
Abstract
Background
Language and communication disorders in dementia with Lewy bodies (DLB) remain understudied and have rarely been explored from the caregiver's perspective. Comparative studies with Alzheimer's disease (AD) are also limited.
Objective
To provide an initial overview of language and communication profiles in DLB, compared to AD and healthy elderly controls (HC); to assess subjective complaints reported by patients, caregivers and healthcare professionals; and to explore their relationships with rapid language screening. A further aim was to aid non-specialist professionals in identifying patients needing speech therapy referral.
Methods
Seventeen DLB patients, 15 AD patients, and 11 HC completed the Diagnostic Tool for Language Assessment and the alpha version of the Communication Support Needs Assessment Tool for Dementia (CoSNAT-D), alongside a semi-directed interview (SDI). Proxy-ratings were also collected from caregivers and healthcare professionals (HP) for the CoSNAT-D and SDI.
Results
Compared to HC, DLB patients showed significantly poorer performance in repetition, verbal working memory, sentence comprehension and dictation, and reported more communication difficulties. Compared to AD patients, DLB patients had greater impairments in phonemic fluency, and more frequent reports of discomfort, vocal changes, and difficulties with writing and handwriting execution. Perceptions of communicative difficulties and their functional impact varied across patients, caregivers, and HP.
Conclusions
This study has identified distinct language and communication deficits in DLB versus AD and HC. Discrepancies between patient and caregiver perceptions were frequent in both groups and may contribute to increased caregiver burden. Findings highlight the potential value of rapid screening tools to better support patients and their caregivers.
Keywords
Introduction
Dementia with Lewy bodies (DLB) is the second most common cognitive neurodegenerative disorder after Alzheimer's disease (AD), accounting for 15–20% of major neurocognitive disorder cases. 1 This occurrence could well be far higher since it has been suggested that two-thirds of DLB patients could be misdiagnosed or remain undiagnosed. 2 The core clinical features of DLB are fluctuations (in cognitive abilities, attention, and alertness), visual hallucinations, rapid eye movement sleep behavior disorder (RBD) and features of parkinsonism (bradykinesia, rigidity or rest tremor). 3 To diagnose probable DLB, two or more of the aforementioned manifestations must be present. Although there is considerable individual variability in DLB, patients generally share common features from the prodromal stage onwards, namely a subcortico-frontal syndrome, 4 visuoperceptive and visuospatial disorders5,6 and working memory impairments. 7
Although a small number of literature reviews have examined, at least partially, the subject in DLB,8–11 language and communication disorders remain poorly characterized in DLB patients.9,12 In contrast, these impairments have been extensively documented in AD. In addition, very few studies have directly compared language and communication characteristics in DLB and AD.8,10,12,13
Verbal fluency and naming skills appear to be impaired from the earliest DLB stages.8,10,14 Phonemic fluency impairment is widely considered to reflect underlying executive dysfunction10,14,15 and appears consequently to be more severely affected in DLB than in AD15–17; whereas no significant differences have been consistently reported for semantic fluency.17–20 Findings regarding naming performance are heterogeneous 8 : some studies have reported greater deficits in AD patients than in DLB patients,17,21 while others found no significant difference. 18 The nature of errors would be predominantly semantic in AD and visual-perceptual in DLB. 21 DLB patients also demonstrate impairments in both the production22,23 and comprehension22,24 of narrative discourse. However, at early stages, DLB patients seem to be less impaired in narrative discourse and more informative than AD patients. 25 Furthermore, syntactic processing deficits have been observed in DLB patients and appear to correlate with working memory impairment.26,27 Impaired verbal working memory in DLB, likely related to underlying executive dysfunction,4,7 in turn affects sentence comprehension. The few studies that have explored comprehension skills reported no significant difference between the two conditions.28–30 Finally, presentation of pictorial material increases language difficulties due to visual-perceptual disorders in DLB. 13 These neurovisual impairments also cause peripheral reading impairment.9,13,31
However, as summarized by Macoir, 9 reading disorders in DLB have not been specifically studied and the few studies that have directly compared reading between AD and DLB have not reached a consensus. In some cases, no difference was found between the two groups, 31 while in others, DLB patients seemed to have a more deficient reading performance than AD patients for word reading. 13 Spelling performance can be impaired from the early stages of DLB, with more pronounced difficulties observed for sentences and non-words than for single words. In addition, most patients with DLB exhibit handwriting abnormalities and report recent changes in their writing style. 32 Handwriting appears to be significantly more impaired in DLB than in AD, 31 although the specific nature of these impairments has not yet been characterized. Writing difficulties in DLB could involve graphomotor impairment related to parkinsonism but also higher-order cognitive deficits such as attention, working memory, alertness, executive functions, 32 visuoperceptual, and visuospatial deficits.4,28
Finally, to the best of our knowledge, only two studies have looked at verbal communication and only one at non-verbal communication in DLB. Patients with DLB showed a decrease in speech flow and word-finding difficulties. 33 In addition to these impairments, DLB patients’ verbal communication was characterized by a diminution in voice volume and in articulatory precision, as well as a reduction and inadequate use of prosody. Comprehension problems were also common. 34 As far as we are aware, only two studies have compared the communicative features of AD and DLB. While DLB patients tended to use circumlocutions, AD patients would have greater recourse to face-saving responses than DLB patients. 35
Communication skills are directly affected by language difficulties. Day-to-day interactions with caregivers can become increasingly challenging, potentially leading to misunderstandings and frustration. 36 In addition, language disorders increase the caregiver's workload. 37 The link between language disorders and caregiver burden is notably mediated by behavioral disorders. Communication difficulties often lead to negative emotional responses in patients, such as frustration, which can in turn give rise to behavioral symptoms that further exacerbate caregivers’ burden.38,39 As interactions deteriorate, a deleterious cycle may emerge, marked by the development of negative attitudes from caregivers toward the patient. Such dynamics can accelerate the decline of cognitive and motor functions, increase the levels of disability and heighten emotional distress in patients.40,41 In this context, language disorders often worsen, reinforcing a vicious cycle that further impairs communication and care.
Although DLB is the subject of growing scientific interest, the study of language and communication disorders in these patients is still emerging. Indeed, despite clinical reports of language/communication-related complaints and the significant impact these have on the paramedical follow-up and quality of life for both DLB patients and their caregivers, research on this topic remains limited. In contrast to DLB, language and communication impairments in AD have been extensively studied and documented. Existing comparisons between AD and DLB are scarce and typically focus on isolated language domains, such as naming and verbal fluency, without offering a comprehensive assessment of language functioning or exploring its relationship with communicative abilities. Integrating language and communication into research is crucial for developing ecologically valid approaches that reflect the everyday challenges faced by patients and their families. Therefore, there is a pressing need for more comprehensive and direct comparative studies, including language and communication aspects, between AD and DLB patients.
The main aims of our study were to provide an initial overview of the language and communication profile of DLB patients, compared with AD patients and healthy elderly controls (HC) and to characterize the initial complaint and subjective perception of communication difficulties in patients, their caregivers and healthcare professionals (HP). We also aimed to expand this preliminary assessment with more detailed qualitative data and to correlate these communication findings with a rapid assessment of the different domains of oral and written language, in both expression and comprehension.
In light of the existing literature, we hypothesized that DLB patients in prodromal to moderate stages would demonstrate language disorders, as well as a subjective complaint about daily communication. We also assumed that the communication and language profile would differ between DLB and AD patients. Specifically, reflecting the predominant executive, visuospatial, and motor impairments in DLB and consistent with existing literature, we hypothesized that DLB patients would exhibit greater deficits in phonemic fluency, writing, and working memory compared to AD patients, as well as potential impairments in sentence comprehension and repetition as a direct consequence of working memory deficits. In addition, we expected to observe a discrepancy in the perception of difficulties and their impact between patients, their caregivers and the interviewed HP.
In order to facilitate a subsequent translation of our findings into recommendations for daily clinical practice, we chose to employ rapid tests that can be used routinely for the assessment and monitoring of patients. These tests should be easy to use for HP who do not have in-depth expertise in communication and language impairments, but who may be in charge of identifying language disorders in these patients and referring them for the necessary speech–language therapy.
Methods
Study population
Forty-three people participated in the study, comprising 17 DLB patients, 15 AD patients and 11 HC. All participants were recruited from the tertiary memory clinic of Strasbourg University Hospital, France, including the geriatrics and neurology departments.
Twenty patients were selected from therapeutic studies currently taking place at the memory clinic. Six DLB patients were selected from the EIP study (EIP22-NFD-505). Fourteen AD patients were selected from the following studies: ENVISION (221AD305) (n = 1), Clarity (BAN2401-G000-301) (n = 2), Gabriella (BP44745) (n = 3), ARIBIO (AR1001-ADP3-US01) (n = 2), EVOKE (NN6535-4730) (n = 5), and EVOKE plus (NN6535-4725) (n = 1). These protocols are employed to assess the effects of the administered compounds on global cognitive decline, synaptic plasticity, and brain connectivity. Consequently, the pharmacological treatments may indirectly affect language and communication functions.
To complete our sample, we required approval from the Research Ethics Committee (CER) of the University of Strasbourg. Our “CommLewy” study (Unistra/CER/2024-12) was approved by the CER on February 22, 2024. We recruited 23 additional participants, including 11 DLB patients, one AD patient and 11 HC.
We collected proxy responses from both caregivers and HP. More precisely, each patient was recruited along with a dedicated caregiver, forming a dyad. Moreover, seven HP participated in the study, including four neurologists/ geriatricians and three neuropsychologists.
All participants had to be native French speakers, be able to understand the aims and risks of the research and give informed, dated and signed consent.
Inclusion criteria were as follows: DLB and AD patients had to be aged 50 years or over, have been diagnosed with probable DLB according to McKeith's criteria3,42 or diagnosed with AD according to Dubois’ criteria 43 and have obtained a Mini-Mental State Examination (MMSE) 44 score greater than or equal to 10 (i.e., prodromal or mild-to-moderate cognitive impairment) at their last medical visit. Patients also needed to be accompanied by a caregiver who volunteered to take part in this study. HC were volunteers aged 50 or over, with no measurable cognitive impairment or complaint (MMSE score greater than or equal to 27). To be included, volunteer medical or paramedical professionals had to have participated in the cognitive assessment and care of the patient at Strasbourg University Hospital.
Exclusion criteria were poor French language abilities, alcohol or substance abuse, sensory or motor disability, an emergency or life-threatening situation, placement under court protection and focal cerebral lesions shown on brain imaging. Additional exclusion criteria were defined for DLB and AD patients: neurological or psychiatric conditions unrelated to DLB and AD, whose symptoms could be confused with those of DLB or AD, and co-occurrence of DLB and AD. Additional exclusion criteria for HC were the presence of cognitive, neurological and/or psychiatric disorders likely to impact cognitive, communicative or language performance. The AD group was restricted to the typical amnestic presentation, excluding atypical variants such as posterior cortical atrophy (PCA) and logopenic variant primary progressive aphasia (lvPPA).
