
Abstract
Background
Alzheimer's disease and related dementia (ADRD) leads to adverse health outcomes, such as higher risk of hospitalizations and long-term institutionalization. However, little is known about differences in ADRD health outcomes for older adults in the Deep South compared to those in the rest of the United States (non-Deep South).
Objective
This study aims to examine the prevalence of hospitalization and long-term use of skilled nursing facilities (SNF) among older adults with ADRD, and factors influencing these healthcare utilization outcomes in the Deep South versus non-Deep South regions.
Methods
We conducted secondary analyses of claims data for 115,879 Medicare beneficiaries with ADRD in 2013–2015. Modified Poisson regression was used to examine the association of outcomes with individual and context-level factors for Deep South and non-Deep South separately.
Results
Hospitalization rates were slightly higher in the Deep South. Utilization of long-term SNF was similar across regions. In adjusted analyses, within each region, differences between non-Hispanic Black and White beneficiaries were not significant. Comorbidities, specialist visits, ADRD drug use, and Medicare/Medicaid dual eligibility were associated with more hospitalizations and SNF use for all beneficiaries in the Deep South. For beneficiaries in the non-Deep South region, context-level factors (limited availability of medical resources and poor population health) were significantly associated with healthcare utilization.
Conclusions
We identified differences across regions in the factors associated with hospitalizations and long-term SNF stays, with patient-level factors being relevant in the Deep South region and context-level factors in the non-Deep South region.
Introduction
Almost 7.2 million older Americans lived with Alzheimer's disease and related dementia (ADRD) in 2025. 1 This number is bound to increase considerably as the proportion of the United States (US) population aged 65 and older grows, 1 and not uniformly across US regions: a higher increase is expected in the eastern and southeastern regions. 2 The serious effects on health of ADRD are demonstrated by the associated higher risk of hospital admissions and long-term institutionalization. In a previous study, older adults with ADRD were more likely to have at least one hospital discharge (32% versus 15%) and long-term skilled nursing facility (SNF) stay (19% versus 4%) per year compared to individuals without ADRD. 1 Preventing the occurrence of these serious adverse outcomes is an important goal for older adults with ADRD. 3 Their occurrence may be influenced by ADRD severity and a host of individual and contextual factors that may predispose or enable patients to use these health care resources. These may vary by US region and should be investigated to better understand whether and how hospitalizations and long-term institutionalizations could be prevented in different contexts.
The Deep South, a sub-region of the southeastern US comprising the states of Alabama, Georgia, Louisiana, Mississippi, and South Carolina, 4 deserves special attention because of a rising number of ADRD cases and its socioeconomic and medical context. 4 The region is characterized by high proportions of people living in poverty (17% poverty rate),5,6 and in rural areas (26%-54%) 7 and limited access to health care services (e.g., all but 5 Alabama counties are designated as Health Professional Shortage Areas). 8 In a previous study, we examined medical care to manage ADRD in and outside this region, specifically the use of specialists, i.e., neurologists, psychiatrists, and geriatricians, and of recommended symptomatic drugs, i.e., donepezil, galantamine, rivastigmine, and memantine. 4 We found that only about 40% of older adults had visits with ADRD specialists, with a lower proportion in the Deep South than in the rest of the US, especially among non-Hispanic Black adults. Moreover, only about 50% of older adults used ADRD drugs, with a slightly higher proportion in the Deep South. 4 This relatively low utilization of care for ADRD management may be accompanied by high prevalence of serious health effects and, thus, hospitalizations and long-term institutionalization: however, the prevalence of these events for various populations of the Deep South is not currently known. Moreover, in our work we found that the individual and contextual factors associated with specialist and ADRD drug use were somewhat different in the Deep South and the rest of the US and did not explain differences across racial groups. Whether the same individual and contextual factors are associated with hospitalizations and long-term institutionalizations in these regions, remains to be investigated.
To address these knowledge gaps, we examined prevalence of hospital admissions and long-term institutionalizations in older adults with ADRD in the Deep South region and the rest of the US. For each region, we examined prevalence in non-Hispanic White and Black individuals and the individual and contextual factors that may affect outcomes and differences across races.
