
Abstract
Background
Alzheimer's disease (AD) is commonly treated with memantine alone or in combination with cholinesterase inhibitors (ChEIs) or second-generation antipsychotics (SGAs), but the safety of these combinations remains unclear.
Objective
To characterize FDA Adverse Event Reporting System (FAERS)-based signals of disproportionate reporting associated with memantine-based combination therapies in patients with AD.
Methods
A disproportionality analysis was conducted using data from FAERS from 2014Q1 to 2025Q2 via the MY FAERS platform. Reporting odds ratios (RORs) with 95% confidence intervals (CI) were calculated to identify safety signals. Sensitivity analyses were conducted using ChEIs or SGAs monotherapy as reference groups to assess the robustness.
Results
2531 patients prescribed memantine were identified, comprising memantine monotherapy (n = 1965), memantine-ChEIs combination (n = 482), and memantine-SGAs combination (n = 84). Compared to memantine monotherapy, the memantine- ChEIs combination showed disproportionate reporting signals for skin (ROR, 3.46; 95% CI, 2.05–5.85), gastrointestinal (ROR, 2.53; 95% CI, 1.92–3.33), musculoskeletal (ROR, 2.13; 95% CI, 1.29–3.50), psychiatric (ROR, 1.60; 95% CI, 1.27–2.00), general (ROR, 1.53; 95% CI, 1.18–1.97), and nervous system disorders (ROR, 1.48; 95% CI, 1.19–1.84). The memantine-SGAs combination was strongly associated with the signals of general (ROR, 3.97; 95% CI, 1.74–9.05), psychiatric (ROR, 2.14; 95% CI, 1.32–3.49), nervous system disorders (ROR, 2.03; 95% CI, 1.20–3.43), and hip fracture (ROR, 15.84; 95% CI, 3.72–67.41). Sensitivity analyses confirmed robustness across subgroups.
Conclusions
Memantine-based combination therapies were associated with distinct safety signals of disproportionate reporting compared with monotherapies. These findings should be interpreted as pharmacovigilance signals that warrant cautious interpretation and further validation in well-designed observational or prospective studies.
Keywords
Introduction
Alzheimer's disease (AD), the most common form of dementia, is a progressive neurodegenerative disorder characterized by cognitive decline, memory impairment, and behavioral changes. 1 As global populations age, AD represents a growing public health challenge, underscoring the urgent need for effective therapeutic interventions. Among the pharmacological options, memantine, an N-methyl-D-aspartate (NMDA) receptor antagonist, was approved by the FDA in 2003 for the treatment of moderate to severe AD and has since become a cornerstone of symptomatic management. 2 It exerts its therapeutic effects by selectively blocking NMDA receptors, thereby modulating glutamatergic excitotoxicity and attenuating calcium influx into neurons, which is believed to slow neuronal degradation and support cognitive function. 3 Memantine is particularly valued for its favorable pharmacokinetic profile, including low protein binding and minimal hepatic metabolism, which reduces the risk of certain drug interactions. 4 Despite its established efficacy in improving cognitive and functional outcomes, the safety profile of memantine, particularly within combination therapies, remains inadequately elucidated, warranting more comprehensive evaluation. 5
In clinical practice, memantine may be co-administered with cholinesterase inhibitors (ChEIs) or with second-generation antipsychotics (SGAs) to enhance therapeutic outcomes, especially for behavioral and psychological symptoms of dementia. The combination of memantine and ChEIs is recommended for patients with moderate-to-severe AD, particularly those exhibiting an inadequate response to monotherapy. 6 The DOMINO trial indicated that this combination therapy confers modest advantages in cognitive and functional outcomes; however, evidence regarding its long-term safety remains limited. 7 For ChEI-related combinations, concomitant use of memantine and donepezil has been associated with emerging safety concerns, including hypertensive crises, significant hyperglycemia, and other serious cardiovascular events. 8 Separately, SGAs may be used for the short-term management (≤ 6 weeks) of severe aggression or psychotic symptoms when non-pharmacological interventions have proven ineffective. 9 However, the addition of SGAs to memantine therapy may aggravate metabolic abnormalities and extrapyramidal symptoms. 10 Thus, although memantine-based combination therapies may provide clinical benefits in selected patients, they may also introduce complex pharmacokinetic and pharmacodynamic interactions that potentiate adverse drug reactions (ADRs). Despite these potential risks, systematic assessments of combination-related ADRs remain limited, reflecting a critical evidence gap regarding the safety of polypharmacy in AD management.
Individual case safety report databases, such as the FDA Adverse Event Reporting System (FAERS), offer a valuable resource for post-marketing pharmacovigilance. These repositories enable the detection of rare, delayed, or subpopulation-specific ADRs that are often undetected in pre-marketing clinical trials due to restricted sample sizes and limited follow-up durations. Disproportionality analysis, a widely employed quantitative method in pharmacovigilance, facilitates the identification of significant associations between drugs and adverse events (AEs) by comparing observed reporting proportions with expected background rates.11–13 This methodology is particularly well-suited for investigating drug-drug interactions and examining risk profiles across patient subgroups.14–16 Thus, in complementing evidence from randomized controlled trials, which may fail to capture long-term or real-world risks, disproportionality analysis provides essential insights into medication safety within diverse clinical contexts.16,17
This study aims to identify and characterize signals of disproportionate reporting (SDRs) of ADRs associated with memantine-based combination therapies. Utilizing the FAERS database, we will identify and characterize safety signals associated with two prevalent combination strategies: memantine with ChEIs and memantine with SGAs. The reference group will comprise patients receiving memantine as a monotherapy. By delineating the SDRs associated with these regimens, our findings seek to contribute to the optimization of safety in the pharmacological management of AD.
Methods
Study design and data mining
A disproportionality analysis was performed based on the READUS-PV framework, 18 using individual case safety data extracted from the FAERS covering the period from 2014Q1 to 2025Q2. The READUS-PV checklist is included as Supplemental Table 1. FAERS, a surveillance database managed by the FDA, represents a critical resource for monitoring drug safety in the post-approval phase. Each entry in FAERS consists of structured information such as patient demographic details, drug indications, AEs, and treatment outcomes, all of which are coded according to the Medical Dictionary for Regulatory Activities (MedDRA), 19 which is a globally recognized terminology system for pharmacovigilance coding.
To support this study, we constructed MY FAERS, a dedicated pharmacovigilance platform that allows tailored query configurations, automated data handling, and dynamic visualization capabilities. 20 The system utilizes MySQL (via MySQL Workbench) for robust database management and bulk data acquisition, while Python's Pandas library facilitates statistical computations, and Matplotlib, Seaborn, and Plotly (under Python 3.6) enable flexible graphical representation of drug safety trends. Primary filtering dimensions comprise: drug and concomitant medication names; patient age, gender, and diagnosis; report date and therapeutic duration ranges; AE terms and outcomes. Dose-related information was not included in the primary disproportionality analysis because dose records in FAERS were frequently incomplete or inconsistently reported across drugs, formulations, and dosing schedules, which precluded reliable dose standardization and dose-stratified ROR estimation.