DLB and AD patients and their caregivers, HC and HP provided written informed consent for the audio recording and their participation in this study.
Demographic and clinical data collection
Patients and their caregivers were evaluated at the Centre Mémoire de Ressources et de Recherche (CM2R). The following clinical data were collected for all patients: fluctuations (Mayo Clinic Fluctuations Scale), 45 hallucinations (Parkinson's disease-associated psychosis [PDAP]), 46 parkinsonian syndrome, in particular akinesia, rigidity and tremor at rest (the Unified Parkinson's Disease Rating Scale [UPDRS], part 3) 47 and RBD. 48 RBD was assessed using a sleep questionnaire from Gjerstad et al., 48 simplified into four questions each for the patient and caregiver, one concerning the patient's movements during sleep and the other concerning dreams and nightmares. The MMSE scores were also used to evaluate neuropsychological difficulties and define the stage of mild cognitive impairment for each patient and HC. Finally, patients’ and caregivers’ age and gender were collected.
The language assessment of patients and HC took approximately 45 min to complete. Our protocol comprised two parts, assessing both language and communication. First, we assessed language skills using the Diagnostic Tool for Language Assessment (DTLA), 49 a speech–language pathology screening protocol. Then, we investigated communication abilities using the Communication Support Needs Assessment Tool for Dementia (CoSNAT-D)50,51 alpha version questionnaire intended for patients. To further explore communication aspects, the questionnaire was integrated into a semi-directed interview (SDI), with a more qualitative focus. The caregivers’ interview took an average of 35 min. The same SDI with a few additional questions including the CoSNAT-D caregiver alpha version was proposed to caregivers in order to specify each patient's communication disorders. Lastly, the patients’ HP were required to complete only the CoSNAT-D HP alpha version. The patients, their caregiver and their HP were usually interviewed on the same day.
The DTLA is a tool used to screen and identify language disorders in people with mild cognitive impairment. It takes only 5 to 10 min to complete. It has been standardized and validated for AD, primary progressive aphasia (PPA), post-stroke aphasia patients and HC (French-speaking, Europeans and Quebecers). However, no study has yet been carried out using this test to investigate language disorders in DLB patients. The DTLA authors have identified the language domains most frequently affected in PPA and early-onset dementia. Nine domains are assessed (Supplemental Material 1):
Picture naming: 6 items (2 animals, 1 fruit, 3 objects: rake, racket, whistle) Repetition of words, non-words, sentences: 3 words, 3 non-words, 3 sentences Verbal fluency: most words in 1 min beginning with the letter D Dictation of words and non-words: 3 words and 3 non-words Spontaneous sentence writing Word and non-word reading: 3 words, 3 non-words Sentence comprehension: 3 sentences, yes/no answers Semantic word comprehension: semantic matching (4 items) Alpha-span: 3 items to be repeated in alphabetical order
The number of points obtained in each subtest is added up to obtain a score out of 100. The DTLA includes alert and cut-off thresholds to indicate, respectively, emerging language difficulties and clinically significant impairments prompting either closer monitoring or immediate referral for in-depth assessment. Thresholds vary according to age (under 65, between 65 and 80, over 80) and years of education (11 years or less, 12 years or more).
The CoSNAT-D is a clinical tool developed to assess the communicative needs of patients with dementia, considering the caregiver's perspective and that of a health professional. It is intended to be used in clinical routine by non-specialist clinicians, to facilitate the referral of patients to a speech–language therapist when necessary. Items cover conversational and communicative difficulties, as well as difficulties with understanding, fluency, writing and reading in everyday ecological situations.
The items used in the present study are those initially defined following a Delphi consensus based on a panel of international experts, 50 as a first step in the CoSNAT-D development and validation process. They do not therefore correspond to the final version of the test, which is currently undergoing further validation. Beyond its primary screening and orientation objective, CoSNAT-D has the potential to provide information on the communication profile associated with various cognitive neurodegenerative diseases, as observed in daily routine by non-specialist HP. In the case of highly under-diagnosed and little-known diseases such as DLB, this information could prove invaluable in contributing to better detection and care of these patients. In the absence of standardization and a definitive scoring system, our treatment of the results of this test is therefore limited to a qualitative analysis, supplemented by quantitative comparisons between the DLB, AD and HC groups.
The eight items from the CoSNAT-D alpha version50,51 have been translated into French (Supplemental Material 2) to enable their administration to our population. For each item, one point was awarded when no difficulty was reported (“NO” answer) and zero points when a difficulty was reported (“YES” answer), for a total score out of 8 points.
Finally, an SDI with open and closed questions was designed, partly inspired by the MEC de poche protocol. 52 The CoSNAT-D alpha items were integrated into these SDI questions to explore more qualitatively the communication needs as expressed by the patient (priority complaints, individual goals), as well as their experience of the disorders (the individual's own perception of their ability to communicate) (Supplemental Material 3). An SDI almost identical (61 similar items) to the one administrated to the patient was also carried out to obtain the caregiver's point of view on the patient's communication needs and experience of disorders. The interview consisted of 65 questions for patients and 64 questions for caregivers. Three additional questions concerning their care recipient's lack of precision, reduced speech and awareness of disorders were addressed to caregivers. Four preliminary questions were addressed exclusively to patients, concerning the presence of visual disorders, the wearing of glasses, the presence of hearing disorders and the wearing of a hearing aid. We estimated the average length of these interviews to be 30 min.
For each question, we used a binary score (1 point for a “NO” answer; 0 points for a “YES” answer”). Of the questions addressed to patients and caregivers, 14 were selected for a subsequent quantitative analysis, as well as two of the additional questions intended for caregivers (which concerned their loved one's awareness of disorders and lack of precision).
Patients’ and caregivers’ responses were audio-recorded and transcribed in writing with a view to a second, more qualitative analysis. Of all the questions asked, 16 from the patient's SDI and 17 from the caregiver's SDI (the additional question to caregivers corresponded to the reduction in speech since the onset of the disease) were selected for this purpose.
Statistical analyses
Statistical analyses were performed using JASP software (https://jasp-stats.org) and R (https://www.r-project.org/).
First, we used an ANOVA for the age variable because of the normality of the distribution. Non-parametric Kruskal-Wallis tests and Dunn post-hoc tests were used for hallucinations, fluctuations, akinesia, rigidity, tremor, RBD and MMSE score comparisons. Chi-square (χ2) tests were applied for categorical data (gender). A Student's t-test was also used for the caregivers’ age variable as it was normally distributed.
The difference in distribution of the DTLA's diagnostic categories (standard, alert, cutoff) between AD and DLB patients was studied using the Monte-Carlo simulation of Fisher's exact test.
Moreover, we used Kruskal-Wallis tests and Dunn post-hoc tests to compare intergroup differences (DLB, AD, HC) for DTLA, CoSNAT-D alpha version and SDI scores. The discrepancies in the perception of difficulties between patients, caregivers and HP for the CoSNAT-D were also studied using Kruskal-Wallis and Dunn post-hoc tests. Only the total mean CoSNAT-D scores of DLB patients, caregivers and HP were normally distributed and required ANOVA and Tukey's post-hoc tests to be compared. Supplementary descriptive statistics were conducted to further explore SDI responses.
Finally, we explored the correlations between the CoSNAT-D and the DTLA, and between these two tests and the MMSE score, using Spearman's correlation test.
Results were regarded as significant at p < 0.05.
Results
Demographic and clinical characteristics
Demographic and clinical data of DLB patients, AD patients and HC are presented in Table 1. There was no difference in terms of age (p = 0.932) and gender (p = 0.446). MMSE scores of DLB and AD patients were significantly lower than those of the HC group (p < 0.001). MMSE scores did not differ between DLB and AD patients.
Demographic and clinical characteristics of the cohort.
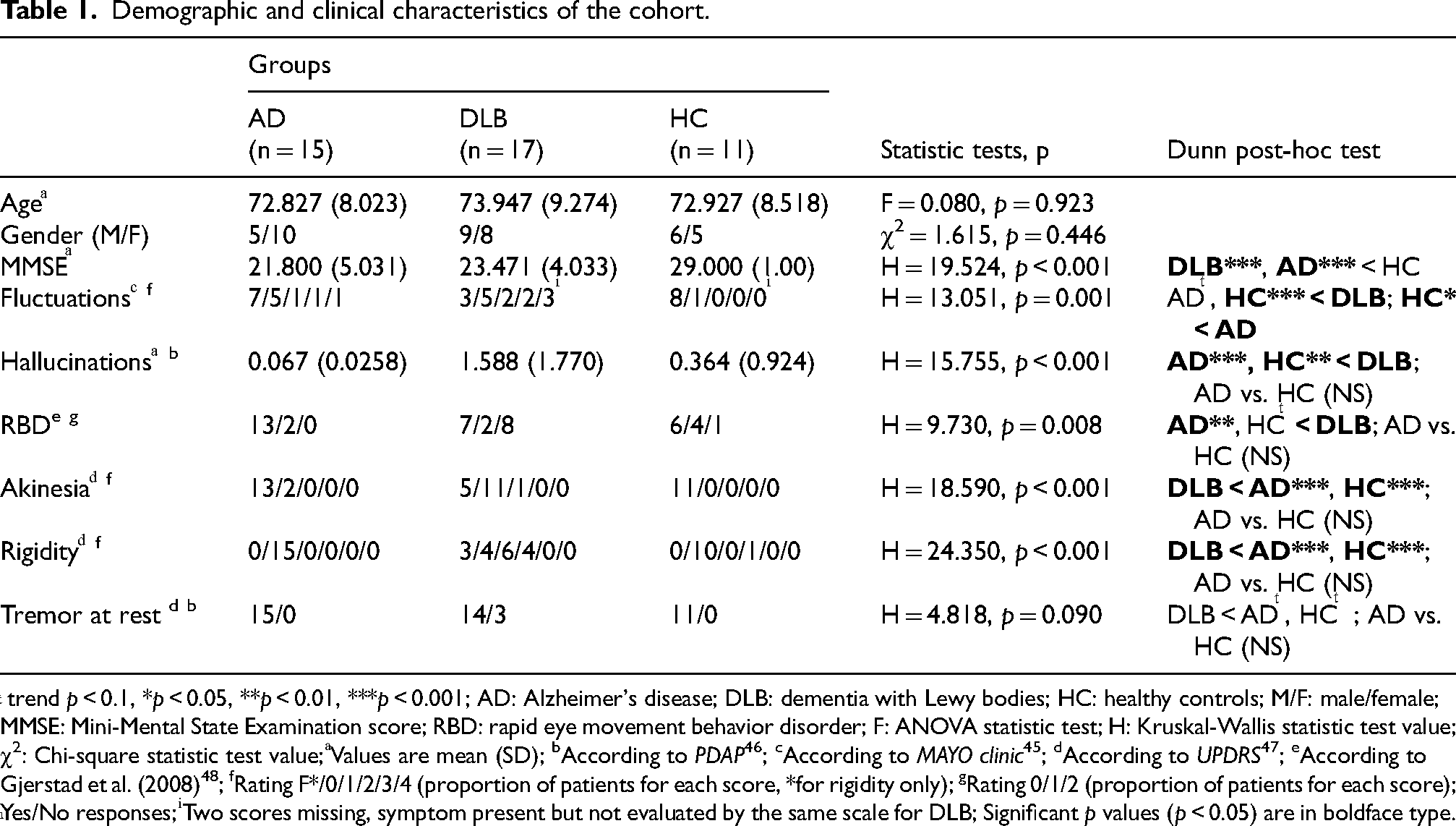
ͭ trend p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001; AD: Alzheimer's disease; DLB: dementia with Lewy bodies; HC: healthy controls; M/F: male/female; MMSE: Mini-Mental State Examination score; RBD: rapid eye movement behavior disorder; F: ANOVA statistic test; H: Kruskal-Wallis statistic test value; χ2: Chi-square statistic test value; ͣValues are mean (SD); bAccording to PDAP 46 ; cAccording to MAYO clinic 45 ; dAccording to UPDRS 47 ; eAccording to Gjerstad et al. (2008) 48 ; fRating F*/0/1/2/3/4 (proportion of patients for each score, *for rigidity only); gRating 0/1/2 (proportion of patients for each score); ͪYes/No responses; ͥTwo scores missing, symptom present but not evaluated by the same scale for DLB; Significant p values (p < 0.05) are in boldface type.
