
Abstract
Background
Previous studies assessed the relationship between caregivers’ characteristics and caregiver burden. However, comprehensive evaluations of caregivers’ behavioral and psychological traits remain comparatively limited.
Objective
To explore the possible association between the cognitive and behavioral characteristics of caregivers of patients with Alzheimer's disease (AD) and the burden they experience, with a focus on sex/gender differences.
Methods
In this multicenter cross-sectional study within the SINdem “Sex and Gender Differences in Dementia” group, informal caregivers of non-institutionalized AD patients attending the Italian Memory Clinics were enrolled. Caregivers completed the Montreal Cognitive Assessment, Revised Scale for Caregiver Self-Efficacy, 20-Item Toronto Alexithymia Scale, Barratt Impulsiveness Scale-11, Brief COPE, 14-Item Resilience Scale, Ten-Item Big Five Inventory, Five Facet Mindfulness Questionnaire, Empathy Quotient–Short, and the Caregiver Burden Inventory. Sex was considered as a binary variable (female/male); gender-related dimensions were explored indirectly through caregivers’ behavioral and psychological characteristics.
Results
238 caregivers and 238 AD patients were enrolled. A higher burden was associated with more daily caregiving hours, lower self-efficacy, greater impulsivity, difficulties identifying feelings, acting without awareness, a stronger tendency to judge, and higher neuroticism. Female caregiver burden was associated with attentional/motor impulsiveness, lower mindfulness, lower resilience, and lower emotional empathy. Male caregivers showed associations with lower self-efficacy, greater reliance on emotion-focused coping, difficulties identifying feelings, lower non-judging, lower agreeableness, and reduced cognitive empathy.
Conclusions
Caregiver burden was associated with caregivers’ own behavioral and psychological profiles and sex, beyond patient-related factors. These findings support the importance of integrating sex/gender perspectives and targeted interventions into caregiver assessment and support.
Introduction
Dementia represents a leading public health issue affecting mainly older people, with Alzheimer's disease (AD) as the most common underlying cause. According to Alzheimer Europe, 1 the number of dementia cases is projected to double by 2050, particularly among people aged 65 years and over. Similarly, in Italy it is currently estimated that there are around 600,000 patients with AD.
Patients with AD have a gradual and irreversible decline in cognitive functions and loss of functional abilities, often accompanied by various neuropsychiatric manifestations such as delusions, hallucinations, sleep disturbances, and somatic complaints.2,3 The impact of dementia extends beyond the individual, profoundly influencing their relationships with informal caregivers, family members in particular. Informal caregiving, however, often present substantial challenges for families and friends of AD patients. This can lead to a subjective experience that reflects the caregiver's individual perceptions of social, physical, psychological, emotional, and financial stressors associated with caregiving, commonly referred to as “caregiver burden”.4,5 Notably, research indicates that caregivers of patients with AD experience a substantially higher burden than those caring for non-demented individuals, so much so that they have been often described as the “invisible second patients”. 6
Previous studies have consistently reported that caregiver burden is largely determined by patient-related factors, such as dementia severity, the care recipient's functional impairment, the presence of medical comorbidities, and disruptive behaviors (e.g., agitation, aggression, disinhibition).7–10 These behaviors can be difficult to manage, due to the potential adverse effects of medications, such as antipsychotics.11–12
While caregiver burden in dementia has been widely associated with caregiver sociodemographic factors (e.g., female sex and older age) and psychological variables (e.g., depression, anxiety, and coping strategies),13–15 evidence remains limited regarding caregivers’ broader behavioral and psychological traits (e.g., impulsivity, alexithymia, mindfulness, empathy, and personality), particularly with respect to sex/gender-specific patterns.
Moreover, unlike many patient-related drivers of burden (e.g., dementia severity or functional decline), several caregiver behavioral characteristics may be potentially modifiable and therefore represent actionable intervention targets. Constructs such as caregiving self-efficacy, coping style, mindfulness, and resilience can benefit from psychoeducational programs, skills training, and structured psychosocial interventions. From a clinical and policy perspective, identifying which caregiver profiles are most strongly associated with burden may support risk stratification, allocation of supportive resources, and the development of tailored interventions. At the same time, these potentially modifiable pathways may operate differently across male and female caregivers, underscoring the need to examine sex/gender-specific patterns.
Indeed, the aforementioned studies did not consider sex and gender-related factors that may influence the caregiver burden.13–15 Emerging evidence suggests that female caregivers of AD patients experience higher physical and psychological care burdens compared to their male counterparts. This disparity may also reflect the gender dimensions of caregiving, encompassing the socially constructed attributes associated with being a man or a woman, including traits, norms, behaviors, and roles traditionally ascribed to each. 16 Across the globe, women are the predominant providers of informal care. 17 Furthermore, women caregivers are more likely to provide care for parents, siblings, relatives, and friends, whereas men caregivers more often care primarily for their spouse. This distinction highlights that women are more frequently tasked with balancing caregiving alongside other responsibilities, such as professional work, household duties, and social commitments, compared to men. 18
Taken together, these observations highlight the importance of moving beyond patient-related factors that influence the caregiver burden and considering specific sex-gender characteristics of caregivers. To address these gaps, the present study aimed to investigate possible associations between caregivers’ burden for AD patients and their socio-demographic and cognitive/behavioral profiles, and to assess how these associations may differ between male and female caregivers.
