
Abstract
Background
Cognitive remediation (CR) combined with transcranial direct current stimulation (tDCS) has been shown to slow cognitive decline in older adults with mild cognitive impairment (MCI) or remitted major depressive disorder (rMDD). Dysregulated angiogenesis is implicated in early neurodegeneration and may influence response to these interventions.
Objective
To determine whether baseline plasma angiogenesis markers moderate short-term and long-term cognitive response to CR + tDCS in older adults at risk for dementia.
Methods
Nineteen angiogenesis-related plasma biomarkers were measured at baseline in participants from the PACt-MD randomized controlled trial. Participants received active or sham CR plus active or sham tDCS for 8 weeks, followed by semi-annual booster sessions and online CR between visits. Cognitive assessments occurred at baseline, 8 weeks, and yearly. Elastic net regression identified relevant markers and baseline variables associated with the 8-week cognitive change. For selected markers, treatment*marker interactions were tested using multivariable linear regression adjusted for relevant demographic, clinical, and genetic covariates. Significant interactions were further examined using likelihood ratio tests in linear mixed-effects models across follow-up.
Results
In 271 participants, angiopoietin-2, endocan, and VCAM-1 were identified as relevant markers. Out of these three markers, only angiopoietin-2 interacted with treatment (β(SE) = 0.17(0.08), p = 0.04, padj = 0.11, f2 = 0.02), with lower levels associated with greater 8-week cognitive improvement in the active treatment group, controlling for covariates. This moderating effect persisted during follow-up (χ2LRT(3) = 24.9, p < 0.001).
Conclusions
Lower baseline angiopoietin-2 may identify older adults with MCI or rMDD that are more likely to benefit from CR + tDCS.
ClinicalTrials.gov; https://clinicaltrials.gov/study/NCT02386670; NCT02386670.
Keywords
Introduction
Transcranial direct current stimulation (tDCS) is a non-invasive neuromodulation intervention that has been experimentally tested for a variety of conditions characterized by cognitive decline. 1 Cognitive remediation (CR) is a behavioral intervention that targets specific cognitive domains through structured training. 2 CR and tDCS were combined in the Prevention of Alzheimer's Dementia with Cognitive Remediation plus Transcranial Direct Current Stimulation in Mild Cognitive Impairment and Depression (PACt-MD) randomized controlled trial (RCT) to assess whether this combination would slow down cognitive decline and prevent the onset of dementia in older adults with mild cognitive impairment (MCI), remitted major depressive disorder (rMDD), or both. 3 Older adults with MCI or rMDD are at increased risk of dementia, including Alzheimer's disease (AD), making these populations important targets for preventative interventions. 4
In PACt-MD, 5 tDCS was hypothesized to augment the pro-cognitive effects of CR, as both interventions have neuroplasticity-enhancing effects.6,7 CR engages cognitive networks through repeated training of specific cognitive domains, while tDCS modulates cortical excitability and synaptic plasticity.2,7 Delivering neuromodulation during active cognitive engagement may enhance activity-dependent plasticity and strengthen task-relevant neural circuits.6 The RCT showed that CR plus tDCS slowed cognitive decline over a median follow-up of 4 years in this population, especially in those with rMDD. 5
Older adults with MCI or rMDD were selected for the PACt-MD trial because both conditions are associated with elevated risk of progression to dementia and represent populations in which preventative interventions may have the greatest impact. 3 While the specific pathological basis of MDD and MCI may differ, impaired brain plasticity is thought to be an important shared mechanism underlying the increased risk for dementia in both conditions. 5 The PACt-MD trial was conceptualized as an RCT in those at high-risk for progression to dementia, aimed at enhancing cognitive reserve by targeting the prefrontal cortex, a brain region believed to be highly adaptive to change and critical for executive functioning across these diagnostic categories.3,5 Identifying biological factors that influence responsiveness to such interventions may help guide more personalized strategies for preventing cognitive decline in individuals at risk.
In this secondary analysis, we explored angiogenesis markers as moderators of response to PACt-MD. Dysregulated angiogenesis signaling and cerebral vascular dysfunction are implicated in early neurodegenerative processes and may contribute to cognitive decline in at-risk populations.8,9 Angiogenesis may increase cerebral blood flow, which is vital for maintaining brain function and supporting cognitive processes. 10 Neuromodulation interventions, including tDCS, have been shown to affect cerebral angiogenesis,11,12 a highly regulated process that involves various growth factors, cell adhesion molecules, and metabolites. 13 In vitro and pre-clinical models suggest that tDCS accelerates endothelial cell migration and elongation, promotes the secretion of pro-angiogenic factors, and increases capillary density.14,15 While CR is not known to promote angiogenesis, it has been associated with increased cerebral blood flow, 16 which in turn has been associated with angiogenesis in people with cognitive impairment. 8
Thus, we explored whether angiogenesis markers can moderate 17 cognitive outcomes in the PACt-MD participants who were randomized to CR plus tDCS versus sham CR plus sham tDCS. As CR plus tDCS requires considerable time and resources—including near-daily clinic attendance for stimulation, intensive cognitive training, and subsequent booster sessions—identifying predictive biomarkers is particularly important for informing personalized use of this intervention and ensuring that the individuals most likely to benefit are prioritized.