The DLB group had higher scores than AD patients and HC for hallucinations (AD p < 0.001; HC p = 0.006), fluctuations (AD p = 0.082; HC p < 0.001) and RBD (AD p = 0.002; HC p = 0.066). DLB patients presented more akinesia (AD p < 0.001; HC p < 0.001) and rigidity (AD p < 0.001; HC p < 0.001) than the other groups, a lower score indicating the presence of the symptom. Tremor also tended to be higher in DLB patients than in AD patients (p = 0.053) and in HC (p = 0.077).
Caregivers of AD and DLB patients were well matched in terms of age (p = 0.583). For both groups, caregivers were family members, mainly the spouse, except for one DLB patient whose caregiver was his nurse (Table 2).
Demographics of the caregivers.
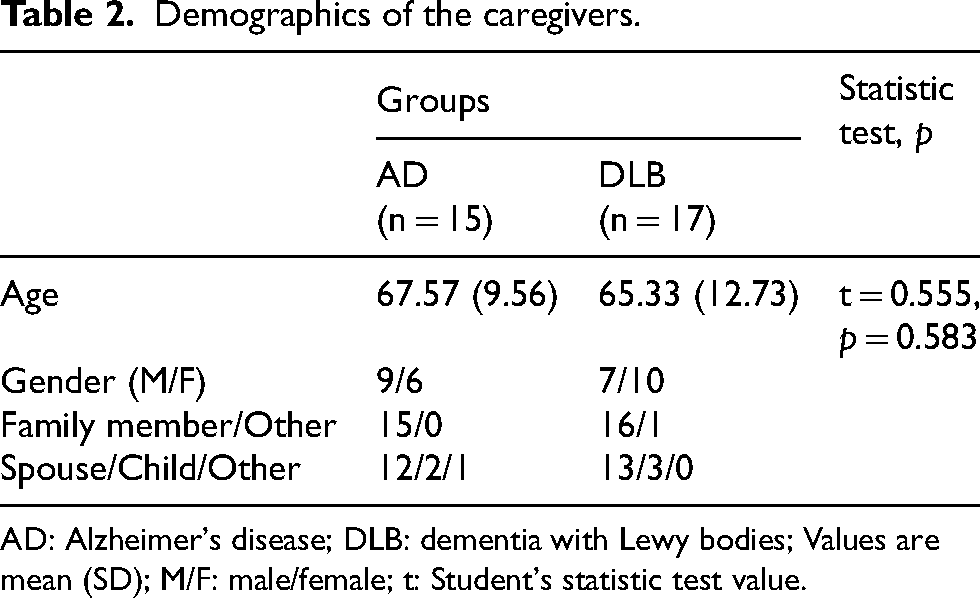
AD: Alzheimer's disease; DLB: dementia with Lewy bodies; Values are mean (SD); M/F: male/female; t: Student's statistic test value.
Language impairments (DTLA)
The DTLA screening scores of patient groups are presented in Table 3. Of the 17 DLB patients, 11 had a pathological score, four were under the alert threshold and only two had normal language performances. Of the 15 AD patients, eight presented normal scores, only three were under the alert threshold and four had a pathological score. The difference in distribution between the two groups appeared significant according to the Monte-Carlo simulation of Fisher's exact test (p = 0.0334).
DTLA screening scores.
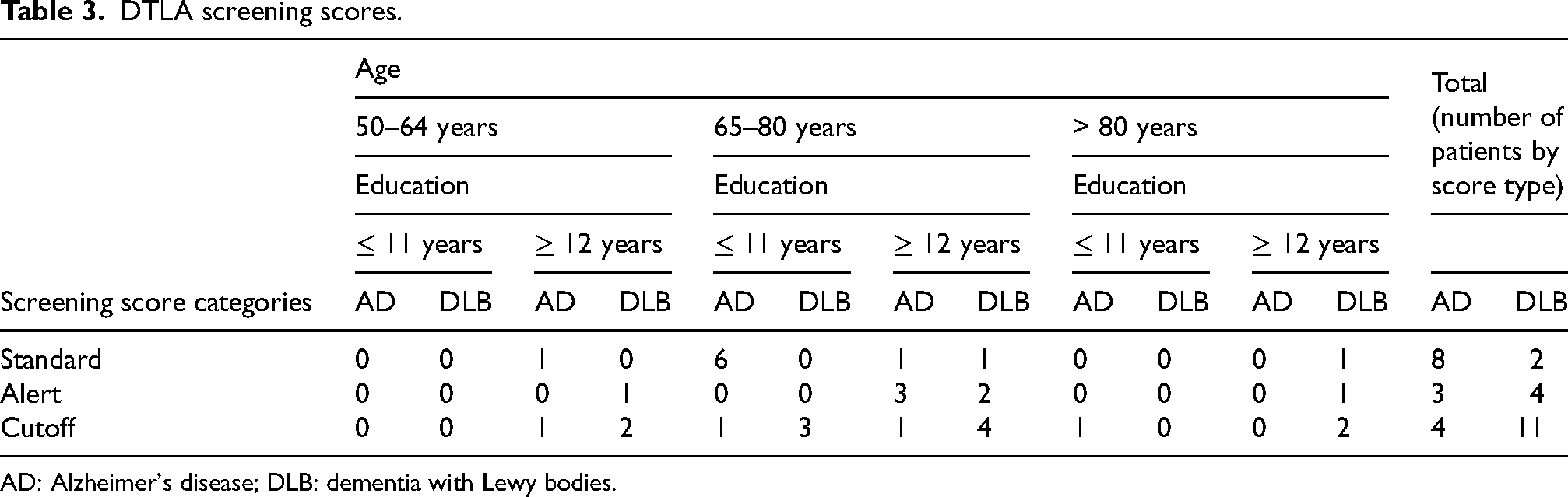
AD: Alzheimer's disease; DLB: dementia with Lewy bodies.
The mean DTLA subscores of DLB patients, AD patients and HC are presented in Table 4. DLB patients had significantly lower language performances (DTLA total scores) than HC (p < 0.001) and AD (p < 0.05). They were significantly more impaired in repetition (p = 0.005), alpha-span (p = 0.035), sentence comprehension (p = 0.019) and dictation (p = 0.001) than HC. Moreover, DLB patients tended to have lower scores in naming (p = 0.063) and phonemic verbal fluency (p = 0.078) than the HC. Their scores in spontaneous writing and articulatory disorder seemed to be lower than those of the HC but there was no significant difference between the two groups (p = 0.160 and p = 0.121, respectively).
Mean DTLA scores of AD, DLB and HC groups.
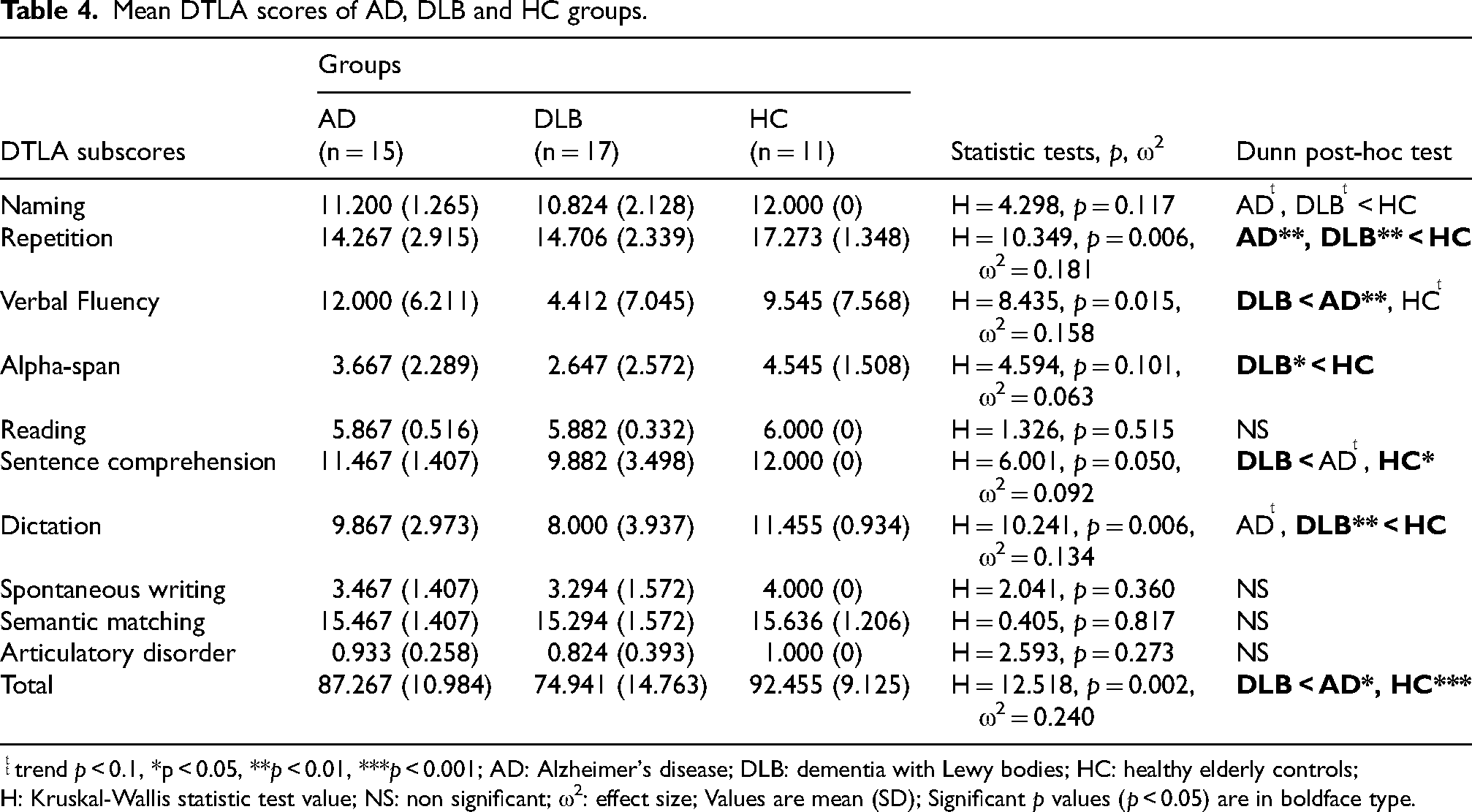
ͭͭ trend p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001; AD: Alzheimer's disease; DLB: dementia with Lewy bodies; HC: healthy elderly controls; H: Kruskal-Wallis statistic test value; NS: non significant; ω2: effect size; Values are mean (SD); Significant p values (p < 0.05) are in boldface type.
