
Abstract
Background
Sex-specific vulnerability to Alzheimer's disease (AD) has been increasingly recognized, with menopause representing a decisive neuroendocrine transition. Estrogen and progesterone modulate synaptic plasticity, glucose metabolism, and amyloid-tau homeostasis, yet the impact of their decline and replacement remains controversial. AD biomarkers provide objective means to assess menopausal hormone therapy (MHT) mechanistic effects beyond cognitive endpoints.
Objective
To determine how MHT influences validated AD biomarkers in peri- and postmenopausal women.
Methods
A systematic review was conducted following PRISMA guidelines (PROSPERO CRD420251149404). PubMed, Embase, Web of Science, and Cochrane Library were searched through September 2025 for interventional and observational studies evaluating MHT and AD biomarkers after non-surgical menopause. Eligible biomarkers included cerebrospinal fluid (CSF) and plasma markers, and amyloid-, tau- or FDG-PET imaging. Study quality was assessed using RoB-2 and ROBINS-I tools, and evidence certainty with GRADE.
Results
Fourteen studies met inclusion criteria. Early or continuous transdermal 17β-estradiol was linked with lower CSF and plasma p-tau181 and preserved glucose metabolism in AD-vulnerable cortical regions. Neuroimaging studies showed decreased amyloid deposition and sustained metabolic benefits years after discontinuation. Conversely, oral conjugated equine estrogens and estrogen-progestin regimens led to neutral or unfavorable biomarker trends, particularly when initiated more than five years after menopause.
Conclusions
MHT's effects on AD biomarkers depend on timing, formulation and hormonal composition. Early transdermal estradiol appears to reinforce neuroprotective biomarker profiles, whereas delayed or combined therapies may nullify these benefits. Genotype-stratified trials with harmonized biomarker reports are needed to define optimal neuroprotective windows for women.
Introduction
Few questions in contemporary neurology produce as much controversy as whether menopausal hormone therapy (MHT) impacts the clinical course of Alzheimer's disease (AD) in women. Millions of women worldwide transition through menopause every year. Yet, the potential neuroprotective benefits of MHT remain uncertain, despite the increasing recognition of sex specific vulnerability to AD and the rising perception of menopause as a neuroendocrine turning point in women's health. 1
Both estrogen and progesterone exert pleiotropic actions in the central nervous system, influencing synaptic plasticity, 2 glucose metabolism, myelin integrity, and clearance of misfolded proteins. 3 In this setting, it is biologically plausible that their abrupt decline during menopause could negatively impact neural homeostasis through destabilization and modulation of multiple molecular cascades, including amyloid-β (Aβ) aggregation, tau hyperphosphorylation, and glial reactivity, all of which represent core aspects of AD pathology. 4
However, clinical studies show notoriously inconsistent5,6 results regarding the role of estrogen and progesterone replacement in dementia. The Women's Health Initiative Memory Study (WHIMS) famously reported an increased risk of dementia associated with the late initiation of conjugated equine estrogens (CEEs), 7 whereas other studies suggest that timing and formulation influence outcomes, but biomarker-level integration remains lacking.8,9 This discrepancy led to the rise of the timing hypothesis, which posits that the neuroprotective potential of MHT depends on the timing of initiation.10,11 Against this backdrop, AD biomarkers may offer clarifying mechanisms, as they reveal preclinical disease processes with greater specificity than cognitive endpoints ever could.
In fact, biomarkers now anchor AD research, due to their quantifiable and pathophysiologically specific readouts: cerebrospinal fluid (CSF) concentrations of Aβ42 and phosphorylated tau, plasma neurofilament light chain (NfL) and glial fibrillary acidic protein (GFAP), as well as amyloid- and tau- positron emission tomography (PET) imaging. 12 These measures represent a unique opportunity to verify whether MHT alters the molecular architecture of AD in vivo. Nonetheless, contemporary available literature contains heterogeneous study designs, populations, formulations, and biomarker modalities, with inconclusive outcomes, hence exacerbating the need for deeper investigation on the subject. 13
In this biomarker-centered systematic review, we evaluate the evidence on the effects of MHT on AD-related biomarkers in peri- and postmenopausal women, aiming to clarify mechanisms through which MHT may influence AD biomarkers and to understand whether MHT could represent a modifying approach in AD pathogenesis or a risk worthy of careful mitigation, in light of different formulations, timing of initiation and biological contexts.
Methods
This systematic review was conducted in accordance with the Cochrane methodology for systematic reviews of interventions and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 14 The protocol was registered on September 29, 2025, in the International Prospective Register of Systematic reviews (PROSPERO) under the registration number CRD 420251149404.
Research question
The research question was elaborated using the PICOTT (Population; Intervention; Comparator; Outcomes; Type of study; Time of follow-up) framework:
Search strategy and study selection
Searches were systematically conducted in MEDLINE/PubMed, Embase, Web of Science, and the Cochrane Library, with no date restrictions, and included studies published in English up to September 3, 2025. The entire search string is available in the Supplemental Material. Additionally, the reference lists of the included studies were manually screened for additional relevant studies. A manual search of the reference lists of included studies was undertaken to ensure that no other studies were overlooked. Two authors (AR and CM) independently extracted the data following predefined search criteria, and any conflict was solved by discussion with a third author (DH).
Eligibility criteria
Eligible studies included perimenopausal or postmenopausal cisgender women of any age, provided that menopausal status was clearly stated. Transgender men were also excluded, as exposure to gender-affirming hormone therapy introduces distinct endocrine dynamics that could confound the interpretation of menopausal hormone effects. Women with surgically induced menopause (e.g., bilateral oophorectomy) were excluded to avoid confounding effects related to abrupt hormonal deprivation. Menopause was hereby considered as the permanent cessation of menstruation resulting from the loss of ovarian follicular activity, with no other obvious pathological or physiological cause. The intervention of interest was MHT, either estrogen alone or in combination with progesterone, administered by any route (oral, transdermal, implant, and other), at any dose or duration. The comparator group consisted of perimenopausal or postmenopausal women not exposed to hormone therapy, either receiving a placebo or no intervention. Outcomes of interest were AD-related biomarkers measured in CSF (Aβ42, Aβ40, total tau, and phosphorylated tau), plasma or serum (including Aβ, p-tau, NfL, GFAP, β-secretase 1, and others), as well as neuroimaging modalities (amyloid-PET, tau-PET, and FDG-PET). Eligible study designs included clinical trials and observational articles (cohort, case-control, and cross-sectional studies), published in English up to September 2025. We excluded: case reports, and conference abstracts; studies combining lithium with other investigational treatments; and studies conducted in animal models. The retrieved articles were imported into the Rayyan systematic review management platform, 15 manually deduplicated, and independently screened by two authors (AR and CM). Articles whose titles and abstracts did not meet the inclusion criteria were excluded. Full texts were then assessed for studies, and those that met the eligibility criteria were included in the review. Any disagreements and conflicts were resolved by supervisors (AS and CB).
