
Abstract
Background
Evidence suggests that dysregulation of the renin angiotensin system (RAS) is associated with the pathophysiologic process of Alzheimer's disease (AD). Few studies have evaluated the relationship between circulating RAS components and incident cognitive decline or impairment.
Objective
Our study aims to evaluate the relationship between circulating RAS biomarkers (angiotensin II [ANGII], angiotensin 1-7 [ANG1-7], angiotensin converting enzyme-1 [ACE-1], and 2 [ACE-2]), in initially cognitively healthy adults, and incident cognitive decline and cognitive impairment.
Methods
In this secondary analysis, 310 community-dwelling participants from the randomized controlled Action for Health in Diabetes (Look AHEAD) study without dementia, who were not on RAS-altering medication, were included.
Results
Participants, compared to those excluded, were more likely to be female (65%), white (76%), overweight (34%), have lower baseline HbA1c (6.7%), lower SBP (119.7 mmHg), lower serum creatinine (0.79 mg/dL), higher total cholesterol (190.1 mg/dL) and LDL (112.5 mg/dL), and higher history of dyslipidemia (65%) at baseline. 1 SD increase of ANG1-7 measured in year 1 was associated with lower odds of cognitive impairment (OR = 0.35, 95% CI 0.16-0.77; p = 0.001), while higher ANG1-7 levels predicted better global cognitive function [β x 10−3 = 1.03 (0.50); p = 0.039], 15 years later.
Conclusions
These results provide preliminary evidence that circulating RAS components are predictive of protection against cognitive impairment and decline and may serve as a marker of the early stages of dementia. Further research is warranted to fully understand the relationship between the brain and the circulatory RAS.
Keywords
Introduction
Neuropathological changes of Alzheimer's disease (AD) begin years before symptom onset. 1 Because neuropathological changes are multifaceted and heterogeneous, there is a continuing need to identify novel treatment targets to prevent or mitigate cognitive impairment.
Emerging evidence suggests that the renin-angiotensin system (RAS) is involved in cognitive decline associated with AD pathogenesis.2–4 In addition to a systemic RAS, a local RAS has been identified in the brain, which, however, interacts with the systemic RAS, and both can modulate AD. 5 The RAS can be mechanistically divided into two pathways. The classical RAS pathway (cRAS), which includes the angiotensin II (ANGII) peptide acting at the angiotensin 1 receptor (AT1R), promotes neuroinflammation, oxidative stress, cerebrovascular dysfunction, and the angiotensin converting enzyme 1 (ACE-1), the enzyme responsible for its production. 5 The protective arm of the RAS, the regulatory pathway (rRAS), involves ACE-2-mediated cleavage of ANGII into angiotensin 1-7 (ANG1-7) and activation of the MAS1 receptor, which mediates vasodilatory, antiproliferative, antioxidant, and anti-inflammatory effects of ANG1-7 and the angiotensin type-2 receptor (AT2R), therefore opposing the effects of AT1R. 5
This cRAS pathway has been extensively studied in relation to cognitive decline and AD. 6 Human autopsy studies show increased levels of ANGII in people with AD, which could be due to numerous processes, but mainly from increased ACE-1 activity that promotes the formation of ANGII from angiotensin I. 2 Elevated levels of ANGII increase the activation of the AT1R, which is associated with disease progression due to the promotion of numerous deleterious processes including the accumulation of amyloid-β (Aβ) and tau.3,5,7–10 In studies in AD patients, the ACE-1 activity was elevated in cerebrospinal fluid (CSF).11,12 Whether changes in systemic circulatory RAS reflect changes in the brain and CSF, and whether these changes are associated with cognitive function in AD, is less clear. One study of 56 unimpaired participants from the Brain Health Substudy of the Baltimore Experience Corps Study showed an association between higher blood ACE-1 levels and worse working memory measures at the 1-year follow-up. 6 In contrast, higher ANGII levels were associated with worse delayed recall. 6 Only one cross-sectional study has evaluated the association between circulatory RAS levels and showed that ACE-1 levels were lower, in both blood and CSF, in AD participants than in cognitively unimpaired individuals. 13
It is thought that the rRAS pathway counteracts the negative effects of the cRAS, and in AD, this balance is disrupted. 7 In a human autopsy study, ACE-2 levels were decreased, while the accumulation of Aβ and tau was increased. 14 Recent studies also reported decreased ANG1-7 brain levels 15 and circulatory levels 16 in people with AD, and Jiang et al. found that decreased ANG1-7 levels were positively associated with cognitive function. 17
Taking all this together, the data suggest that circulating RAS markers in the blood may be related to cognitive function and decline and could serve as a potential proxy for brain RAS signaling.
One limitation of the literature on RAS and aging brain is that a comprehensive assessment of the relationship between circulatory RAS peptides, central to both cRAS and rRAS, and in relation to cognitive function and impairment, has not been undertaken. 5 Additionally, no studies have assessed the longitudinal associations between RAS peptides and enzymes, risk of cognitive impairment, and cognitive function.
Another limitation of the RAS-brain literature is that this relationship is not very well characterized in the context of including type 2 diabetes mellitus (herein “diabetes”) diabetes, which is highly prevalent and increases Alzheimer's disease and related dementias (ADRD) risk.18,19 The RAS is involved in diabetes-associated micro- and macrovascular complications and plays a vital role in obesity.20,21 However, no studies have evaluated the role of RAS and cognitive impairment in a population enriched for diabetes, obesity, and overweight.