Data retrieval involved relational queries across multiple FAERS tables, including DRUG, DEMO, OUTCOME, INDICA, THER, REAC, and RPSR. Before formal analysis, raw FAERS data were purged using the deduplication module embedded in the MY FAERS platform to reduce potential overestimation caused by duplicate or follow-up reports. After all quarterly FAERS files were imported and integrated, duplicate and follow-up records were identified using FAERS case identifiers. For reports sharing the same CASEID, only the most recent version was retained according to the latest FDA_DT. If multiple records had the same CASEID and FDA_DT, the record with the highest PRIMARYID was retained. The deduplicated PRIMARYIDs were then used to link the DEMO, DRUG, REAC, OUTCOME, INDICA, THER, and RPSR tables. In the disproportionality analyses, counts were calculated based on unique deduplicated reports rather than raw table rows, thereby minimizing inflation of signal estimates due to duplicate reporting.
The platform produces interactive visual outputs such as: (1) demographic histograms for baseline summaries; (2) top probability distribution of preferred terms (PTs) for evaluating AE profiles; (3) time-to-onset analyses presented through cumulative probability curves and violin plots; and (4) disproportionality signals visualized via ROR forest plots and comparative heatmaps. An infographic-style overview of the study design and analytical workflow is provided in Figure 1.
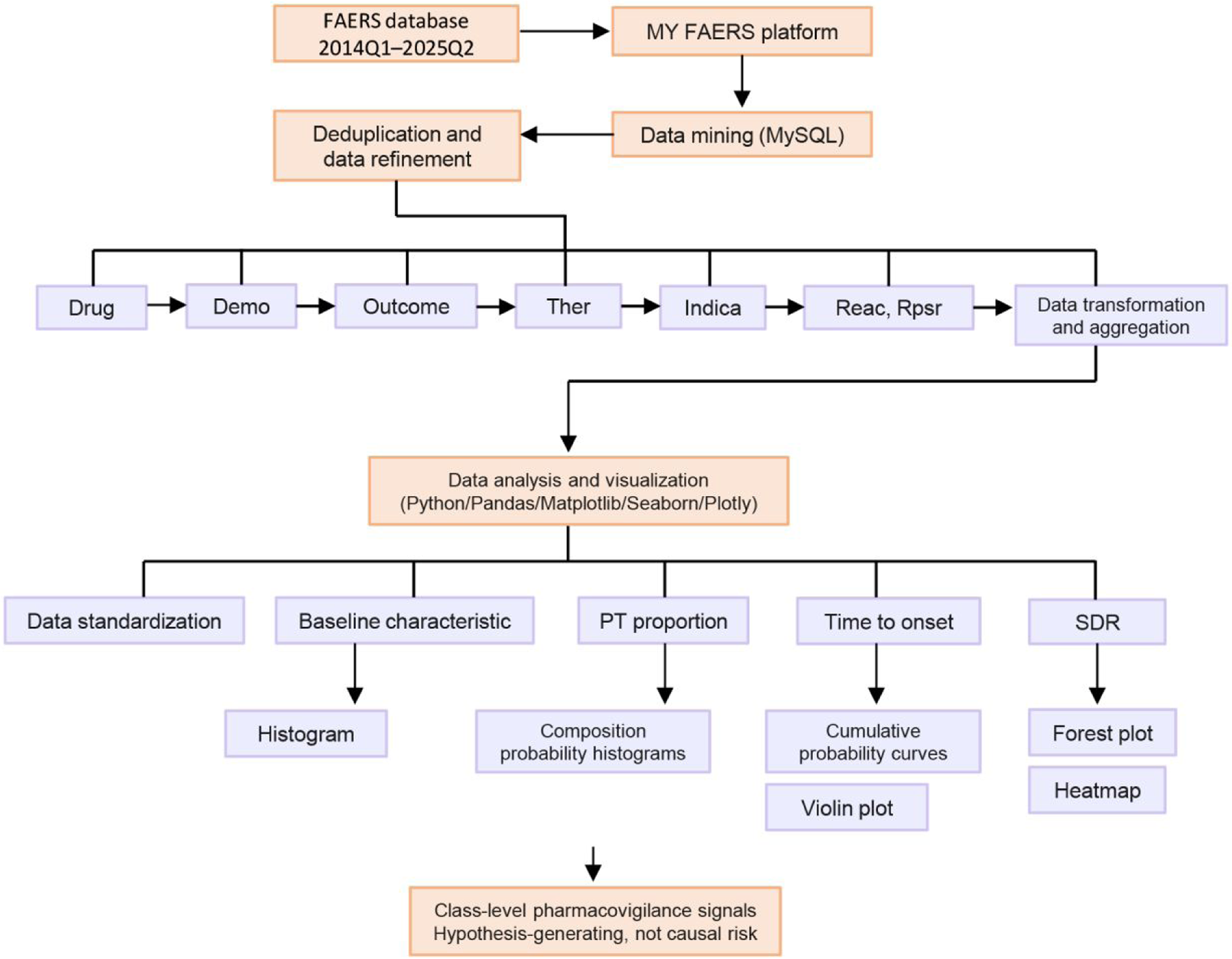
Infographic-style overview of the FAERS-based disproportionality analysis using the MY FAERS platform. FAERS reports from 2014Q1 to 2025Q2 were imported into the MY FAERS platform, followed by data integration, deduplication, and refinement. Reports were classified into memantine monotherapy, memantine-ChEIs combination, memantine-SGAs combination, ChEIs monotherapy, and SGAs monotherapy groups. Reporting odds ratios were calculated to identify signals of disproportionate reporting at the SOC and PT levels. The identified signals were interpreted as class-level pharmacovigilance signals rather than evidence of causal clinical risk. PT: preferred term; SOC: system organ class; SDR: signal of disproportionate reporting; ChEIs: cholinesterase inhibitors; SGAs: second-generation antipsychotics.
Study population and data refinement
The study cohort comprised patients treated with memantine. During the initial screening phase, reports in which memantine was designated as the “Primary Suspect” were extracted from the FAERS database. Subsequently, a concomitant medication screening phase was conducted, restricting the analysis to reports involving the concomitant use of either ChEIs or SGAs. Concurrently, reference screenings were carried out for reports related to monotherapy with ChEIs or SGAs, specifically excluding any reports involving concomitant memantine use, and restricted to those with the “dementia alzheimers type” as the indication. Overall, the data mining outcomes were categorized into five distinct groups: memantine monotherapy, memantine-ChEIs combination, memantine-SGAs combination, ChEIs monotherapy, and SGAs monotherapy. The specific drug names included in each category are detailed in Supplemental Table 2. ChEIs and SGAs were analyzed as therapeutic classes rather than as individual agents, because the primary objective of this study was to characterize class-level safety reporting patterns associated with memantine-based combination therapy. Given the limited number of reports for some individual agents, particularly within the memantine-SGAs group, agent-specific disproportionality analyses were not performed to avoid unstable estimates.
