
Abstract
Background
Previous work has shown that proper name recall from the Logical Memory (LM) task is sensitive to PET and cerebrospinal fluid biomarkers of Alzheimer's disease (AD) in older adult populations. These findings indicate potential utility in identifying preclinical AD.
Objective
The purpose of this study is to validate previous findings of the association of proper name recall and blood-based plasma pTau217.
Methods
Participants came from the Wisconsin Registry for Alzheimer's Prevention study. We fit linear mixed effects models of longitudinal LM and proper name recall as a function of most recent pTau217 values. Follow-up analyses added interaction terms to models for group differences in sex and APOE ε4 allele carriage. As an exploratory aim, logistic regression models were used to examine if proper name recall aided in predicting clinical diagnosis.
Results
Participants with higher concentrations of pTau217 showed a steeper decline on both conventional LM and proper name recall. APOE ε4 allele carriers with higher concentrations of pTau217 showed a greater decline in longitudinal task performance, while there was no significant interaction for sex, indicating that men and women with high pTau217 show similar rates of decline.
Conclusions
Our findings validate that proper name recall is sensitive to blood-based pTau217. Measuring proper name recall may be an efficient marker assessing early cognitive change that could be leveraged when designing future cognitive tests.
Introduction
The accumulation of Alzheimer's disease (AD) pathology, amyloid-β plaques (Aβ) and neurofibrillary tau tangles, lead to cell death and symptoms of cognitive decline and dementia.1,2 These neuropathological changes accumulate an estimated 10–20 years prior to the onset of cognitive symptoms.3–5 The ability to identify and monitor at-risk individuals would aid in determining who might benefit from interventions and assist in monitoring clinical trials. The benefits and utility of anti-amyloid immunotherapy treatments are still being explored, as are the potential side effects of such treatments.6,7 As such, it could be useful for clinicians and patients to have easy to use tools at their disposal to adopt a watchful-waiting approach to determine when would best suit them to begin treatment. Two possible targets that may assist with identifying the early-stage changes are lexical-semantic measures, such as the proper names derived from the Logical Memory task, and blood-based biomarkers.
Previous studies from our lab have found that poor recall of proper names from the Logical Memory task are more sensitive than total delayed recall and other cognitive measures to AD biomarkers, measured in both cerebrospinal fluid (CSF) 8 and positron emission tomography (PET) biomarkers, 9 in cognitively unimpaired participants. These findings suggest that although participants are cognitively unimpaired, they may be in early stages of decline that traditional tests may not reflect. These changes in proper name recall are possibly due to the patterns of early AD pathology accumulation overlapping with brain regions responsible for proper name recall, both of which occur in the left and right anterior temporal lobe and parahippocampal gyri.10–14 Utilizing proper names as a measure of semantic memory has several other potential advantages. For example, it is a simpler measure (range: 0–9) that can be derived from the Logical Memory Story Recall from the Wechsler Memory Scale, 15 which is commonly utilized in memory clinic settings. Additionally, the task of remembering and retelling a short story including names of people and places is an ecologically valid measure of an everyday activity and may better represent communication-related declines in episodic and semantic memory. Finally, proper names compose a metric that could be collected remotely, reducing participant burden and improving access to research studies.
The rise of blood-based biomarkers has also been of crucial interest to the AD research community for the same goal of improved access. Several plasma phospho-tau (pTau) species have emerged in recent years that have shown promise in detecting AD biomarkers in blood. 16 Of these species, pTau217 has been shown to be closely related to AD disease progression. 17 Plasma pTau217 has outperformed magnetic resonance imaging (MRI) features in identifying AD pathology18,19 and performed comparably to CSF biomarkers in detecting PET biomarker positivity. 19 In addition, pTau217 has also demonstrated sensitivity in more diverse populations, 20 further highlighting its potential clinical utility. Together, these variables could be useful in clinical settings to track possible preclinical disease changes: with proper name recall as an early indicator of cognitive decline, and plasma pTau217 as a confirmation of biomarker status.
In addition to validating the association of plasma pTau217 and proper name recall, we sought to explore potential moderators of this relationship. The first moderator we considered was sex. Previous work from our lab has shown that while females tend to perform better on both Logical Memory total and proper name recall, their overall rate of decline is similar to that of males. 21 Additionally from this study, there was not a significant interaction of age x a four-level sex & amyloid PET status variable, indicating that there was no difference in longitudinal performance between amyloid positive males and females. 21 Given that we have more plasma biomarker data available than PET biomarkers due to the ease and cost-efficiency of blood draws compared to gold-standard PET scans, we sought to test this trend with a larger sample size.
The second moderator we considered was APOE ε4 allele carriage. The impact of APOE ε4 on AD progression is well established: it is a major risk factor for AD in both men and women in middle- to late-adulthood. 22 The presence APOE ε4 allele(s) increases the risk of AD: for those with one copy of the allele by three to four times; homozygous carriers are twelve to fifteen times more likely to develop AD.23–26 While increasing the likelihood of developing AD, this allele also tends to accelerate decline in executive function, memory, processing speed, and attention prior to a diagnosis of AD.27–30 Given this accelerated trajectory of decline seen in APOE ε4 carriers, we sought to determine if APOE ε4 status might differently impact the longitudinal trajectories of those with differing levels of plasma pTau217.
In this study, we investigate whether longitudinal proper name recall is associated with plasma pTau217, thereby validating our prior investigations with AD PET and CSF biomarkers (Aim 1). Due to the strong correlation between pTau217 and other AD biomarkers used in previous studies on proper name recall, we hypothesized that proper name recall will be similarly associated with pTau217. Our second aim examined whether sex or APOE ε4 allele status moderated the longitudinal trajectories of proper name recall. Of these potential moderators, we hypothesized that sex would not moderate the longitudinal trajectories of proper name recall by pTau217 concentration, and that APOE ε4 allele status would, such that carriers with higher concentrations of pTau217 would have the most dramatic decline in proper name recall over time. Lastly, in an exploratory aim (Aim 3), we tested whether inclusion of the proper names score improved stepwise logistic regression models predicting concurrent cognitive impairment. We hypothesized that the inclusion of proper name recall would improve predictive power of logistic regression models.
Methods
Sample
Participants were drawn from the Wisconsin Registry for Alzheimer's Prevention Study (WRAP), an ongoing longitudinal cohort of late-middle aged participants enriched for family history of AD. 31 Recruitment for WRAP requires that participants do not have a prior diagnosis of dementia or evidence of dementia upon completing baseline assessment. Participants in the WRAP study perform cognitive testing every two years, completing a cognitive battery that takes approximately two hours. Blood draws occur at every cognitive testing visit. The current participants were drawn from the November 2023 semi-annual data freeze. Participants were included in this analysis if they: (1) had item-level Logical Memory data available, (2) had plasma pTau217 data available, (3) had a normal diagnosis at their baseline visit, and (4) had no reported history of epilepsy, MS, Stroke, and Parkinson's disease (Figure 1, n = 805).