Data extraction
Two blinded reviewers (AR and GT) extracted the following data from each study: study design, authors, year of publication, country of the study and patient characteristics, such as sample size per group, age of participants, menopausal status, type of MHT, dosage, time of follow-up, years of education, Mini-Mental State Examination (MMSE) scores, body mass index (BMI) and APOE ε4 carrier status. All data were collected using Google Sheets and cross-checked to ensure accuracy (AS). Table 1 presents the general characteristics of each study. Authors were contacted via e-mail to obtain data not reported in the published studies, allowing a response period of 60 days.
The final dataset comprised clinical trials and observational studies published between 2003 and 2025.
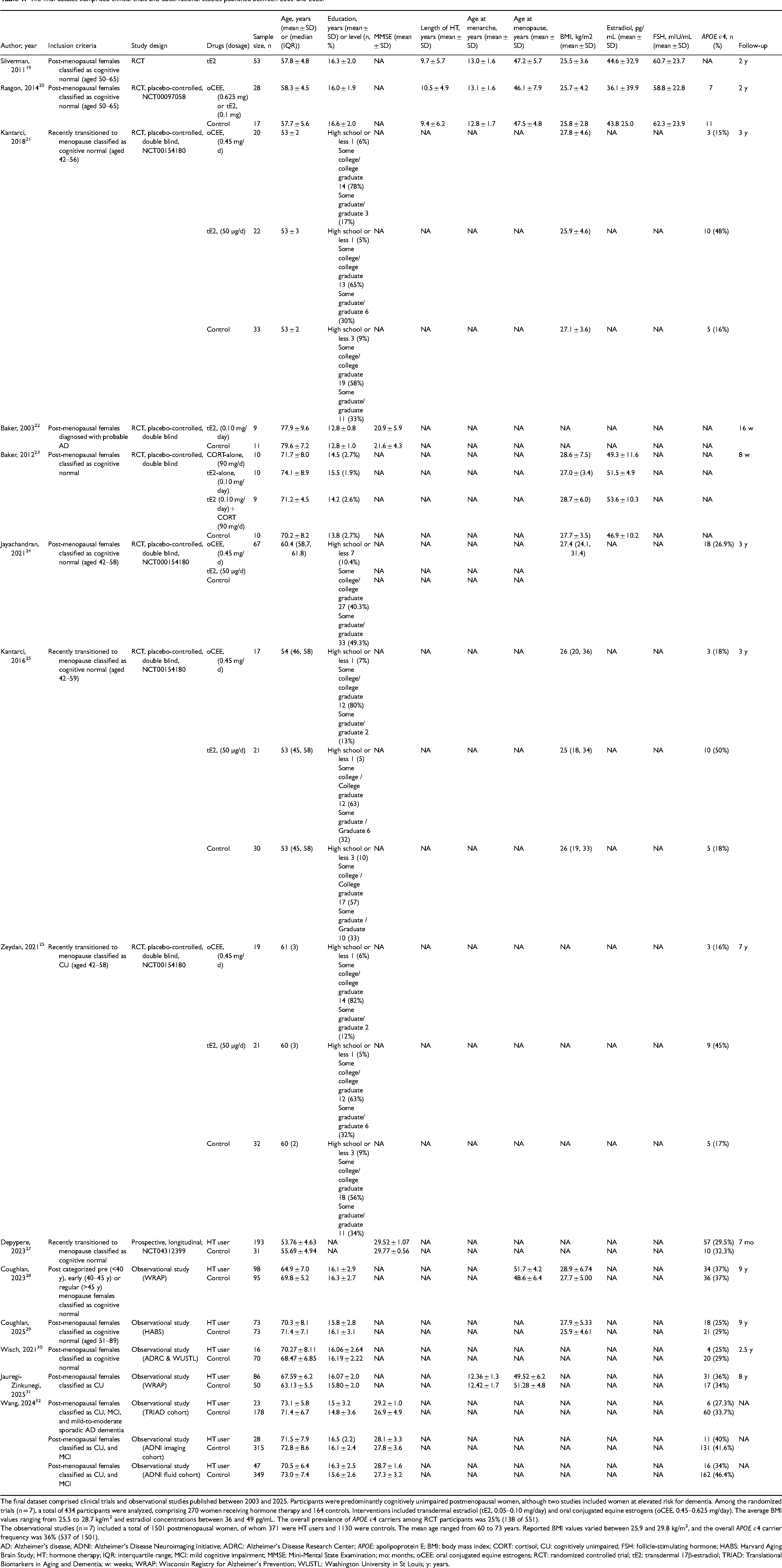
The final dataset comprised clinical trials and observational studies published between 2003 and 2025. Participants were predominantly cognitively unimpaired postmenopausal women, although two studies included women at elevated risk for dementia. Among the randomized trials (n = 7), a total of 434 participants were analyzed, comprising 270 women receiving hormone therapy and 164 controls. Interventions included transdermal estradiol (tE2, 0.05–0.10 mg/day) and oral conjugated equine estrogens (oCEE, 0.45–0.625 mg/day). The average BMI values ranging from 25.5 to 28.7 kg/m2 and estradiol concentrations between 36 and 49 pg/mL. The overall prevalence of APOE ε4 carriers among RCT participants was 25% (138 of 551).
The observational studies (n = 7) included a total of 1501 postmenopausal women, of whom 371 were HT users and 1130 were controls. The mean age ranged from 60 to 73 years. Reported BMI values varied between 25.9 and 29.8 kg/m2, and the overall APOE ε4 carrier frequency was 36% (537 of 1501).