Methods
Study design
This was a secondary analysis of PACt-MD (NCT02386670).3,5 PACt-MD showed that combined CR and tDCS slowed cognitive decline in older adults at risk of cognitive decline, particularly in those with rMDD (with or without MCI) and in those who were not carriers for Apolipoprotein E (APOE) ε4 allele. 5 All participants provided written informed consent as approved by the local research ethics board. Details of the trial, inclusion eligibility criteria, assessments, and collection of blood samples have been described previously.3,5,18 To summarize, eligible participants diagnosed with rMDD (with normal cognitive status), MCI, or rMDD + MCI were randomized to receive either active CR plus active tDCS or sham-CR plus sham-tDCS for 5 days per week for 8 weeks, followed by “booster” sessions 5 days every 6 months until participants had progressed from normal cognitive status to MCI or MCI to dementia, or until the end of study. 5 In this analysis, we included all participants with baseline plasma angiogenesis marker data and cognitive change data, excluding those with past or current cancer, as angiogenesis marker levels have been known to be affected by cancer. 19
Plasma markers of angiogenesis
The following 19 plasma markers were examined in this analysis as they have been known to contribute to angiogenesis13,20–22 and are associated with dementia or cognition. They were measured simultaneously using the Luminex® LX200 platform (Luminex Corp., Austin, TX, USA) and a customized multiplex immunoassay from R&D/Biotechne (Minneapolis, MN, USA) as described previously 18 : Angiogenin, 23 angiopoietin-1, 24 angiopoietin-2, 25 endothelial cell-specific molecule-1 (endocan), 26 endostatin, 27 e-selectin, 28 hepatocyte growth factor (HGF), 29 interleukin-33 (IL-33), 30 suppression of tumorigenicity-2 (ST2), 30 oncostatin-M, 31 platelet-derived growth factor-AA (PDGF-AA), 32 platelet-derived growth factor AB (PDGF-AB), 33 placental growth factor (PlGF), 34 tissue inhibitor of metalloproteinases-1 (TIMP-1), 35 vascular cell adhesion molecule-1 (VCAM-1), 36 VEGF,37,38 VEGF receptor-1(VEGFR1),38,39 VEGF receptor-2 (VEGFR2),38 and VEGF receptor-3 (VEGFR3).39 APOE variants were genotyped using standard TaqMan SNP genotyping assays (LifeTechnologies, Burlington, ON) at the Center for Addiction and Mental Health (CAMH) Biobank and Molecular Core Facility according to standardized genotyping protocols.5
Neuropsychology assessments
The primary outcome of the PACt-MD RCT5 was a composite cognitive score derived from the average z scores of 18 measures across 6 cognitive domains (processing speed, working memory, executive function, verbal memory, visual memory, and language) from 12 neuropsychological tests (Digit Symbol Subtest from Wechsler Adult Intelligence Scale-III: total correct responses; Trail Making Test Part A: seconds per correct connections; Continuous Performance Task: d’ across all three trials; Paced Auditory Serial Addition Test: total correct responses across both types of trials; Clock Drawing: total score; Trail Making Test Part B: ratio of seconds per correct connections for Trail Making Test Part B over Part A; Stroop Neuropsychological Screening: time for color word divided by time for words; California Verbal Learning Test: total correct responses for trials 1–5, percent retained at long delay trial from trial 5 at immediate recall condition, d’ hits and false alarms of recognition yes/no responses; Boston Visual Memory Test, Revised: total correct responses for trials 1–3, percent retained on delayed recall trial; Boston Naming Test: total spontaneous correct responses; Category Fluency: total spontaneous correct responses; Letter Fluency: total score).3 In our primary analysis, we focused on the change in composite cognitive scores from baseline to the end of the 8-week intervention (i.e., the “acute phase” of the RCT), to assess the initial cognitive response to CR plus tDCS3 compared with sham CR plus sham tDCS. For our secondary analysis, we analyzed the composite cognitive scores at timepoints after the 8-week intervention to see if the effects were sustained during follow-up.
Statistical analysis
Data were analyzed using R version 4.4.1. 40 Chi-Square (χ2), Fisher's exact test, 41 or t-tests (t) were used to determine whether there were significant differences in the demographic, clinical, and cognitive characteristics between the overall sample and the subset included in the analysis to assess whether the subset was representative of the overall sample. Missing data for the outcomes and other variables were handled using available case analysis. Data were visually inspected for normality. All baseline plasma angiogenesis marker levels (pg/mL) were log-transformed to better approximate a normal distribution. For the three markers with non-detectable values, PIGF (n = 5), VEGF (n = 71), and IL-33 (n = 87), values were imputed using half of the minimum value 42 for each marker prior to transformation. A priori covariates that can predict cognitive changes included age (in years at study enrollment),43,44 diagnosis (MCI, rMDD, or rMDD + MCI), 45 self-reported gender (female or male), 46 highest level of education (high school and less than high school, university degree and partial university, or graduate degree), 46 APOE ε4 carrier status (non-carriers or carriers with either one/two ε4 alleles), 47 and number of vascular risk factors. 48 The number of the vascular risk factors was based on the presence of the following conditions 48 : hypertension, hypercholesterolemia, smoker status, body mass index (BMI) >= 30 kg/m2, heart disease, diabetes, and history of stroke/transient ischemic attack.