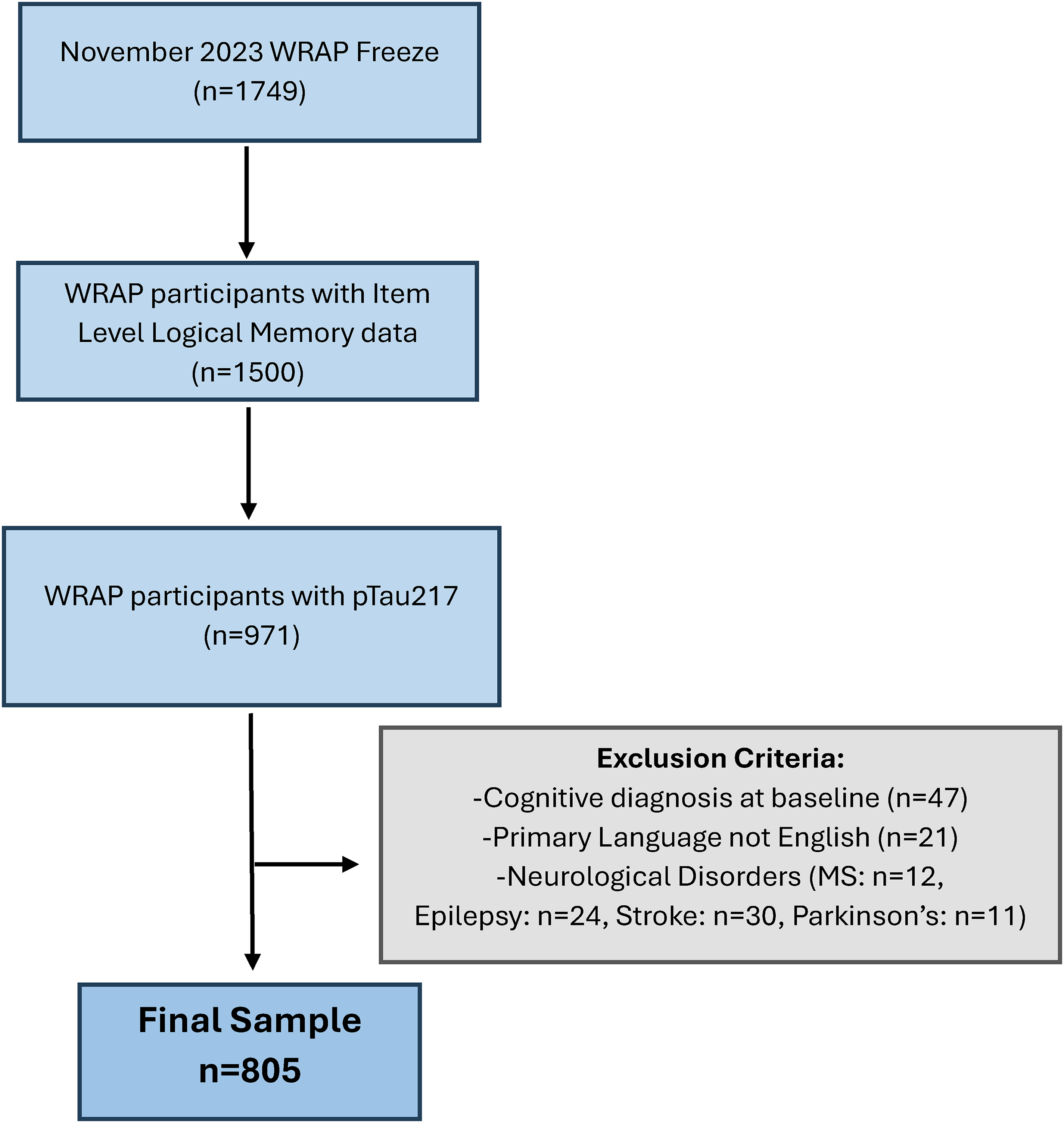
Consort diagram of inclusion criteria.
Logical memory
Total scores
Our outcome of interest was the Weschler Memory Scale-Revised, Logical Memory, 32 a standardized, norm-referenced neuropsychological test that evaluates learning and episodic memory. We considered the total score from stories A & B combined for both immediate and delayed recall trials (0–50 points possible for each immediate and delayed). Given our particular interest in proper name recall, these items were removed from the total score models (adjusted range: 0–41).
Proper names
The WRAP study first added the Logical Memory task to the test battery in 2007. In 2018, efforts began to enter item-level data to consider particular lexical categories of idea units. From this effort, we were able to create a sum of participants’ recall of proper names from these two stories (range 0–9, further details of these items located in Supplemental Table 1).
AlzPath plasma pTau217
EDTA plasma samples were analyzed using AlzPath pTau217 Simoa assay on a Quanterix HD-X. The assay uses a proprietary monoclonal p-tau217 specific capture antibody, N-terminal detector antibody, and peptide calibrator. This assay has been shown to have high accuracy in predicting abnormal amyloid-beta PET signal in the WRAP cohort, with an AUC of 0.93, CI: (0.90, 0.97). 19
Cognitive status determination
Cognitive status is determined via a two-step review process. All participants are screened using an algorithm that flags participants that may be showing signs of cognitive decline by comparing both their test scores and their study partner questionnaire scores against thresholds defined using empirical composites,33,34 robust norms,34,35 and/or absolute criteria for impairment. 36 The participants that are not flagged are determined to be cognitively unimpaired-stable, while the charts for participants who are flagged by the algorithm are reviewed by a multi-disciplinary team including neuropsychologists, nurse practitioners, geriatricians, psychometricians, and others, who assign a cognitive status that take into account neuropsychological test scores, prior performance, biomarker and medical history, and other pertinent information. These participants are diagnosed as either cognitively unimpaired-stable, cognitively unimpaired-declining, mild cognitive impairment (MCI), or dementia. 36
Statistical analysis
Statistical analyses were performed using R (Version 4.4.3). 37 Linear mixed effects (LME) models were fit using the lme4 package 38 to elucidate the longitudinal relationship of Logical Memory total score and proper name recall with most recent plasma pTau217. For each aim's analyses, separate models were fit for Logical Memory total score, as well as for the proper name scores, from the immediate and delayed recall tasks. Outcome scores from Logical Memory were transformed into z-scores.