Methods
Study design and participants
This study was a secondary analysis of 2012–2016 administrative claims data for a 5% random sample of Medicare beneficiaries. The methods and study design are described in detail elsewhere. 4 Briefly, here we include a total sample of 115,879 non-Hispanic Black and White patients identified from administrative claims over 3 years (2013–2015) using ICD-9 and 10 codes from a highly sensitive and specific algorithm by Taylor et al. 9 An index event was the first claim that contributed to ADRD case identification. The follow-up was the period after the index event and until institutionalization in a SNF or hospice for 30 days or more, or death, or one year, whichever came first, with a minimum of 7 days. 4
Variables
Outcomes
The outcomes defined for this study were binary for: i) having at least one claim for hospital admission in the follow-up period, and ii) long-term institutionalization, defined as having at least one claim for SNF admission that lasted 30 days or longer. We defined outcomes by place of residence, i.e., Deep South including the states of Alabama, Georgia, Louisiana, Mississippi, and South Carolina, and non-Deep South, defined as the remainder of the US states. 4
Individual and contextual factors potentially affecting study outcomes
In our previous study, building on a behavioral access to care framework, we identified patient-level factors, including personal predisposing factors, enabling factors, and medical need factors, that impact the utilization of needed care and, ultimately, health outcomes. 4 Personal predisposing factors included sex, race, and age; enabling factors included Medicare/Medicaid dual eligibility as a poverty indicator, residential Area Deprivation Index (ADI) scores (scale 1–100, with higher scores indicating higher deprivation) 10 and residence in large or small metro, micropolitan or rural areas (based on the Urban Influence Code). 11 Medical need factors included comorbid conditions identified in a one-year look-back period using the Charlson comorbidities algorithm, 12 and dementia types (defined based on ICD-9 and ICD-10 codes as Alzheimer's Disease, vascular, senile, and other). 4
The contextual factors were determined with an exploratory factor analysis of data from the Area Health Resources Files 13 (AHRF). 6 For the Deep South, the contextual factors were: i) Availability of Medical Resources (number of neurologists, psychiatrists, and PCPs per capita; number of hospital beds per 1000 population in 2015; percent of owner-occupied housing units in 2010; percent of county population aged 65 and older in 2015); ii) Socioeconomic and Health Context (percent of county population aged 25 + with less than high-school diploma in 2012–2016; percent of Medicare beneficiaries in the county eligible for Medicaid in 2015; percent of civil noninstitutionalized county population aged 65 and older on disability in 2012–2016; emergency department visits per 1000 Medicare Fee for Service beneficiaries in the county in 2015; number of SNF beds per 1000 population in 2015; three-year number of deaths per 1000 population in 2013–2015); iii) Health Insurance Market Context (number of Medicare beneficiaries in Fee for Service plans per 1000 population in 2015; percent of Medicare beneficiaries in Advantage Care Plans in 2015; percent of eligible Medicare beneficiaries with Part D Prescription Drug Plans in 2015); and iv) Other Context (percent of Black/African American county population in 2015; unemployment rate for the county population aged 16 and older in 2015; three-year number of deaths per 1000 population in 2013–2015). For the non-Deep South, the context factors were: i) Availability of Medical Resources (same as Deep South); ii) Socioeconomic Context (percent of county population aged 25 and older with less than high-school diploma in 2012–2016; percent of Medicare beneficiaries in the county eligible for Medicaid in 2015; percent of civil noninstitutionalized county population aged 65 and older on disability in 2012–2016; percent of persons aged 65 and older in deep poverty in 2012–2016); iii) Poor Population Health (three-year number of cardiovascular and cerebrovascular deaths per 1000 population in 2013–2015; emergency department visits per 1000 Medicare Fee for Service beneficiaries in the county in 2015; number of SNF beds per 1000 population in 2015); and iv) Health Insurance Market Context (number of Medicare beneficiaries in Fee for Service plans per 1000 population in 2015; percent of Medicare beneficiaries in Advantage Care Plans in 2015; percent of eligible Medicare beneficiaries with Part D Prescription Drug Plans in 2015).
Statistical analysis
We conducted adjusted analyses for Deep South and non-Deep South separately using the modified Poisson regression (PROC GENMOD) to examine the association of outcomes with individual and contextual factors. The results were considered statistically significant and practically meaningful when the accompanying statistical test yielded a two-tailed probability of 0.0001 and confidence intervals for the risk ratio did not include 1. We opted to use a very conservative significance level because, due to the large sample size, most differences are significant at the 0.05 level even if negligible. All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC). The UAB Institutional Review Board considered this study-exempt research.
Results
Of 115,879 Medicare beneficiaries with ADRD, 89.2% were non-Hispanic White, 10.8% were non-Hispanic Black, 72.3% were females, and 47.4% were 85 or older. A detailed comparison of beneficiaries in the Deep South versus those in the non-Deep South region is given in Table 1. Overall, personal-level medical need factors included 50.8% Medicare beneficiaries with 3 or more comorbid conditions (Charlson comorbidity index), with the most common (more than 25% of the sample) being diabetes, cerebrovascular disease, peripheral vascular disease (PVD), depression, chronic pulmonary disease (COPD), congestive heart failure, and chronic kidney disease. Enabling factors included more than 31.1% with Medicare/Medicaid dual eligibility and a mean ADI of 48.9 (scale 1–100, with higher scores indicating higher deprivation).
Characteristics of Medicare beneficiaries * with Alzheimer's disease and related dementia in 2013–2015 (N = 115,879) by region of residence.