To mitigate the risk of multicollinearity and overfitting, elastic net regressions 49 were performed to select the most relevant variables among the 19 angiogenesis markers, the treatment group assignment, baseline cognitive score, and the six a-priori selected covariates against the 8-week cognitive change scores, using the add-on R packages glmnet and caret with a repeated cross-validation approach (10-fold cross-validation, repeated 10 times) to set hyperparameter combinations based on root mean squared error. To assess their predictive capacity, relevant angiogenesis markers from the elastic net were then individually assessed in linear regression analyses with relevant variables and treatment interaction for coefficient estimates (β) and standard error (SE); false discovery rate (FDR) correction based on the Benjamini-Hochberg method was applied to adjust for p-values of those treatment*angiogenesis marker interaction terms to predict cognitive change during the 8-week period. 50 The likelihood ratio test (LRT) was used to assess statistically significant differences in model fit with the addition of the interaction term (treatment*angiogenesis marker). The effect size of each statistically significant variable was calculated using Cohen's f2. 51 Post-hoc analyses included pairwise comparisons using estimated marginal means and SE with Tukey's method correction to determine where significant differences lie. For any angiogenesis markers that showed significant interactions in the primary analysis, we performed linear mixed-effect random intercept models with addition of time (of the follow-up period) variable using the add-on R package lmerTest. The LRT was conducted to compare the fit of the three-way interaction with angiogenesis marker*time*treatment interaction against the two-way interaction with only time*treatment interaction, testing whether the inclusion of the angiogenesis marker significantly improved model fit.
Results
Participant characteristics
Out of the 418 randomized PACt-MD participants, 5 271 met inclusion criteria for this analysis (Supplemental Figure 1). This subset of participants did not differ from the overall randomized sample (Supplemental Table 1). Demographic, clinical, and cognitive characteristics of the 271 participants included in this analysis are summarized in Table 1.
Demographic, clinical, and cognitive characteristics.
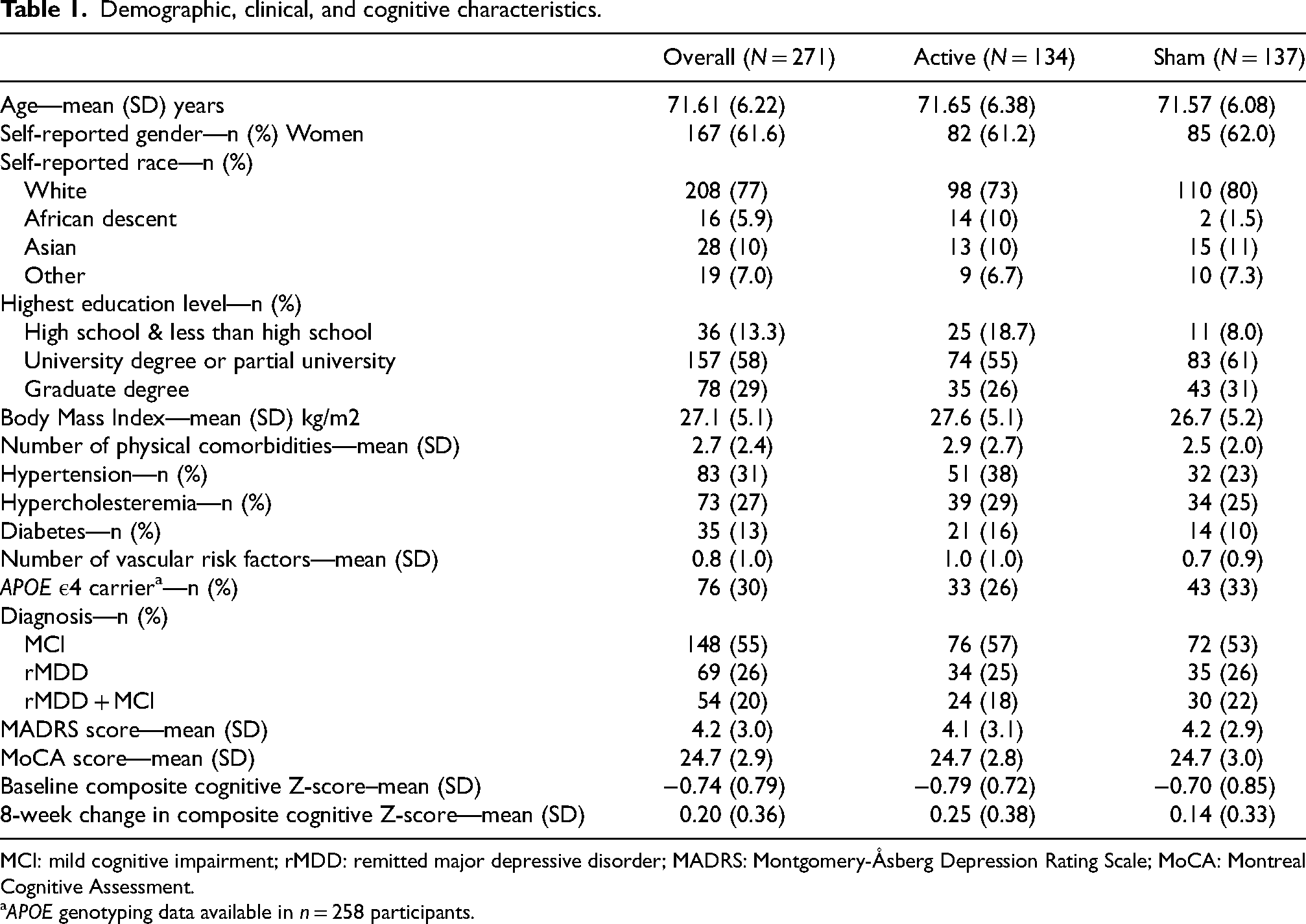
MCI: mild cognitive impairment; rMDD: remitted major depressive disorder; MADRS: Montgomery-Åsberg Depression Rating Scale; MoCA: Montreal Cognitive Assessment.