In this study, we examined the associations between blood ANGII, ANG1-7, ACE-1, and ACE-2, in adults initially free of dementia with diabetes, who were overweight or obese, and the risk of cognitive impairment or cognitive decline with an average follow-up of 15 years. Our study aims to determine to evaluate the relationship between circulating RAS biomarkers (ANGII, ANG1-7, ACE-1, and ACE-2), in initially nondemented adults and incident cognitive decline and impairment.
Methods
Study populations and study design
The Action for Health in Diabetes (Look AHEAD) was a multicenter, randomized controlled trial that recruited 5145 individuals from 16 centers across the USA from 2001 to 2004 who were overweight or obese and had diabetes. At enrollment, participants were 45-76 years of age with body mass index (BMI) > 25 kg/m2 (>27 kg/m2 when on insulin), glycated hemoglobin (HbA1c) < 11%, systolic/diastolic blood pressure <160/<100 mmHg, triglycerides <600 mg/dl, and reported consuming <14 alcoholic drinks per week. 22 Participants were randomly assigned with equal probability to a multidomain Intensive Lifestyle Intervention (ILI) or a Diabetes Support and Education (DSE) control intervention. The ILI included frequent group and individual sessions focused on individualized discussions of diet modification and physical activity designed to induce and maintain an average weight loss of >7%. 22 The DSE group received three group sessions per year, providing general information on diet, physical activity, and social support, for the first four years, followed by annual group meetings thereafter. 22 At initial and yearly follow-up visits, medical history and medications were assessed, and weight, height, and blood pressure were measured.
The trial and intervention arms were stopped in September 2012 after an average of 9.6 years due to futility. Despite achieving greater weight loss and improved glycemic control, there was no difference in the primary composite outcome of cardiovascular events between the ILI and DSE groups. 23 The study continued as an observational cohort through 2021. As part of several separately funded ancillary studies, the cohort study and cognitive tests were continued.
For this study, participants were included from the original Look AHEAD study, the Look AHEAD Extension (Look AHEAD-E), the Look AHEAD Continuations (Look AHEAD-C) studies, as well as the Look AHEAD Brain (Look AHEAD-Brain) MRI imaging, the Look AHEAD Movement and Memory (Look Ahead-M&M), and the Look AHEAD-MIND studies all of which had blood samples available at years 1 and 4. We limited participants to those not taking medications that directly affect the RAS, including ACE-I or angiotensin II receptor blockers (AT1R), at the time of the blood draw (and 6 months before the yearly study visit) and during any other study visits. This exclusion, vital for accurate measurement of RAS enzymes and peptides, resulted in a significant reduction in our study sample. At year 1, 62% reported the use of ACE-I or AT1R, which increased to 71% by year 4, aligning with treatment guidelines for people with type 2 diabetes mellitus, where ACE-I and AT1R blockers are recommended as first-line treatments for hypertension. 24
As a result, our final study sample consisted of N = 310 participants who had blood available and stored at years 1 and 4, and all underwent standardized cognitive testing and dementia adjudication. To measure RAS markers in years 1 and 4 was chosen because a previous study by Yasar et al. 6 showed that there was no change in RAS markers during a one-year interval in cognitively unimpaired individuals with a high burden of vascular risk factors.
The study was approved by the Johns Hopkins University Institutional Review Board (IRB) under protocol number #IRB00274756. The requirement for obtaining informed consent was waived as this was a secondary data analysis, and the dataset was anonymized.
Measurement of RAS
Plasma ACE-1 concentration was measured using a commercially available Duoset sandwich ELISA kit (R&D Systems) as previously described for the measurement of ACE-1 protein in serum.13,25 Plasma samples were diluted 1:160, and the concentration of ACE-1 was measured in duplicate and averaged after interpolation from the reference standard curve (8000–125 pg/mL) for each case.
Plasma ACE-2 concentration was measured using a commercially available DuoSet sandwich ELISA kit (R&D Systems), which we have previously used to measure ACE-2 in postmortem CSF. 11 We followed the manufacturer's protocol with minor modifications using the capture antibody (4 μg/mL) and detection antibody (200 ng/mL) at 2-fold higher concentrations. ACE-2 concentrations were measured in duplicate, and the average was calculated after interpolation from the standard curve for each sample (2500–40 pg/mL).
Plasma ACE-1 enzyme activity was measured using an immunocapture-based fluorogenic activity assay as previously described in serum.13,25 The assay is based upon cleavage of an ACE-1 FRET peptide (Abz-FRK(Dnp)-P) (Enzo Life Sciences), used previously to measure ACE-1 enzyme activity in serum, 26 with the addition of a ‘capture’ antibody to immobilize ACE-1 and remove potential enzymes with overlapping specificity, before the addition of the FRET peptide, to improve specificity. 27 ACE-1 activity was expressed as relative fluorescence units (r.f.u).
Plasma ACE-2 enzyme activity was measured using an immunocapture-based fluorogenic activity assay using an ACE-2 FRET substrate (Mca-APK(Dnp) (Enzo Life Sciences), as previously described for serum. 28 For plasma measurements, an initial capture antibody was required to immobilize ACE-2 before the addition of the FRET peptide. ACE-2 activity was expressed as r.f.u.