Signal of disproportionate reporting analysis
Disproportionality analysis is widely regarded as the benchmark approach for identifying potential safety signals within AE databases. In modern pharmacovigilance research, the SDR serves as the primary analytical endpoint.
21
In this study, we employed the reporting odds ratio (ROR) along with its 95% confidence intervals (CI) as the principal measure of disproportionality. The ROR values and corresponding CI were calculated following well-documented methodologies,22,23 with the detailed equations presented as Equation 1 and Equation 2.


Where “a” represents the number of reports containing both target drugs and target AEs; “b” represents the number of reports containing both other drugs (except target drugs) and target AEs; “c” represents the number of reports containing both target drugs and other AEs (except target AEs); “d” represents the number of reports containing both other drugs and other AEs. A significant SDR of AEs was established based on the lower ROR limit of the 95% CI being greater than 1, and when the interaction group had a minimum of 3 cases. 24
Using memantine as the reference group established the primary analytical framework. To further evaluate the robustness of the findings, we conducted sensitivity analyses under the consideration that concomitant medications might exhibit simple additive effects that amplify the detection of drug-related signals. Specifically, ChEIs and SGAs were alternatively used as reference groups (i.e., memantine-ChEIs combination versus ChEIs and memantine-SGAs combination versus SGAs) to confirm whether the observed AEs were exacerbated by synergistic drug interactions rather than additive effects. A signal was considered robust only if it remained statistically significant across the sensitivity analyses.
Results
Data mining
During the initial screening phase, we identified 2531 patients prescribed memantine in the FAERS database between 2014Q1 and 2025Q2. Following predefined study criteria and concomitant medication screening, reports were classified into three groups: memantine monotherapy (n = 1965), memantine-ChEIs combination (n = 482), and memantine-SGAs combination (n = 84). These groups exhibited 838, 379, and 115 PTs of AEs, respectively. In the reference screening phase, we identified 10291 patients treated with either ChEIs or SGAs, which were stratified into two reference groups: ChEIs monotherapy (n = 9344) and SGA monotherapy (n = 622). The complete data mining workflow is detailed in Figure 2.
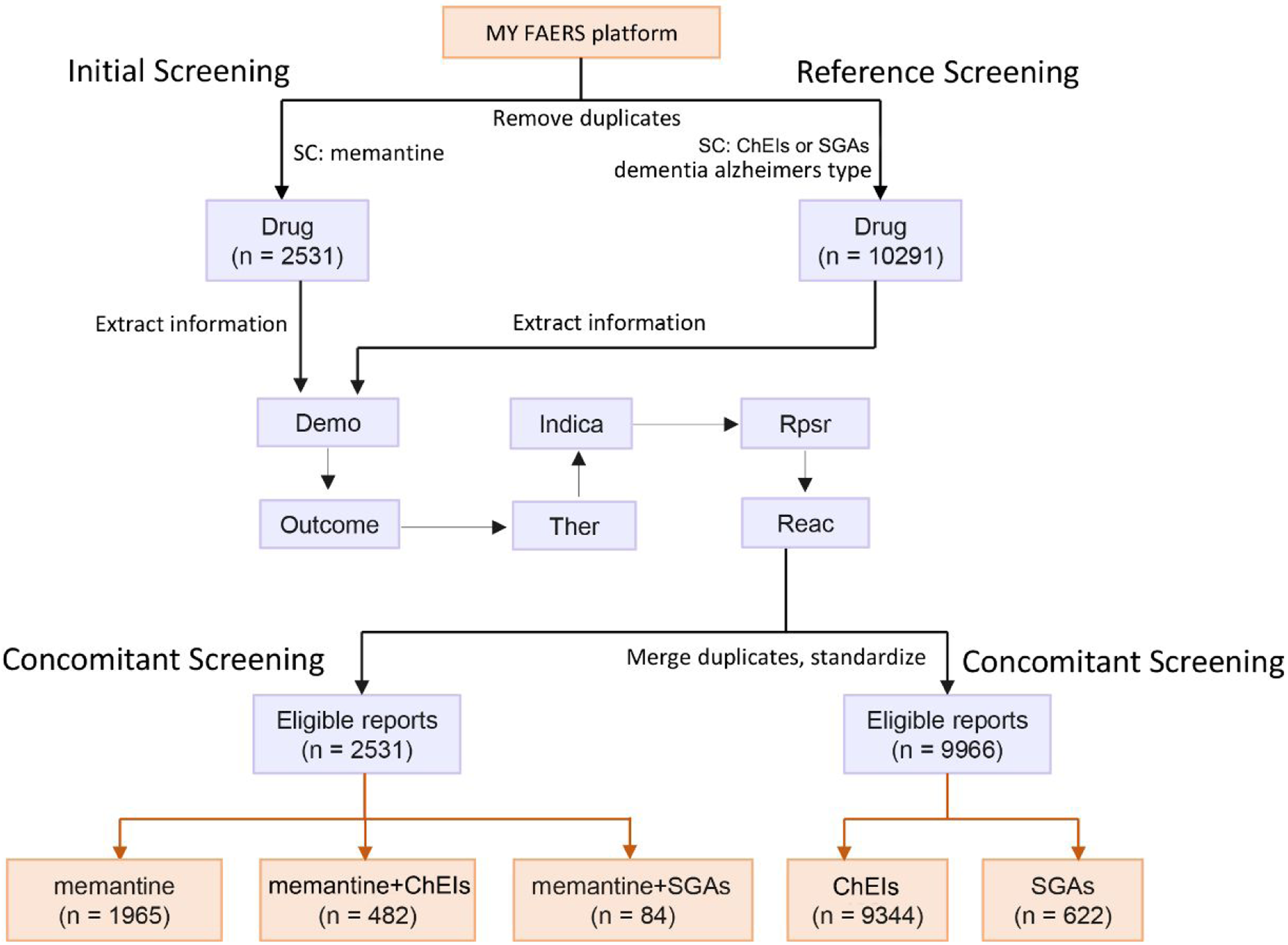
Data mining workflow for adverse event analysis using the MY FAERS platform. SC: screening criteria; ChEIs: cholinesterase inhibitors; SGAs: second-generation antipsychotics.