APOE genotyping data available in n = 258 participants.
Angiogenesis marker levels and 8-week cognitive response to treatment
Among the 19 baseline angiogenesis markers and other variables, elastic net regression identified 3 angiogenesis biomarkers and 7 demographic and clinical variables for cognitive changes, with the following non-zero regression coefficients: angiopoietin-2 (−0.018), endocan (−0.036), VCAM-1 (−0.0013), age (−0.0020), education (−0.036), APOE ε4 carrier status (−0.029), diagnosis (0.0080), vascular risk factors (0.015), treatment group assignment (−0.038), and baseline cognitive composite scores (−0.038).
As shown in Table 2, controlling for other relevant variables in the model, angiopoietin-2 and treatment had an interaction effect on the cognitive response (p = 0.04, padj = 0.11; Figure 1). Lower baseline levels of angiopoietin-2 predicted greater cognitive improvement in the active treatment group only (Table 2, Figure 2). The interaction between treatment and angiopoietin-2 had additional effects on the model (χ2LRT(1) = 4.7, p = 0.03). In this model, the presence of APOE ε4 was also inversely associated with cognitive improvement, and older age was associated with less cognitive improvement. Within the model, there was no evidence of an overall effect of diagnostic group on cognitive improvement (F(2, 246) = 1.98, p = 0.14), and post-hoc comparisons using Tukey's adjustment indicated no differences in cognitive improvement between diagnostic groups. The other two relevant angiogenesis markers at baseline, endocan and VCAM-1, did not interact with treatment to predict cognitive changes at the 8-week follow-up, controlling for other relevant variables (Supplemental Tables 2 and 3; Supplemental Figures 2 and 3).
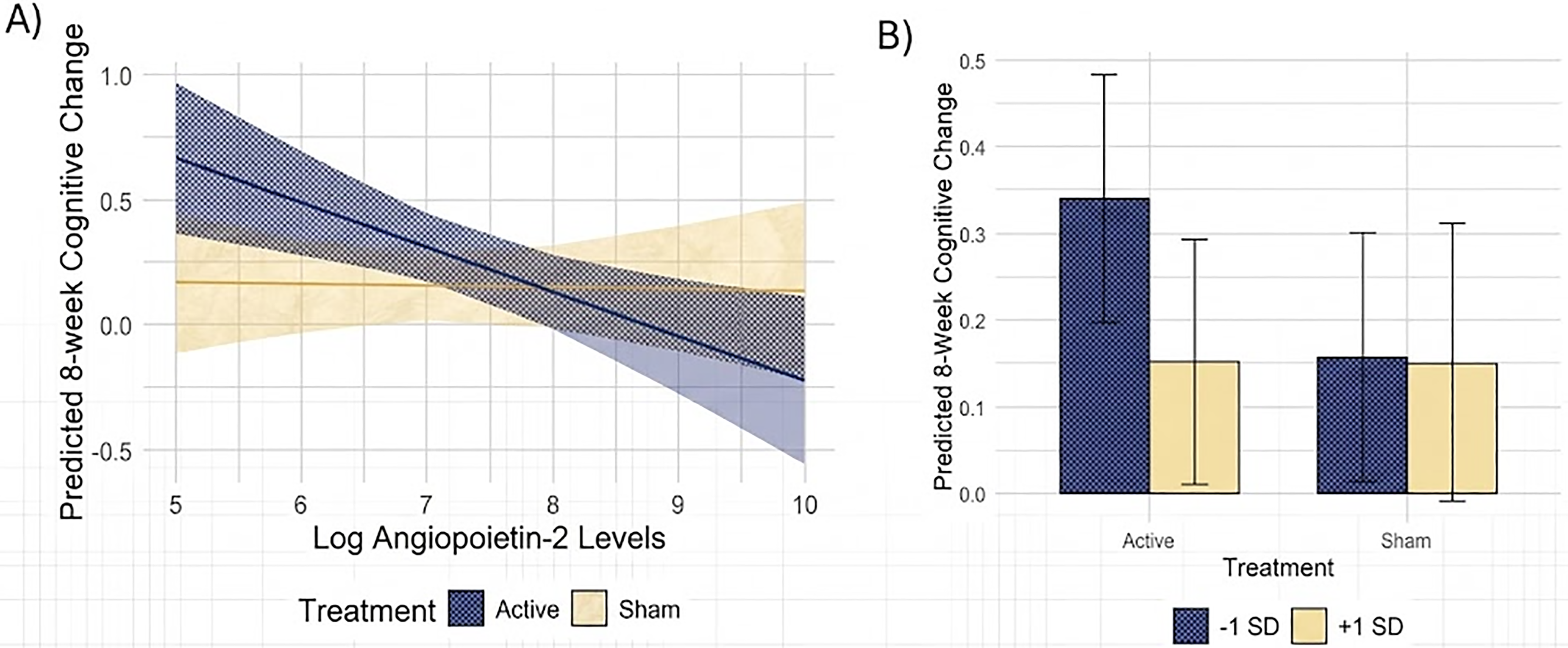
The interaction effect of log angiopoietin-2 levels and treatment group on the 8-week cognitive change. (A) The interaction plot of log angiopoietin-2 levels and predicted 8-week cognitive change between treatment groups. Positive values indicate improvement in global cognition at the 8-week assessment from baseline. (B) Predicted cognitive changes in response to treatment for low (−1 SD) and high (+1 SD) 52 values of log angiopoietin-2 marker levels.