Methods
Design and participants
The SexDemCare Multicentric Italian Study is a cross-sectional observational study designed and carried out within the Italian Neurological Association for dementia (SINdem) study group “Sex and Gender differences in Dementia”. From 1 May 2024 to 1 August 2025, a consecutive enrollment of informal caregivers of non-institutionalized AD patients, and their care recipients, referring to the participant Italian Neurological Centers for Cognitive Decline and Dementia (CDCDs) for a scheduled outpatient visit, was conducted. The study has been approved by the Ethical Committee of the Coordinator Center (Kore University of Enna, Umberto I Hospital, Enna, Italy, Protocol number 97/2024 CEL) and by the other participant centers, and it was in accordance with the Helsinki Declaration. Full written consent was obtained by all the participants, caregivers, care-recipients or, when applicable, their legal guardians. Eligible participants were Italian mother tongue informal caregivers of AD patients, aged ≥18 years, providing care for at least 6 months, and for at least 2 h per day, to ensure a stable and regular caregiving exposure, consistent with inclusion thresholds used in previous dementia caregiving studies.19,20
Exclusion criteria were less than 5 years of education and severe visual impairment, which could interfere with completing self-administered questionnaires.
Measurements
Caregiver's assessment
Data on socio-demographic factors (e.g., sex, age, education) and the caregiving relationship (e.g., cohabitation with the care recipient, number of hours spent caring per day, and relationship to the care recipient) were recorded in a study-specific Case Report Form (CRF).
The financial burden was evaluated through the “Economic Costs” subscale of the Cost of Care Index, which includes five Likert-type items assessing perceived financial strain, such as reduced standard of living, unaffordable expenses, and financial sacrifices related to caregiving. 21
Moreover, the overall cognitive functioning was assessed using the Montreal Cognitive Assessment (MoCA). 22 The following questionnaires were used: Revised Scale for Caregiver Self-Efficacy, 23 Toronto Alexithymia Scale-20 (TAS-20), 24 Barratt Impulsiveness Scale-11 (BIS-11), 25 Coping Orientation to Problems Experienced Inventory (Brief-COPE), 26 14 item Resilience Scale (RS-14), 27 10-Item Big Five Personality Scale (10-BFI), 28 Five Facet Mindfulness Questionnaire (FFMQ), 29 Short-Empathy Quotient (EQ-Short), 30 Caregiver Burden Inventory (CBI) 31 (Supplemental Table 1).
AD patient's assessment
As for caregivers, data on socio-demographic factors (e.g., sex, age, education) and medical history (e.g., age at dementia onset, disease duration, AD therapy, medical comorbidities) were recorded. Moreover, the overall cognitive functioning was evaluated through the Mini-Mental State Examination (MMSE),32,33 and the following questionnaires/clinical scales were administered: Activities of Daily Living (ADL), 34 Instrumental Activities of Daily Living (IADL), 35 Clinical Dementia Rating Scale (CDRS), 36 (Supplemental Table 1).
Statistical analysis
Continuous variables were expressed as mean and standard deviation (SD) and compared with the T-test. Categorical variables were expressed as counts and percentages and compared using the chi-square test. In case of missing values, no imputation was performed, and variable distributions were reported using available cases.
Since no established cut-offs exist for the CBI, for logistic regression analysis, the total CBI score was dichotomized at the sample median, and caregivers were classified into those with CBI ≤ the median and those with CBI > the median. Univariate logistic regression was performed to evaluate possible associations between caregiver burden (outcome) and caregivers’ socio-demographic, cognitive, and behavioral characteristics. A multivariate analysis was performed. Given that ADL impairment and “hours spent caring per day” directly reflect care demands and are known determinants of caregiver burden, these variables were considered a priori confounders. A sex-stratified analysis was carried out. Sex was analyzed as a binary variable (female/male). Gender identity, roles, and norms were not directly assessed; therefore, any references to gender are conceptual and based on caregivers’ psychological/behavioral characteristics, rather than on validated measures of gender identity or gender roles. Odd ratios and 95% confidence intervals were reported. p-value<0.05 were considered significant. Given the exploratory nature of our approach and the potential for false negatives with a strict Bonferroni correction, only uncorrected p-values were reported. 37 Data were analyzed with STATA v.18.
Results
Two hundred thirty-eight caregivers [157 (65.9%) women, mean age 59.6 ± 12.4 years, mean education 12.6 ± 3.9 years] and 238 AD patients [153 (64.3%) women, mean age 77.5 ± 7.9 years, mean education 8.5 ± 4.3 years, mean disease duration 4.2 ± 2.5] were enrolled.