AD: Alzheimer's disease; ADNI: Alzheimer's Disease Neuroimaging Initiative; ADRC: Alzheimer's Disease Research Center; APOE: apolipoprotein E; BMI: body mass index; CORT: cortisol; CU: cognitively unimpaired; FSH: follicle-stimulating hormone; HABS: Harvard Aging Brain Study; HT: hormone therapy; IQR: interquartile range; MCI: mild cognitive impairment; MMSE: Mini-Mental State Examination; mo: months; oCEE: oral conjugated equine estrogens; RCT: randomized controlled trial; tE2: transdermal 17β-estradiol; TRIAD: Translational Biomarkers in Aging and Dementia; w: weeks; WRAP: Wisconsin Registry for Alzheimer's Prevention; WUSTL: Washington University in St Louis; y: years.
Quality assessment and certainty of evidence
The methodological quality of evidence was assessed independently by two authors (AR and FV), using the ROBINS-I v2 assessment tool for follow-up (cohort) and non-randomized studies. 16 The risk of bias in randomized trials was assessed using the RoB-2 tool. 17 This tool covers seven domains, as follows: risk of bias due to confounding factors, classification of interventions, participant selection, deviation from intended interventions, missing data, outcome measurement, and selection of reported results. Discrepancies were resolved by a third author (CB). Two authors (AR and FV) independently assessed the studies for quality and certainty of evidence, using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool. 18
Due to expected heterogeneity in hormone formulations and biomarker platforms, studies were stratified a priori according to formulation (transdermal 17β-estradiol (tE2) versus CEE versus combined), timing of initiation (<5 years versus >5 years post-menopause), and APOE genotype where available.
Results
Study selection
The initial systematic literature search yielded 2480 records. After removing 1051 duplicates, 1429 articles were screened based on their titles and abstracts, leading to the exclusion of 1405 studies. The full texts of the remaining 24 articles were assessed for eligibility. Of these, studies were excluded for reasons including publication as congress abstracts or errata (n = 4), incorrect population (n = 1), lack of completed results (n = 1), or unavailability for retrieval (n = 4). Finally, 14 studies19–32 fulfilled all eligibility requirements and were included in the review. The screening process is illustrated in the flowchart in Figure 1.
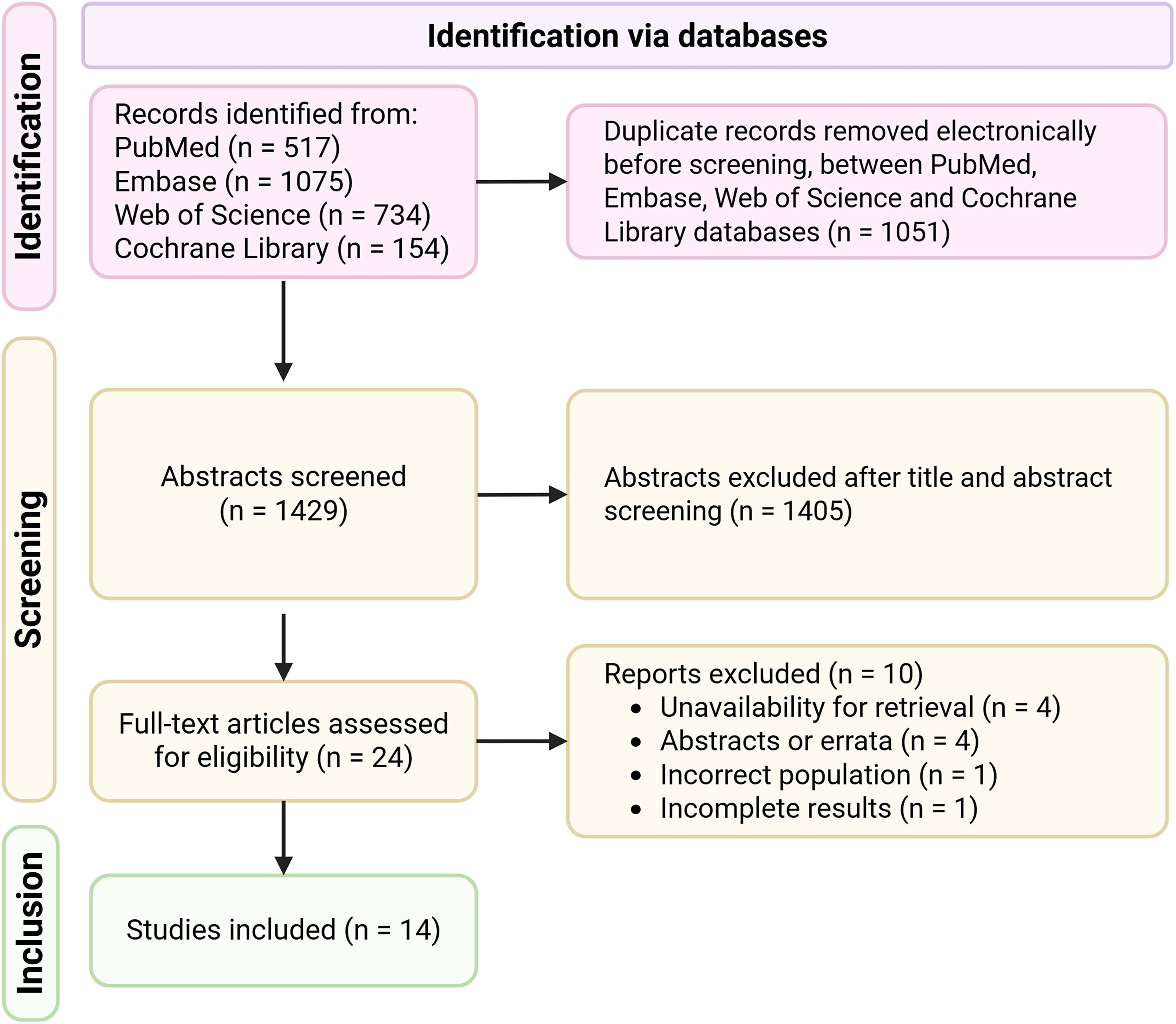
PRISMA flow diagram for systematic reviews.