Baseline characteristics and reporting patterns
The total number of reported events differed substantially among these groups. Memantine monotherapy accounted for the highest number of reports (n = 1965), followed by memantine-ChEIs combination (n = 482), and memantine-SGAs combination (n = 84), indicating pronounced disparities in either usage patterns or reporting frequency. Gender distribution was similar across all groups, with a higher proportion of reports submitted for female compared to male patients, which aligns with the higher incidence of AD in women. 25 Age stratification indicated that the majority of reports occurred in patients aged 65 years or older, consistent with the use of these therapies in elderly populations, particularly for AD. 26 Temporal trends revealed distinct trajectories in reporting rates. Memantine monotherapy reports peaked around 2015, with fluctuations observed in subsequent years, suggesting initial widespread adoption followed by stabilization. In contrast, the memantine-ChEIs combination exhibited a moderate increase starting in 2017, reaching a maximum in 2017 before declining. Memantine-SGAs combination maintained consistently low reporting volumes throughout the study period. In terms of AE severity, other serious and hospitalizations were the most frequently reported serious outcomes across all three regimens. Life-threatening events and death were also documented but occurred less commonly. The primary sources of reports were physicians and consumers, with additional contributions from pharmacists and other health professionals. Together, these findings underscore distinct profiles in utilization, patient demographics, and reporting patterns associated with memantine-based therapies (Figure 3).
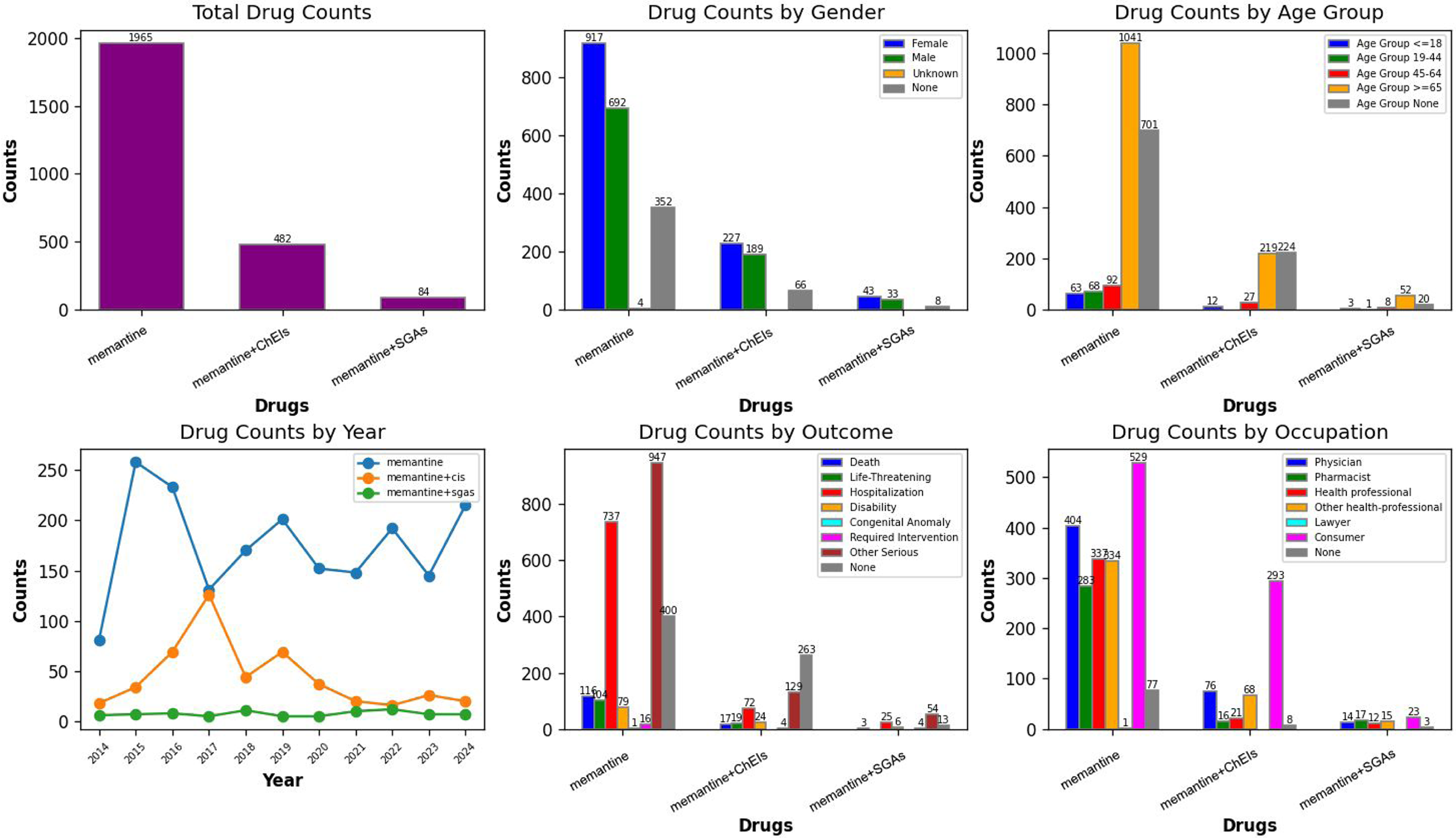
Multidimensional characterization of cases reported for memantine-based therapies. ChEIs: cholinesterase inhibitors; SGAs: second-generation antipsychotics.
Proportional analysis of AEs
Our systematic evaluation of the top ten AEs by proportion revealed both distinct and overlapping safety profiles across memantine-based therapies (Figure 4). In the memantine monotherapy group, drug ineffective and pulmonary embolism were prominent, together accounting for approximately 15% of reported events, markedly higher than observed in the other groups. The memantine-ChEIs combination group was characterized by a cluster of gastrointestinal and general events, including fatigue, nausea, diarrhea, and vomiting, which collectively represented nearly 40% of AEs, significantly exceeding their occurrence in the other regimens. In contrast, the memantine-SGAs combination group showed a distinct profile dominated by medication error, somnolence, and accidental overdose, together constituting nearly 35% of reports, which was substantially higher than in the other treatment groups. Several AEs were notably shared across regimens. Dizziness, fall, and hallucination were frequently reported in both the memantine monotherapy and memantine-ChEIs combination groups, with combined percentages exceeding 25%. Bradycardia was common to both memantine monotherapy and memantine-SGA combination therapy, reported in over 7% of cases in each. Furthermore, off-label use, confusional state, and agitation were consistently reported across all three treatment groups, jointly accounting for approximately 30% of events. Complete proportional data for all PTs are provided in Supplemental Table 3.