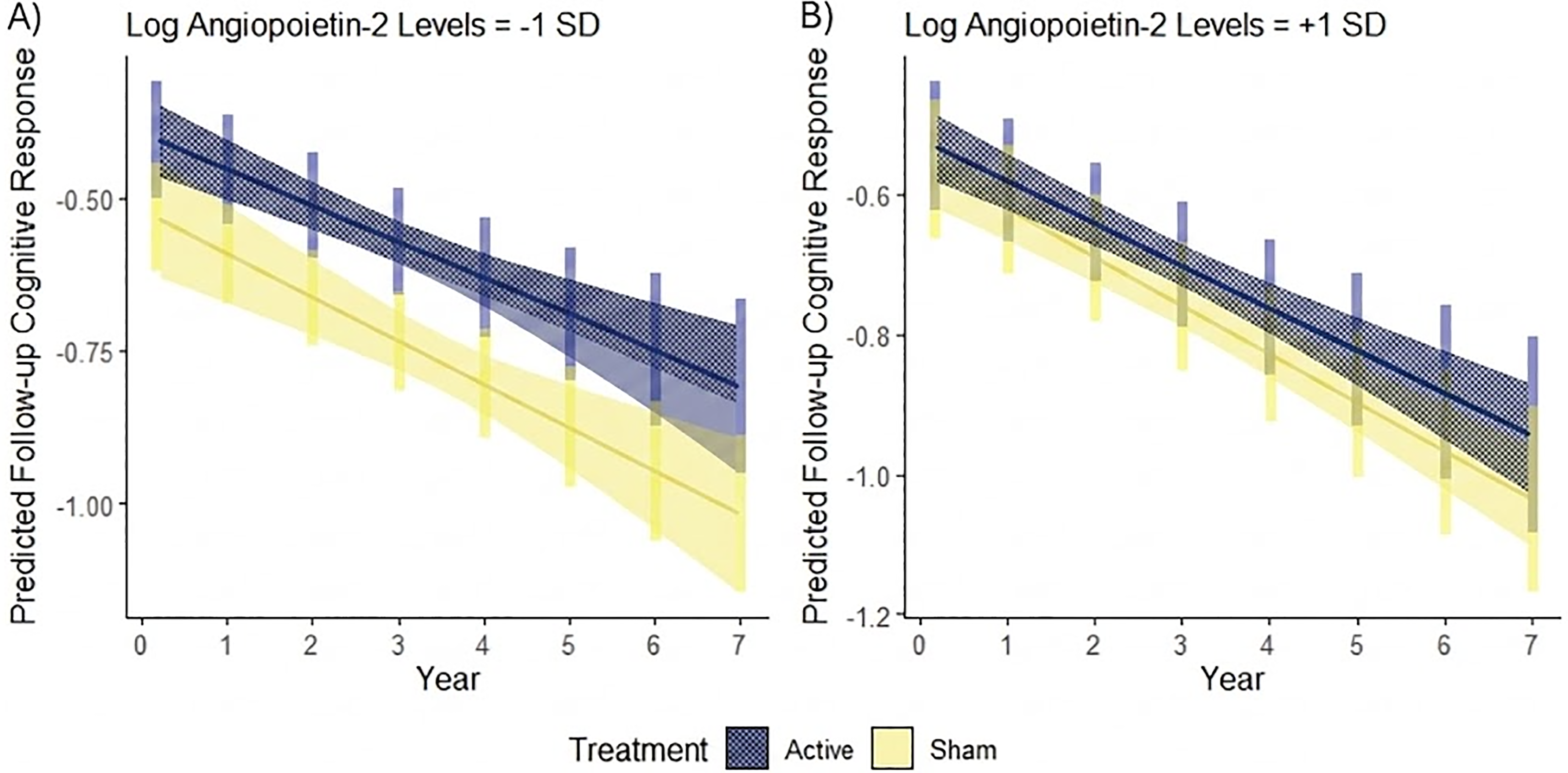
The moderation effect of log angiopoietin-2 levels on treatment group effect on the predicted follow-up cognitive response over time. (A) Low (−1 SD) and (B) high (+1 SD) 52 log angiopoietin-2 marker levels on the predicted cognitive response in response to treatment during follow-up.
Multiple linear regression on angiopoietin-2 and 8-week cognitive changes with other relevant variables.