Baseline characteristics of the included studies and patients
The final dataset comprised clinical trials and observational studies published between 2003 and 2025, which enrolled a total of 2164 patients. Study designs included early-postmenopausal intervention trials and large cohort or cross-sectional biomarker analyses. Participants were predominantly cognitively unimpaired postmenopausal women, although some studies included women at elevated risk for dementia or diagnosed with probable AD.19,20,22,32 Across studies, mean age ranged from the early 50 s to mid-70 s, and the proportion of APOE ε4 carriers varied from 15% to 50%. MHT interventions included oral CEEs (oCEEs), tE2, and combined estrogen-progesterone regimens. Routes of administration were primarily oral or transdermal, preferably with the applied formulation specified. AD-related biomarkers were assessed through CSF assays, plasma-based markers, and neuroimaging (Pittsburgh compound B or fluorodeoxyglucose PET). CSF and plasma studies primarily measured Aβ42, Aβ40, p-tau, t-tau, GFAP, and NfL, whereas neuroimaging studies employed amyloid-PET, tau-PET, and FDG-PET modalities. Regarding the quality of evidence, randomized controlled trials demonstrated a lower risk of bias in allocation concealment, although adherence and blinding of outcome assessors varied. In contrast, observational studies showed moderate methodological quality, mostly limited by self-reported hormone therapy use and a cross-sectional design. Detailed assessments and summary figures are provided in the Supplemental Material (Supplemental Figures 1–3).
Cerebrospinal fluid biomarkers
Overall evidence from CSF biomarker studies revealed mixed effects of MHT on these biomarkers. The study by Jauregi-Zinkunegi and colleagues 31 found that APOE ε4-positive MHT users displayed the worst CSF biomarker profiles, characterized by elevated p-tau/Aβ42 ratios and significantly lower Aβ42/Aβ40 ratios compared to non-users and non-carriers. Conversely, Wang et al. 32 discussed potential benefits of early and ongoing MHT use in the ADNI Fluid Cohort, showing significant decreases in both CSF p-tau181 and a modest reduction in amyloid-PET SUVR among active MHT users. In the same cohort, APOE ε4 carriers undergoing MHT displayed tau and Aβ levels comparable to non-carriers, suggesting a mitigating effect of hormone therapy on APOE ε4's detrimental role on tau accumulation. Depypere et al. 27 demonstrated that, in early perimenopausal women, estrogen replacement therapy was linked to a more stable or even favorable CSF Aβ1−42/p-tau231 ratio over six to seven months compared with controls, notably in APOE ε4-positive women, which appears to stabilize the amyloid-tau balance.
All things considered, CSF biomarker studies suggest potential protective effects of early or ongoing MHT, particularly estradiol-based regimens, albeit results diverge according to formulation, time of initiation, and genotype.
Plasma biomarkers
Plasma-based studies investigating MHT and AD biomarkers suggest that short-term estradiol treatment in MHT-naïve women may reduce plasma Aβ40 levels. 32 However, the clinical significance of isolated changes in Aβ40 is uncertain, as Aβ40 is less aggregation-prone than Aβ42. Technical interpretations of amyloid ratios are critical; lower Aβ42/Aβ40 ratios are considered a primary biomarker of poor prognosis, as they reflect the brain sequestration and aggregation of Aβ42.22,23 Subsequent research 23 has demonstrated complex interactions between estradiol and cortisol: estradiol alone may increase the Aβ40/42 ratio, whereas concomitant cortisol exposure reverses this effect, shifting profiles toward relatively higher Aβ42 and lower Aβ40 levels. These shifts are modulated not only by central amyloidogenesis but also by cortisol-induced alterations in plasma lipid profiles, which may influence the transport of amyloid peptides across the blood-brain barrier (BBB). In this sense, plasma Aβ ratios do not seem to directly mirror brain amyloid dynamics, and peripheral shifts may reflect stress-related endocrine modulation rather than direct central effects on amyloid deposition. 12 In peripheral blood, Jayachandran et al. 24 reported that tE2 resulted in significantly fewer circulating Aβ1−42-positive microvesicles relative to placebo and oral conjugated estrogens, while no significant differences were observed in microvesicles derived from astrocytes (GFAP) or neurons (tau).
Neuroimaging biomarkers
Neuroimaging evidence provided the most consistent pattern supporting estradiol-related neuroprotection. Two randomized trials by Kantarci et al.21,25 displayed considerably lower cortical Aβ deposition in women receiving tE2 compared with placebo, especially among APOE ε4 carriers. Furthermore, preserved prefrontal volume correlated with lower amyloid burden in the tE2 group, which suggests structural benefits connected with estradiol exposure.
FDG-PET data from Rasgon et al. 20 and Silverman et al. 19 revealed higher cerebral glucose metabolism, reflecting preserved synaptic function, in regions vulnerable to AD, such as the posterior cingulate gyrus, precuneus, and prefrontal cortex in patients who continued or were currently using estradiol. Discontinuation of hormone therapy or the use of CEE formulations led to pronounced metabolic decline, particularly in the precuneus and parietal cortices. Combined estrogen-progestin therapy was consistently associated with insufficient or nonexistent neuroprotective effects.
The follow-up of the KEEPS cohort by Zeydan et al. 26 demonstrated a sustained association between better sleep quality and lower cortical Aβ deposition detected by PiB-PET among women previously treated with tE2, an effect that does not seem to happen in those who had received oCEEs. This relationship endured for seven years after MHT discontinuation, which implies long lasting neurophysiological benefits of early transdermal estrogen replacement therapy.
In contrast, recent large-scale imaging studies presented a more complex picture. Coughlan et al. 29 reported that late initiation of MHT (beyond five years after menopause) was linked to higher regional tau-PET signals in temporo-parietal and occipital cortices, independent of amyloid load. In a companion longitudinal analysis, women over 70 years with prior hormone therapy exposure exhibited faster tau accumulation and greater cognitive decline than non-users, despite comparable Aβ deposition. Similarly, Wisch et al. 30 observed only modest, non-significant reductions in tau burden among hormone users after correction for multiple comparisons.
These findings reinforce the concept of a critical window for hormone therapy. tE2 initiated early in the menopausal transition appears to support cerebral metabolism and limit Aβ and tau pathology, whereas delayed or prolonged exposure later in life may coincide with adverse tau-related changes.