Concerning AD patients, 199 (84.3%) were treated with anti-dementia drugs. Among them, 61 (26.9%) patients with rivastigmine, 49 (21.8%) with donepezil, 4 (1.8%) with galantamine, and 123 (53.9%) with memantine. One-hundred and fifteen (70.1%) patients had hypertension, 29 (17.8%) diabetes, and 35 (21.2%) heart disease (atrial fibrillation, previous myocardial infarct). The MMSE mean score was 16.5 ± 7.4, the ADL mean score was 4.1 ± 1.8, IADL 3.1 ± 2.4. The CDR was available for 223 AD patients: 37 patients (16.5%) had CDR=0.5; 62 (27.8%) had CDR=1; 65 (29.1%) had a CDR=2; 53 (23.8%) had CDR=3; 6 (2.7%) had CDR=4.
Concerning caregivers, 88 (37.4%) were the care recipients’ spouses, 134 (57%) were adult children, and 13 (5%) were cousins. Thirty-seven (19.8%) were tobacco users, 156 (82.9%) were moderate coffee drinkers, and 53 (28.6%) were alcohol drinkers. Socio-demographic and behavioral characteristics of caregivers are shown in Table 1.
Socio-demographic, cognitive, and behavioral characteristics of caregivers.
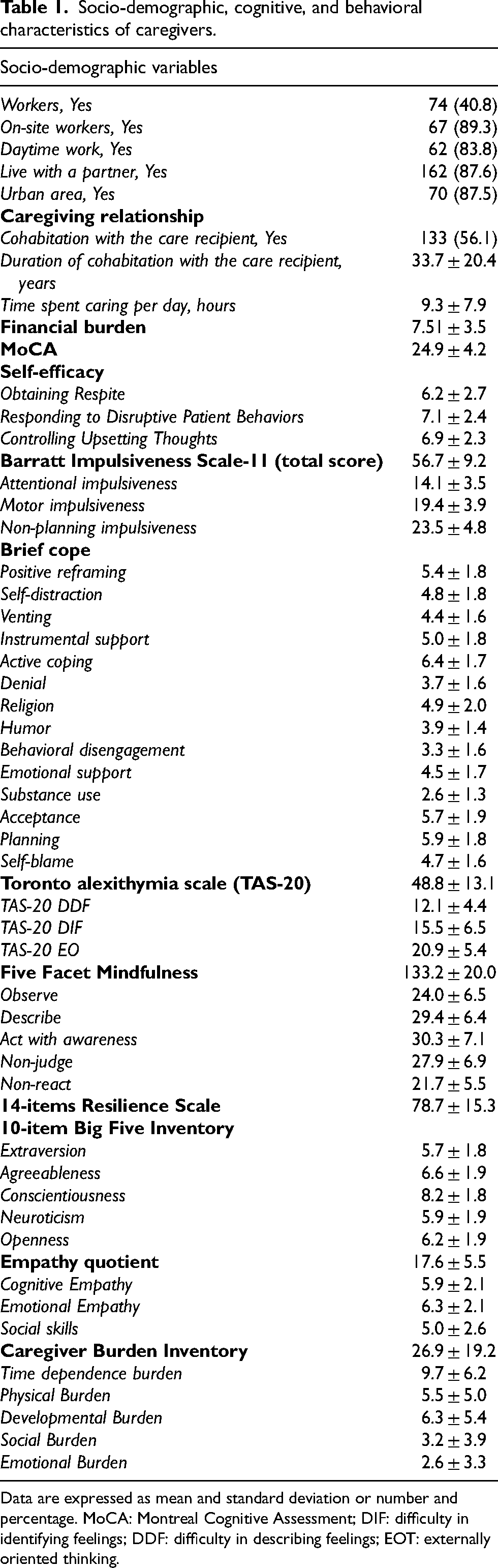
Data are expressed as mean and standard deviation or number and percentage. MoCA: Montreal Cognitive Assessment; DIF: difficulty in identifying feelings; DDF: difficulty in describing feelings; EOT: externally oriented thinking.
One-hundred and fifteen caregivers (48.1%) experienced high burden CBI >23. In the univariate analysis, high burden was significantly associated with several caregivers’ characteristics; the strongest associations were observed for some sub-items of self-efficacy, impulsiveness, and mindfulness. These associations were also confirmed in the multivariate analysis, adjusting for ADL and time spent in caregiving per day, considered a priori confounders (Table 2).
Characteristics of caregivers according to level of burden.