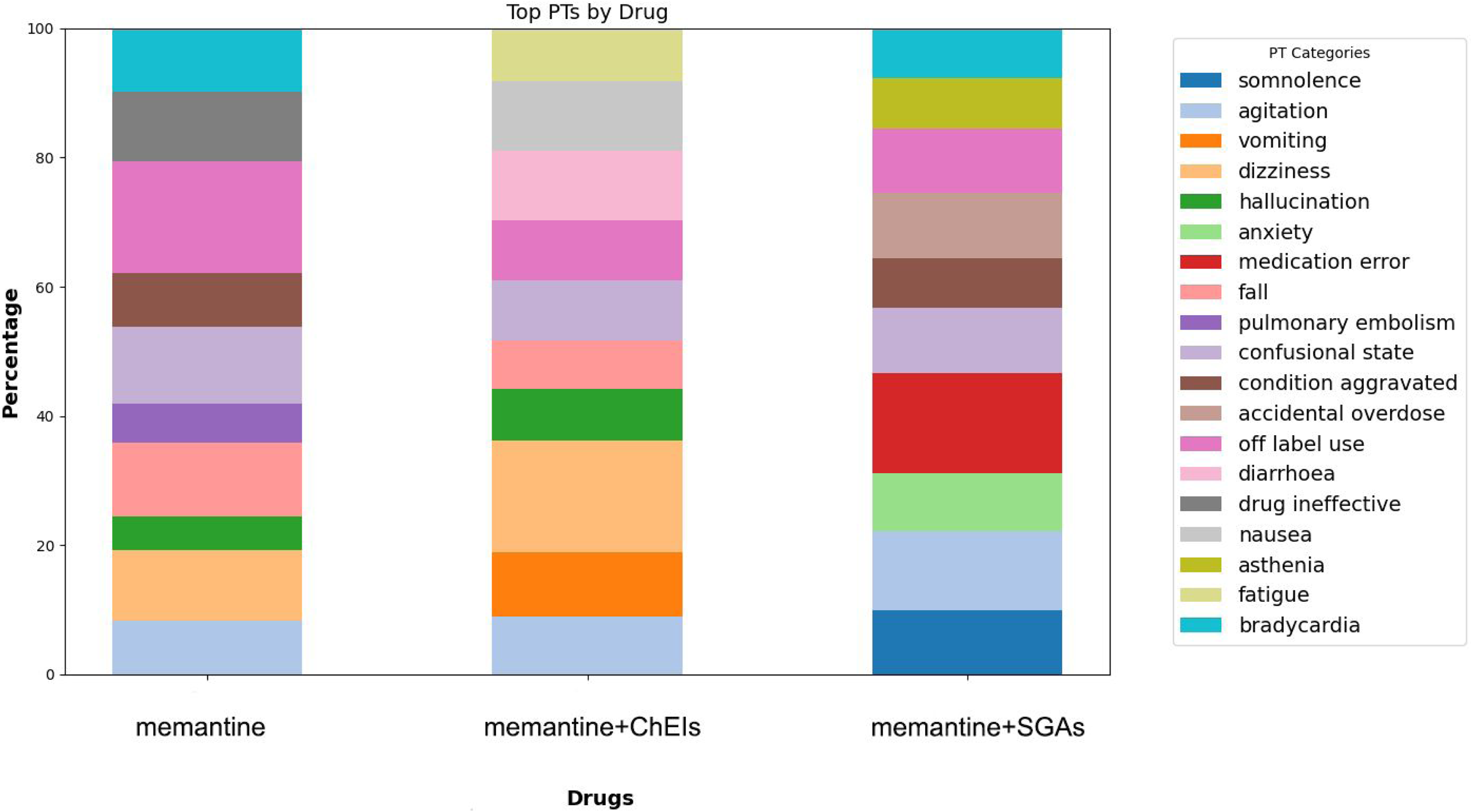
Top ten proportional distribution of adverse events across memantine-based therapies. PT: preferred term; ChEIs: cholinesterase inhibitors; SGAs: second-generation antipsychotics.
Temporal analysis of AE onset patterns
Our analysis of the time-to-onset of AEs across memantine-based therapies, utilizing both cumulative distribution plots and violin plot visualizations (Figure 5), revealed some temporal heterogeneity in AE emergence patterns. The memantine-ChEIs combination regimen exhibited the most rapid early-phase AE onset, reaching approximately 80% cumulative probability within the first 100 days post-treatment, indicating a steep initial rise in AE incidence. In contrast, the two other groups showed a slower but steady increase in AE occurrence, achieving 70% cumulative probability by day 200, reflecting a more gradual manifestation of adverse outcomes.
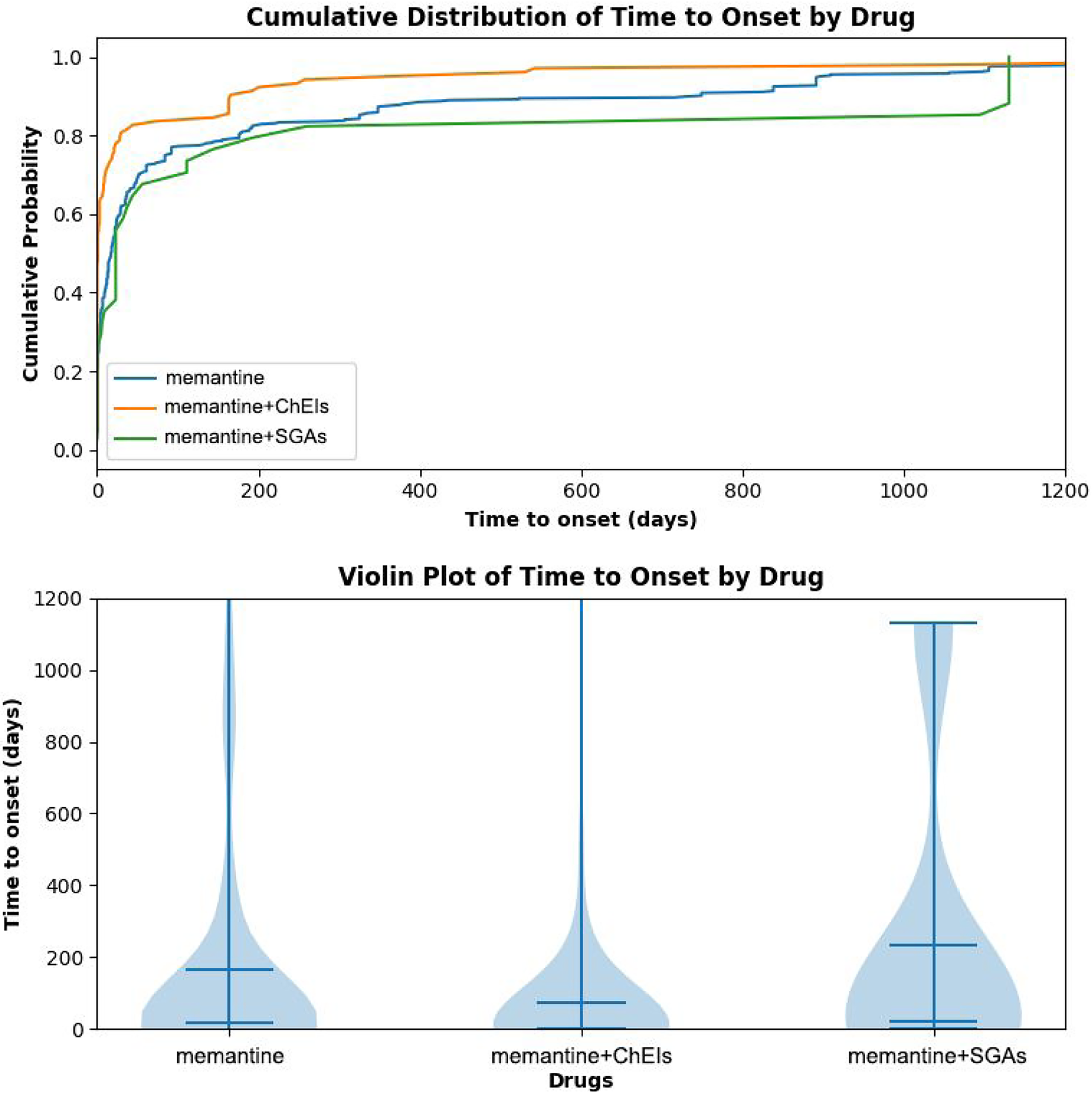
Time-to-onset profiles of adverse events across memantine-based therapies. ChEIs: cholinesterase inhibitors; SGAs: second-generation antipsychotics.