Transdermal 17β-estradiol
Transdermal estradiol consistently demonstrated the most favorable association with AD biomarkers. Across the KEEPS studies,21,25,26 tE2 users exhibited lower cortical amyloid burden and preserved prefrontal volume compared with placebo, effects that were most pronounced among APOE ε4 carriers. Supporting this, FDG-PET findings from Rasgon et al. 20 and Silverman et al. 19 identified preserved metabolism in regions vulnerable to early AD, including the posterior cingulate and precuneus, even after the expected age-related decline. Plasma and CSF data were broadly consistent with the imaging patterns. Baker et al. 22 and Jayachandran et al. 24 reported reductions in circulating Aβ40 levels and Aβ1−42-positive microvesicles among women receiving tE2, while Depypere et al. 27 and Wang et al. 32 observed lower p-tau in both CSF and plasma. Notably, GFAP was not significantly altered by tE2 in microvesicle assays, suggesting that the initial protective effect focuses primarily on the amyloid and tau pathways. 11 Overall, these studies suggest a biomarker pattern consistent with reduced amyloidogenic processing, attenuated tau phosphorylation, and maintained neuronal metabolism in association with early tE2 use.
Oral conjugated equine estrogens
oCEE formulations were more associated with neutral or unfavorable trends. In both the KEEPS-Cog 26 and Kantarci et al. cohorts,21,25 oCEE users showed no significant differences in Aβ deposition compared with placebo. FDG-PET studies19,20 even suggested reduced metabolic activity among oCEE users relative to tE2, especially in temporoparietal regions. Jayachandran et al. noted that oCEE failed to decrease the number of circulating Aβ1−42-positive microvesicles, and in some cases elevated peripheral amyloid levels. These findings suggest that hepatic first-pass metabolism and differential estrogenic receptor activation may weaken the neuroprotective effects of oCEEs in comparison to tE2.
Combined regimens
When progesterone or synthetic progestins were co-administered, results tended toward depletion or reversal of estrogen-related benefits, possibly due through opposing effects on glial reactivity and synaptic signaling pathways. In the study by Rasgon et al., 20 women continuing unopposed estradiol maintained higher metabolic activity on FDG-PET than those who switched to combined regimens. Similar trends were noted by Kantarci et al.21,25 and Coughlan et al.,28,29 where the association between estrogens and progesterone led to greater tau accumulation and accelerated cognitive decline, particularly in late initiators.
Biomarker profile associations with global cognitive scores
Baseline MMSE scores were reported in three studies,22,27,32 although none provided longitudinal global cognitive trajectories. In the study by Baker et al., 22 women with probable AD (mean MMSE 20.95 at baseline) received tE2. After 8 weeks, MHT-naïve participants showed a reduction in plasma Aβ40, which was accompanied by improvement in memory performance measured by the Buschke Selective Reminding Test. The cognitive change was domain-specific, not in global cognition, and the short follow-up precludes conclusions about durability.
In the study by Depypere et al., 27 published in 2022, cognitively healthy, highly educated women (mean MMSE 29.65) were included, but global cognition was not evaluated in the 6-month follow-up, as significant cognitive change was not anticipated in this timeframe.
Overall, while isolated biomarker shifts were sometimes associated with short-term memory improvements in symptomatic populations, the findings from these included studies were not replicated across cognitively normal cohorts nor supported by consistent global cognitive measures. Previous meta-analyses and systematic reviews have shown that MHT has no confirmed benefits for verbal memory or other cognitive domains, even when it is initiated within the first 5 years of menopause.33,34 Observational studies have stated that earlier menopause is linked with worse cognitive performance and that estradiol based-MHT could bring modest improvements in specific domains, however these findings have not been supported by trials, 35 hence the trends towards biomarker-centered analyses. 36