Aim 1 and Aim 2 analyses
In Aim 1, we used LME models to investigate how Logical Memory total scores and proper name recall change over time when including interactions for linear age x continuous pTau217 concentration. LME models included random effects for participant-level intercepts. Fixed effects included in the models were gender, linear and quadratic age (centered at mean = 63.08), and baseline WRAT-III standard reading score. To account for possible practice effects, the number of previous exposures to the Logical Memory task (n visit – 1) were included in our models. Centered age accounted for both participants’ age at visit and varying time between visits per participant. To ensure the overlap in time-variance of both variables of age and practice effects were not introducing high levels of multicollinearity, we checked the variance inflation factor (VIF) of all models and did not find any indication that these measures were highly correlated with each other (VIF < 5.0), potentially due to subtle differences between participants in follow up time between visits.
Aim 2 analyses added 3-way interactions to the Aim 1 models to explore whether Logical Memory or proper names trajectories were moderated by pTau217 and either sex or APOE ε4 status (0 = no alleles, 1 = 1 or more alleles). The sex x pTau217 concentration x age and binary APOE ε4 x pTau217 concentration x age were tested in separate models for each logical memory outcome.
For graphing the LME models, we utilized cutoffs proposed by Ashton and colleagues to view participant characteristics by levels of pTau217 in a meaningful way, such that pTau217 values less than 0.4 pg/mL were considered “low”, values between 0.4–0.63 pg/mL were “intermediate”, and values above 0.63 pg/mL were “high.” 19 We selected the median value for each of these categories as the pTau217 concentration in figures.
Aim 3 analysis
In Aim 3, we compared a set of six models to investigate which model best explained risk of a concurrent cognitive diagnosis (defined as either MCI or dementia) at their most recent available Logical Memory visit. The model set includes a base model consisting of covariates, the base model plus most recent pTau217 concentration, and 4 additional models, each of which adds one logical memory predictor to the base + pTau217 models. We excluded participants who had diagnoses unrelated to AD (n = 2); we also removed 1 participant who was missing delayed recall scores to ensure equal n's across models to compare AIC (total sample: n = 802, n with a clinical diagnosis = 35, 4.3% of the included sample). We performed stepwise models to compare the additive effects of our predictors of interest as follows:
Base model: covariates only (centered age (linear), sex, and WRAT-III reading score) Base model + pTau217 Base model + pTau217 + proper names immediate Base model + pTau 217 + proper names delayed Base model + pTau217 + random 9-items from Logical Memory immediate Base model + pTau217 + random 9-items from Logical Memory delayed
We used AIC criteria to determine which model had the best fit, comparing models 1, 2, 3, and 5 for the immediate recall condition and models 1, 2, 4, and 6 for the delayed recall condition. We did not consider the Logical Memory total score in these analyses, as inclusion would be circular since the score is also used to aid in diagnosis. In lieu of the total score, we selected 9 random items from Stories A & B (Supplemental Table 1) to compare with the proper name inclusion in models to see if proper names specifically were helpful in aiding diagnosis.
Results
Demographics
Participant characteristics by categorical pTau217 level 19 are displayed in Table 1. Over half of our participants had low (<0.4 pg/mL) plasma pTau217 concentration values (n = 492, 61.1%) at their most recent plasma assay. The sample is majority female (70.4%) and white (93.4%), with high levels of education (mean = 15.8 years, sd = 2.26), and a mean baseline Logical Memory age of 58.6 (sd = 6.72). The sample's overall average age at their blood draw visit was 67.9 years (sd = 7.35).
Participant characteristics overall and by most recent plasma pTau217.
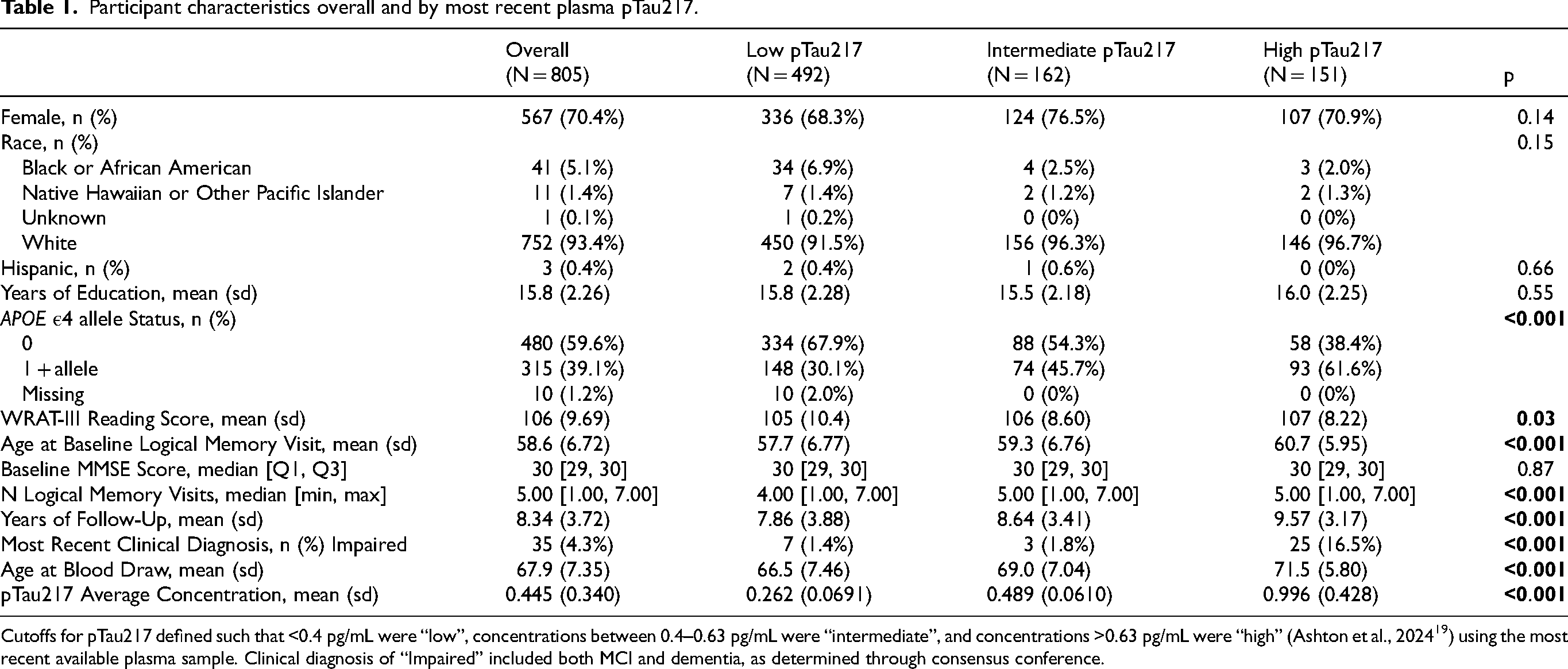
Cutoffs for pTau217 defined such that <0.4 pg/mL were “low”, concentrations between 0.4–0.63 pg/mL were “intermediate”, and concentrations >0.63 pg/mL were “high” (Ashton et al., 2024 19 ) using the most recent available plasma sample. Clinical diagnosis of “Impaired” included both MCI and dementia, as determined through consensus conference.