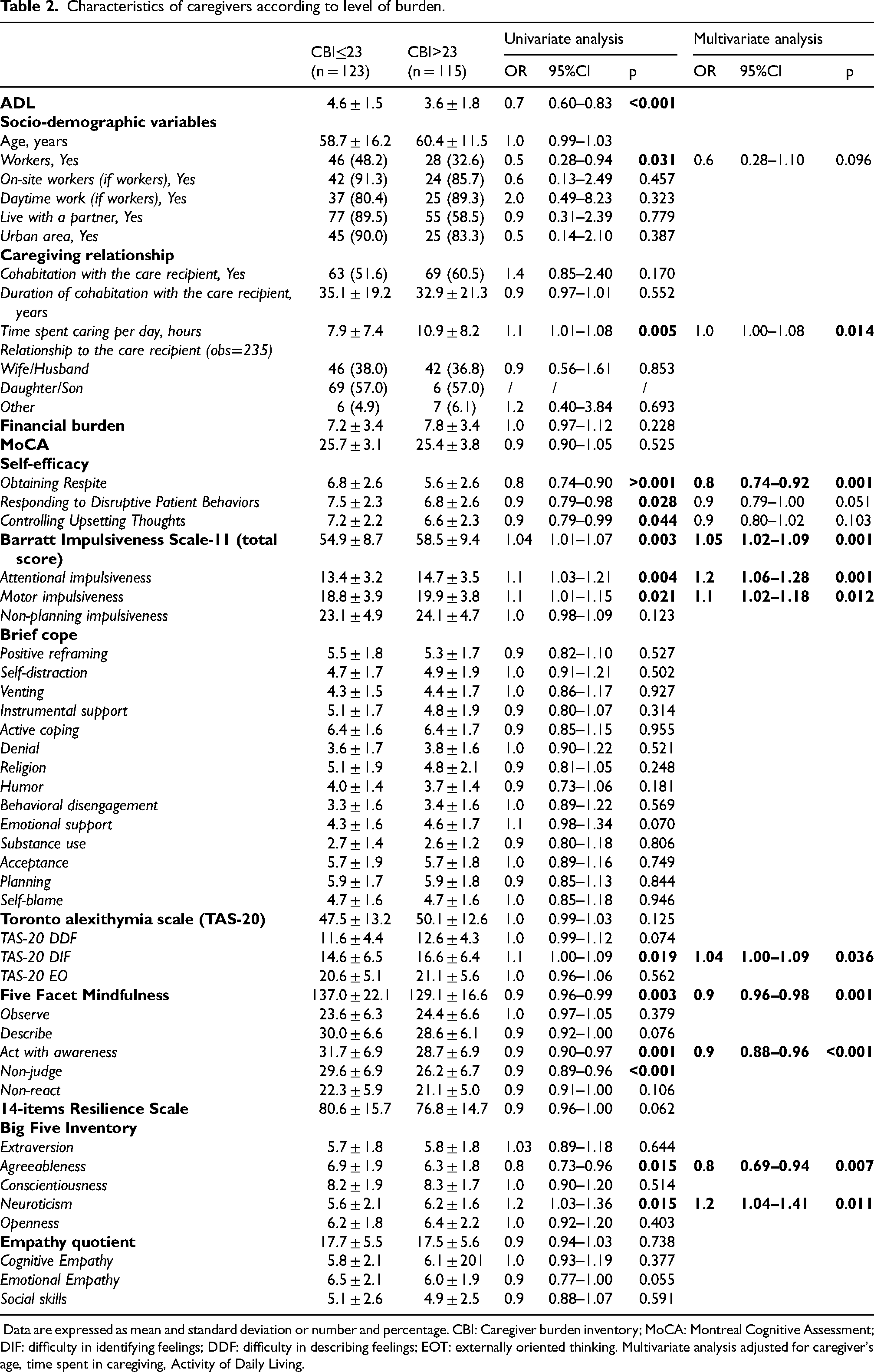
Data are expressed as mean and standard deviation or number and percentage. CBI: Caregiver burden inventory; MoCA: Montreal Cognitive Assessment; DIF: difficulty in identifying feelings; DDF: difficulty in describing feelings; EOT: externally oriented thinking. Multivariate analysis adjusted for caregiver's age, time spent in caregiving, Activity of Daily Living.
Regarding sex differences, females were younger than males (57.4 ± 11.0 versus 63.7 ± 13.8, p < 0.001) and experienced a higher burden (28.8 ± 20.1 versus 23.2 ± 17.0, p = 0.033; Figure 1). Moreover, compared to men, women reported lower self-efficacy in obtaining respite, mindfulness abilities (particularly acting with awareness and non-judging), and resilience. However, women scored higher on the self-distraction sub-item of the brief-cope scale, lower externally oriented thinking, and higher on emotional empathy (Table 3).