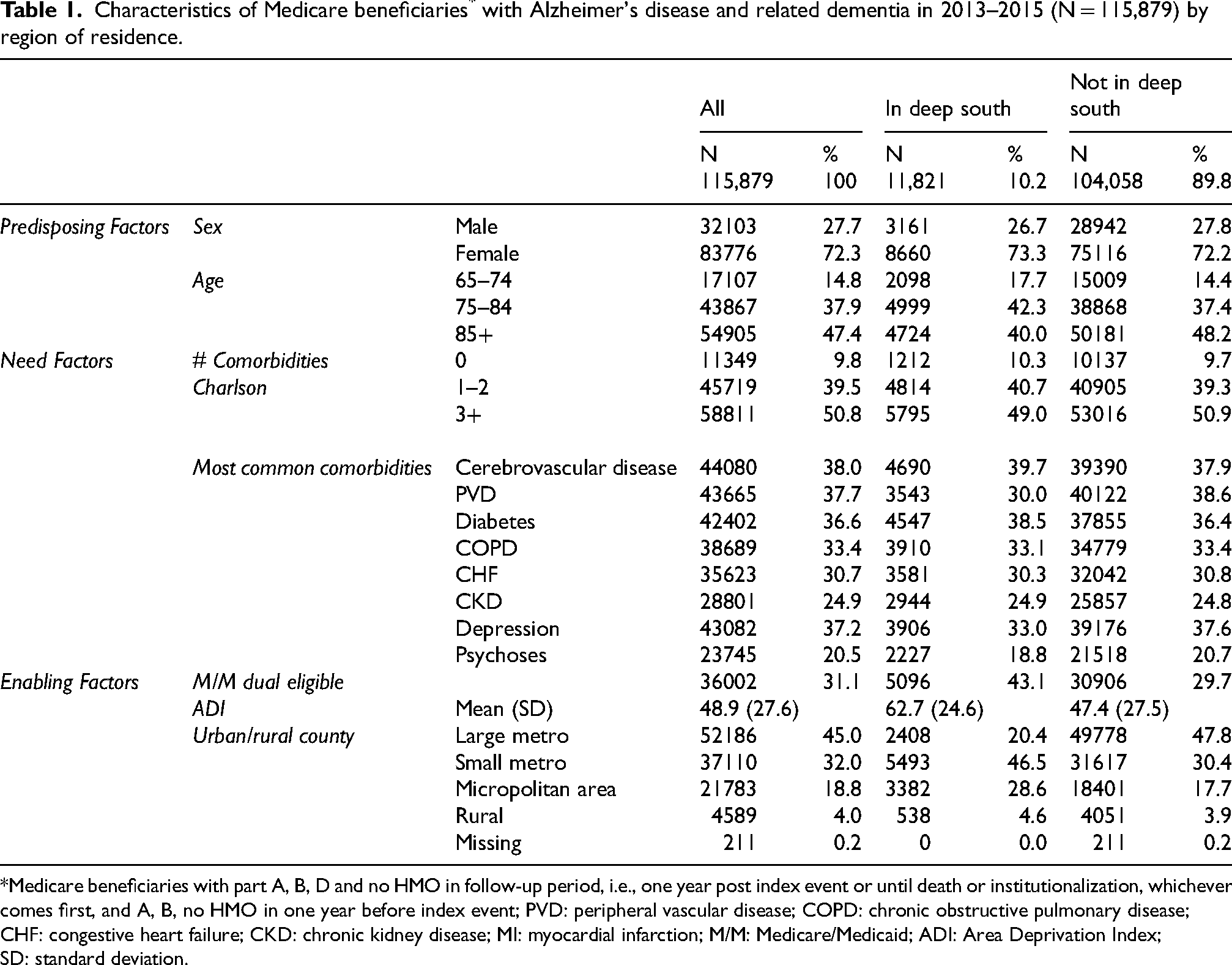
Medicare beneficiaries with part A, B, D and no HMO in follow-up period, i.e., one year post index event or until death or institutionalization, whichever comes first, and A, B, no HMO in one year before index event; PVD: peripheral vascular disease; COPD: chronic obstructive pulmonary disease; CHF: congestive heart failure; CKD: chronic kidney disease; MI: myocardial infarction; M/M: Medicare/Medicaid; ADI: Area Deprivation Index; SD: standard deviation.
Beneficiaries who resided in the Deep South differed from those in the non-Deep South in age (40% versus 48.2% aged 85 and older), prevalence of some conditions (PVD 30% versus 38.6%, depression 33% versus 37.6%), proportion of Medicare/Medicaid dual eligible beneficiaries (43% versus 29.7%), ADI (62.7 versus 47.4), and proportion residing in urban (20.4% versus 47.8%) or small metro (46.5% versus 30.4%) areas (Table 1). Moreover, differences were observed between non-Hispanic Black and non-Hispanic White beneficiaries in both regions across individual need and enabling factors (Supplemental Table 1). In the Deep South, non-Hispanic Black beneficiaries were more likely than White to have three or more comorbid conditions (Charlson, 57.4% versus 46.6%), cerebrovascular disease (44.0% versus 38.4%), and diabetes (51.6% versus 34.7%). They also had higher rates of dual Medicare–Medicaid eligibility (71.1% versus 35%) and were more likely to live in areas with higher ADI scores (75 versus 59.2). Similar patterns appeared in the non–Deep South region: non-Hispanic Black beneficiaries more often had three or more comorbidities (63.2% versus 49.7%), cerebrovascular disease (45.2% versus 37.1%), and diabetes (54.6% versus 34.5%), and were more likely to be dually eligible for Medicare and Medicaid (58.5% versus 26.7%) and live in areas with higher ADI scores (61.2 versus 46) than their White counterparts.
Hospitalizations
Almost half of the beneficiaries had at least one hospital admission in the follow-up period (Figure 1A). This proportion was higher for Deep South (51.6%) than non- Deep South (47.0%) beneficiaries. Within the Deep South, 53.4% of Black beneficiaries and 51.1% of White beneficiaries had at least one hospital admission, while in the non-Deep South, 51.8% of Black beneficiaries and 46.5% White beneficiaries had at least one hospitalization. In analyses adjusted for personal and context-level factors, differences across racial groups were not statistically significant in the Deep South or in non-Deep South regions (Figure 2 and Supplemental Table 2).