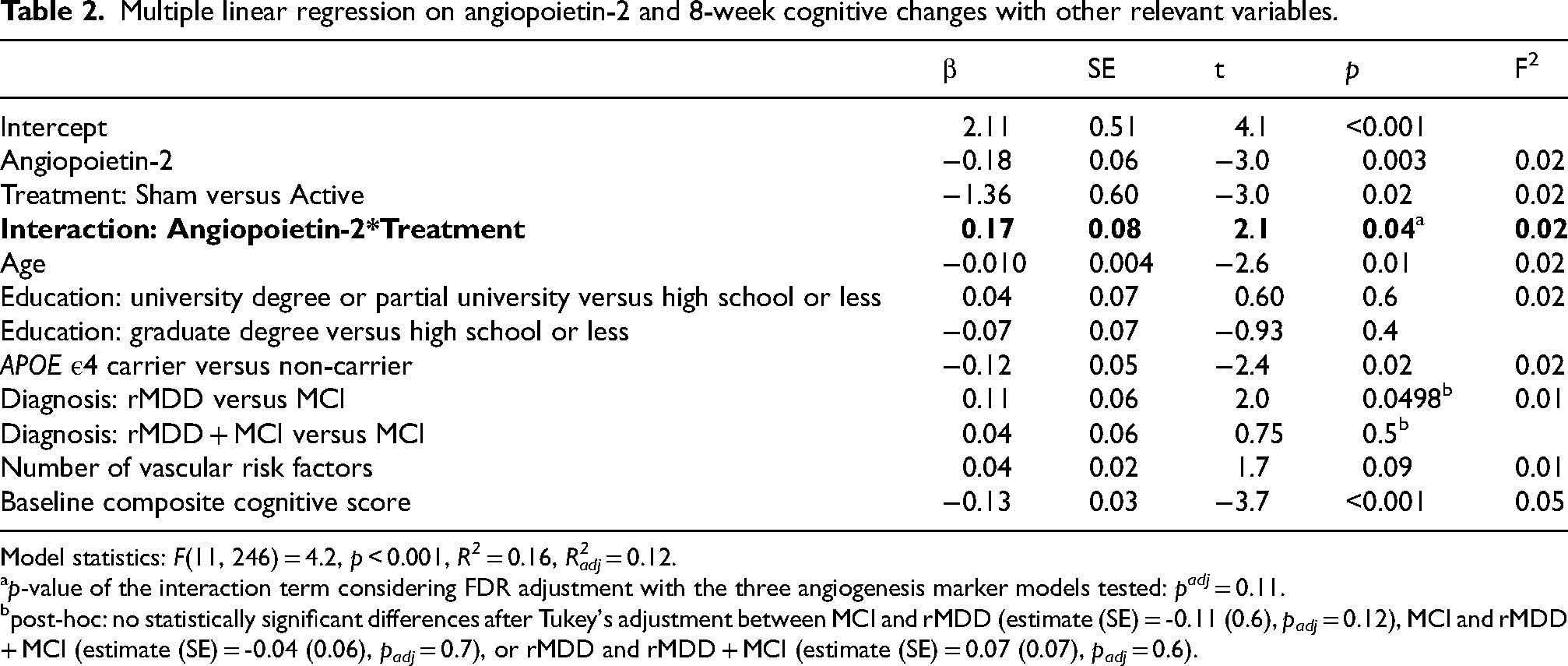
Model statistics: F(11, 246) = 4.2, p < 0.001, R2 = 0.16, Radj2 = 0.12.
p-value of the interaction term considering FDR adjustment with the three angiogenesis marker models tested: padj = 0.11.
post-hoc: no statistically significant differences after Tukey's adjustment between MCI and rMDD (estimate (SE) = -0.11 (0.6), padj = 0.12), MCI and rMDD + MCI (estimate (SE) = -0.04 (0.06), padj = 0.7), or rMDD and rMDD + MCI (estimate (SE) = 0.07 (0.07), padj = 0.6).
For the secondary analysis, the three-way interaction between treatment, time, and angiopoietin-2 improved model fit, suggesting that cognitive decline over time differed by treatment group and were moderated by angiopoietin-2 levels during follow-up (χ2LRT(3) = 24.9, p < 0.001; Figure 2).
Discussion
This study suggested angiopoietin-2 as a possible moderator of response to CR plus tDCS while controlling for known covariates, including: age, diagnosis, education, APOE ε4 carrier status, and vascular risk factors. The elastic net regression facilitated variable selection and regularization, 49 identifying three (among 19 potential) angiogenesis predictors most relevant to cognitive change: angiopoietin-2, endocan, and VCAM-1. Of those, the individual interaction models suggested that only angiopoietin-2 was associated with the cognitive outcome of the intervention: people with lower baseline angiopoietin-2 levels appeared to have better cognitive response to the combined intervention, although this finding did not have a large enough effect size to remain significant after adjusting for multiple comparisons. Subsequent analysis on the cognitive decline during follow-up showed that this moderating effect of angiopoietin-2 was sustained after the acute 8-week intervention.