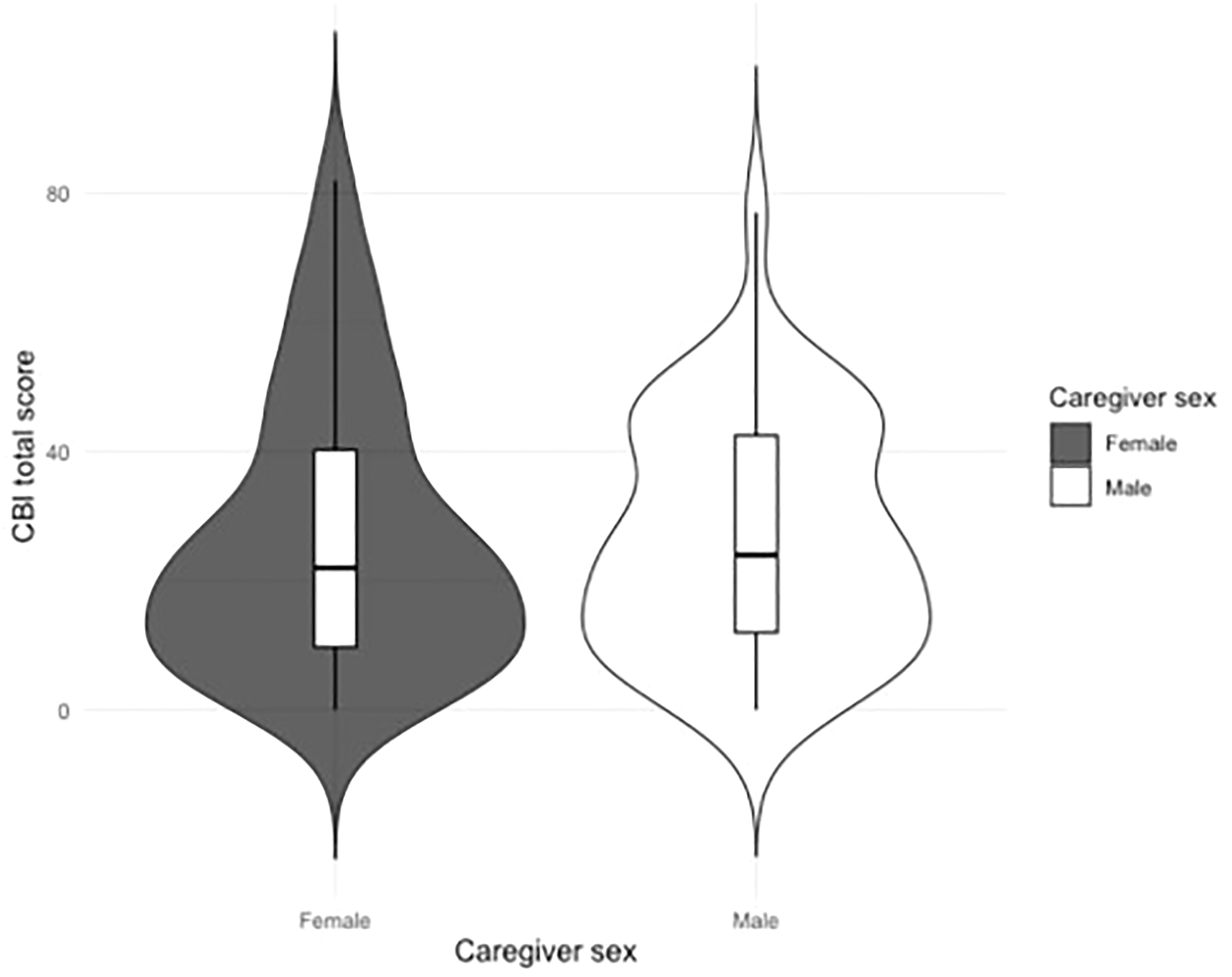
Caregiver Burden Inventory in females and males. The violin plot shows the distribution of total Caregiver Burden Inventory (CBI) scores by caregiver sex. The central boxplots represent median values and interquartile ranges, while the surrounding violins display the density of score distributions. Female caregivers show higher and more variable burden scores compared to male caregivers.
Characteristics of caregivers according to sex/gender.
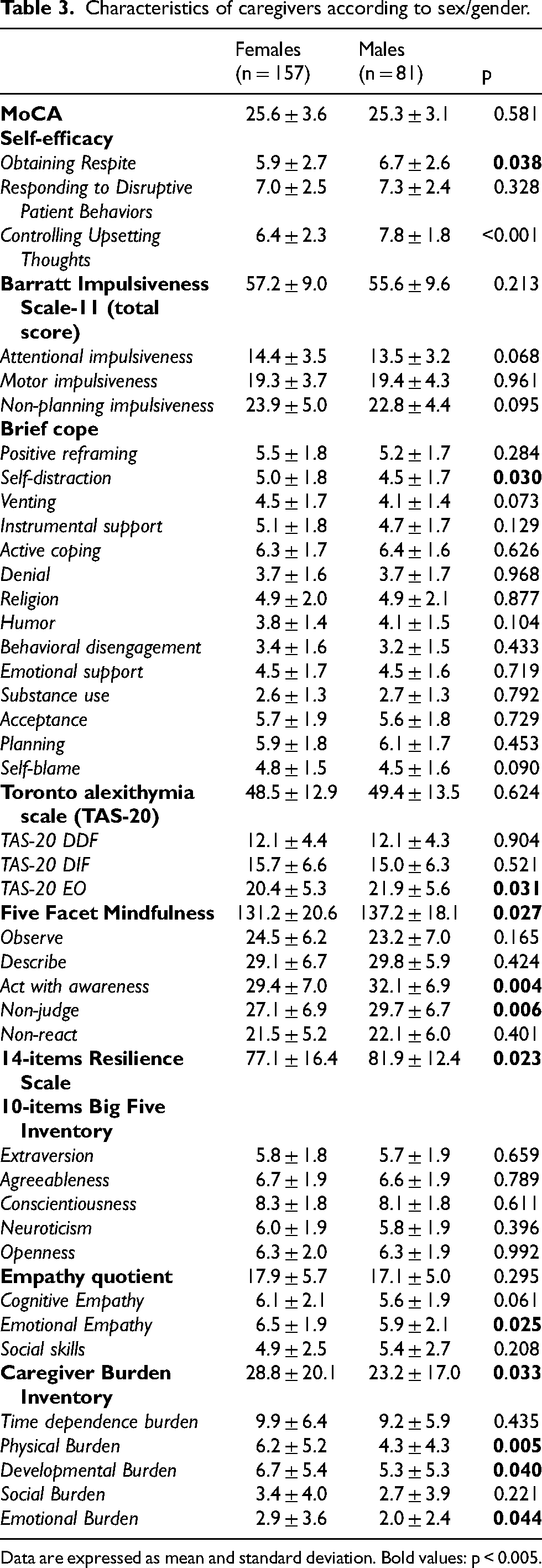
Data are expressed as mean and standard deviation. Bold values: p < 0.005.