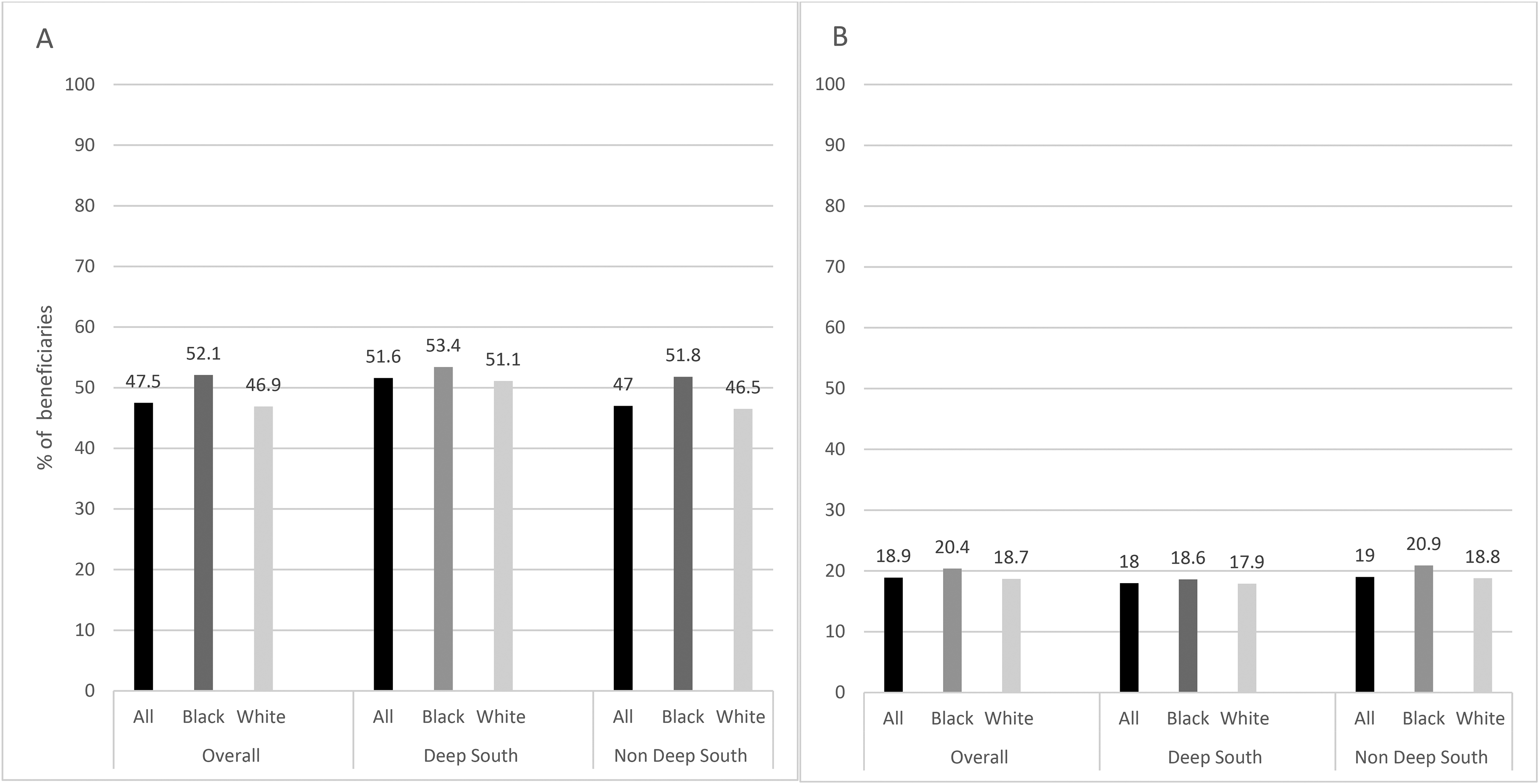
Proportion of Black and White Medicare beneficiaries with ADRD with ≥ 1 hospitalization (A) and ≥1 SNF admission longer than 30 days (B), overall, by race and geographic region (Deep South versus non-Deep South).
