circuit dysfunction.31,51,53
In summary, eye movement abnormalities hold promise as non-invasive biomarkers for AD, with potential for preclinical screening and differential diagnosis. To advance translation, future research should prioritize AI-driven multi-modal integration, standardized detection protocols, portable device development, and preclinical longitudinal validation.
Footnotes
Acknowledgements
Thanks for the technical support by the Core Facilities Platform, Health Science Center, Ningbo University, and the Laboratory Animal Center of Ningbo University.
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Zhejiang Key Research and Development Project (grant number 2024C03101), National Research and Development Project of China (grant number 2023YFF0724802), Ningbo Key Research and Development Project (grant number 2023Z173), Ningbo Science and Technology Plan Project (grant number 2025S168), and K.C. Wong Magna funded at Ningbo University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Not applicable