In the sex-stratified analysis, in the female group, burden was significantly associated with several caregiver characteristics; the strongest associations were found for attentional impulsiveness (p = 0.003) and low emotional empathy (p = 0.011). These associations were confirmed at the multivariate analysis (Table 4, Supplemental Table 2).
Socio-demographic, clinical, and behavioral characteristics of women caregivers and burden experienced.
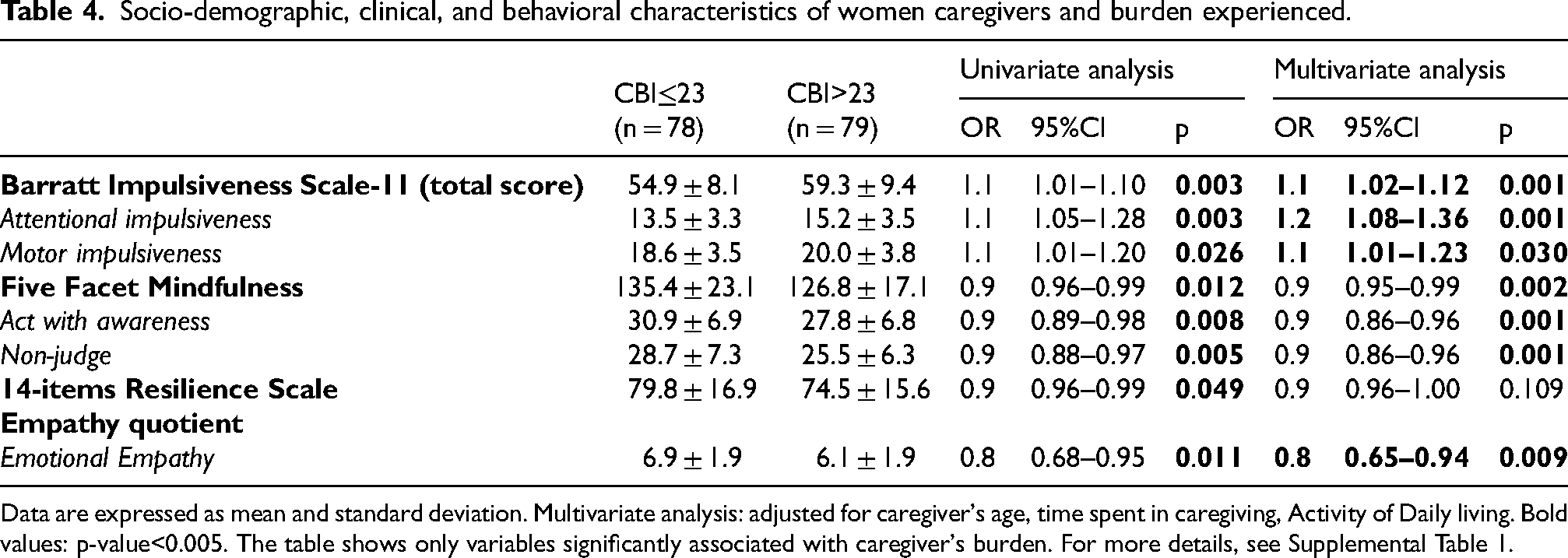
Data are expressed as mean and standard deviation. Multivariate analysis: adjusted for caregiver's age, time spent in caregiving, Activity of Daily living. Bold values: p-value<0.005. The table shows only variables significantly associated with caregiver's burden. For more details, see Supplemental Table 1.
In contrast, within the male group, caregiver burden was strongly associated with low self-efficacy in obtaining respite (p < 0.001) and managing disruptive patient behavior (p = 0.013), difficulties in identifying emotions (p = 0.010). All these associations were confirmed in the multivariate analysis (Table 5, Supplemental Table 3).
Socio-demographic, clinical, and behavioral characteristics of male caregivers and burden experienced.

Data are expressed as mean and standard deviation. Multivariate analysis: adjusted for caregiver's age, time spent in caregiving, Activity of Daily living. Bold values: p-value<0.005. The table shows only variables significantly associated with caregiver's burden. For more details see Supplemental Table 2.
Discussion
This multicentric Italian study explored the role of cognitive/behavioral and socio-economic determinants in the burden experienced by caregivers of patients with AD, with a focus on sex and gender differences.