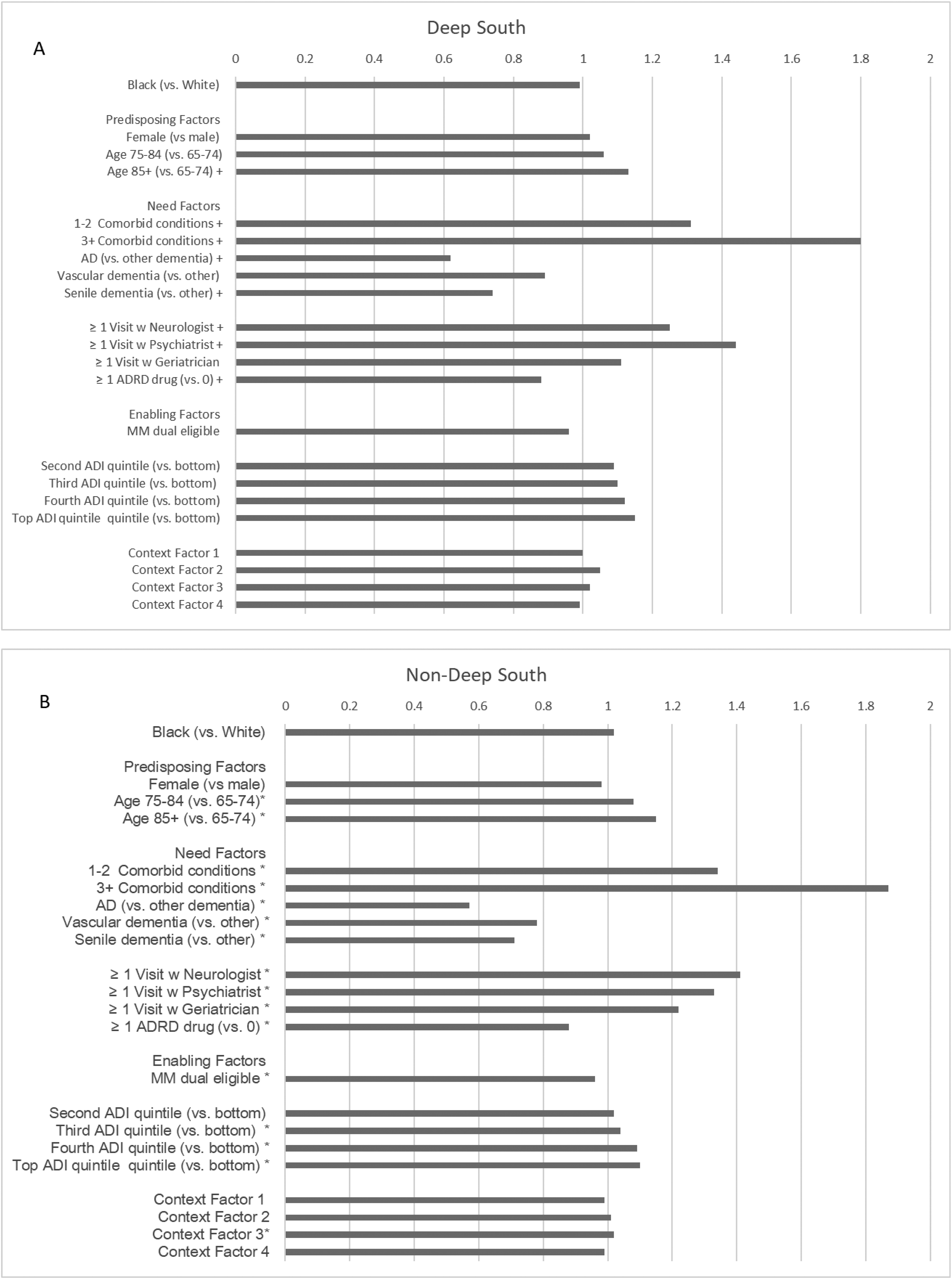
Relative Risk of having ≥ 1 hospitalization among black and white Medicare beneficiaries by geographic region (Deep South (A) and Non-Deep South (B)).
Factors positively associated with having hospitalizations in the Deep South (Figure 2, Supplemental Table 2) included predisposing factor of age (age 85 + versus 66–74 RR = 1.13, p < 0.0001), and personal need factors such as having comorbidities (1–2 comorbidities: RR = 1.31; ≥3 comorbidities: RR = 1.80; p < 0.0001), having visits with a neurologist (RR = 1.25, p < 0.0001), or psychiatrist (RR = 1.44, p < 0.0001). Factors negatively associated with having hospitalizations were having at least one ADRD medication prescription (RR = 0.88, p < 0.0001), having Alzheimer's Disease and senile dementia versus “other” dementia (AD: RR = 0.62, p < 0.0001; senile dementia: RR = 0.74, p < 0.0001; vascular dementia: RR = 0.89, p < 0.0001). No other individual or contextual factor was associated with having hospitalizations.
In the non–Deep South region, age, having comorbidities (1–2 comorbidities: RR = 1.34; ≥3 comorbidities: RR = 1.87; p < 0.0001) and visits with a neurologist (RR = 1.41, p < 0.0001), psychiatrist (RR = 1.33, p < 0.0001), or geriatrician (RR = 1.22, p < 0.0001) were associated with increased hospitalization risk. Having ADRD drug prescriptions (RR = 0.87, p < 0.0001) or having Alzheimer's Disease, senile, or vascular dementia versus “other” dementia risk (AD RR = 0.57, p < 0.0001; senile dementia RR = 0.71, p < 0.0001; vascular dementia RR = 0.78, p < 0.0001) were associated with lower hospitalization risk. In this region, personal enabling factors were associated with hospitalization risk, namely being Medicare/Medicaid dually eligible (RR = 0.96, p < 0.0001) and ADI (top versus bottom quintile RR 1.1, p < 0.0001), as well as contextual factors, namely Poor Population Health (RR = 1.03, p < 0.0001).
Long-term SNF
Admission to an SNF that lasted longer than 30 days occurred in 18.9% of the overall study population (Figure 1B). This proportion was slightly lower in the Deep South (18.0%) than in the non-Deep South (19.0%). Within the Deep South, 18.6% of Black beneficiaries and 17.9% of White beneficiaries had at least one long-term SNF, while in the non-Deep South, 20.9% of Black beneficiaries and 18.8% of White beneficiaries had at least one long-term SNF. In analyses adjusted for individual- and context-level factors, the relative risk of long-term SNF for Deep South Black versus White beneficiaries was 0.84 (p = 0.0014), and for non-Deep South Black versus White beneficiaries it was 0.94 (CI 0.89–0.98, p = 0.0035) (Figure 3 and Supplemental Table 3).