Aim 1: Validation of association between Logical Memory and proper names with pTau217
Linear mixed effects model results can be seen in Table 2 for the Logical Memory total and proper names. We observed similar trends across the total scores and proper name recall for both immediate and delayed recall. For the immediate recall outcomes, there was a significant interaction between linear age and pTau217 (total score: β = −0.04, p < 0.001; proper names: β = −0.03, p < 0.001). For the delayed recall outcomes, there was similarly a significant interaction between linear age and pTau217 (total score: β = −0.05, p < 0.001; proper names: β = −0.04, p < 0.001). The predicted scores of these interactions between age and pTau217 are displayed in Figure 1 and indicate that participants with higher concentrations of pTau217 perform worse over time on the Logical Memory task for both the total score and proper names.
Aim 1: Age x pTau217 LME model results.
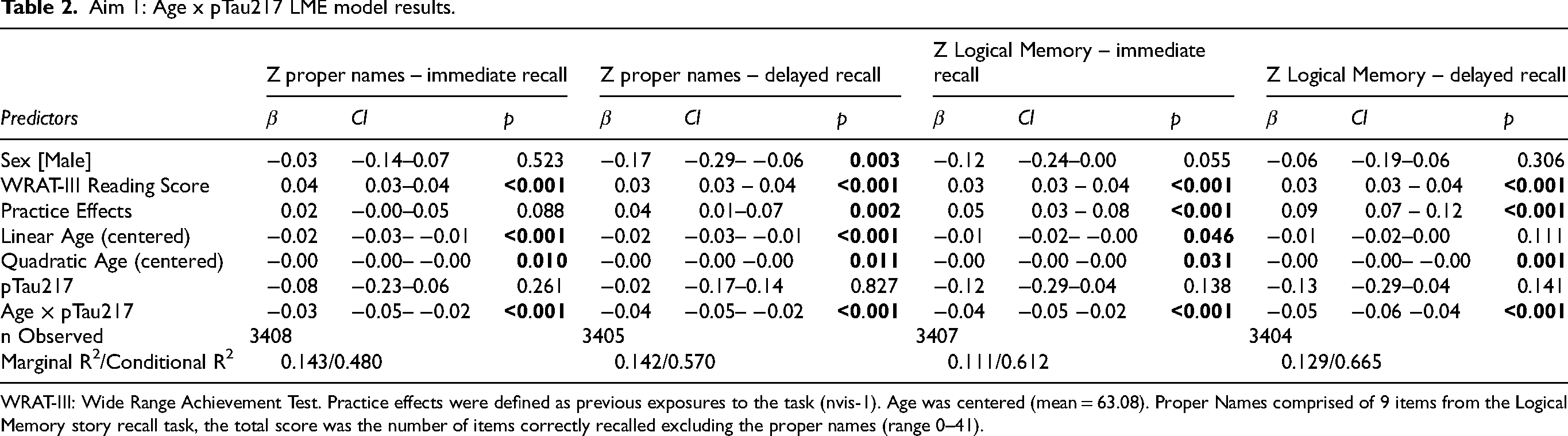
WRAT-III: Wide Range Achievement Test. Practice effects were defined as previous exposures to the task (nvis-1). Age was centered (mean = 63.08). Proper Names comprised of 9 items from the Logical Memory story recall task, the total score was the number of items correctly recalled excluding the proper names (range 0–41).
Aim 2: Sex x pTau217 x age interaction