On the other hand, phonemic verbal fluency was significantly more impaired in DLB patients than in AD patients (p = 0.004). AD patients also tended to score higher in sentence comprehension than DLB patients (p = 0.099).
Finally, repetition scores (of words, non-words and sentences) were significantly lower in AD patients than in HC (p = 0.003). In addition, AD patients tended to be more impaired on naming (p = 0.066) and dictation (p = 0.084) subtests than HC.
Communication impairments (CoSNAT-D alpha version)
CoSNAT-D data of DLB patients, AD patients and HC are presented in Table 5. DLB patients had greater communication difficulties in all sub-domains compared HC (p < 0.001). They felt significantly more uncomfortable in communication situations (p = 0.027) and reported significantly more difficulties to hold a one-to-one (p < 0.001) or a group (p = 0.002) conversation, to speak fluently (p < 0.001), to understand TV or radio broadcasts (p = 0.007) and to write (p < 0.001) than HC. Compared to HC, DLB patients also tended to experience more reading difficulties (p = 0.085) and to request more help to communicate (p = 0.054).
Mean CoSNAT-D alpha version scores of patients and HC groups.
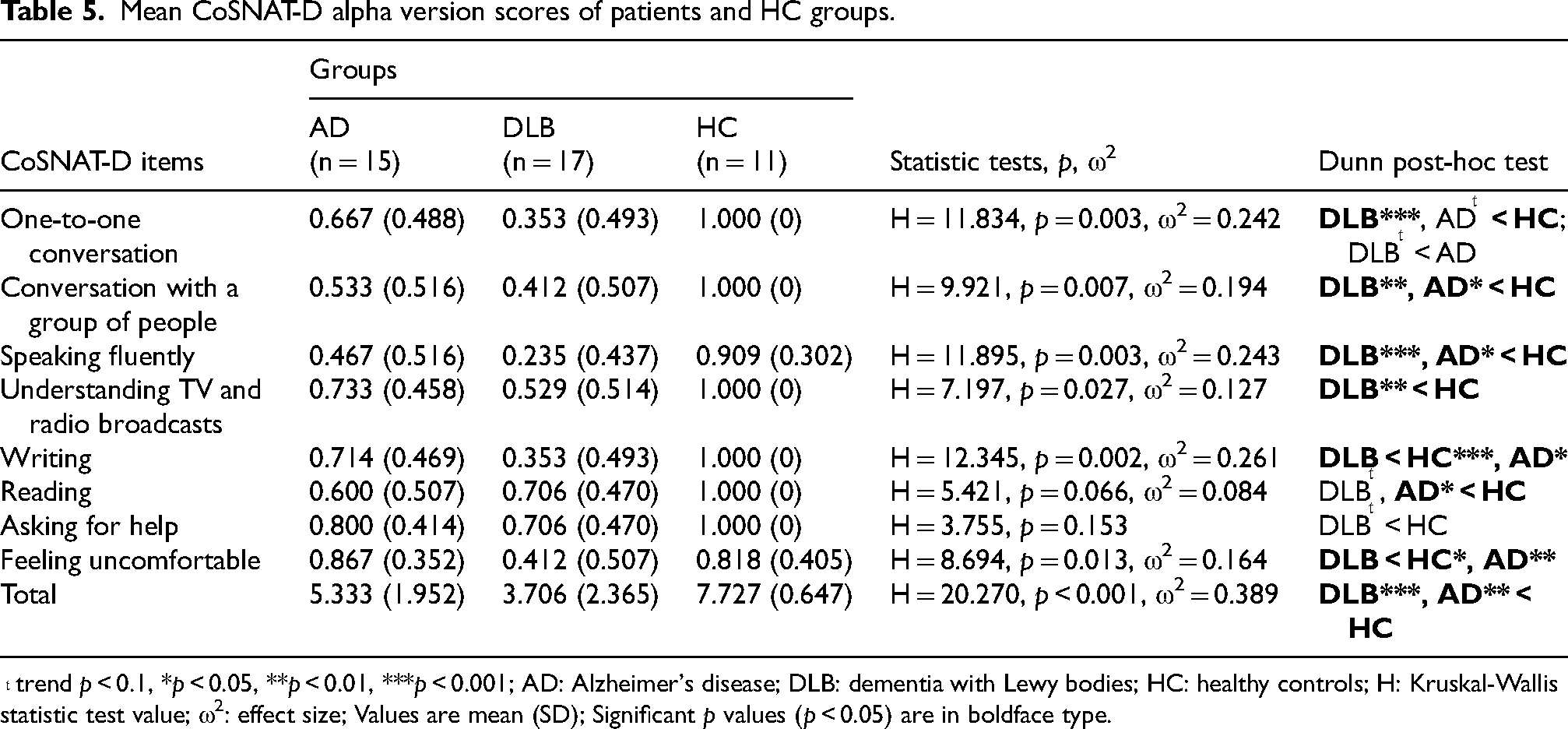
ͭ trend p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001; AD: Alzheimer's disease; DLB: dementia with Lewy bodies; HC: healthy controls; H: Kruskal-Wallis statistic test value; ω2: effect size; Values are mean (SD); Significant p values (p < 0.05) are in boldface type.
DLB patients differed from AD patients in more frequently reporting feelings of discomfort during interactions with others (p = 0.007), and in having writing difficulties (p = 0.039). They also tended to report more one-to-one conversation difficulties than AD patients (p = 0.070).
Moreover, in comparison with HC, AD patients had significantly more communication difficulties (p = 0.003). They experienced significantly more difficulties to hold a group conversation (p = 0.017), to speak fluently (p = 0.028) and to read (p = 0.022). AD patients also tended to have more one-to-one conversation difficulties than HC (p = 0.086).
CoSNAT-D data of patients, caregivers and HP are presented in Table 6. DLB and AD caregivers reported more difficulties than HP in writing (DLB p = 0.004; AD p = 0.012) and asking for help (DLB p = 0.031; AD p = 0.001).
Comparison of mean CoSNAT-D (alpha version) scores between patients, caregivers, HP within the DLB and AD groups.
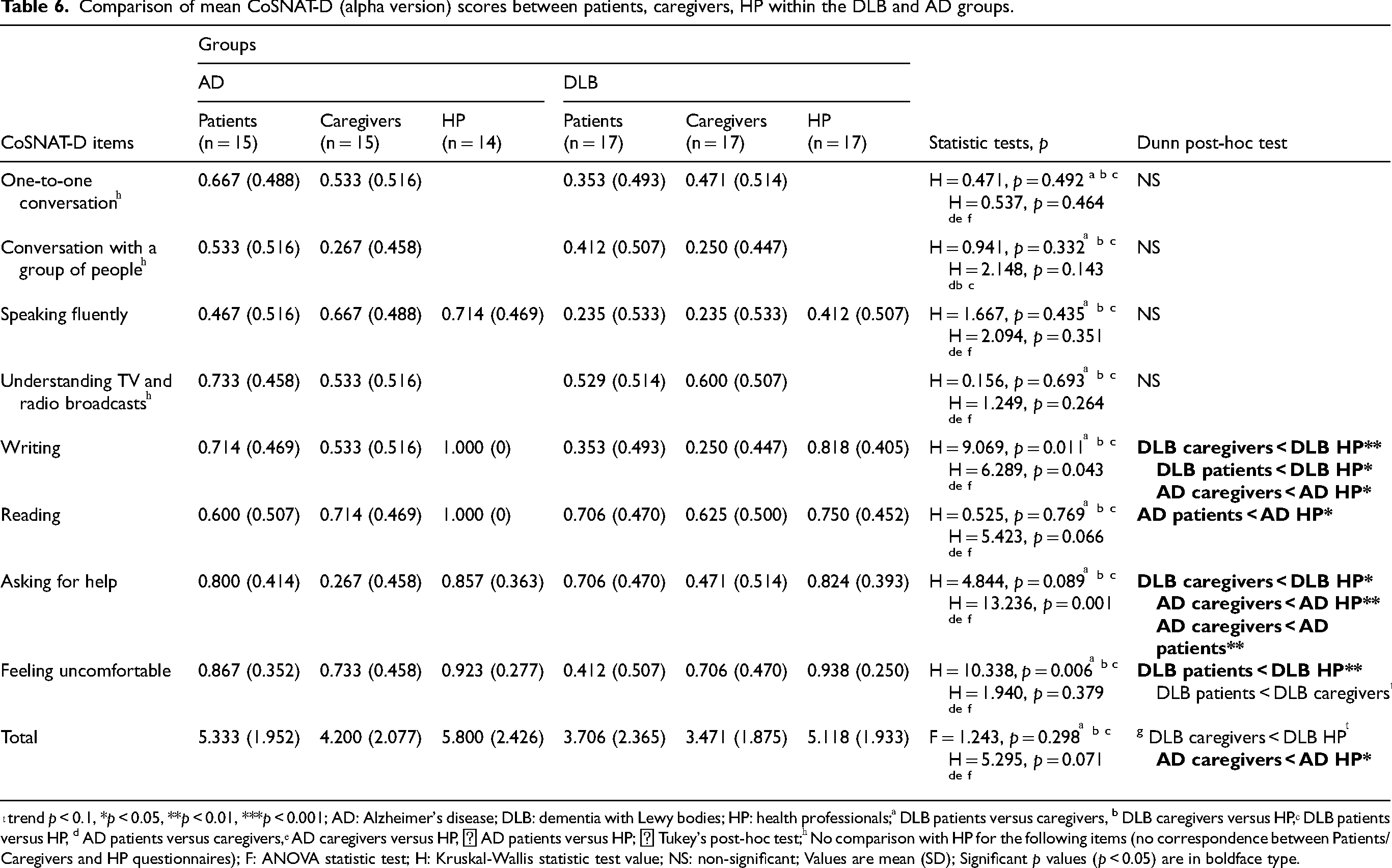
ͭ trend p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001; AD: Alzheimer's disease; DLB: dementia with Lewy bodies; HP: health professionals; ͣ DLB patients versus caregivers, b DLB caregivers versus HP, ͨ DLB patients versus HP, d AD patients versus caregivers, ͤ AD caregivers versus HP, ᶠ AD patients versus HP; ᵍ Tukey's post-hoc test; ͪ No comparison with HP for the following items (no correspondence between Patients/Caregivers and HP questionnaires); F: ANOVA statistic test; H: Kruskal-Wallis statistic test value; NS: non-significant; Values are mean (SD); Significant p values (p < 0.05) are in boldface type.