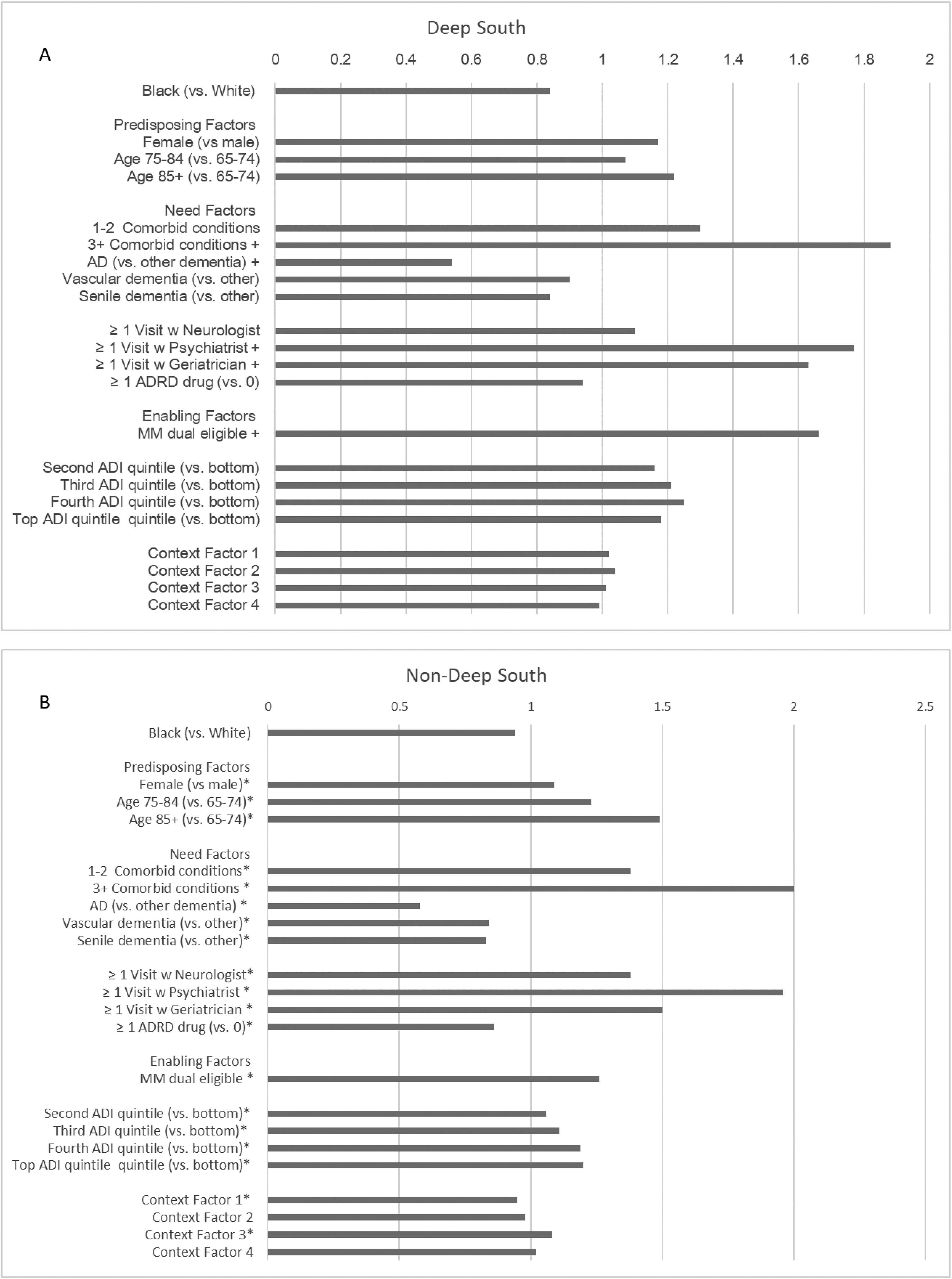
Relative Risk of having ≥ 1 SNF admission longer than 30 days among black and white Medicare beneficiaries by geographic region (Deep South (A) and Non-Deep South (B)).
In the Deep South, personal need factors associated with a higher risk of long-term SNF admissions included having a higher number of comorbid conditions (3 + comorbidities, RR 1.88, p < 0.0001), having visits with psychiatrist (RR = 1.77, p < 0.0001) or geriatrician (RR = 1.63, p < 0.0001); personal enabling factors associated with a higher risk of long-term SNF included being Medicare/Medicaid dually eligible (RR 1.66, p < 0.0001). Beneficiaries with Alzheimer's Disease versus “other” dementia were less likely to have long-term SNF admissions (RR = 0.54, p < 0.0001). No other personal or contextual factors were associated with long-term SNF risk.