The violin plot further elucidates these temporal dynamics by highlighting the distributional characteristics of AE onset times. For memantine, the onset distribution is tightly clustered around the lower end of the timeline, with a narrow interquartile range and minimal tail extension, indicating high consistency in early AE emergence. The memantine-ChEIs combination group shows a similarly concentrated distribution, though slightly shifted toward earlier onset. In contrast, the memantine-SGAs group exhibits a markedly broader and more dispersed onset profile, with a wide interquartile range and a substantial upper tail extending beyond 1000 days. The observed differences may reflect underlying pharmacodynamic interactions, differential clearance kinetics, 27 or varying thresholds for toxicity induction across treatment combinations. 28 The extended latency period seen with memantine-SGAs combination warrants careful long-term monitoring in clinical practice, while the early-onset patterns in memantine-ChEIs combination highlight the need for vigilant short-term surveillance.
Reporting odds ratios
To systematically evaluate signal frequencies across memantine-based therapies, disproportionality analyses were conducted using the ROR method at the SOC level (Figure 6). Based on integrated primary and sensitivity analyses, six robust SDRs were identified for the memantine-ChEIs combination compared to memantine monotherapy. These included: skin and subcutaneous tissue disorders (ROR, 3.46; 95% CI, 2.05–5.85), gastrointestinal disorders (ROR, 2.53; 95% CI, 1.92–3.33), musculoskeletal and connective tissue disorders (ROR, 2.13; 95% CI, 1.29–3.50), psychiatric disorders (ROR, 1.60; 95% CI, 1.27–2.00), general disorders and administration site conditions (ROR, 1.53; 95% CI, 1.18–1.97), and nervous system disorders (ROR, 1.48; 95% CI, 1.19–1.84). Conversely, three pronounced SDRs were detected for the memantine- SGAs combination relative to memantine monotherapy: general disorders and administration site conditions (ROR, 3.97; 95% CI, 1.74–9.05), psychiatric disorders (ROR, 2.14; 95% CI, 1.32–3.49), and nervous system disorders (ROR, 2.03; 95% CI, 1.20–3.43).
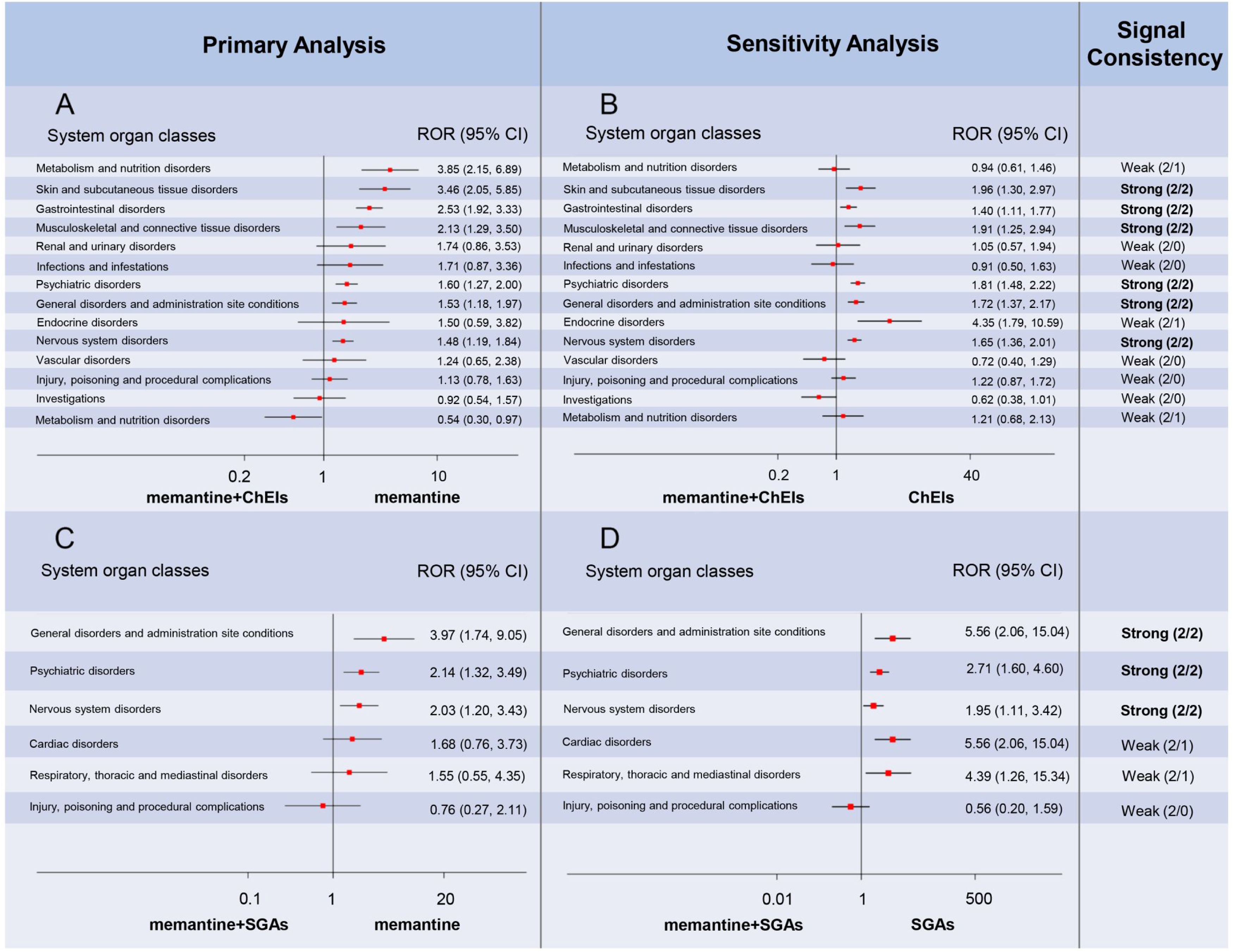
Reporting odds ratios for memantine-based therapies stratified by MedDRA system organ class categories.