There was no significant difference between the responses of AD patients and their caregivers. On the other hand, DLB patients more often reported feeling uncomfortable during conversations than their caregivers indicated in their responses (p = 0.069).
Finally, DLB patients reported more difficulties in writing (p = 0.016) and greater discomfort during conversations (p = 0.001) compared to healthcare professionals, whose responses indicated these issues less frequently. The same applies to AD patients, who reported more reading difficulties than HP indicated in their responses (p = 0.022).
Associations between DTLA, CoSNAT-D alpha version, and MMSE tests
Association between DTLA/CoSNAT-D and MMSE scores
There was no significant correlation between the DTLA and MMSE scores in AD patients (Supplemental Table 1). However, the MMSE score of DLB patients correlated to denomination naming (p < 0.001), repetition (p = 0.007) and sentence comprehension (p = 0.013).
In the DLB group, only the speech fluency item from the CoSNAT-D correlated with the MMSE score (p = 0.017), while this latter score correlated only with writing in the AD group (p = 0.006) as presented in Supplemental Table 1.
Association between DTLA and CoSNAT-D scores
There was no significant correlation between any of the DTLA and CoSNAT-D scores in DLB patients (Table 7). However, we found several positively significant correlations between DTLA and CoSNAT-D scores in AD patients. The experience of discomfort during communication correlated with naming (p = 0.012), repetition (p = 0.017), reading (p = 0.005) and articulatory disorder (p = 0.005). Naming was also correlated with fluent speech (p = 0.008), which in turn correlated with dictation (p = 0.042). Finally, we found a significant correlation between semantic matching and one-to-one conversational ability (p = 0.032).
Correlations between DTLA and CoSNAT-D (alpha version) scores.
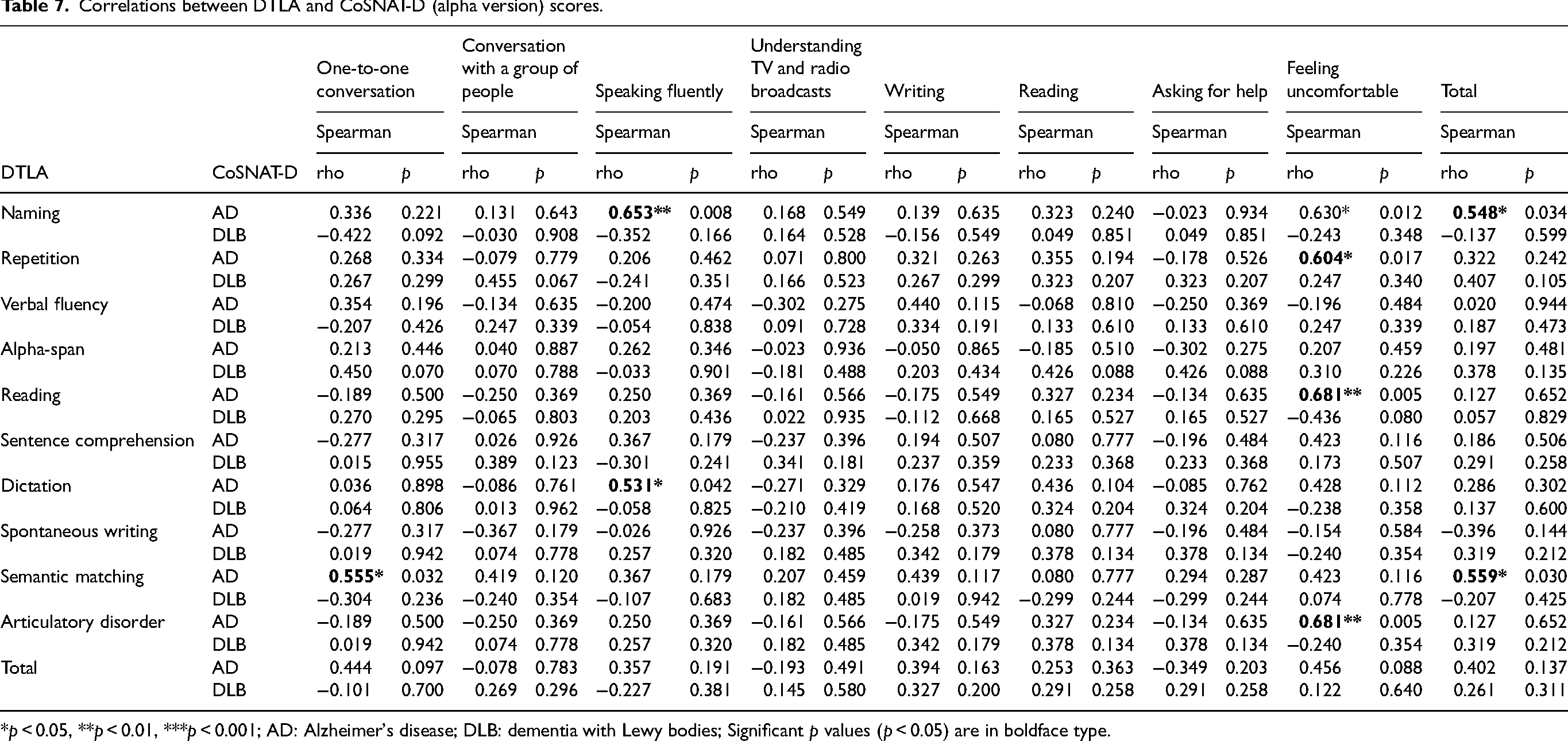
*p < 0.05, **p < 0.01, ***p < 0.001; AD: Alzheimer's disease; DLB: dementia with Lewy bodies; Significant p values (p < 0.05) are in boldface type.
Associations between DTLA, CoSNAT-D alpha version and parkinsonian syndrome
No significant correlations were found between parkinsonian syndrome severity and performance on writing, voice, or articulatory tasks (Supplemental Table 5), which may suggest that the observed impairments are not primarily driven by motor dysfunction, although these results should be interpreted with caution given the limited sample size.
Communication characteristics (SDI)
Between-group comparisons: patients
Patients’ and HC's quantitative SDI data are presented in Table 8. DLB patients showed significantly lower performances than HC on several items: global difficulties (p = 0.007), forgetting the beginning of a sentence or conversation (p < 0.001), gestural difficulties (p = 0.016), writing (p = 0.009), attention and focus (p = 0.004), activity limitation (p = 0.042) and telling a story (p = 0.022). DLB patients also tended to ask for repetition more often than HC (p = 0.053), to express their needs less often (p = 0.080) and to speak with greater difficulty (p = 0.062).
Mean patients’ and HC's responses to the SDI.
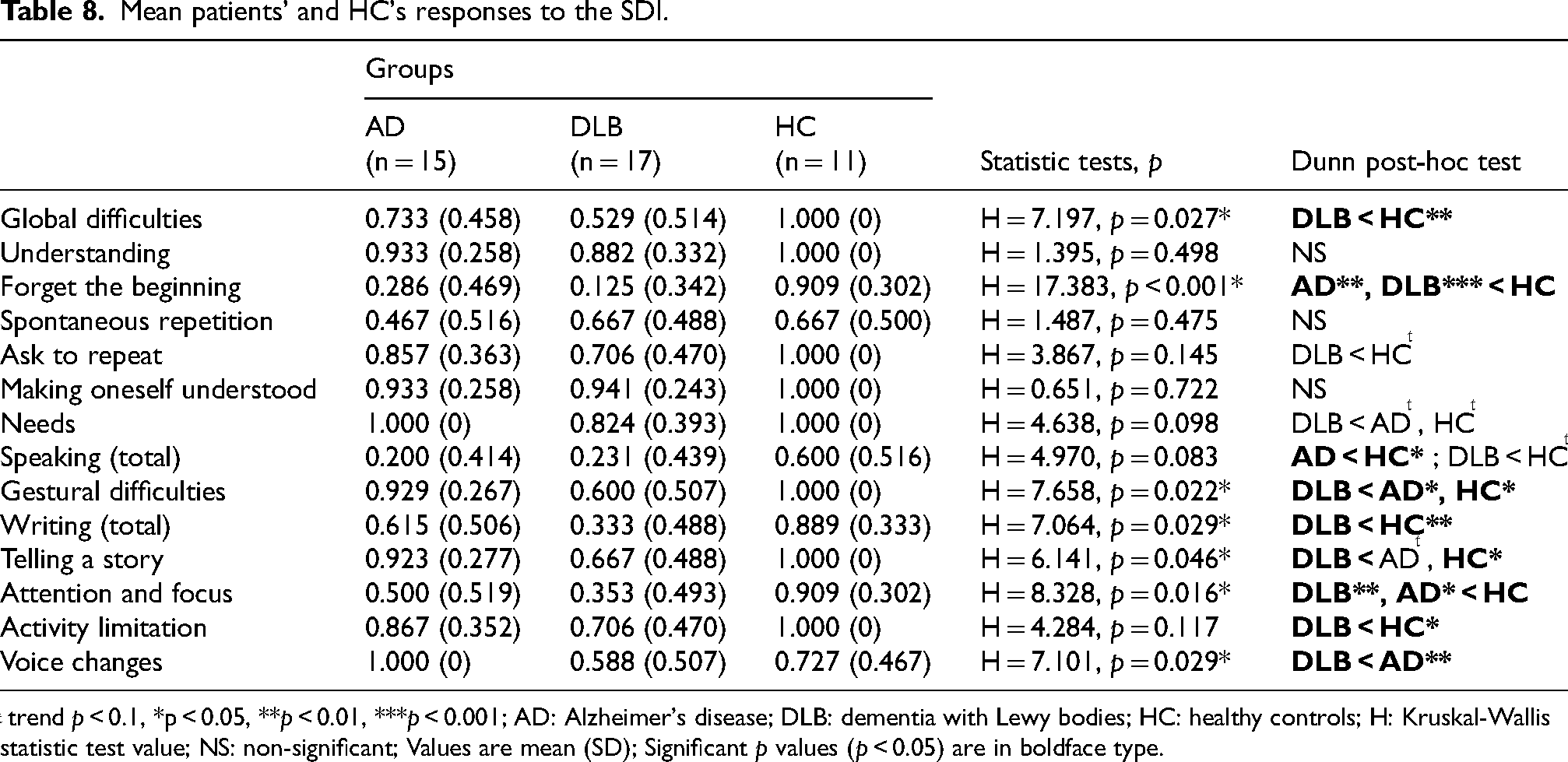
ͭ trend p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001; AD: Alzheimer's disease; DLB: dementia with Lewy bodies; HC: healthy controls; H: Kruskal-Wallis statistic test value; NS: non-significant; Values are mean (SD); Significant p values (p < 0.05) are in boldface type.