Linear mixed effects models displaying the addition of sex to our primary models’ interaction can be seen in Supplemental Table 2. In our models, the three-way interaction terms were not statistically significant (β range = −0.03 – −0.01, p-value range = 0.06–0.66). Simple slopes from our models indicated that task performance decreased at higher levels of pTau217 similarly for males and females; all simple slopes of age were negative, indicating decreased performance with each in unit increase in age (Supplemental Figure 1).
Aim 2: APOE ε4 status x pTau217 x age interaction
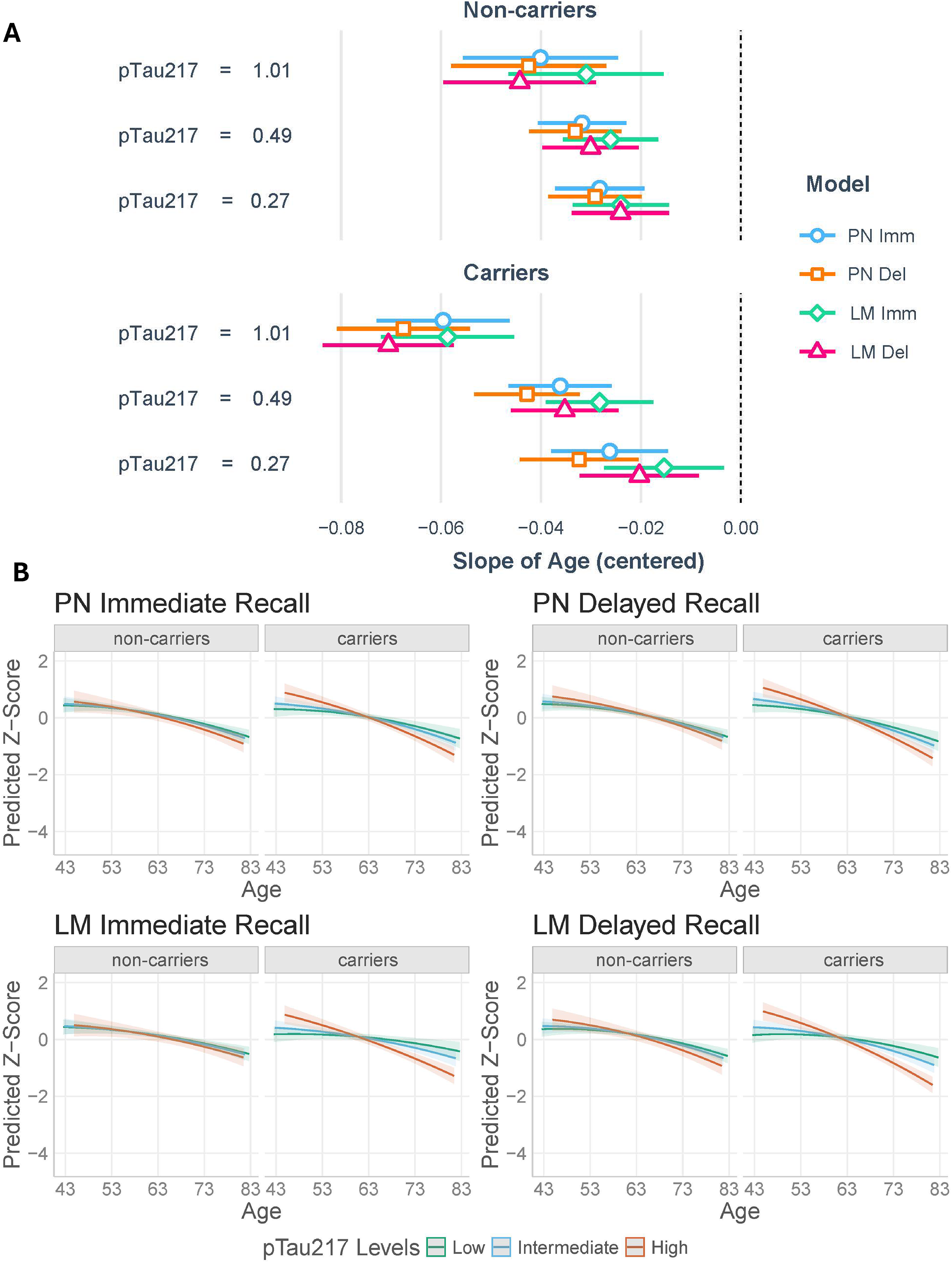
Of our total sample, n = 795 participants had APOE ε4 allele data available (Table 1). The three-way interaction of APOE ε4 allele status x pTau217 x age was statistically significant for all proper name and Logical Memory total score outcomes (Table 3, β range = −0.05 – −0.03, p-value range: <0.001–0.04). Simple slopes (Figure 2) from our models indicate that APOE ε4 allele carriers with higher concentrations of pTau217 showed a greater decrease in task performance (simple slopes: proper name and total score immediate recall β = −0.06; proper name and total score delayed recall β = −0.07) compared to non-carriers with higher pTau217 (simple slopes: proper name immediate, proper name delayed, and total score delayed recall β = −0.04, total score immediate recall β = −0.03).
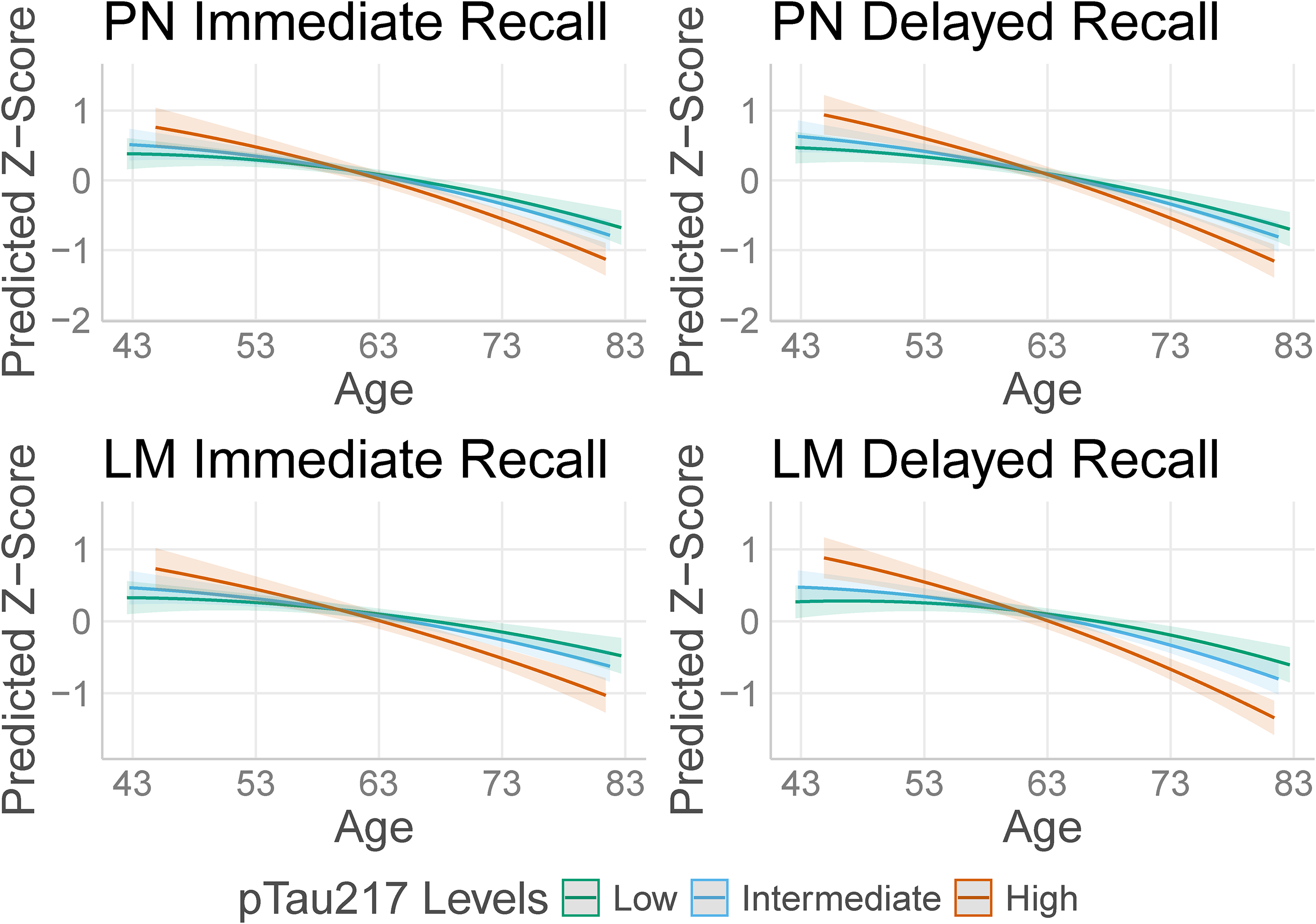
Aim 1 analysis: Age x pTau217 LME model interaction plots.
Aim 2 analysis: APOE ε4 allele status x pTau217 x age interaction model results.