Further disproportionality analyses at the PT level revealed additional significant associations (Figure 7; only significant results shown). For the memantine-ChEIs combination, eleven robust SDRs were observed, including: contusion (ROR, 5.62; 95% CI, 2.45–12.90), paranoia (ROR, 5.38; 95% CI, 2.11–13.70), swelling face (ROR, 4.29; 95% CI, 1.69–10.87), dysphagia (ROR, 4.28; 95% CI, 1.49–12.25), muscle spasms (ROR, 3.94; 95% CI, 1.73–8.99), feeling abnormal (ROR, 3.88; 95% CI, 2.00–7.53), crying (ROR, 3.55; 95% CI, 1.08–11.68), fatigue (ROR, 2.62; 95% CI, 1.56–4.39), psychomotor hyperactivity (ROR, 2.25; 95% CI, 1.04–4.87), dizziness (ROR, 1.87; 95% CI, 1.32–2.64), and hallucination (ROR, 1.65; 95% CI, 1.01–2.70). For the memantine-SGAs combination, nine robust SDRs were identified: personality change (ROR, 19.31; 95% CI, 6.00–62.19), hip fracture (ROR, 15.84; 95% CI, 3.72–67.41), anger (ROR, 13.50; 95% CI, 4.51–40.43), paranoia (ROR, 13.50; 95% CI, 4.51–40.43), delusion (ROR, 11.24; 95% CI, 3.87–32.68), mania (ROR, 9.69; 95% CI, 3.02–31.10), anxiety (ROR, 5.83; 95% CI, 2.63–12.93), asthenia (ROR, 3.97; 95% CI, 1.74–9.05), and agitation (ROR, 2.84; 95% CI, 1.46–5.51). Complete ROR values and corresponding 95% confidence intervals for all PT-level analyses are provided in Supplemental Table 4.
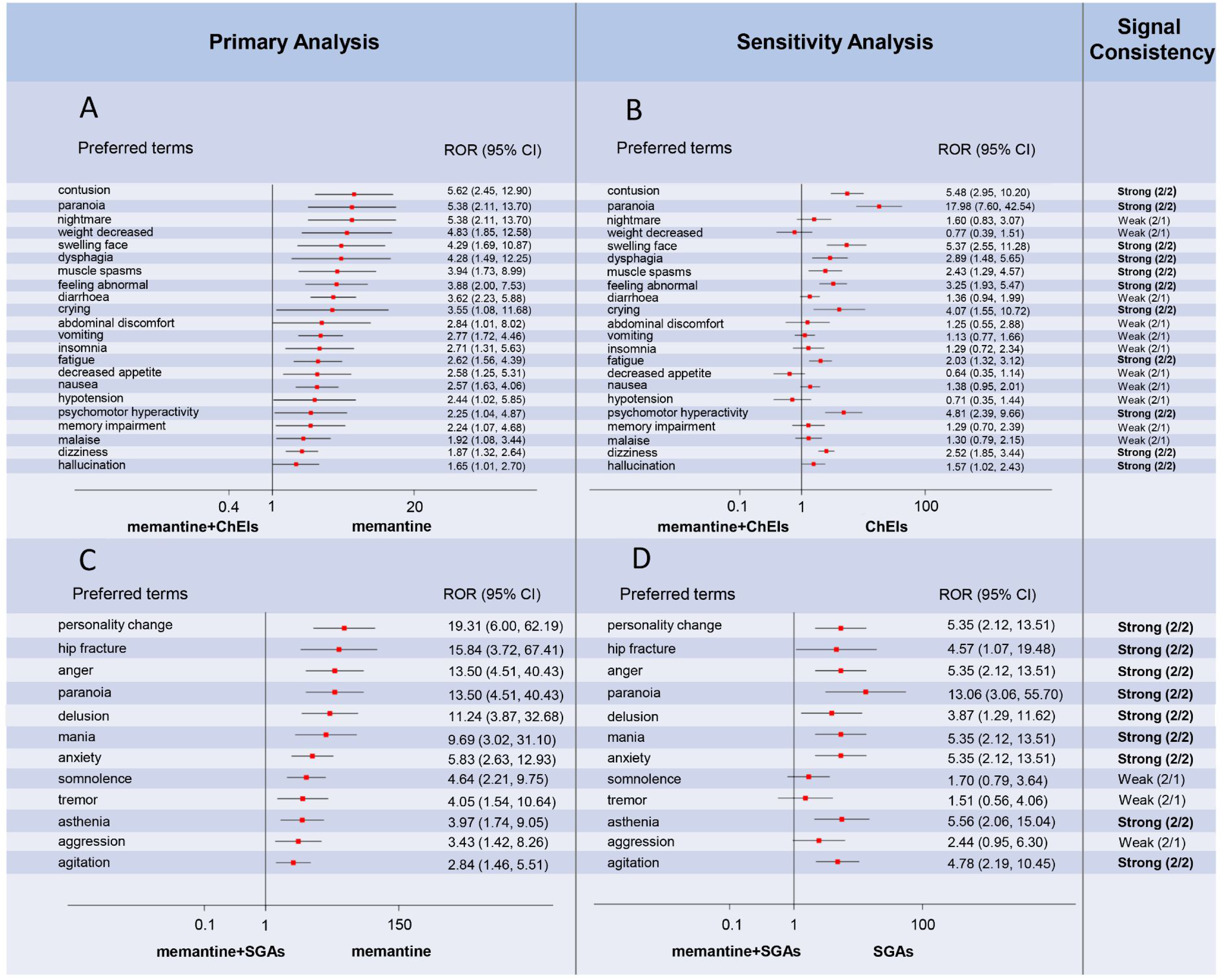
Reporting odds ratios for memantine-based therapies stratified by preferred term categories. (A) memantine-ChEIs combination versus memantine; (B) memantine-ChEIs combination versus ChEIs; (C) memantine-SGAs combination versus memantine; (D) memantine-SGAs combination versus SGAs; ROR: reporting odds ratio; CI: confidence interval; ChEIs: cholinesterase inhibitors; SGAs: second-generation antipsychotics.
Discussion
This study employed disproportionality analysis of the FAERS database to evaluate the safety profiles of memantine-based combination therapies compared to memantine monotherapy in patients with AD. Our findings identified distinct and disproportionately reported safety signals associated with memantine when combined with ChEIs or SGAs, corroborating and extending previously recognized AE profiles.