AD patients performed better than DLB patients regarding gestural difficulties and voice changes (p = 0.024 and p = 0.008 respectively). They also tended to express their needs better (p = 0.061) and tell a story better (p = 0.064). However, AD patients showed significantly greater difficulty remembering the beginning of a conversation or sentence (p = 0.002), speaking (p = 0.038) and remaining attentive and focused (p = 0.044) than HC.
Finally, no significant difference was found between the three groups for comprehension performance, spontaneous repetition skill and being understood.
Between-group comparisons: caregivers
We only found two main differences between DLB and AD caregivers. Caregivers of AD patients reported significantly more spontaneous repetitions (p = 0.009) and less difficulties in writing (p = 0.007) in the person they cared for than caregivers of DLB patients. They also tended to report fewer attention difficulties in the person they cared for than did DLB caregivers (p = 0.064).
Patient/caregiver discrepancies within groups
In the DLB group, patients’ comprehension difficulties were reported significantly less by themselves than by their caregivers (p = 0.042).
AD patients mentioned significantly fewer difficulties in expressing their needs than what was reported by their caregivers (p = 0.034). However, they tended to report a greater lack of words (p = 0.067) and also less change in voice (p = 0.082) compared to their caregivers’ perception.
No other SDI item differed significantly between patients and their caregivers within either group.
Descriptive statistics of patients’ and caregivers’ SDI responses
An analysis of AD and DLB patients’ responses to qualitative items of the SDI is presented in Supplemental Table 2. First, DLB patients appeared less talkative (DLB: 29.41%; AD: 60%) and less involved in exchanges (DLB: 47.06%; AD: 60%) than that of AD patients. Compared to AD patients, DLB patients were more likely to participate in conversation with only “yes”, “no” or head movements (DLB: 47.06%; AD: 26.67%) and to show an inhibited behavior (DLB: 58.82%; AD: 40%). On the contrary, when communication difficulties appeared, AD patients presented more logorrhea behavior than DLB patients (DLB: 11.76%; AD: 33.33%). Moreover, the way people talk (speed, articulation, pitch, volume) had a greater impact on DLB patients than on AD patients (DLB: 70.59%; AD: 40%). Having less time to express themselves (DLB: 11.76%; AD: 0%) and being cut off (DLB: 35.29%; AD: 20%) were slightly more frequently mentioned by DLB patients than by AD patients. Finally, it was more common for someone else to speak for them in the case of DLB patients than in the case of AD patients (DLB: 52.94%; AD: 33.33%).
No difference was found between AD and DLB patients concerning the impression that others talked about too complicated topics (DLB: 52.94%; AD: 46.67%), concerning gradual fog formation (DLB: 64.71%; AD: 66.67%) and concerning the impact of conversation topics (DLB: 76.47%; AD: 66.67%), people (DLB: 52.94%; AD: 60%), context (DLB: 64.71%; AD: 66.67%) and implicit elements (DLB: 29.41%; AD: 33.33%) on comprehension.
The means of agreement (DLB: 59.38%; AD: 56.25%) and of difference (DLB: 36.72%; AD: 36.25%) between patients’ and their caregivers’ responses were comparable for both diseases (Supplemental Table 3).
Response discrepancies between patients and caregivers (i.e., the number of cases where the patient response was “yes” and the corresponding caregiver response was “no”) is presented in Supplemental Table 3. The most underestimated items by caregivers of DLB patients were the occurrence of a temporary cognitive fog, the impact of the topics discussed on the patient's understanding and the participation in exchanges only through “yes”, “no” or head movements. Balanced participation in conversations and the impact of the way people talk on patient's understanding were also underestimated, but to a lesser extent.
Caregivers of AD patients notably underestimated the patient's balanced participation in exchanges, the occurrence of a temporary cognitive fog and the impact of the interlocutor's adaptation on the patient's understanding. Furthermore, other items were moderately underestimated: the influence of proximity to the interlocutor and the way people talk on comprehension, increasing difficulties with jokes and implicit elements and participation in the conversation only through “yes”, “no” or head movements.
Patients’ language and communication patients’ profiles
Figure 1 summarizes the language and communication results of DLB and AD patients. The scores represent the mean of each individual DTLA and CoSNAT-D alpha version item. The language profile visually highlights the greater deficit of verbal phonemic fluency in DLB patients compared to AD patients. This figure also illustrates a more impaired communication profile in DLB than in AD patients.
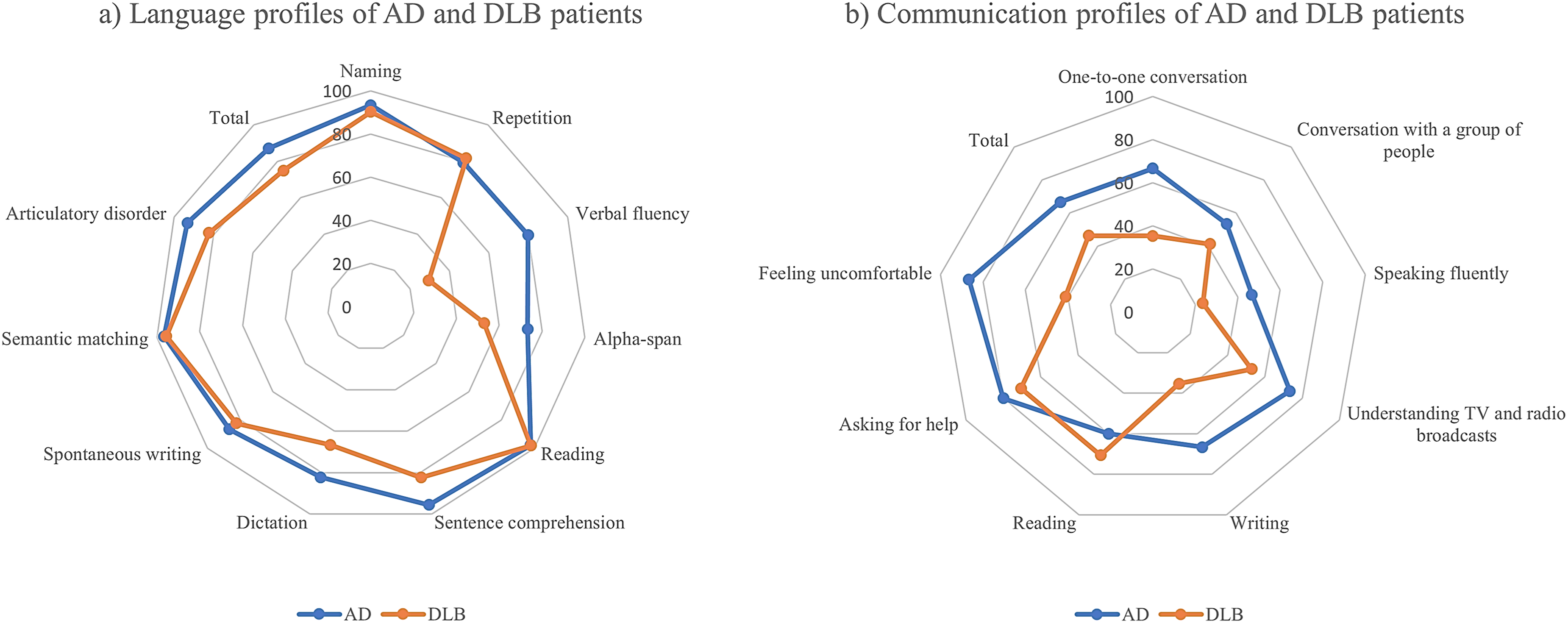
Alzheimer's disease (AD) and dementia with Lewy bodies (DLB) patients’ language and communication profiles.
Discussion
The main goal of the present study was to conduct a preliminary exploration of the overall language and communication profile of early-to-moderate DLB patients (MMSE ≥ 10) compared to that of AD patients and HC. Our study also aimed to characterize the initial complaint and subjective perception of communication difficulties in patients, their caregivers and the HP. Our last goal was to expand this preliminary assessment with more detailed qualitative data and to correlate these communication findings with a rapid assessment of the different domains of oral and written language, in both expression and comprehension. To our knowledge, this is the first study to evaluate language and communication needs in DLB patients also taking into account their caregivers’ and clinicians’ point of view.
In accordance with our initial hypotheses, both DLB and AD patients exhibited language impairments compared to HC, and both patient groups reported subjective difficulties with daily communication. Moreover, the communication and language profiles were more impaired in DLB than in AD patients, particularly in the domains of phonemic fluency, writing and working memory. Finally, perceptions of communicative difficulties and their functional impact varied across patients, caregivers and HP.
Language impairments (DTLA)
DLB patients exhibited significantly greater language and communication impairments than HC. Their DTLA language profile was characterized by a significant impairment of repetition. No previous study to date appears to have focused on this aspect as a DLB symptom. Only a few studies have reported repetition impairment in the presence of PPA.53–55 However, PPA as a presenting syndrome of DLB is rare and therefore unlikely to explain our results. The impairment of working memory described in the literature4,56,57 and found in our study (alpha-span) could contribute to the deficit in repetition, particularly of sentences. Phonemic fluency scores also tended to be lower in DLB patients, as reported in the literature.4,58,59 Executive disorders would explain the deficit in phonemic verbal fluency 4 and partly the deficit in repetition due to attentional difficulties. Moreover, the poorer performance observed in dictation tasks has, to our knowledge, been reported by only one study, where DLB patients were shown to be generally slow, with difficulties in dictating non-words and long sentences partially linked to a parkinsonian syndrome. 32 Deficit results in comprehension in DLB patients compared to HC are consistent with the literature 59 and relatively better documented than dictation. The reduced performance in comprehension of complex sentences can be explained by impairment of executive functions 22 and working memory. 26 Finally, DLB patients also tended to have impaired naming performance. This impairment has been described in the literature4,8 and has been reported as early as the prodromal stage. 14
Difficulties with repetition and sentence comprehension, in particular, may also result from a combination of all these impairments—motor, executive, attentional, and visuospatial 60 - which also makes it difficult to determine whether language disorders are primary or secondary in nature. Indeed, in terms of underlying mechanisms, it is hypothesized that language disorders are mostly secondary in nature, that is, resulting from the cognitive impairments characteristic of the disease, such as executive and attentional deficits. 9 A study conducted on a small cohort of British DLB patients 61 thus showed that only 5% of participants presented with isolated language disorders as an initial symptom of the disease, whereas in 49% of them, the disease had emerged as a combination of language, memory, and visuoperceptual disorders. However, two recent articles have described cases of DLB patients characterized by an initial primary progressive logopenic aphasia.53,62 These findings support the hypothesis put forward by some authors63,64 that language deficits in DLB are not necessarily secondary to cognitive decline. Further investigation, particularly using neuroimaging, is needed to better understand the origin of these deficits.