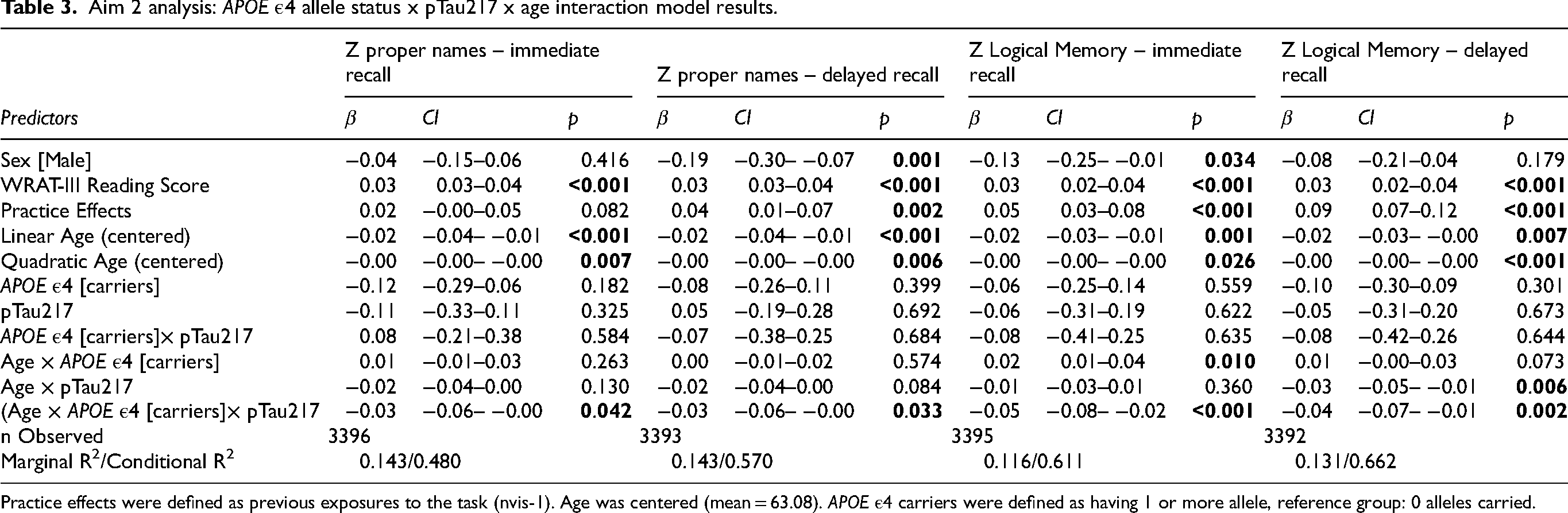
Practice effects were defined as previous exposures to the task (nvis-1). Age was centered (mean = 63.08). APOE ε4 carriers were defined as having 1 or more allele, reference group: 0 alleles carried.
Exploratory analysis (Aim 3): Logistic regression models predicting clinical diagnosis
The results from our logistic regression models can be seen in Table 4. The models containing our covariates, pTau217, and the proper names scores had lower AICs (AICImmediate = 211.48, AICDelayed = 177.97), indicating a better fit compared to our base model (AIC = 271.03) and our covariate + pTau217 model (AIC = 225.89). Our randomly selected items from the Logical Memory task (Supplemental Table 1) performed better compared to proper name recall (AICRand_Immediate = 200.21, AICRand_Delayed = 169.17), indicating that this random selection of items improved model fit the most. Using a rule of thumb of ΔAIC <10 being equivalent, 39 we found that the random-item score outperformed proper names for immediate recall (ΔAICRand_Immediate−PN_Immediate = 11.27), but performed equivalently with proper names for the delayed recall condition (ΔAICRand_Delayed−PN_Delayed = 8.8). In post-hoc analyses to aid interpretation of these results, we examined the Spearman correlations between the total delayed recall score and each of these two predictors; the correlation with proper name delayed recall was 0.75 (95% CI: 0.72, 0.78) and the correlation with the 9-item random subset was 0.78 (95% CI: 0.75, 0.80).
Logistic regression model results: predicting clinical diagnosis.
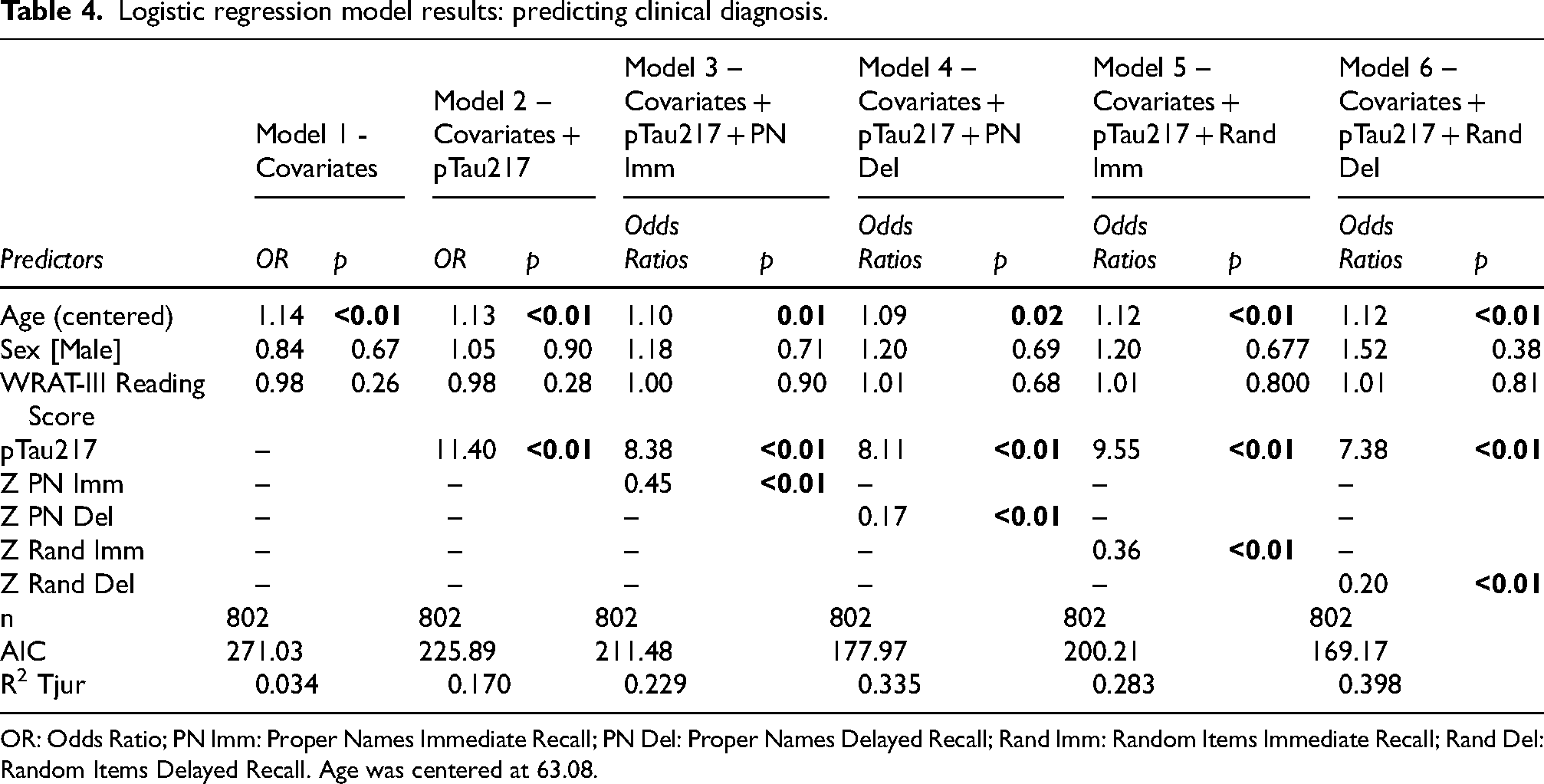
OR: Odds Ratio; PN Imm: Proper Names Immediate Recall; PN Del: Proper Names Delayed Recall; Rand Imm: Random Items Immediate Recall; Rand Del: Random Items Delayed Recall. Age was centered at 63.08.