Plasma concentrations of ANGII and ANG1-7 were measured using in-house, directly developed ELISAs as previously described.26,29 Plasma samples were diluted 1:4 for the ANGII assay and 1:6 for the ANG1-7 assay. Concentrations of ANGII and ANG1-7 were interpolated from serially diluted recombinant ANGII and ANG1-7 (20,000–312.5 ng/mL) (Enzo Life Sciences). The concentrations of each angiotensin peptide were interpolated from the standard curve, and the average values for duplicate readings were calculated. Minimal cross-reactivity was observed between angiotensin peptides using the in-house direct ELISAs, as previously shown. 29
Cognitive assessment and dementia diagnosis
Cognitive assessments were conducted between August 2009 and February 2020 in various ancillary and extension studies: Look AHEAD M&M (August 2009 - June 2012, N = 977), Look AHEAD Brain (November 2011 – August 2013, N = 319), and Look AHEAD-C (August 2013 – December 2014, N = 3075). The same cognitive protocol was applied in the Look AHEAD-MIND (May 2018-Feb 2020, N = 2451), allowing for a total of 4 possible cognitive assessments at years 8–9, 10–11, 12–14, and 15–18 from randomization.
The cognitive testing included the Rey Auditory Verbal Learning Test (RAVLT) to assess verbal learning and memory, 30 Digit Symbol Substitution Test (DSST) to determine attention and processing speed, 31 the Modified Stroop Color and Word Test (Stroop) to assess interference, 32 and the Trail Making Test Parts A and B (TMT, Part A and B) to evaluate attention, processing speed and executive function, respectively (Reitan, 1958). 33 The Modified Mini Mental Status Exam (3MSE) assessed global cognitive function. 34
Cognitive adjudication started in year 10. When a participant scored below the pre-specified age- and education-specific cut point, it triggered the administration of the Functional Assessment Questionnaire (FAQs) 35 to a friend or family member previously identified by the participant to assess functional status and performance in instrumental activities of daily living, aiming to help identify cognitive impairment. Two masked adjudicators independently reviewed all Look AHEAD cognitive test and depression scores, FAQ, and medical and health information to classify participants as not impaired, having mild cognitive impairment (MCI), 36 or having probable dementia. 37 Due to the relatively small number of dementia cases, participants diagnosed with MCI and/or probable dementia (N = 19, 6%) were combined into a “cognitive impaired” group.
Covariates
Based on previous literature, we assessed baseline covariates hypothesized to be related to diabetes, obesity, or dementia. These included baseline: age, sex, race/ethnicity, education (high school or less, college graduate, post-college), randomization arm, BMI (kg/m2) category (≥25 - < 30, ≥30 - < 40, and ≥40), HbA1c % (< 7.0, 7.0–8.9, >9.0), serum creatinine, mean systolic and diastolic blood pressure (SBP, DBP), apolipoprotein ε4 (APOE) allele (no ε4, one ε4, two ε4 alleles), history of chronic kidney disease, history of hypertension, history of heart failure and history of cardiovascular disease (CVD). History of CVD included self-report of myocardial infarction, coronary artery bypass graft, carotid endarterectomy, lower leg angioplasty, aortic aneurysm, congestive heart failure, or history of stroke. APOE ε4 carrier status was determined for participants who provided consent (80% of women versus 86% of men, p < 0.001) using TaqMan genotyping (rs7412 and rs429358).
Blood samples to measure Aβ42 and Aβ40 levels were collected at baseline and at approximately 8–12 years later. EDTA plasma samples were sent to Medpace Reference Laboratories. All samples were run in a single batch using the same lot of reagents. Aβ42 and Aβ40 were measured using an assay kit (Simoa Human Neurology 4-Plex E Advantage Kit) on a bead-based immunoassay analyzer (Quanterix Simoa HD-X, Quanterix Corp). The within-run coefficients of variation ranged between 3%-19%, and the between-run coefficients of variation ranged between 6%-13%.
Statistical analysis
We examined the differences in RAS enzymes (ACE-1 and ACE-2 levels and activity) and peptides (ANGII and ANG1-7 levels) over time (years 1 and 4), as well as those between subgroups, using linear mixed models adjusted for potential confounders to account for the correlation between repeated measures. For these models, in which outcomes are highly skewed, we used log-transformed values to model these relationships and subsequently back-transformed the adjusted means and standard errors.
Logistic regression was used to examine the relationship between RAS components, measured in years 1 and 4 (ACE-1 and ACE-2 levels and activity; ANGII and ANG1-7 levels), and cognitive impairment, assessed at the end of the original study between years 10 and 18, after adjusting for potential confounders.
Simple linear regression was used to examine further the relationships between RAS components (ACE-1, ACE-2, ANGII, and ANG1-7 levels) measured in years 1 and 4, and z-scores of cognitive outcomes from the first measurement timepoint in the subsample of participants who remained cognitively unimpaired, as adjudicated by the study at year 10 (n = 291), after adjusting for potential confounders.
Because our goals are descriptive, rather than inferential, we do not control for multiple comparisons.
Results
Study participants and study design
Figure 1 illustrates the Look AHEAD study timeline, including ancillary studies, blood draw timing, and cognitive assessment dates.