Discussion
The novelty of this review lies not in proposing a new therapeutic indication for MHT, but in integrating AD biomarker evidence across fluid and imaging modalities to clarify how timing, formulation, and biological context may shape divergent findings. Across all studies, tE2 was the formulation most consistently associated with AD biomarker profiles indicative of lower disease risk or pathology, while oCEEs and combined estrogen-progestin regimens tended to show neutral or adverse results. These differences make sense given the distinct pharmacokinetics, receptor affinity, and vascular effects of each compound.37–39 tE2 avoids first-pass hepatic metabolism, yielding steadier hormone levels and fewer prothrombotic effects than oCEEs, constituted by multiple equine estrogens with variable estrogen α and β receptor affinities. CEEs have been linked to greater hepatic production of coagulation factors, contributing to higher venous thromboembolism and cardiovascular risk. Synthetic progestins vary widely in receptor selectivity, promoting different effects that may counterbalance estradiol benefits. Older agents, like medroxyprogesterone acetate and norethisterone, show androgenic or glucocorticoid activity that may blunt estrogen's vascular benefits and impair endothelial function.40,41 A summary of MHT formulation-specific effects on AD biomarkers is represented in Figure 2.
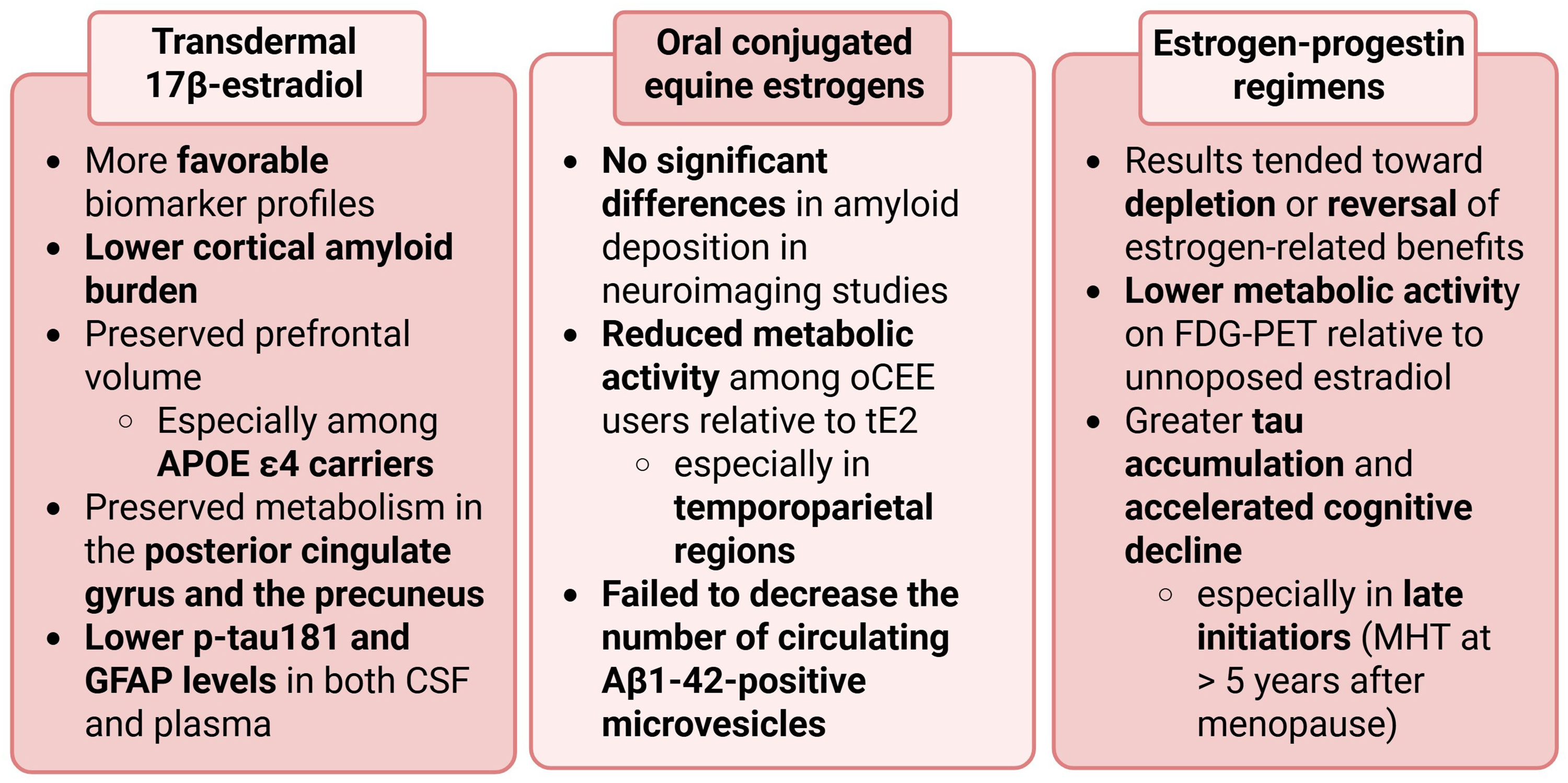
Summary of menopausal hormone therapy (MHT) formulation–specific effects on Alzheimer's disease biomarkers.
Timing appeared to play a key role in MHT cognitive implications: estradiol therapy started within five years of menopause was associated with lower amyloid and tau levels, while delayed use correlated with greater tau deposition and faster cognitive decline. 29 These findings are consistent with the “window of opportunity”, which posits that estrogen's neuroprotective effects may depend on the timing of exposure relative to menopause. 42 Importantly, emerging human imaging data indicate that menopause is accompanied by region- and subtype-specific alterations in estrogen receptor signaling, with evidence of preserved or even increased cerebral estrogen receptor density after menopause, likely reflecting compensatory upregulation in response to estrogen deprivation, rather than a uniform decline in receptor expression. 36 Early tE2 use was associated with preserved metabolism, reduced Aβ deposition, and more stable cortical structure, whereas late exposure often coincided with metabolic decline and tau accumulation. The route of administration also seems to exert an essential role in this complex scenario: oCEE undergoes hepatic first-pass metabolism, altering the estradiol-to-estrone ratio and likely weakening its central effects. 43
The mechanisms proposed by the included studies describe how estrogenic compounds could influence AD-related processes at several biological pathways. Estradiol promotes non-amyloidogenic AβPP processing by increasing α-secretase activity and reducing BACE1 expression21,22,24 and lessens tau phosphorylation through GSK-3β and CDK5 inhibition.27,32 These actions are coherent with lower Aβ and p-tau measures among early MHT users. Estradiol also maintains mitochondrial function and glucose transport, reflected in preserved FDG-PET metabolism in key cortical regions vulnerable in AD.19,20 Its anti-inflammatory role, characterized by reduced microglial and astroglial activation and lower GFAP levels,27,32 likely supports the metabolic and structural advantages seen in imaging studies. On the contrary, synthetic progestins and oCEEs may disrupt these networks by changing receptor signaling and glial reactivity.25,28,29 The interactions between formulation, timing, and the menopausal neurobiological environment across the life-course is represented in Figure 3.
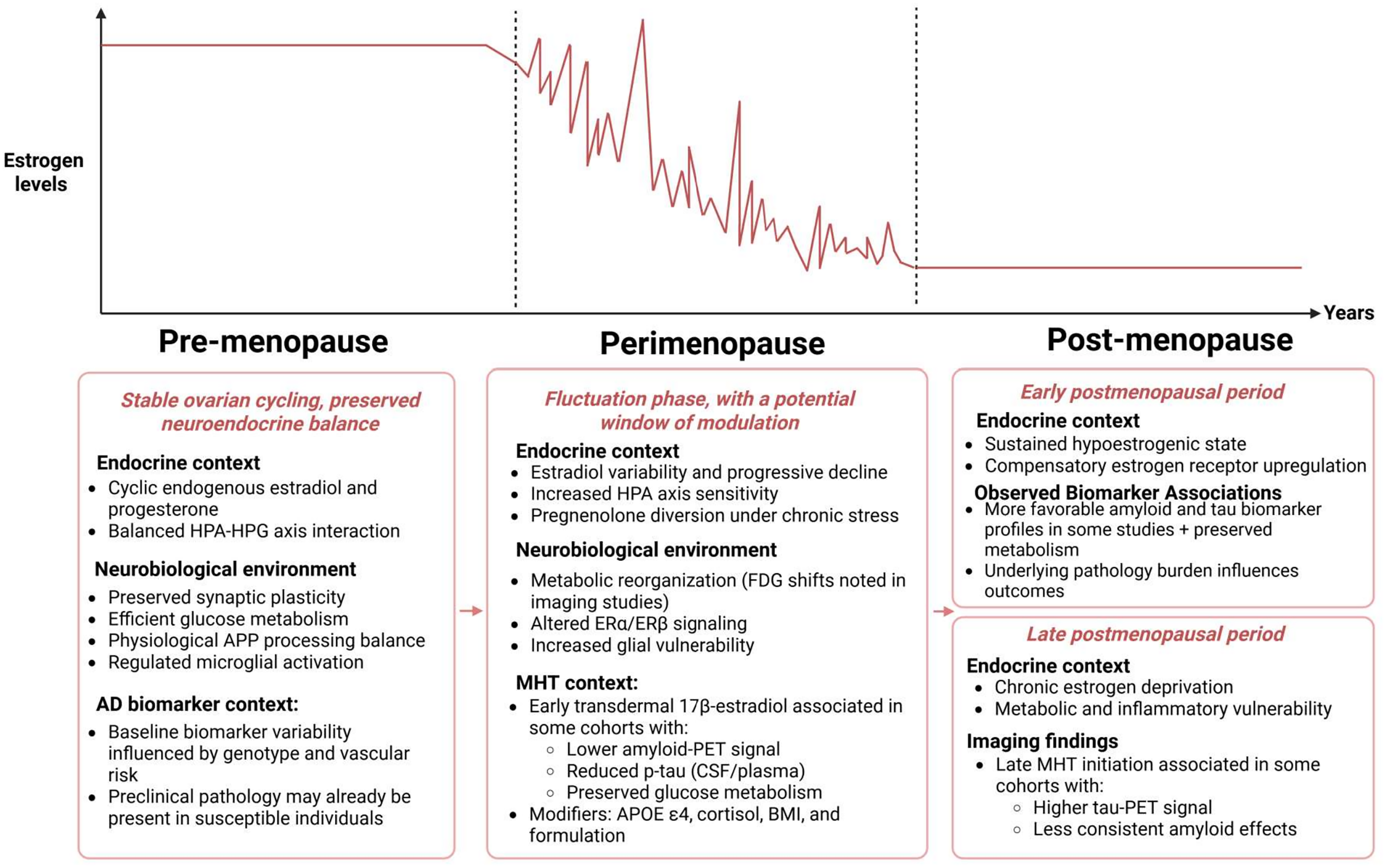
Timing, endocrine context and biomarker trajectories across the manopausal transition.