Discussion
This study examined the relationship between plasma pTau217 concentration and longitudinal performance on two different measures derived from the Logical Memory task: the traditional total score, and a metric based on the lexical category of proper names recalled in late-middle-aged adults who were unimpaired at their baseline visit. The main finding was that participants with higher concentrations of pTau217 showed a more rapid rate of decline in both Logical Memory total scores (adjusted range 0–41) and proper name recall (range 0–9) over the course of the study. We did not find that sex moderated these relationships significantly, but APOE ε4 allele status did, such that participants with higher values of pTau217 and at least 1 copy of the APOE ε4 allele declined faster on average compared to participants with high values of pTau217 and no ε4 alleles. We also explored the potential clinical utility of pTau217 concentrations and proper names scores in predicting a clinical diagnosis of either MCI or dementia and found that a model including both pTau217 and the proper names scores performed better than base models with just covariates and pTau217 values by AIC criteria (Figure 3).
Aim 2 analysis: APOE ε4 allele status x pTau217 x age model results.
Aim 1: Validation of proper names in pTau217—Logical Memory and proper name recall trajectories were moderated by pTau217 concentration
The results of our primary aim examining the relationship between pTau217 and longitudinal Logical Memory and proper names scores validated our labs’ previous findings utilizing other AD biomarkers. Our previous findings indicated that proper names were sensitive to CSF 8 and PET biomarkers. 9 Due to the high correlation between pTau217 and these other previously examined biomarkers,18,19,40,41 we expected to see similar results. All four of our models showed that both Logical Memory total score and proper names followed similar patterns of decline, with participants with higher pTau217 declining faster over time on both immediate and delayed measures, indicating that both learning and memory are impacted by biomarker positivity. A similar decline in memory and language in relation to pTau217 has been noted in other studies using multi-test composite scores. 42 Other process scores, alternative ways of scoring and examining common neuropsychological tests, have been used from Logical Memory, such as one study that showed forgetting the story across the immediate and delayed time was a better predictor of pTau217 cross-sectionally compared to the total score. 43
Our work is unique in that we are only using single task scores in each of our models and finding the Logical Memory scores, both the total scores and the proper names, are sensitive to these differences. One possible reason for the sensitivity of proper names to AD biomarkers is due to the shared location of proper name recall and early neuropathology accumulation in the anterior temporal lobe and parahippocampal gyri.10–13 On the contrary, recall of proper names is a common memory complaint in older, otherwise cognitively healthy adults. 44 Proper name recall is more difficult than common name recall, regardless of age, and often elicits a tip-of-the-tongue phenomenon.45,46 It is possible that proper name recall is more generally taxing on the brain itself, as was demonstrated by Pelamotti and colleagues through their study examining the impact of higher altitude, and thus lower oxygen levels, negatively impacting proper name recall but not common name recall. 47 Early stages of AD pathological changes impacting these shared locations of proper name recall may make compensatory efforts to recall proper names more challenging, and thus impact those individuals more than those without significant accumulation of AD pathology. Gaining insight into how AD pathology exacerbates difficulties in recalling proper names may reveal additional neural mechanisms underlying the semantic memory system in both aging and disease. Future research will examine regional amyloid, tau, and neurodegeneration (particularly in the temporal pole and parahippocampal gyri, as well as in broader AD-related regions of interest) to further understanding of these mechanisms. Altogether, our findings indicate the potential strength of proper name recall. In our study, longitudinal proper name decline was similar to the overall total of the Logical Memory task, despite consisting of fewer items, which highlights its potential as an efficient, sensitive lexical-semantic measure of episodic memory. The awareness of the efficiency of proper names could be further utilized in designing new neuropsychological tests by potentially increasing the number of and/or better dispersing proper names throughout story recall tasks to assess if position effects are also impacting the proper names, which is another factor that has been observed in biomarker positive individuals through loss of primacy between immediate and delayed recall conditions. 48
Aim 2: Sex did not moderate Logical Memory and proper name recall trajectories
Previous studies have shown that females generally tend to perform better at baseline on Logical Memory tasks compared to males.49,50 Additionally, a previous study from our group showed no statistically significant sex differences in longitudinal trajectories by amyloid PET status, 21 which has also been shown on story recall in other biomarkers among older cohorts.51,52 Similarly, our results showed the interaction term of sex x pTau217 x age failed to reach a statistically significant p-value (<0.05) for both the Logical Memory total score and the proper name recall. However, the total score p-values were nearing significance (p-values <0.10), which warrants further study to better understand the longitudinal trajectories by sex.
Aim 2: APOE ε4 allele status moderated Logical Memory and proper name recall trajectories
Previous studies have shown the impact of APOE ε4 allele status, particularly within participants who carry two copies of the gene. 53 Further, the Logical Memory delayed recall score has been shown to decrease more rapidly in APOE ε4 allele carriers. 54 We anticipated that our results would show that allele carriers would decline more rapidly on Logical Memory total and proper names scores, particularly those that had higher values of pTau217. Our findings support this, with the carriers declining more rapidly on both measures than non-carriers.