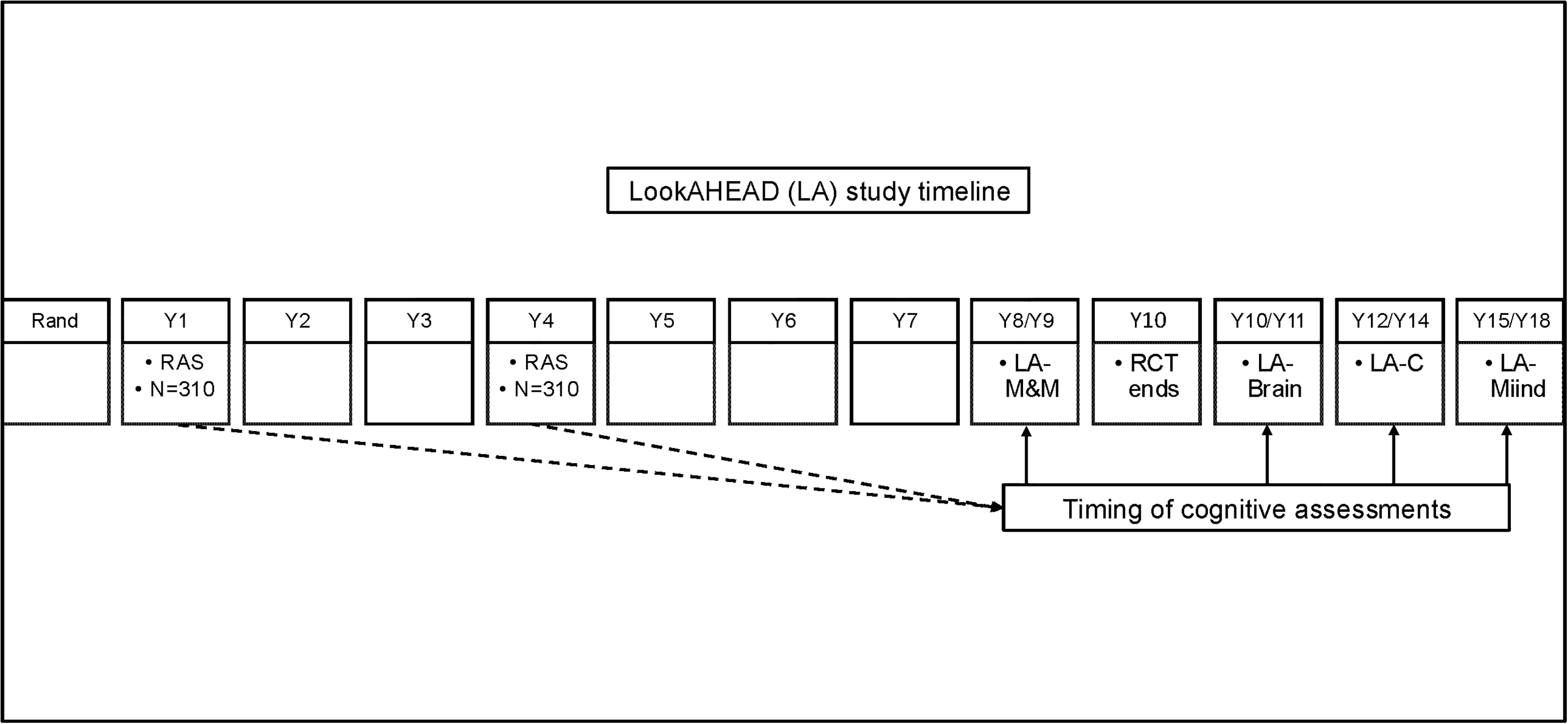
Timeline of the Look AHEAD study and ancillary studies, blood draws, and cognitive assessments. Randomization of the trial begins (Rand). Randomized Controlled Trial (RCT) ends at year 10. Renin angiotensin system (RAS), blood draws to measure the renin angiotensin system peptides and enzymes at year 1. Renin angiotensin system (RAS), blood draws to measure the renin angiotensin system peptides and enzymes at year 4. Cognitive assessment during different ancillary studies allowing for a total of 4 possible cognitive assessments: Look Ahead Movement and Memory (LA-M&M) at years 8–9. Look AHEAD Brain (LA Brain) at years 10–11. Look AHEAD-Continuation (LA-C) at years 12–14. Look AHEAD-MIND (LA-MIND) at years 15–18 years.
Participants, compared to those excluded, were more likely to be female (65%), be non-Hispanic white (76%), be overweight (34%), and have lower baseline HbA1c (6%), lower SBP (119.7 mmHg), lower serum creatinine (0.79 mg/dL), higher total cholesterol (190.1 mg/dL) and LDL (112.5 mg/dL), higher history of dyslipidemia (65%) and lower diabetes medication use (64%) (Table 1) measured at baseline.
Baseline characteristics of participants who were included (who did not report any use of antihypertensive medication acting through the renin angiotensin system [RAS-AHM]) and participants who were excluded (the rest of the Look AHEAD).