These mechanistic pathways describe a setting in which early, physiological estradiol exposure protects neuronal and glial function, 44 while delayed or inappropriate regimens interact with the pre-existing pathology, potentially worsening tau and inflammatory cascades. Preclinical data seems to support this hypothesis: prolonged estrogen deprivation may lead to mitochondrial dysfunction, oxidative stress, and increased tau phosphorylation,45–47 whereas timely estradiol replacement may restore synaptic plasticity and glucose metabolism. 20 Estrogen's anti-inflammatory signaling through ERβ and microglial modulation also appears time-dependent, with late exposure enhancing glial reactivity and cytokine release. 3 Therefore, the interaction between formulation, timing, and the menopausal neurochemical environment offers a plausible explanation for the heterogeneity observed across studies.25,26,28,29
The populations across the included studies were predominantly cognitively unimpaired, highly educated postmenopausal women, recruited from research cohorts such as KEEPS and ADNI. Most participants were in early or mid-postmenopause and there was a substantial overrepresentation of white, non-Hispanic women with above-average education levels, with diminished socioeconomic and ethnic diversity. This recruitment pattern narrows the generalizability of findings, as it represents a subset of women with probable high health literacy and access to both expert and preventive care, a reflection of the underrepresentation of diverse populations in AD clinical studies.48,49 Consequently, while results inform mechanisms of estradiol action in healthy brain aging, their applicability to community or clinical populations, especially in low- and middle-income countries, remains limited. Future trials should broaden recruitment to include women with diverse backgrounds and menopausal experiences, in order to capture the full clinical spectrum of hormone-related neurobiology.
APOE ε4 status consistently was a key biological modifier of MHT effects on AD biomarkers, though findings diverged depending on timing, formulation, and disease stage, indicating a non-linear interaction between these factors. In the KEEPS trials,21,25,26 early tE2 use in recently menopausal women was repeatedly associated with lower cortical amyloid load, particularly among APOE ε4 carriers. Kantarci21,25 reported that tE2 users carrying ε4 had markedly lower PiB-PET signal than both placebo and oCEE groups, whereas non-carriers showed no such difference. Long-term follow-up demonstrated that preserved frontal cortical volume correlated with lower amyloid deposition in the tE2 arm, independent of APOE ε4 status, suggesting that structural benefits may extend beyond genotype once amyloid accumulation is reduced. Jayachandran 24 and Zeydan 26 reinforced this pattern, with tE2-treated women ε4 carriers displaying lower global cortical PiB uptake, though limited sample size precluded definitive interaction testing. In contrast, later-life or heterogeneous MHT exposure produced less consistent or even adverse biomarker associations in ε4 carriers. Jauregi-Zinkunegi 31 found that ε4-positive MHT users exhibited worse CSF p-tau/Aβ42 and Aβ42/40 ratios than any other subgroup, implying that exogenous estrogen may exacerbate pre-existing vulnerability once pathological cascades have already begun. In view of these findings, the authors proposed the theory of “healthy-cell bias”, 50 in which estrogens may benefit healthy neurons but accelerate degeneration in those already compromised. This contrasts with the data presented by Depypere et al., 27 who observed stabilization in perimenopausal carriers, highlighting that MHT benefits may be confined to women who initiate therapy before significant neuronal injury or amyloid sequestration occurs. Findings from the study by Wang et al., 32 further underscore this complexity: in non-users, ε4 carriers showed the expected higher amyloid and tau-PET burden, yet among current HT users, APOE genotype no longer predicted biomarker differences, suggesting that MHT may attenuate ε4-related risk when initiated in an optimal window. Coughlan28,29 observed that HT use in older women (>70 years) was linked to faster tau accumulation despite adjustment for APOE ε4, pointing to a possible loss or reversal of benefit with delayed initiation.
Among the identified biological modifiers of MHT impacts on AD biomarkers, there is cortisol, which affects plasma lipid profiles and BBB transport mechanisms. Chronic psychological stress and elevated cortisol have independently been associated with increased brain amyloid load and neurodegenerative risk, particularly in postmenopausal women. 23 Elevated cortisol may interfere with estrogen's neuroprotective and cognitive-enhancing effects, probably due to hippocampal glucocorticoid-estrogen receptor interactions, as discussed in the study by Baker et al., in 2012. 23 It appears to attenuate or counteract the cognitive benefits associated with estradiol by altering neuroendocrine and neuromodulatory signaling in brain regions critical for memory and executive function, particularly the hippocampus and prefrontal cortex.51–60 While estradiol alone is associated with improvements in verbal episodic memory, attention, and working memory, concurrent increases in cortisol may shift neural activation beyond the optimal range predicted by the inverted U-shaped arousal-performance relationship, thereby diminishing or reversing these benefits.61–63 Because estradiol also enhances hypothalamic-pituitary-adrenal axis responsiveness,64–66 the combined presence of estradiol and elevated cortisol may produce excessive monoaminergic and stress-related signaling in prefrontal circuits, leading to impaired working memory and reduced cognitive efficiency under stress conditions. 67 An additional mechanistic layer to these estrogen-cortisol interactions lies in the so-called “pregnenolone diversion”. Pregnenolone is a common precursor of both glucocorticoids and sex steroids, and may be preferentially metabolized toward cortisol synthesis under conditions of chronic stress. Such interactions further complicate the neuroendocrine landscape in postmenopausal women, particularly when exogenous estradiol is administered in the context of elevated stress hormone exposure. It is also noteworthy to discuss that changes in peripheral amyloid beta may result from both increased amyloidogenesis within the brain and altered transport mechanisms across the BBB, which are modulated by plasma lipid profiles and, upstream, by cortisol.