Aim 3: Proper name score is associated with risk of clinical impairment
Given our previous findings regarding the associations between proper names and AD biomarkers, we anticipated that inclusion of proper names in our logistic regression models would improve the prediction of cognitive diagnosis, though we have not previously explored the associations of proper names recall with cognitive diagnosis. One caveat to this analysis is the small sample size of those with a clinical diagnosis: 802 participants were included in this analysis, but only 4% (n = 35) of these participants had a clinical diagnosis at their most recent visit. Our models indicated that including proper names improved the fit of the logistic regression models, as measured by AIC, compared to base models that only used demographics and plasma pTau217 concentration. However, when we tested additional models that included nine randomly selected items from the Logical Memory task, proper names performed worse on the immediate recall task, indicating that the initial learning of the random nine items better predicted clinical impairment compared to the proper names, and showed roughly equivalent performance (AIC difference < 10) 39 on the delayed recall task, indicating that memory performance was equivalent between the two when predicting clinical impairment.
This pattern likely reflects the nature of MCI-related memory impairment and the episodic memory tests used to diagnose MCI. Previous work from our group examined the difficulty of recalling individual items from the Logical Memory task, 55 so it is possible that the random nine items were more difficult to recall than the proper names, better mimicking the overall test score. Additionally, this previous study found that the largest discrepancy in remembering between the immediate and delayed conditions were the first two items from each story, all of which are proper names. Furthermore, two of the items from the random nine items selected in our analyses (Story B, items 5 & 16) improved in recall from the immediate to the delayed condition, which did not occur for any of the proper names. 55 The changes in difficulty between the immediate and delayed conditions for the specific items assessed may have made the composite scores more similar in difficulty. This could explain why the nine random items predicted MCI diagnosis better than proper names in the immediate recall condition, whereas in the delayed recall condition, the AIC difference was not large enough to indicate that one model was clearly superior.Additionally, post-hoc analyses showed that these nine items were more strongly correlated with the Logical Memory total score than proper names. Because the Logical Memory total score, along with other episodic memory measures, informs MCI status, it is logical that these nine items provided better predictive power for MCI. We also hypothesize that proper name recall may not be as predictive of clinical progression, and instead might be more sensitive to early, subtle changes in cognition. This sensitivity could stem from the aforementioned overlap between brain regions responsible for proper name recall and early neuropathology accumulation.10–13 It is also possible that proper names are not more sensitive to disease progression than the Logical Memory total score. Instead, the specific idea unit of proper names, which has been shown to be associated with biomarkers in a way that other idea units are not, 9 may perform comparatively to the total score, with its primary advantage being greater efficiency (9 items versus 50 items).
While story recall tasks have shown sensitivity to cognitive decline and the development of AD biomarkers, our novel measure of proper name retrieval performs similarly to the total score, despite comprising a smaller range of items. The implications of this include development of new tests designed to detect subtle change in cognition associated with AD biomarkers, while also considering ecologically valid, accessible, and low burden metrics.
Limitations
The WRAP cohort is enhanced for parental history of AD and mostly identifies as white. Additionally, the participants in WRAP are highly educated: the sample in these analyses had an average of 15.8 years of education. Therefore, our sample is not representative of the population, which limits the generalizability of our findings. We also acknowledge the role that the language of testing and cultural importance placed on names in the US may contribute to improved recall of this type of information. This limits the generalizability across different cultures and languages. In our logistic regression models, we had a small number of participants who received a clinical diagnosis of MCI or dementia at their most recent visit (only ∼4% of our sample, n = 35), due to this, we feel these results in particular should be taken with caution and should be repeated in a larger sample in the future to better assess clinical utility of proper name recall.
Future directions
As noted in the limitations, culture and language may impact performance on proper name recall. A future direction for this research would be to analyze global datasets to explore proper name recall in other cultures, countries, and languages.
Due to the longitudinal trajectories demonstrated in our group's work, a proper names score could also be used to monitor disease progression over time. To assist in better understanding the potential utility of proper names as a marker of semantic processing, future directions could include expanding this type of testing to a clinical population to assess if the same associations can be seen outside of a research-based population. Additional plasma biomarkers considering ATN status or other forms of dementia should also be considered in future analyses. Due to the p-values nearing significance in our Aim 2 analyses including sex, we recommend repeating in a sample that includes more male participants to explore further if sex moderates the longitudinal trajectories of Logical Memory story recall. To further explore the possible diagnostic patterns, future studies could evaluate a measure of proper name recall that is independent of the Logical Memory test in a larger, clinically diagnosed cohort to better assess its potential as an early marker of impending MCI. Additionally, as proper names may be better suited to diagnosing the earliest, pre-MCI cognitive changes, future work could consider other diagnostic criteria, such as a subtle cognitive impairment or cognitively unimpaired-declining classifications.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261446477 - Supplemental material for Validation of longitudinal change in proper name recall with pTau217 as a marker of early cognitive decline in cognitively unimpaired adults at risk for Alzheimer's disease dementia
Supplemental material, sj-docx-1-alz-10.1177_13872877261446477 for Validation of longitudinal change in proper name recall with pTau217 as a marker of early cognitive decline in cognitively unimpaired adults at risk for Alzheimer's disease dementia by Kristin Basche, Deling He, Rebecca Langhough, Erin Jonaitis, Lianlian Du, Davide Bruno, Rachael Wilson, Bruce Hermann, Sterling Johnson and Kimberly Mueller in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We would like to thank all participants and their families, and the faculty and staff at the University of Wisconsin's Wisconsin Alzheimer's Institute and Wisconsin Alzheimer's Disease Research Center, whose contributions make this work possible.
Ethical considerations
This study is approved under the University of Wisconsin – Madison Institutional Review Board and was conducted in accord with the ethical standards of the Helinski Declaration of 1975.
Consent to participate
WRAP participants gave written informed consent to participate.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge the National Institutes of Health, the National Institute on Aging, the National Institute of Child Health and Human Development, and the Alzheimer's Association for financial support of this work under the following grants: NIH R01 AG021155, R01 AG027161, R01 AG054059, R01 AG070940. These funding sources had no role in the design and conduct of the study or collection, management, and analysis of the data. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.C.J. has consultancy agreements with Enigma Biomedical and with AlzPath. All other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The ethical regulations that govern the WRAP study prevent unrestricted public archiving of anonymized study data. Data can be requested from the WRAP Executive Committee at: ![]() . Data will be released to internal and external investigators following confirmation of IRB approval together with an evaluation by the WRAP executive committee of scientific merit and resource availability.
. Data will be released to internal and external investigators following confirmation of IRB approval together with an evaluation by the WRAP executive committee of scientific merit and resource availability.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.