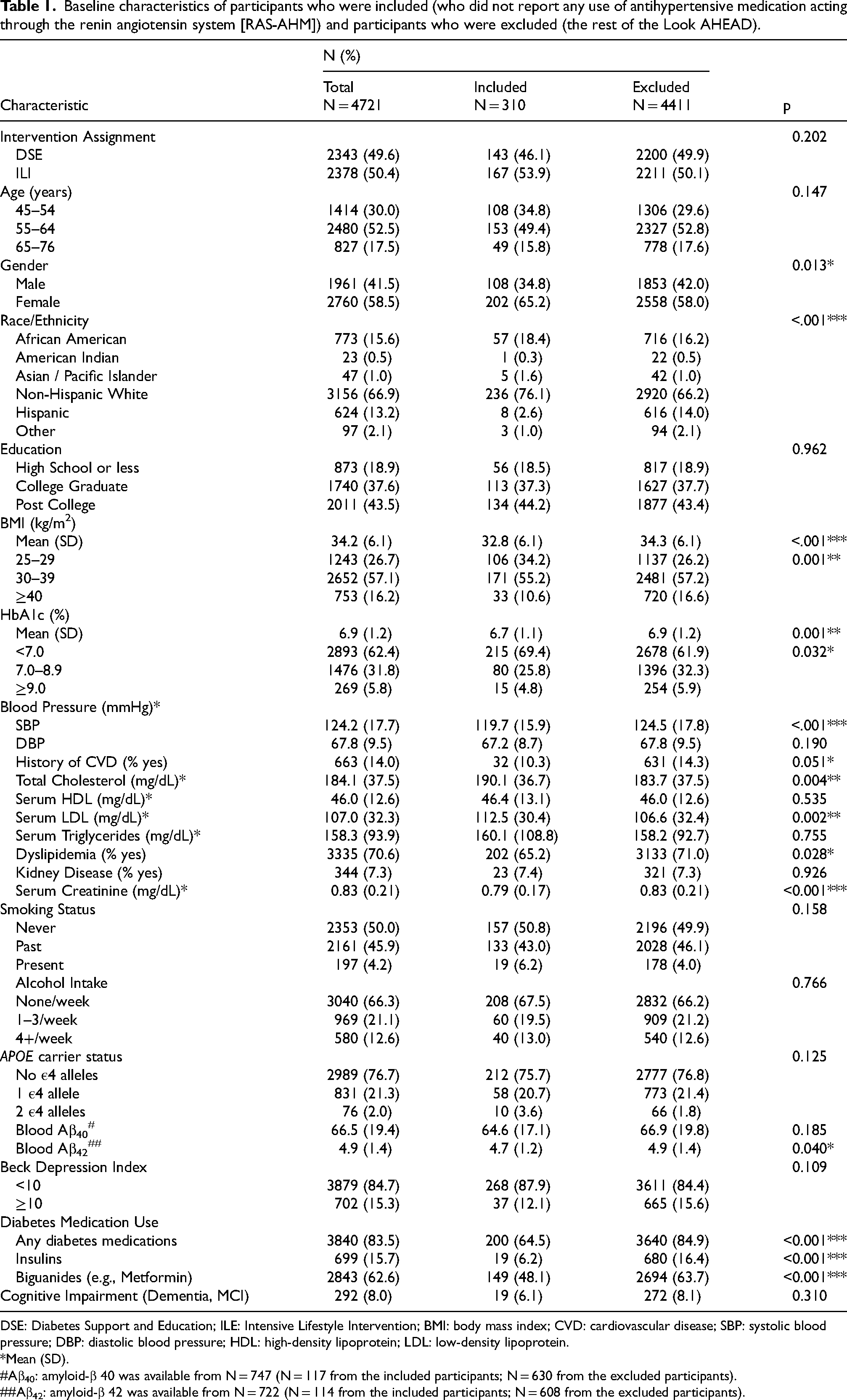
DSE: Diabetes Support and Education; ILE: Intensive Lifestyle Intervention; BMI: body mass index; CVD: cardiovascular disease; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: high-density lipoprotein; LDL: low-density lipoprotein.
*Mean (SD).
Aβ40: amyloid-β 40 was available from N = 747 (N = 117 from the included participants; N = 630 from the excluded participants).
Aβ42: amyloid-β 42 was available from N = 722 (N = 114 from the included participants; N = 608 from the excluded participants).
Participants included n = 202 females (65%), of whom 76% were postmenopausal. The age range of participants at baseline was 45–76 years. The majority were non-Hispanic white (76%) and had a college education (44%), were overweight (55%), and had controlled diabetes (Table 1).
RAS enzyme and peptides measures
ACE-1 and ACE-2 levels and activity, and ANGII and ANG1-7 levels are shown in Supplemental Table 1. We found that in the fully adjusted model, ANG1-7 measured in years 1 and 4 was significantly lower in the ILI arm compared to the DSE arm. Similarly, ACE-2 activity measured in year 1 was lower in the ILI arm (Supplemental Table 2). ACE-2 activity was significantly lower in years 1 and 4 in females (Supplemental Table 4). There is evidence that estrogen affects RAS 38 ; thus, we evaluated RAS peptides and enzymes and found that ANGII levels were significantly lower in postmenopausal women (Supplemental Table 5). Therefore, all analyses were adjusted for menopausal status. Interestingly, SBP was not associated with RAS enzyme levels/activity or peptide levels (Supplemental Table 6); however, ANG1-7 levels measured in years 1 and 4 were significantly lower, and ACE-1 activity measured in year 4 was significantly higher in people with serum creatinine ≥ 0.8 mg/dL (Supplemental Table 7).
Association between RAS enzymes and peptides and cognitive impairment
Nineteen participants developed cognitive impairment (MCI or all-cause dementia) during an average of 14.8 years of follow-up.
In the fully adjusted model, a 1 SD increase in circulating ANG1-7 levels was significantly associated with reduced odds of developing cognitive impairment (OR = 0.35, 95% CI 0.16–0.77; p = 0.009), a mean of 14.8-years years later (Table 2). There was no association between ACE-1 or ACE-2 levels and risk of cognitive impairment.
Logistic regression results of renin angiotensin system (RAS) peptide and enzyme measures at year 1 and year 4, predicting cognitive impairment (mild cognitive impairment or probable dementia) over mean of 14.8 years.