According to previous studies,38,39 the high prevalence of burden, with nearly half of caregivers reporting elevated levels of distress, was confirmed in our sample. Caregiver burden has long been conceptualized as a multidimensional construct, encompassing physical, psychological, emotional, social, and financial stressors. 4 Traditionally, the severity of the patient's dementia, functional decline, behavioral disturbances, and comorbidities have been recognized as the primary drivers of caregiver strain.7,39,40 Our findings are consistent with this evidence, as both the time spent caregiving and the patient's functional abilities (ADL) were strongly associated with burden. However, these clinical factors alone do not fully capture the complexity of the caregiving experience. Some studies indeed emphasize the role of caregiver-related psychological determinants, such as coping styles, mood, resilience, and personality traits, in modulating burden.13,41,42 In our study, a high burden was associated with impulsivity, alexithymia, low mindfulness, low resilience, maladaptive coping, and certain personality dimensions (low agreeableness, high neuroticism). These findings support the assumption that caregiver burden arises not only from external demands but also from the interaction with individual psychological vulnerabilities and resources.
A longitudinal study by Fang et al. found that caregiver neuroticism was associated not only with greater caregiver burden but also with higher level of physical and psychological abuse, supporting the importance of implementing caregiver-centered intervention. 42 Similarly, Vespa et al. reported an association between problematic personality traits (e.g., poor self-care and inability to care for oneself) and caregiver burden in a small sample of caregivers. 43
An underexplored factor contributing to caregiver burden is alexithymia, defined as a difficulty in identifying and describing emotions, along with a tendency toward externally oriented thinking. 44 To date, no studies have specifically investigated the role of alexithymia in the burden experienced by caregivers of patients with AD, highlighting a significant gap in the literature. Emotional awareness and regulation are critical when managing the progressive cognitive and behavioral decline characteristic of AD. Alexithymic caregivers may have limited emotional insight, potentially impairing their ability to employ adaptive coping strategies and thereby increasing stress. Supporting this notion, studies of relatives of patients with traumatic brain injury have shown that alexithymia, and specifically the difficulties in describing feelings and a preference for concrete, externally oriented thinking, is strongly associated with emotional exhaustion and burnout. 45 Similarly, studies on partners of individuals with multiple sclerosis reported that alexithymia may be linked to negative and potentially dysfunctional illness perceptions. 46 Extending these findings to the AD context is warranted, as unrecognized or unaddressed alexithymia may not only amplify subjective caregiver burden but also reduce the caregivers’ capacity to provide effective emotional support and guarantee clear, empathetic communication with the patient. 47
In the present study, high caregiver burden was associated with greater caregiver impulsivity. This finding is clinically relevant as impulsivity can hinder the use of effective coping strategies and the regulation of emotional responses in stressful caregiving situations. 48 Caregivers with high impulsivity are more likely to react strongly to behavioral disturbances in patients with AD, experience greater interpersonal conflict and struggle in maintaining consistent routines. 49 These challenges can, in turn, heighten the perceived burden of care. Additionally, impulsivity has linked to lower frustration tolerance and increased stress reactivity, which may contribute to emotional exhaustion over time. Overall, these findings suggest that impulsivity represents a potential vulnerability factor that influences how caregivers perceive and manage the care demands, ultimately affecting their well-being and the quality of care they provide.
Moreover, in our sample, we found an association between resilience and burden. To date, only a few studies have explored this relationship, often reporting that caregivers with higher resilience experience lower burden and are more likely to use adaptive coping strategies and effective decision-making, which may mitigate stress.50–52 Finally, in the present study, a relationship between caregiver burden and mindfulness was also found. Mindfulness, defined as the practice of maintaining awareness and fully experiencing the present moment without judgment, has been investigated in relation to caregiver outcomes, with inconclusive results. 53 While some studies failed to confirm this relationship, large caregiver cohorts have shown that higher mindfulness scores are dynamically associated with better cognitive and emotional outcomes in both patients and caregivers.54,55
The sex-stratified analyses revealed notable differences: as commonly reported across cultures, female caregivers experienced a significantly higher burden than male caregivers.18,56,57 Previous studies have suggested that this data may be related to the greater difficulty women experienced in balancing caregiving responsibilities with daily activities.18,58 However, to the best of our knowledge, the literature on sex-related cognitive and behavioral determinants of caregiver burden remains limited. In our sample, among female caregivers, burden was associated with impulsivity (particularly attentional and motor impulsiveness), low resilience, reduced mindfulness (acting with awareness, non-judging), and diminished emotional empathy. These findings suggest that female caregivers may experience caregiving as more emotionally taxing, characterized by challenges in emotion regulation and in maintaining adaptive coping strategies. It is also important to note that previous research has shown that women are more likely to rely on emotion-focused coping and ruminative styles, which may exacerbate subjective distress.59,60
By contrast, male caregivers showed a different pattern: burden was linked to lower self-efficacy in managing caregiving demands, coping strategies based on emotional support, lower agreeableness, difficulties in identifying feelings, and reduced cognitive empathy. This profile indicates that men may perceive burden more in terms of inefficacy in role performance and difficulties in managing interpersonal and behavioral aspects of care. This finding is consistent with prior evidence suggesting that men tend to use more problem-focused coping, but when these strategies are perceived as insufficient, they may experience a sense of failure or helplessness.61,62
Our findings have several clinical implications: first, our results suggest that interventions should be tailored to the caregiver's sex and psychological profile. For women, interventions promoting mindfulness, resilience, and emotional regulation may be particularly effective, whereas for men, training programs aimed at enhancing self-efficacy, problem-solving skills, and cognitive empathy could help in reducing perceived burden and improve coping strategies in men.