Different markers can reflect different aspects of the angiogenesis process. In particular, angiopoietin-2 is a context-dependent regulator of angiogenesis, while VCAM-1 and endocan more broadly reflect endothelial activation and vascular remodeling states that can accompany angiogenesis.26,36,52 Angiopoietin-2's suggested regulatory mechanisms may explain why it was identified as the top indicator to moderate cognitive response in this study. As a tightly regulated growth factor, it destabilizes the vessels by inhibiting the phosphorylation of the Tie2 receptor by angiopoietin-1. 53 The destabilization can lead to angiogenesis in collaboration with other pro-angiogenic factors, such as VEGF, or vessel regression in their absence. 53 If Tie2 is low, angiopoietin-2 can also switch to bind integrins, promoting angiogenesis. 53 In MCI and AD, high angiopoietin-2 have been suggested to be associated with blood brain barrier leakiness, indicating dysregulated angiogenesis. 54 Hence, lower angiopoietin-2 in our findings might indicate better angiogenic balance with vascular stability. A more stable vascular environment may allow for better neurovascular coupling, the ability to match blood flow to neural activity 55 ; this could enhance responsiveness to CR 56 and tDCS. 7
To our knowledge, no previous studies have reported the relationship between angiogenesis markers and CR or tDCS in older adults with MCI or rMDD. There was a small study in minimally conscious traumatic brain injury patients, which found that tDCS reduced serum angiopoietin-2 and interferon gamma-induced protein 10, a pro-inflammatory marker, but increased VEGF-C, a pro-angiogenic marker. 57 Compared to our trial, the cohort sample size was much smaller at n = 10; the tDCS placement and duration were also different from our set-up. 57 The background pathologies of the target populations are also quite different; traumatic brain injury features structural brain damage and neuroinflammation caused by an external mechanical force, while MCI and rMDD face progressive alterations in neurobiological systems. Nevertheless, it suggests that reduced angiopoietin-2 along with increased VEGF-C could indicate beneficial controlled angiogenesis instead of dysregulated angiogenesis. In addition, CR may be indirectly associated with VEGF, which contributes to the angiogenesis mechanisms of angiopoietin-2. 53 CR can increase CBF, 16 which was found to be associated with serum levels of VEGF in older adults with MCI and mild AD. 8 Further research on the expression of other angiogenesis markers in the physiologic environment with angiopoietin-2 can help elucidate its angiogenesis effects.
Our results suggest that angiopoietin-2 interacts with the cognitive outcome of CR plus tDCS, a novel intervention that has been shown to slow down cognitive decline in older adults at risk of dementia. 5 However, our study has some limitations. First, the adjusted p-value after FDR correction for three interaction terms is 0.11, above the standard threshold of 0.05 defining statistical significance. As this analysis was exploratory, future work in a separate dataset is needed to confirm the current findings. Additionally, it is not possible to distinguish whether the moderating effect of angiopoietin-2 on the cognitive response is due to CR or tDCS or both through this trial design and this should be investigated further in future studies. In different conditions, such as with traumatic brain injury mentioned previously, tDCS has shown potential to directly increase levels of angiogenesis markers; yet, CR has also been mechanistically linked with angiogenesis markers through CBF in older adults with cognitive impairment. Furthermore, since the majority of our participants were white and highly educated, it limits the generalizability of our findings to broader population. Moreover, in this parallel design trial only baseline values of angiogenesis markers were examined; longitudinal changes in angiogenesis markers, particularly within-subject comparisons in a cross-over trial, could provide more evidence on how t change with cognition in response to the intervention. Other interventions, such as physical exercise, may change angiogenesis marker levels as suggested by our recent meta-analysis in older adults. 58 More research is needed to understand how angiogenesis responds to cognitive-enhancing interventions in MCI and rMDD.
Angiogenesis may play a key role in the progression of at-risk groups to dementia, as vascular dysfunction has been implicated as one of the earliest pathological transformations that distinguishes AD from healthy aging.59,60 Our findings show that baseline angiopoietin-2 levels moderated the effect of CR plus tDCS on cognitive remediation in older adults with MCI or rMDD. Lower angipoietin-2 levels may identify those who are more likely to benefit from this novel combined intervention. By enhancing our understanding of how angiopoietin-2 interact with cognitive interventions, we can optimize therapeutic strategies to slow cognitive decline and improve cognitive health in our aging population.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261457934 - Supplemental material for Angiogenesis markers and cognitive response in a randomized trial of cognitive remediation plus transcranial direct current stimulation in older adults at risk of dementia
Supplemental material, sj-docx-1-alz-10.1177_13872877261457934 for Angiogenesis markers and cognitive response in a randomized trial of cognitive remediation plus transcranial direct current stimulation in older adults at risk of dementia by Bing Xin Song, Julian Schecter, Erica Vieira, Damien Gallagher, Breno S. Diniz, Corinne E. Fischer, Alastair J. Flint, Nathan Herrmann, James L. Kennedy, Linda Mah, Benoit Mulsant, Bruce G. Pollock, Tarek K. Rajji, Clement Ma, Krista L. Lanctôt and in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
PACt-MD Study Group: Benoit H. Mulsant, MD, MS (Principal Investigator); Tarek K. Rajji, MD (Co-PI; site PI, Centre for Addiction and Mental Health, Lead, neurostimulation and neurophysiology); Nathan Herrmann, MD (Co-PI; site PI, Sunnybrook Health Sciences Centre), Bruce G. Pollock, MD, PhD (Co-PI); Daniel Blumberger, MD, MSc (Co Investigator); Christopher Bowie, PhD, C.Psych (Co-Investigator; lead, cognitive remediation and neuropsychology); Meryl Butters, PhD (Consultant, neuropsychology); Corinne Fischer, MD (Co Investigator; site PI, St Michael's Hospital); Alastair Flint, MD (Co-Investigator; site PI, University Health Network); Angela Golas, MD (lead, CSF); Ariel Graff, MD (Lead, neurochemistry); James L. Kennedy, MD (Lead, genetics); Sanjeev Kumar, MD (Co-Investigator); Krista Lanctot, PhD, (site PI, Sunnybrook Health Sciences Centre), Lillian Lourenco, MPH (study co-manager), Linda Mah, MD, MHS (Co-Investigator; site PI, Baycrest Health Sciences); Shima Ovaysikia, MA (study co-manager); Mark Rapoport, MD (Co-Investigator); Kevin Thorpe, MSc (Biostatistician); Nicolaas P.L.G. Verhoeff, MD, PhD (Co-Investigator); Aristotle Voineskos, MD, PhD (Lead, neuroimaging). We also acknowledge the contribution of Kathleen Bingham, MD; Lina Chiuccariello, PhD; Tiffany Chow, MD; Pallavi Dham, MD; Breno Diniz, MD, PhD; Dielle Miranda, Carmela Tartaglia, MD; and the PACt-MD Research Staff. Genotyping was performed by the CAMH Biobank and Molecular Core Facility (previously CAMH Microarray Facility) and funded by the Discovery Fund. APOE variants rs7412 and rs429358 were genotyped using standard TaqMan SNP genotyping assays (LifeTechnologies, Burlington, ON) as per the manufacturer's directions. The authors would like to thank Huijue Wang and Alina Lee for their statistical analysis support.