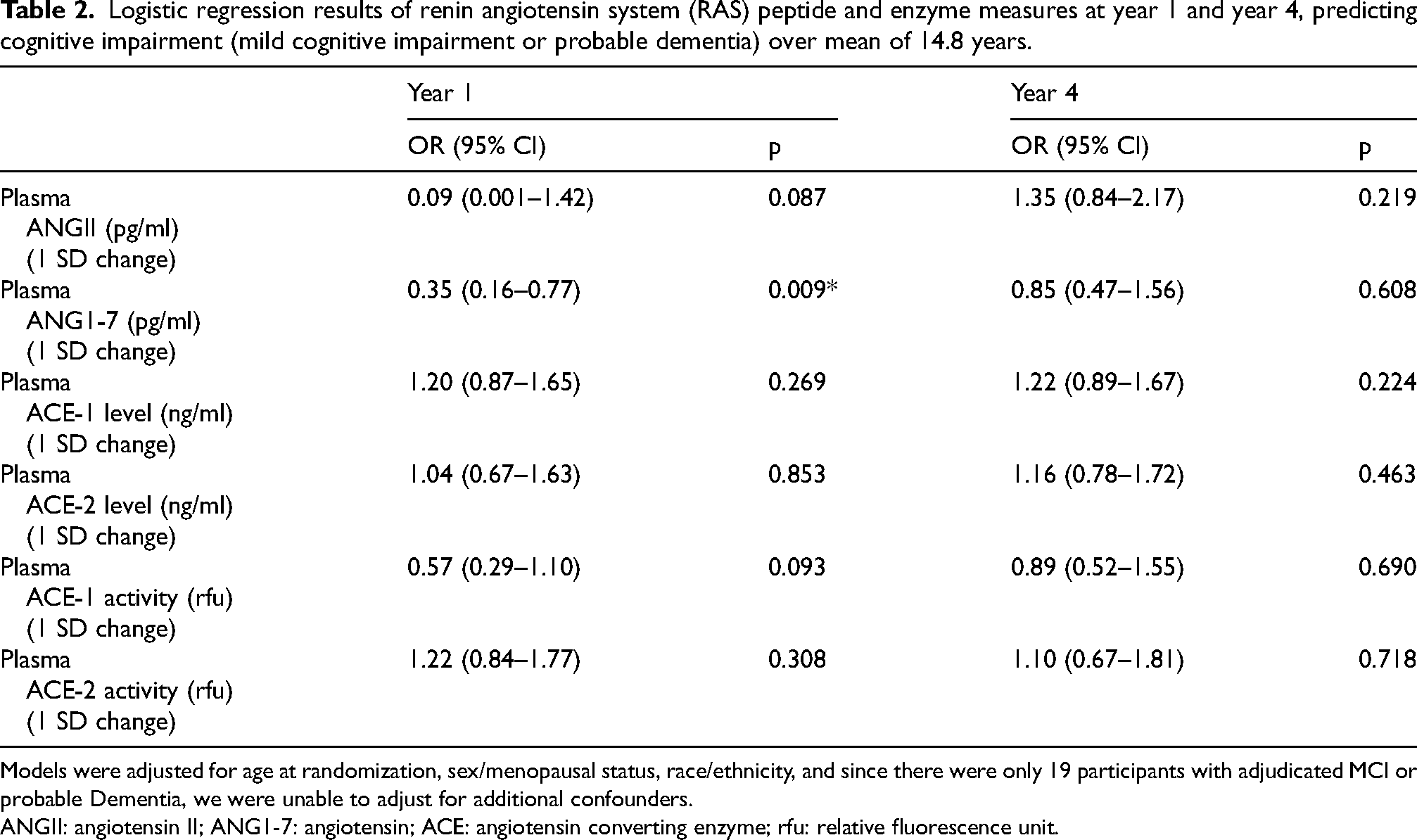
Models were adjusted for age at randomization, sex/menopausal status, race/ethnicity, and since there were only 19 participants with adjudicated MCI or probable Dementia, we were unable to adjust for additional confounders.
ANGII: angiotensin II; ANG1-7: angiotensin; ACE: angiotensin converting enzyme; rfu: relative fluorescence unit.
Association between RAS enzymes and peptides and cognitive function
The cognitive characteristics from n = 310 participants at the first measured visit [means (SD)] 3MSE, TMT part A and part B times (sec), Stroop, DSST, RAVLT immediate and delayed; and composite scores were indicative of a high-functioning cohort (Supplemental Table 7). Participants included in this study performed significantly better than those excluded at the baseline visit on all measures except for the RAVLT delayed (Supplemental Table 8).
Mean levels of ACE-1, ACE-2, and ANGII measured at year 1 and year 4 were not associated with any of the markers of domain-specific cognitive functions (Table 3), an average of 15 years later. Only ANG1-7 measured in year 1 was positively associated with global cognition [β×10−3 = 1.03 (0.50); p = 0.039] (Table 3).
Linear regression results of renin angiotensin system (RAS) peptide and enzyme measures at year 1 and year 4, predicting cognitive function over a mean of 14.8 years.