Importantly, several signals observed in the memantine-ChEIs group appear largely consistent with known adverse event profiles of ChEIs. Specifically, the elevated RORs for gastrointestinal disorders (e.g., dysphagia) and nervous system disorders (e.g., psychomotor hyperactivity, dizziness) align with the well-established cholinergic adverse effects of ChEIs such as donepezil. 29 Prior studies reporting high incidences of nausea (35–64%) and dizziness (11–43%) under combination therapy further support that these findings should be interpreted as confirmatory rather than novel signals, likely reflecting known pharmacological interactions between cholinergic and glutamatergic pathways. 30 It should be noted that the present study evaluated ChEIs as a pharmacological class rather than comparing individual ChEI agents. Donepezil was discussed as an illustrative example because it is commonly used in combination with memantine and is also available as a fixed-dose combination product. However, the observed signals should not be interpreted as being exclusively attributable to donepezil or to any other individual ChEI. Similarly, the memantine-SGAs analysis was performed at the class level and was not intended to determine whether specific SGAs differed in their contribution to the observed neuropsychiatric or fracture-related signals.
Beyond these confirmatory findings, additional signals were detected in less commonly emphasized categories, including skin and subcutaneous tissue disorders, musculoskeletal and connective tissue disorders (e.g., muscle spasms), psychiatric disorders (e.g., paranoia, hallucination), and general disorders and administration site conditions (e.g., swelling face, feeling abnormal, crying, fatigue). These signals should be interpreted as potentially less well-characterized or underexplored reporting patterns rather than definitive novel safety risks, and they warrant cautious interpretation and further clinical investigation.
In contrast, the memantine-SGAs combination demonstrated prominent disproportionality signals for psychiatric and neurological events, including personality change, mania, delusion, paranoia, and hip fracture. These findings are partially consistent with existing literature, which suggests that SGAs may exacerbate manic-like symptoms in patients with AD, particularly when co-administered with other central nervous system agents such as memantine. 31 Moreover, prior studies have reported that the sedative and extrapyramidal effects of SGAs may contribute to an increased risk of falls and fractures in older adults. 32 From a mechanistic perspective, it is conceivable that memantine, through modulation of glutamatergic signaling, may interact with the central nervous system effects of SGAs and potentially intensify inhibitory or neuropsychiatric responses. 33 Overall, these findings may offer incremental pharmacovigilance insights into the safety reporting patterns associated with memantine-SGAs co-administration.
The generalizability of our findings to the broader AD population is limited by the inherent characteristics of the FAERS database, which relies on spontaneous reporting and is susceptible to underreporting and various reporting biases.34,35 Although the demographic profile of the reported cases, which was predominantly female and aged over 65 years, is consistent with the known epidemiology of AD,36,37 enhancing the contextual relevance of our observations, the absence of denominator data precludes calculation of true incidence rates. Therefore, while the signals identified in this study reflect disproportionate reporting patterns, they should not be interpreted as direct measures of real-world risk. These findings are most relevant to the segment of the AD population that experiences adverse events severe or notable enough to trigger reporting to regulatory authorities.
From a pharmacovigilance perspective, these findings should not be interpreted as direct clinical effects in the management of AD. For memantine-ChEIs combinations, the observed signals may suggest the need for increased clinical awareness of gastrointestinal adverse events and dizziness, 30 particularly during the early phase of treatment, as indicated by the relatively rapid time-to-onset patterns (Figure 5). In addition, signals involving skin and subcutaneous tissue disorders, musculoskeletal and connective tissue disorders, psychiatric disorders, and general disorders warrant cautious interpretation and further clinical investigation. Regarding memantine-SGAs combinations, prominent PT-level signals (e.g., mania, paranoia, personality change, and hip fracture) may reflect underlying confounding factors, including disease severity, indication for BPSD, advanced age, and comorbidity burden, rather than a direct causal effect of the drug combination. Instead, they should be considered hypothesis-generating safety signals derived from spontaneous reporting data. Generally, these findings align with current clinical guidelines that support the use of memantine-ChEIs combinations in moderate-to-severe AD, 6 but also emphasize that memantine-SGAs regimens should be employed with extreme caution, reserved for short-term use when absolutely necessary, and subject to thorough risk-benefit evaluation. 9
To confirm and quantify the SDRs identified in this pharmacovigilance study, prospective, well-controlled observational investigations or pragmatic clinical trials are essential. A large-scale cohort study leveraging electronic health records could accurately estimate incidence rates while adjusting for key confounders such as disease severity, comorbidities, and concomitant medications. In particular, a study specifically designed to compare the risk of manic-like symptoms and fractures in AD patients exposed to memantine-SGAs combination therapy versus those receiving SGAs monotherapy would yield highly valuable evidence for clarifying the incremental risk associated with combination therapy.
This study has several limitations inherent to its pharmacovigilance design and the FAERS data source. First, disproportionality analysis based on spontaneous reporting systems cannot establish causality or estimate true clinical risk.38,39 ROR reflects reporting disproportionality rather than incidence, and an elevated ROR does not demonstrate that the drug combination directly caused the adverse event. 40 Second, the analysis may be affected by reporting bias and incomplete information. 41 Although duplicate and follow-up reports were purged using the deduplication procedure embedded in the MY FAERS platform, residual duplication or inconsistencies cannot be completely excluded. In addition, severe, novel, or highly publicized events are more likely to be reported.42,43 Third, confounding by indication remains an important concern. Patients receiving combination therapies, particularly memantine with SGAs, may have more severe or treatment-resistant disease, which itself may increase the risk of falls or neuropsychiatric events. Although sensitivity analyses using ChEIs or SGAs monotherapy as reference groups were performed, these analyses could not fully account for channeling bias or differences in disease severity.44,45 Fourth, ChEIs and SGAs were analyzed as therapeutic classes rather than individual agents. While this approach improved statistical stability, it limited our ability to identify agent-specific associations, especially in the relatively small memantine-SGAs group. Fifth, dose-response relationships could not be evaluated because dose information in FAERS is often incomplete, inconsistently reported, and difficult to standardize across formulations and concomitant regimens. Therefore, the observed SDRs should be interpreted as dose-unadjusted, class-level, hypothesis-generating signals that require confirmation in well-designed observational or prospective studies.
Conclusion
In summary, this FAERS-based disproportionality analysis identified distinct safety SDRs associated with memantine-based combination therapies compared with monotherapy. The memantine-ChEIs combination showed signals involving skin, gastrointestinal, musculoskeletal, psychiatric, general, and nervous system disorders, while the memantine-SGAs combination demonstrated notable signals for psychiatric disorders, nervous system disorders, general disorders, and hip fracture. These findings should be interpreted as hypothesis-generating rather than evidence of causal risk and warrant further validation in well-designed real-world or prospective studies.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261458818 - Supplemental material for Adverse events of Alzheimer's disease patients treated with memantine-based therapies: A disproportionality analysis of the FAERS database based on the MY FAERS platform
Supplemental material, sj-docx-1-alz-10.1177_13872877261458818 for Adverse events of Alzheimer's disease patients treated with memantine-based therapies: A disproportionality analysis of the FAERS database based on the MY FAERS platform by Xiaozhen Wang, Wei Zhang, Jing He, Xu Zhang, Rong Wang and Ze Li in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The National Natural Science Foundation of China (grant numbers: 82504761).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data generated or analyzed during this study are included in this published article and its Supplemental Material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.