In the non- Deep South region, female sex (RR = 1.08, p < 0.0001) and older age were personal predisposing factors associated with long-term SNF risk. Significant personal-level need factors included having comorbidities (1–2 comorbidities: RR = 1.38, p < 0.0001; 3 + comorbidities: RR = 2.0, p < 0.0001), visits with a neurologist (RR 1.38, p < 0.0001), psychiatrist (RR 1.96, p < 0.0001), or geriatrician (RR = 1.50, p < 0.0001), ADRD drugs (RR = 0.86, p < 0.0001), and dementia subtypes (AD RR = 0.54, senile dementia RR = 0.84 vascular dementia RR = 0.90, versus “other”—p < 0.0001). Significant personal enabling factors included being Medicare/Medicaid dually eligible (RR = 1.26, p < 0.0001) and living in areas with higher ADI scores (third versus bottom quintile RR 1.11, p < 0.0001 and fourth versus bottom quintile RR 1.19, p < 0.0001). Lastly, Availability of Medical Resources (RR = 0.95, p < 0.0001) and Poor Population Health (RR = 1.08, p < 0.0001) were contextual factors associated with the risk of long-term SNF.
Female beneficiaries had higher relative risk of long-term SNF compared to males in both regions (Deep South: RR = 1.17, NS; non-Deep South region (RR = 1.08, p < 0.0001). Personal-level need factors associated with having a higher risk of long-term SNF included a higher number of comorbidities (Deep South: 3 + comorbidities, RR 1.88, p < 0.0001; non-Deep South: 1–2 comorbidities: RR = 1.38, p < 0.0001; 3 + comorbidities: RR = 2.0, p < 0.0001); having a visit with a neurologist (Deep South: RR = 1.10, NS; non-Deep South: RR 1.38, p < 0.0001), psychiatrist (Deep South: RR = 1.77, p < 0.0001; non-Deep South: RR 1.9, p < 0.0001), or geriatrician (Deep South: RR = 1.63, p < 0.0001; non-Deep South: RR = 1.5, p < 0.0001). Having received ADRD drugs was associated with a lower risk of long-term SNF (Deep South: RR = 0.94, NS; non-Deep South: RR = 0.862, p < 0.0001).
Personal enabling factors associated with a higher risk of long-term SNF included being Medicare/Medicaid dually eligible in both regions (Deep South: RR 1.66, p < 0.0001; non-Deep South: RR = 1.26, p < 0.0001) and having a higher ADI score in the non-Deep South (third versus bottom quintile RR 1.11, p < 0.0001 and fourth versus bottom quintile RR 1.19, p < 0.0001). For non-Deep South beneficiaries, Availability of Medical Resources (RR = 0.95, p < 0.0001) and Poor Population Health (RR = 1.08, p < 0.0001) were contextual factors associated with the risk of long-term SNF.
Discussion
In the present study, we found that nearly half of Medicare beneficiaries with a diagnosis of ADRD had at least one hospitalization, and nearly one in 5 had one long-term SNF admission of at least 30 days, in a one-year follow-up period. The proportion of beneficiaries with hospitalizations was higher in the Deep South than in the other regions of the country, while the proportion with long-term SNF was similar across regions. Moreover, in the Deep South, only personal-level factors, e.g., age, comorbidities, specialist visits, and Medicare/Medicaid dual eligibility, were associated with the risk of hospitalizations and SNF. In other states, in addition to those personal-level factors, contextual factors (area deprivation, poor population health, and limited resource availability) were also significantly associated with these healthcare utilization outcomes. Across both regions, we observed modest differences in hospitalizations between Black and White beneficiaries, which were not statistically significant in adjusted analyses. The likelihood of long-term SNF stays were similar for all groups and regions.
ADRD leads to increased healthcare utilization, including hospitalizations and SNF admissions, through a variety of mechanisms that reflect patients’ overall health conditions over the course of the disease. 14 Overall, we find a higher hospital utilization in our study compared to data for the year 2019, when about a third of Medicare beneficiaries with ADRD had at least one hospital discharge. 1 This difference may reflect overall time trends in hospital utilization, or different methodology, e.g., by focusing on a follow-up period after an index event, we may have selected beneficiaries at higher risk. Long-term use of SNF, however, was comparable to previous reports, suggesting that probably reflecting aspects of disease progression and functional decline associated with ADRD may drive prolonged SNF stays despite ADRD or other comorbid conditions management.
Notably, the slightly higher hospitalization rates we found for the Deep South suggest potential regional differences that may have existed in this region in disease management, access to outpatient care, or underlying health. Our prior research showed that access to outpatient specialty care—including geriatrics and neurology services—was limited in the Deep South region,4,15 which may have led to delayed management of acute ADRD-related conditions and greater reliance on hospital-based care. Inadequate access to primary and specialty care has been consistently associated with higher rates of avoidable hospitalizations among older adults with ADRD, that could be due to poor management of chronic comorbid conditions highly prevalent in the US South, e.g., diabetes, obesity, and cardiovascular disease.16–18
Here we found that having specialist visits was associated with a higher risk of hospitalizations and SNF stays, indicating that severity or complexity of ADRD and underlying conditions lead to a higher likelihood of referral to scarce specialists while concurrently leading to unfavorable outcomes. Earlier data supports the relationships between multimorbidity, emergency department and clinic visits, and also mortality among older diverse older adults. 19 Older adults with two or more chronic conditions, including ADRD, had higher rates of emergency department and clinic visits, and ADRD was the most significant predictor of 5-year mortality in Black individuals. 19 Thus, interventions to improve the management of chronic conditions are necessary. Furthermore, in line with previous studies, the use of ADRD symptomatic drugs was associated with a lower risk of hospitalizations and long-term SNF stays: appropriate use of these medications optimizes symptom management, reduces avoidable hospitalizations, and delays SNF placement.20,21 In our previous study, we found that ADRD medication adherence was lower among beneficiaries in the Deep South, especially among racial and ethnic minority groups and in beneficiaries who had visits with specialists. 15 Therefore, interventions to improve adherence to ADRD are also necessary. These personal-level factors should be key intervention targets, especially for the Deep South, in light of our findings that those were the only ones associated with hospital and SNF utilization. However, while contextual factors did not predict healthcare utilizations in this region, it is important to note the substantially high proportion of rural residents in the Deep South. 7 Rurality has been associated with later-stage diagnosis of ADRD, primarily due to limited availability of providers and SNFs. This delayed diagnosis leads to individuals often entering care pathways at more advanced stages of disease when options for intervention are limited. Therefore, the rurality context of the Deep South cannot be ignored, and future studies should further clarify drivers of healthcare utilization to inform appropriate targeted interventions in this high-burden region.