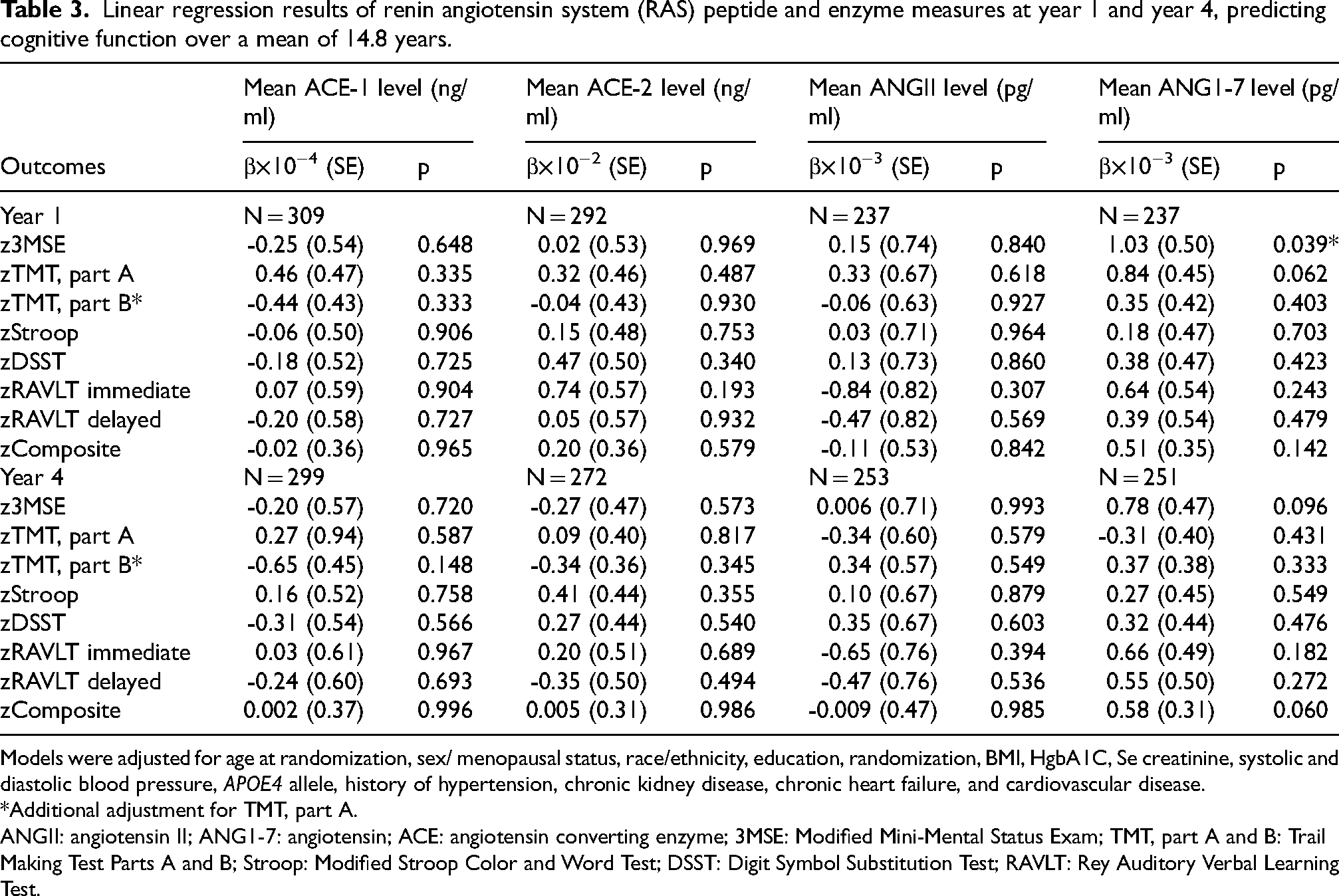
Models were adjusted for age at randomization, sex/ menopausal status, race/ethnicity, education, randomization, BMI, HgbA1C, Se creatinine, systolic and diastolic blood pressure, APOE4 allele, history of hypertension, chronic kidney disease, chronic heart failure, and cardiovascular disease.
*Additional adjustment for TMT, part A.
ANGII: angiotensin II; ANG1-7: angiotensin; ACE: angiotensin converting enzyme; 3MSE: Modified Mini-Mental Status Exam; TMT, part A and B: Trail Making Test Parts A and B; Stroop: Modified Stroop Color and Word Test; DSST: Digit Symbol Substitution Test; RAVLT: Rey Auditory Verbal Learning Test.
In participants who remained cognitively intact (n = 291) (Table 4), a positive association was found between ACE-1 levels measured in years 1 and 4 and global cognition [β×10−4 = 1.28 (0.61); p = 0.037, β×10−4 = 1.36 (0.63); p = 0.033, respectively], and a negative association was found between ANGII measured in year 1 and immediate recall [β×10−3 = -1.54 (0.69); p = 0.027].
Linear regression results of renin angiotensin system (RAS) peptide and enzyme measures at year 1 and year 4, predicting the first measurement of cognitive function in a subset of n = 291 participants who did not develop cognitive impairment over a mean of 14.8 years.