The observed distribution of the DTLA's diagnostic categories (standard, alert, cutoff) was significantly different between our AD and DLB groups. This supports the hypothesis that AD and DLB patients show distinct language profiles. It also demonstrates the sensitivity and value of the DTLA in detecting language disorders in DLB patients. Moreover, DLB patients showed significantly more impaired performance in phonemic fluency compared to AD patients. This difference was expected in the light of the existing literature16,17,65,66 and would reflect the executive aspect of this task. 66 Furthermore, DTLA sentence comprehension tended to be more impaired in DLB patients than in AD patients. Oral comprehension, particularly sentence comprehension, has been little studied in DLB. Comparisons with AD are therefore rather unspecific and rare. The few articles that tested this skill in a non-specific way in AD and DLB found no significant differences.28–30,59,67
Finally, AD patients’ repetition performance was significantly lower than that of HC. This impairment is consistent with the literature, which notably mentions sentence repetition difficulties68–71 in connection with impaired verbal short-term memory 70 and the potential presence of AD-associated PPA (logopenic variant). 71 AD patients also tended to present greater difficulties in naming and dictation compared with HC. Impaired naming is well documented in the literature.68,72–74 It would be one of the main language characteristics of AD, 68 and would be reflected in mostly lexical–semantic errors. 72 Finally, dictation difficulties in AD patients have also been described.75–78 A regularity effect is seen, 76 with mostly phonologically plausible errors 77 involving irregular words.75,78 Dictation impairments appear to worsen as the disease progresses, 75 and are primarily attributed to lexical–semantic deficits.75,77
Communication impairments (CoSNAT-D alpha version and SDI)
The communication profile of DLB patients was characterized by impairment in all the domains assessed in the present study compared with HC. While DLB patients tended to report greater reading difficulties and more frequent requests for help in communicating, all other fields of communication tested by the alpha version of the CoSNAT-D showed significantly lower results. This is consistent with the SDI results and with data from the literature that mention overall communication difficulties of DLB patients.36,79 Television and radio broadcasts were particularly difficult for them to understand. Compared to HC, they also had more problems with conversational comprehension, as expected, 34 and more often felt uncomfortable in such situations. Indeed, DLB patients were specifically impaired in group conversations, but they were even more impaired in one-to-one interactions. If group conversations appeared to be more demanding in terms of attentional resources, the greater difficulties in dual conversations could be linked to the often more inhibited nature of DLB patients reported by the SDI. Group conversations could enable them to remain in the background. These conversational difficulties may also be explained by findings from the SDI, which highlight increased forgetting of the beginning of a sentence or conversation in DLB patients Clearly, the existence of memory problems make it more difficult to hold a one-to-one conversation. Fluency of speech is also frequently impaired in DLB,33,34 which corroborates the significantly more frequent reports of difficulties in speaking fluently. The tendency for DLB patients to report more word-finding difficulties during SDI may be considered as a serious clue to explain this fluency impairment. The narrative organization deficits correlated with the executive and speech fluency deficits described in the literature22,80 may help to explain the difficulties experienced by patients in telling a story or explaining something. Moreover, writing appeared to be one of the main areas of impairment in these patients. As the responses to our SDI concerning writing gesture were also impaired, this would partly explain the lower performance in writing.32,81 Indeed, for some patients with a parkinsonian syndrome as a proven cardinal criterion, the writing deficit would be partially linked to their difficulty in making tracings. Another hypothesis to explain the handwriting disorders would be the impaired word-finding performance reported by the SDI. In addition, DLB patients also had their conversation partners repeat more than HC. Poor comprehension, attention and concentration deficits, hearing problems and the fluctuations inherent to the pathology are all possible causes of this phenomenon. Finally, this impaired language and communication profile results in activity limitation, as reported by DLB patients.
DLB patients differed from AD patients in having greater difficulty writing, as well as higher voice changes and feelings of discomfort during exchanges.
The greater voice changes and writing difficulties of DLB patients compared to AD patients are consistent with the literature.81,82 This result does not seem surprising, since both handwriting and voice of DLB patients would be partly affected by the parkinsonian syndrome,32,81 similarly to what is observed in Parkinson's disease (PD). To our knowledge, no study has directly compared handwriting and voice between patients with DLB and PD. As synucleinopathies, these conditions share core clinical and pathological features, including parkinsonism, reflecting a common underlying α-synuclein pathology. 83 Consequently, motor-related impairments affecting voice and handwriting may partially overlap between the two disorders. Yet divergence is expected given differences in Lewy body distribution: while DLB is characterized by early cortical and limbic involvement, 81 PD follows a brainstem-predominant pattern, with cortical spread occurring only at later stage. 84
This divergence is particularly apparent in writing. In PD, writing disorders are mainly characterized by micrographia and primarily reflect motor dysfunction, 85 whereas in DLB, writing impairments appear to arise from an interaction between motor deficits, occasionally associated with parkinsonian features, and cognitive impairment, with a notable impact of working memory, attention and executive functions.9,60 Handwriting in DLB may also be compromised in its spatial organization and letter form due to visuoperceptual and visuospatial deficits.3,28,86 Finally, praxis impairments 4 may also contribute to writing difficulties observed in DLB by disrupting the integration of visuospatial processing and motor planning required for coherent graphomotor output.
With regard to voice, both PD and DLB patients appear to exhibit reduced prosodic modulation (monotony)82,87,88 as well as increased frequency instability (jitter) and amplitude instability (shimmer).82,87,89 However, no study mentions hypophonia in DLB, even though it is the characteristic symptom of voice changes in PD.90,91
Furthermore, the increased feeling of discomfort in exchanges in DLB patients compared to AD patients could be explained by a greater awareness of their own language difficulties. However, the few articles that have compared awareness/anosognosia of cognitive disorders between DLB and AD lead to heterogeneous and inconsistent conclusions. 92 This difference could also be linked to a greater deficit in emotion identification in AD. To our knowledge, no direct comparison of emotion identification between AD and DLB patients has been conducted. However, the perception of emotions, particularly negative ones, would be impaired in AD 93 whereas it would be preserved in DLB. 4 The results are nevertheless sometimes inconsistent for AD and no real consensus for the emotional processes in this disease exists.94,95 A divergence in theory of mind between AD and DLB could lead to this more frequent feeling of discomfort in DLB. The absence of any significant difference in theory of mind between AD and DLB patients reported in the literature 96 does not support this hypothesis. DLB patients show difficulties in theory of mind from the early stages of the disease in cognitive rather than affective theory of mind.4,96,97 In AD, the impairment appears to be less specific and may affect certain complex components of both cognitive and affective theory of mind, 95 notably the recognition of false beliefs and the other's intentions.95,97 Finally, the frequency of some neuropsychiatric symptoms in DLB, such as apathy, depression and visual hallucinations, 98 could also explain this greater feeling of discomfort.
Compared with AD patients, DLB patients’ participation in exchanges was slightly less balanced and could be the result of a more frequent use of head movements and the short words “yes” and “no”. In addition, the way in which people talk had less impact on AD patients than on DLB patients. At the onset of communication difficulties, AD patients would be more logorrheic than DLB patients, while DLB patients would be more likely to have an inhibited behavior. Finally, interlocutors gave DLB patients less time to express themselves and cut them off more often than AD patients. This difference may be linked to the greater language and communication difficulties in our sample of DLB patients, leading to a change in interactional dynamics.99–101 It is therefore not surprising to find that DLB caregivers spoke more frequently instead of the person they care for than was the case with AD caregivers.
AD patients showed communicative impairments and complaints from the earliest stages of the disease, sometimes in absence of any objectified language disorders. First, they had significantly more reading disorders than HC. This impairment is described in the literature 102 and would be greater for irregular words. Compared with HC, AD patients also reported significantly more difficulty in group conversation and tended to have more difficulty in one-to-one conversation. The literature seems to agree with our findings: AD patients would have impaired communication from the earliest stages of the disease. 39 Communication difficulties may be explained by more frequent attention and concentration problems, as well as more frequent forgetting of the beginning of a conversation or sentence. The latter could be linked to the impaired short-term memory often described in AD103–105 or to an attentional disorder, also well-described.106,107 Furthermore, AD patients reported significantly more difficulties with speech fluency and word finding compared to HC. Lexical access deficits are also consistent with the literature68,108,109 and could explain conversation difficulties.
Association between DTLA and CoSNAT-D in DLB and AD
While expected correlations are seen between language and communication in AD patients, it is surprising that no significant correlation was found between the DTLA and the CoSNAT-D alpha-version in DLB patients. To some extent, this apparent discrepancy could be explained by the greater day-to-day stability of performance in AD. However, AD patients may experience episodes of contextual emergent confusion, linked to cognitive demand and memory disorders. Caregivers also sometimes describe “good” and “bad” days, but these are occasional. 110 Furthermore, the lack of correlation in DLB could be related to different symptoms of the disease. Among the explanatory hypotheses for the various disorders identified, we cited executive disorders. 4 These difficulties would play a key role in the selection and organization of ideas, notably due to the striatal damage. 24 It also appears that daily communication situations are more complex and less structured than theoretical language tests. 111 This may partly explain the deficits in performance. Attention and concentration were two aspects of SDI significantly impaired in DLB patients. This underperformance, highlighted in the literature, 112 could be a cause of major difficulties, particularly in comprehension and conversation. They also may themselves be the consequence of the fluctuations present in DLB. Indeed, these fluctuations can affect attention, but also vigilance and overall cognitive performance, which can have an irregular impact on language test results. Therefore, this also may reduce the possibility of observing a consistent association between language scores derived from a formal assessment situation, and communication difficulties in daily life.111,113,114 Finally, depression is another factor likely to dissociate performance on framed language tests, involving targeted tasks from performance in daily communication, in an ecological context. Indeed, depression is frequently associated with DLB.98,115 This strong emotional and social component is likely to have a greater impact on communication and interactions with others than formal language tests. Likewise, formal language tests could generate more stress and anxiety in patients than a communicative test enabled by a more ecological interaction. This may explain why there was no correlation between the DTLA and CoSNAT-D results. Therefore, it is as possible to have a normal score for language and a deficient score for communication as the reverse.