Rather than generating a new therapeutic hypothesis, the novelty of this review lies in demonstrating that much of the inconsistency in prior literature can be attributed to conflation of timing of initiation, hormone formulation, and APOE genotype effects, not solely irreproducibility of hormonal effects. Although transdermal estradiol has shown more favorable vascular and metabolic profiles in other organ systems, such findings cannot be automatically extrapolated to neurodegeneration, as the brain represents a distinct endocrine microenvironment, characterized by region-specific estrogen receptor distribution, BBB transport constraints, glial-neuronal metabolic coupling, and activity-dependent mitochondrial demand. Therefore, systemic benefit does not necessarily guarantee central neuroprotection, making a review of MHT impacts on the brain necessary for a better understanding of women's brain health and dementia occurrence.
Prior clinical investigations of MHT have largely relied on cognitive endpoints, which may fail to capture early molecular alterations that precede symptom manifestation by years or decades. Cognitive outcomes represent late, network-level behavioral manifestations of pathology that may emerge decades after initial amyloid and tau dysregulation. In this context, hormonal modulation occurring during peri- and early postmenopause may therefore influence molecular trajectories long before measurable cognitive divergence appears. Investigating MHT through biomarker-centered lenses allows us to assess whether hormonal exposure interacts with core disease mechanisms, independent of cognitive performance. While these findings do not support initiation of MHT solely for dementia prevention, they suggest that when MHT is clinically indicated for menopausal symptoms, timing and formulation may influence neurobiological trajectories in ways not detectable through cognitive testing alone.
Our findings suggest that when MHT is clinically indicated for menopausal symptom management, consideration of timing and formulation may have differential neurobiological consequences. Specifically, early initiation of tE2 appears to align with more favorable biomarker profiles compared with delayed or combined regimens. While this does not establish causality or clinical benefit, due to the previously reported data heterogeneity, it highlights the importance of appropriately discussing MHT in routine practice and promoting individualized decisions regarding MHT initiation. Therefore, these findings should not be interpreted as evidence to initiate MHT for dementia prevention. At present, AD biomarkers should not be used to guide MHT selection outside research settings.
Limitations
One of the key stepbacks of this systematic review relies on the heterogeneity of data reporting, which precluded a formal meta-analysis. Most studies expressed results as regression outputs rather than standardized means and deviations, often using distinct covariate adjustments and biomarker platforms. This inconsistency highlights a recurring problem in neuroendocrine research: the absence of harmonized endpoints, which restricts the strength of evidence synthesis and restrains large-scale recommendations.
A recurrent limitation in the reviewed literature consisted of the lack of detail about the exact hormone therapy regimen. Several studies28–32 referred to participants simply as “MHT users”, with no specification of dosage, route of administration and compound. This absence of details restricts interpretation, due to different metabolism, receptor binding and vascular impact of each type of MHT formulation. These articles were discussed in the biomarker-based analyses for completeness, but could not contribute to the comparisons organized by MHT type, narrowing the scope of the synthesis. Age at menarche was reported infrequently, limiting the analysis of lifetime estrogen exposure as a modifier of biomarker trajectories in our pooled synthesis. BMI was recorded more often and reveals relevant between-study variation. Only a minority of studies adjusted biomarker models for BMI,24,28 and when considered it sometimes covaried with amyloid or metabolic outcomes. Since adiposity affects peripheral estrogen synthesis, inflammation and vascular risk, the heterogeneity in BMI and its inconsistent adjustment across studies is a plausible source of the mixed biomarker results and should be accounted for in future analyses.
According to the GRADE assessment (Supplemental Figure 3, Supplemental Material), the certainty of evidence supporting MHT effects on AD biomarkers ranged from moderate in observational studies to low in randomized trials. This grading reflected structural differences in design, population samples, and variable biomarker methods rather than inconsistency in outcomes. Both study types appear to point towards the same pattern: early transdermal estradiol was associated with more favorable biomarker profiles, while delayed or combined regimens tended to show neutral or adverse results. Both clinical trials and observational works carried inherent selection and exposure bias. It is important to note that biomarker associations do not establish causality, and residual confounding inherent to observational exposure patterns cannot be excluded.
Thus, future work should favor longitudinal, randomized designs with more uniform biomarker definitions and reporting, precise characterization of hormonal regimen, start age and timing, as well as analysis stratified by APOE genotype and other comorbidities. The integration of molecular, imaging, and cognitive endpoints within the same cohorts could clarify the sequence of biological events connecting menopause, hormone therapy, and neurodegeneration. Consistent methodological standards across studies will make it possible to move beyond correlation and establish causal, mechanism-based frameworks for preventive or therapeutic use of MHT in brain aging.
Conclusions
Early tE2 use appears to preserve molecular and metabolic markers of brain health, while delayed or combined regimens may lose this effect or even favor tau accumulation. Establishing standardized biomarker reporting and stratified trial designs will be key to determining when, for whom, and under which conditions MHT can genuinely protect against neurodegenerative change.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261456766 - Supplemental material for Impacts of menopausal hormone therapy on Alzheimer's disease biomarkers: A systematic review
Supplemental material, sj-docx-1-alz-10.1177_13872877261456766 for Impacts of menopausal hormone therapy on Alzheimer's disease biomarkers: A systematic review by Amanda C. Rodrigues, Filipe G. Valério, Carolina B. Moura and Anderson M. P. Da Silva, Gabriel C. N. Tudella, Sephora S. Almeida, Ana Carolina Gomes, Carlos E. M. Oliveira, Samira Luisa Apóstolos-Pereira, Diogo H. Santos in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
ORCID iDs
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Anderson MP da Silva is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available within the article and/or its supplemental material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.