The multicenter design, relatively large sample size, and the comprehensive evaluation of cognitive/behavioral dimensions represent the strengths of this study. However, some limitations should be noted. First, the generalizability of the findings may be limited by recruitment from specialized memory clinics, the inclusion of only Italian native speakers, and the exclusion of caregivers with fewer than 5 years of education. Moreover, the cross-sectional design prevents causal inference, and reverse causation (i.e., higher burden influencing caregiver-reported traits/behaviors) cannot be excluded. However, several behavioral characteristics are often considered relatively stable over time; thus, it is possible to hypothesize that some behavioral characteristics may predispose caregivers to a higher burden. Longitudinal studies are needed to confirm our findings. Furthermore, the extensive assessment battery might also have increased respondent fatigue, potentially affecting data quality. However, most of the tests were self-administered, and in cases of fatigue, no time limits were imposed on completing the questionnaires. Moreover, several constructs assessed (e.g., mindfulness, resilience, coping strategies, and personality traits) may partially overlap conceptually and statistically, raising the possibility of shared variance/collinearity that could complicate the interpretation of specific associations. Furthermore, reliance on self-reported measures may introduce biases, despite the use of validated instruments. Additionally, most caregivers were assisting patients with a CDR between 0.5 and 2, which did not allow us to analyze caregiver burden stratified by the care recipient's disease severity. Nevertheless, we included ADLs in the multivariate analysis, considering them a priori confounders to account for differences in care intensity. Dichotomizing caregiver burden at the median may reduce statistical power; moreover, given the number of predictors examined, the risk of Type I error cannot be excluded despite the exploratory nature of the study. In addition, sex was assessed only as a binary variable (female/male), and we did not collect validated measures of gender identity, roles, or norms; therefore, the findings should be interpreted as sex-specific associations and may not generalize to broader gender diversity. Finally, although previous studies have supported the existence of health disparities (i.e., higher prevalence of mood disorders, suicide risk, stress) among sexual and gender minority (SGM) populations, the present study did not assess SGM caregivers; thus, generalizability to these groups is limited and should be addressed in future studies. 63
In conclusion, in the SexDemCare study, caregiver burden was strongly influenced by caregivers’ own psychological characteristics, and these determinants differed between sexes. These findings underscore the need to integrate sex and gender perspectives into both research and clinical practice. Tailoring interventions to the caregiver's psychological profile and gendered experience may help reduce burden, enhance well-being, and ultimately improve the care provided to individuals with AD. Our findings support a more personalized approach to caregiver burden, in which routine clinical pathways incorporate a brief caregiver assessment. Using short, validated instruments to screen domains such as self-efficacy, impulsivity, emotion identification, mindfulness facets, and coping style may help identify caregivers at higher risk of burden and inform tailored psychosocial support. For example, low self-efficacy in obtaining respite may indicate the need for enhanced education and case-management support; maladaptive coping may point to problem-solving–based interventions; and reduced mindfulness/acting with awareness may suggest mindfulness-based or attention-regulation training.
This is particularly important given the dyadic nature of dementia care: when caregivers are healthier and less burdened, patients themselves experience better quality of life and more stable symptoms throughout the trajectory of AD. Longitudinal studies are needed to clarify temporal relationships and potential bidirectional effects, and intervention studies are required to determine whether targeting these caregiver characteristics can meaningfully reduce burden and improve caregiver outcomes.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261435213 - Supplemental material for Cognitive and behavioral determinants of burden in caregivers of patients with Alzheimer's disease: A focus on sex and gender. The SexDemCare Multicentric Italian Study
Supplemental material, sj-docx-1-alz-10.1177_13872877261435213 for Cognitive and behavioral determinants of burden in caregivers of patients with Alzheimer's disease: A focus on sex and gender. The SexDemCare Multicentric Italian Study by Antonina Luca, Tommaso Piccoli, Alice Tomaselli, Salvatore Di Marco, Alessandra Nicoletti, Daniele Lo Coco, Elena Rolandi, Stefano L. Sensi, Patrizia Sucapane, Amalia Cecilia Bruni, Daniela Perani, Biancamaria Guarnieri and in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We would like to thank the patients and their caregivers for contributing to the study.
Ethical considerations
The study has been approved by the Ethical Committee of the Coordinator Center (Kore University of Enna, Umberto I Hospital, Enna, Italy, Protocol number 97/2024 CEL) and of the other participant centers and it was in accordance with the Helsinki Declaration.
Consent to participate
Full written consent was obtained by all the participants, caregivers, care-recipients or, when applicable, their legal guardians.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The dataset used and analyzed during the current study is available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.