Discrepancies between self-rated and proxy-rated CoSNAT-D and SDI responses
Regarding perceived difficulties, DLB patients reported significantly fewer comprehension difficulties than their caregivers, but a greater feeling of discomfort during exchanges. Caregivers of AD patients reported significantly more vocal changes and difficulties in expressing needs than their relative. However, AD patients tended to report a lack of words more frequently than their caregivers, suggesting a rather preserved awareness of this disorder. This trend may also be explained by a heavy reliance on appearance-saving responses that can partly hide this disorder. 35 Qualitatively, only the gradual onset of mental fog was underestimated by caregivers of both AD and DLB patients. All these discrepancies may be linked to a slight denial, the caregiver's burden116,117 or a lack of awareness of language disorders among caregivers. To our knowledge, the perception of communication difficulties by caregivers has not been directly studied. However, family members often have difficulty recognizing initial cognitive symptoms until multiple domains are affected, 118 suggesting that caregivers may initially underestimate these impairments. Overestimation of difficulties by the patient is also possible, and could be heightened by the presence of neuropsychiatric symptoms (depression / tendency to focus on their decline / paranoia).115,119 Indeed, patients with higher levels of depressive and anxiety symptoms tended to diverge more from their caregivers, 120 and depression is a commonly reported feature (20 to 35%) in both DLB 121 and AD. 122 The few items underestimated by patients may be associated with anosognosia in AD, 123 and potentially in DLB as well. 92 Finally, Jin and Cheon 120 showed that discrepancies between patients and caregivers increase with both the severity and duration of the disease in PD. Reflecting our results, the direction of these discrepancies is not uniform and varies according to the patient's mood and the caregiver's burden. 120
Furthermore, the means of agreement of responses between patients and caregivers were the same in both diseases. This similarity suggests that the perception of communication difficulties by caregivers and patients does not differ between AD and DLB. This may also suggest that awareness of language and communication disorders does not differ between AD and DLB patients. This hypothesis needs to be qualified, however, by the possibility of anosognosia on the part of the patient and denial on the part of the caregiver, leading to similar responses. On the other hand, this similar percentage of discordance between patient and caregiver responses was high, and could therefore contribute to increasing the caregivers’ burden. 124
DLB patients reported greater writing difficulties and feelings of discomfort during exchanges than their HP. Likewise, the HP of AD patients reported significantly fewer reading difficulties than the patients themselves.
To some extent, the frequent underestimation by HP was linked to a high number of non-responses due to the absence of assessment of the targeted language skills, particularly writing and reading. In addition, this difference may have been due to the frequency of interviews between patients and HP. Non-protocol patients were often seen once a year at the day hospital, which did not give the HP an accurate picture of the patient's communication and language difficulties. Clinical reasoning frequently relies on intuitive, experience-based heuristics and pattern recognition.125,126 While these strategies allow rapid identification of prototypical or severe cases, they can lead to under-recognition of subtle or atypical impairments. This cognitive mechanism may thus contribute to the underestimation of milder communication disorders, particularly when symptoms do not match the most characteristic features of the disorder, as observed for reading difficulties in AD in the current study. A lack of awareness among HP about communication disorders and their early detection could also explain these differences. The literature highlights limited awareness and insufficient training and attention among healthcare professionals regarding communication disorders.127–129 Evidence suggests that these limitations may originate during early professional training and are already observable among students. 130 As a result, communication disorders may be under-recognized in clinical practice, potentially leading to reduced quality of care, particularly in the management of language impairments. Moreover, the questions relating to feelings of discomfort and requests for help referred to all interactions in the questionnaires of patients and caregivers, whereas they referred only to interaction with the HP in their questionnaire. This restriction of context may therefore explain the underestimation of these items by HP.
Finally, an improvement in performance during the consultation with the HP is often seen because of the assessment's stakes. This may be explained by increased motivation and attentional engagement in evaluative contexts, consistent with the Hawthorne effect, whereby individuals modify their behavior when they are aware of being observed or assessed. 131 Consequently, assessments may reflect optimal rather than everyday performance.
Limitations
The results of this exploratory study should be interpreted with caution, due to the limited number of participants in our cohort. It would be advisable to reproduce this preliminary protocol with a larger number of patients in future studies. In addition to the limited sample size, several inferential limitations should be considered. In particular, the reliance on self-report measures warrants cautious interpretation, as individuals may have limited introspective access to their own cognitive and emotional processes, potentially leading to inaccurate or incomplete reporting. 132 Moreover, such instruments are susceptible to multiple sources of systematic bias, including social desirability, recall-related distortions, and common method variance, which can distort results and affect the validity of inferences.133,134 The place of recruitment is also a major bias. This term encompasses not only the location of the day hospital, Strasbourg, but also the various departments within the hospital. Indeed, we recruited patients from both the day hospital and the specific research unit. Patients from the research protocols met specific criteria, which may explain better results on language and communication tests. The same patients often participate in different protocols. They are therefore closely monitored by the memory center's specialists and become experts in their pathology. For example, they are better able to cope with the stress of cognitive examinations and to present more palliative strategies to overcome their difficulties. These factors could explain the better performance of participants from the specific research unit in which AD subjects are in the majority. This should be considered in future studies to try to ensure better homogenization of profiles. Patients were recruited from a single tertiary memory clinic, which may introduce selection and referral biases, potentially limiting the generalizability of the findings to broader DLB and AD populations.135–137 Additionally, pharmacological treatments were not controlled across participants and may have exerted some influence on language performance. However, for the majority of the clinical protocols included in this study, no published evidence exists regarding a direct effect of the administered treatments on language outcomes, and language was not a specifically evaluated endpoint in the remaining trials. Fluctuations in DLB patients also represent a potential bias. As they are still poorly defined and identified, we do not know how much impact fluctuations may have had on patients’ results. Their influence on performance can be seen as a bias, but also as the cause of heterogeneous or even surprising results. A better understanding of this phenomenon in DLB is currently a real challenge. Another limitation lies in the absence of cognitive data collected from caregivers, which could have provided valuable complementary insights into their responses and communicative interactions with patients. Finally, the patients’ categorization was not based on confirmed postmortem analyses, but diagnoses were carried out by expert neurologist/geriatrician clinicians, and complemented by a longitudinal follow-up.
Conclusion
The present study is the first to provide initial insights into the overall language and communication profile of DLB patients in comparison with healthy elderly subjects and AD patients. Indeed, language performance in DLB has been little studied, particularly in relation to writing abilities, including reading and repetition.
In line with our first hypothesis, DLB patients’ language performances were impaired. DLB patients’ language profile was mostly characterized by impairments in repetition, verbal working memory, sentence comprehension and dictation. Performance in naming and phonemic fluency of DLB patients also tended to be lower than HC. In accordance with our second hypothesis, DLB patients exhibited greater deficits in phonemic fluency and a tendency towards poorer sentence comprehension compared to AD patients. Regarding communication, DLB patients reported more difficulties with writing than AD patients, as well less frequent feeling of discomfort and fewer voice changes during exchanges. As we supposed, patients’ perception of their communication difficulties sometimes differed from the perception of these difficulties reported by caregivers and health professionals. Indeed, DLB patients reported a greater sense of discomfort in exchanges and fewer difficulties in understanding than their caregivers. On the other hand, AD patients reported greater word finding difficulties, but fewer vocal changes and fewer difficulties in expressing their needs than their caregivers. Consideration of these different perceptions allows for a better understanding of the communication profile of the patients and its impact on daily life. This preliminary study provides specifically valuable initial clinical information on the DLB profile, as it may be observed on a daily basis by HP other than speech therapists.
Future directions to further explore the language and communication profile of DLB patients include proposing longer language items and using more specialized speech-therapy tests, and conducting qualitative analyses on communication, currently neglected and yet at the heart of our human interactions. Replicating this study on a larger scale would also enable us to characterize the profile of these patients in greater detail and offer solid validation of our results. Finally, it might be useful to consider the caregiver's feelings, and not only their perception of their partners’ difficulties. Although some emerging studies have explored communication within the patient–caregiver dyad in dementia, no research has yet examined this aspect in the context of DLB. Therefore, this area deserves further attention in future studies, in order to better understand and define the implications of language and communication disorders on everyday family dynamics in DLB.
Supplemental Material
sj-pdf-1-alz-10.1177_13872877261458679 - Supplemental material for Language and communication disorders in dementia with Lewy bodies versus Alzheimer's disease: Objective screening and subjective perspectives of patients, their caregivers and clinicians
Supplemental material, sj-pdf-1-alz-10.1177_13872877261458679 for Language and communication disorders in dementia with Lewy bodies versus Alzheimer's disease: Objective screening and subjective perspectives of patients, their caregivers and clinicians by Marie Balohé, Julie Thivet, Frédéric Blanc, Luisa Krein, Yun-Hee Jeon, Anne Botzung, Léa Sanna, Alix Ravier, Catherine Demuynck, Candice Muller and Éléna Chabran in Journal of Alzheimer's Disease
Supplemental Material
sj-docx-2-alz-10.1177_13872877261458679 - Supplemental material for Language and communication disorders in dementia with Lewy bodies versus Alzheimer's disease: Objective screening and subjective perspectives of patients, their caregivers and clinicians
Supplemental material, sj-docx-2-alz-10.1177_13872877261458679 for Language and communication disorders in dementia with Lewy bodies versus Alzheimer's disease: Objective screening and subjective perspectives of patients, their caregivers and clinicians by Marie Balohé, Julie Thivet, Frédéric Blanc, Luisa Krein, Yun-Hee Jeon, Anne Botzung, Léa Sanna, Alix Ravier, Catherine Demuynck, Candice Muller and Éléna Chabran in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We are grateful to the patients, their relatives and the control subjects who took part in the study. The authors thank the neuropsychologists of the Memory Centre of Strasbourg (CM2R), Timothée Albasser, Guillaume Jung, Jeanne Mérignac, the Research Clinical Assistants, Fanny Huselstein, Fabienne Saab and the secretary, Gabrielle Huck, for the essential collection of the clinical data. They also thank Nick Barton for language editing.
Ethical considerations
This research was approved by the local ethics committee (“Comité d’éthique pour la recherche Unistra”, Unistra/CER/2024-12).
Consent to participate
All participants provided written informed consent to participate.
Consent for publication
Written informed consent was obtained from the participants for publication of their individual details in this manuscript. The consent form is held by the authors’ institution and is available for review by the Editor-in-Chief. We have also obtained the consent of DTLA and CoSNAT-D authors to use their tests.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on reasonable request to the corresponding authors and subject to a data sharing agreement.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.