For beneficiaries in regions of the country outside the Deep South, we found some evidence of the importance of contextual factors, which is also in line with research on the social determinants of health1,22 and research that shows geographic variability in outcomes.22–24 These included indicators of limited availability of medical resources and poor overall population health (e.g., higher prevalence of cardiovascular and cerebrovascular disease and emergency department visits). This context may influence healthcare treatment patterns despite personal predisposing, need, and enabling factors. Our findings are consistent with prior research in the northeast region pointing to area-level demographic characteristics (population aged ≥50 years) as contributing to higher admission rates in individuals with cancer and dementia regardless of the area-level socioeconomic status. 25 Research should further investigate the contribution of the contexts in which people live and seek medical care, and the underlying mechanisms that may affect access to and use of medical resources and the resulting health outcomes. For example, further research is needed to explore what characterizes each context, e.g., examining interactions between individual- and area-level factors, such as social support services, housing and living conditions, transportation access, and healthcare access policies and programs (e.g., Medicaid expansion, Medicare advantage penetration) within regions to better explain the predictors of patterns of health services use and outcomes.
Hospital utilization was somewhat higher among Black beneficiaries, consistent with prior evidence of increased preventable hospitalizations among Black individuals with ADRD. 26 This disparity may reflect a higher burden of comorbidities, lower use of specialist and ADRD-related care, and differences in mental health diagnosis and treatment. In particular, Black beneficiaries had fewer depression-related claims than non-Hispanic White beneficiaries, consistent with documented underdiagnosis or undertreatment of depression in older Black populations, 27 which may contribute to elevated hospitalization risk. Overall, however, we found that differences by racial groups were not statistically significant when adjusting for personal and context-level factors, suggesting that observed differences are due to some modifiable factors like management of comorbid conditions and access to ADRD care. Therefore, as suggested by others, factors such as sociodemographic and cultural characteristics, e.g., disease perceptions, caregiver experiences, and ADRD health literacy, that may prevent prompt access to healthcare, warrant further study. 28
Limitations
This study has some limitations. Our results are not generalizable to beneficiaries on managed care or on fee-for-service Medicare without Part D coverage. In our study period, between a quarter and a third of Medicare beneficiaries were enrolled in managed care plans, and some racial groups were overrepresented among the enrollees. 29 The exact ADRD diagnosis date cannot be established in these data: healthcare utilization and drug use may vary depending on how far individuals are from their diagnosis. The severity of ADRD or chronic conditions was not captured. The geographic level used was constrained by the data available: for example, ADI scores were obtained at the ZIP code level, which may be too large to capture the true personal neighborhood disadvantage. 30 Finally, limitations of the ADI noted recently,31,32 specifically the lack of standardization that reduced the measure to a weighted average of just two variables (household income and home values) rather than the advertised multidimensional measure, may have affected the results.
Conclusions
In this national study of Medicare beneficiaries with ADRD, we found that the factors that impact utilization of hospitals and long-term SNF care may be different across US regions. Utilization was driven primarily by personal-level need and enabling for beneficiaries in the Deep South, whereas for those in other non–Deep South regions, contextual factors—including poverty, population health burden, and limited healthcare resources—played an additional role. These findings underscore the need for regionally tailored strategies to reduce hospitalizations and improve health care and outcomes for older adults with ADRD.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261453901 - Supplemental material for Hospitalizations and long-term care for older adults with Alzheimer's disease and related dementia: Differences across geographic regions of the United States
Supplemental material, sj-docx-1-alz-10.1177_13872877261453901 for Hospitalizations and long-term care for older adults with Alzheimer's disease and related dementia: Differences across geographic regions of the United States by Giovanna Pilonieta, Maria Pisu, Roy C. Martin, Liang Shan, Richard E. Kennedy, Gabriela R. Oates, Young-Il Kim and David S. Geldmacher in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
The UAB Institutional Review Board deemed this exempt study research.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by National Institutes of Health through a supplement from the National Institute of Aging to the Obesity Health Disparities Research Center under the award number U54MD000502-17S2.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study were obtained and accessed by the principal investigator under a data use agreement (DUA) with The Centers for Medicare and Medicaid Services (CMS), which does not allow data sharing. The data can be obtained under a new DUA with CMS.
Supplemental material
Supplemental material for this article is available online.