Ethical considerations
All participants provided written informed consent as approved by the local research ethics board.
Consent to participate
All participants provided written informed consent as approved by the local research ethics board.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has been made possible by Brain Canada through the Canada Brain Research Fund, with the financial support of Health Canada and the Chagnon Family and the CAMH Discovery Fund. B.H.M held and received support for this work from the Labatt Family Chair in Biology of Depression in Late-Life Adults at the University of Toronto. B.X.S has received funding from the Ontario Graduate Scholarship and CAN-TAP-TALENT Doctoral Award supported by the CIHR. K.L.L has received a grant from CIHR (PJT 183584). C.E.F has received funding from Novo Nordisk, ADDF, NIH, NIA, CCNA, CIHR, and the Hilary and Galen Weston Foundation. T.K.R. has received research support from Brain Canada, Brain and Behavior Research Foundation, BrightFocus Foundation, Canada Foundation for Innovation, Canada Research Chair, CIHR, Centre for Aging and Brain Health Innovation, National Institutes of Health, Ontario Ministry of Health and Long-Term Care, Ontario Ministry of Research and Innovation, and the Weston Brain Institute. T.K.R. also received for an investigator-initiated study in-kind equipment support from Newronika, and in-kind research online accounts from Scientific Brain Training Pro, and participated in 2021 and 2022 in an advisory activity for Biogen Canada Inc. Between September 1, 2023 and September 30, 2024, T.K.R. was an ex officio member of the Board of Trustees of the CAMH in his role as Chair of the Medical Advisory Committee at CAMH. T.K.R. maintains a collaborator scientist and a courtesy appointment at CAMH and a Status-Only appointment at the University of Toronto. T.K.R. is also an inventor on the United States Provisional Patent No. 17/396,030 that describes cell-based assays and kits for assessing serum cholinergic receptor activity.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.S.D is a consultant to Bough Bioscience Inc in an area unrelated to the current work. C.E.F. receives grant support from Novo Nordisk, the Hilary and Galen Weston Foundation, ADDF, NIH/NIA, CIHR/CCNA, Temerty-Tanz-TDRA. A.J.F has received grant support from the U.S. NIH, Patient-Centered Outcomes Research Institute, CIHR, Brain Canada, Ontario Brain Institute, Alzheimer's Association, AGE-WELL, the Canadian Foundation for Healthcare Improvement, and the University of Toronto. J.L.L is a member of the SAB of Myriad Neuroscience Inc and is an author on patents for pharmacogenetic testing. B.H.M. holds and receives support from the Labatt Family Chair in Biology of Depression in Late-Life Adults at the University of Toronto. He currently receives or has received within the past three years research support from Brain Canada, the CIHR, the CAMH Foundation, the Patient-Centered Outcomes Research Institute (PCORI), the U.S. NIH, and HAPPYneuron (software used in a study founded by Brain Canada). T.K.R has received research support from Brain Canada, Brain and Behavior Research Foundation, BrightFocus Foundation, Canada Foundation for Innovation, Canada Research Chair, CIHR, Centre for Aging and Brain Health Innovation, NIH, Ontario Ministry of Health and Long-Term Care, Ontario Ministry of Research and Innovation, and the Weston Brain Institute. T.K.R. also received for an investigator-initiated study in-kind equipment support from Newronika, and in-kind research online accounts from Scientific Brain Training Pro, and participated in 2021 and 2022 in an advisory activity for Biogen Canada Inc. Between September 1, 2023 and September 30, 2024, T.K.R. was an ex officio member of the Board of Trustees at CAMH in his role as Chair of the Medical Advisory Committee at CAMH. T.K.R also received for an investigator-initiated study in-kind equipment support from Newronika, T.K.R. maintains a collaborator scientist and a courtesy appointment at CAMH and a Status-Only appointment at the University of Toronto. T.K.R. is also an inventor on the United States Provisional Patent No. 17/396,030 that describes cell-based assays and kits for assessing serum cholinergic receptor activity. K.L.L. has received consulting fees from Boehringer Ingelheim, Bristol Meyers Squibb, Eisai Co. Ltd, Exciva, Ironshore Pharmaceuticals, H Lundbeck A/S, Novo Nordisk, Otsuka and Praxis Therapeutics.
K.L.L is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
Data availability statement
The data generated and analyzed in the current study is available from the PACt-MD Study Group upon request as described previously. 5
Supplemental material
Supplemental material for this article is available online.