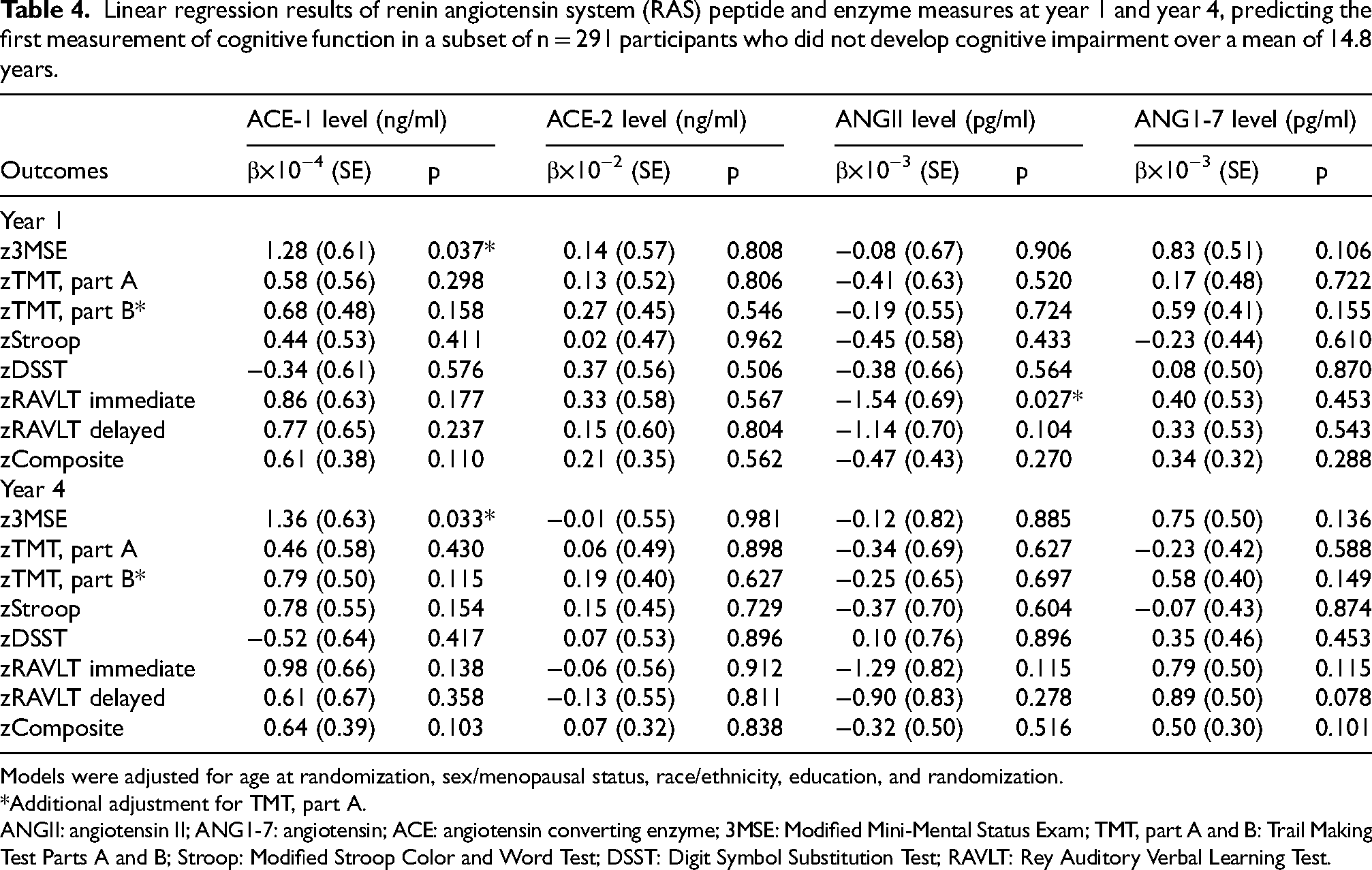
Models were adjusted for age at randomization, sex/menopausal status, race/ethnicity, education, and randomization.
*Additional adjustment for TMT, part A.
ANGII: angiotensin II; ANG1-7: angiotensin; ACE: angiotensin converting enzyme; 3MSE: Modified Mini-Mental Status Exam; TMT, part A and B: Trail Making Test Parts A and B; Stroop: Modified Stroop Color and Word Test; DSST: Digit Symbol Substitution Test; RAVLT: Rey Auditory Verbal Learning Test.
Due to the small number of participants who developed cognitive impairment (n = 19), we did not further investigate the associations between RAS markers and cognitive function.
Discussion
In the present study, we evaluated a subset of participants from the Look AHEAD clinical trial who had a history of diabetes, were overweight or obese, and had no dementia at baseline, to determine the associations between blood RAS enzymes and peptides and cognitive function over a mean of 14.8 years.
We report that a 1 SD increase in circulating ANG1-7 levels was significantly associated with a reduced odds of developing cognitive impairment, 14.8 years later. Interestingly, circulating ACE-1 and ACE-2 levels and activity were not found to be associated with cognitive impairment. In addition, we found no associations between mean levels of ACE-1, ACE-2, ANGII, and ANG1-7 and domain-specific cognitive function in the total cohort, except that ANG1-7 measured at year 1 was associated with better global cognitive function, 14.8 years later. In the subset of participants who remained cognitively intact, we found that ACE-1 levels in years 1 and 4 were associated with better global cognitive function 14.8 years later, while ANGII levels in year 4 were associated with worse immediate recall.
Our study is the first to evaluate associations between ACE-2 or ANG1-7 blood levels and cognitive function in an older adult population without dementia. Additionally, it is the first study to assess associations in a large sample size with extended follow-up.
In a previous study by Yasar et al., 6 the associations between blood levels of ACE-1 and ANGII and cognitive function were investigated in cognitively healthy participants with a high baseline vascular disease burden, with cognition tested 1 year after ACE-1 and ANGII. A significant association was found between higher ACE-1 levels and worse working memory. In the current study of a cognitively normal but high-risk population for cognitive impairment, we found that in participants who later remained cognitively intact, there was an association between higher ACE-1 and better global cognitive function. Higher ACE-1 levels, which are involved in the conversion of angiotensinogen to ANGII, were associated with better global cognition; however, there was no association between ANG II and global cognition. Interestingly, higher ANGII levels were associated with worse immediate memory. These results are consistent with previous findings.
We also report that an increase in ANG1-7 levels was associated with lower odds of cognitive impairment, and that higher levels of ANG1-7 were associated with better global cognitive function.
Previous findings from autopsy studies indicate deregulations in the brain RAS components. MacLachlan et al. 26 recently showed that in patients with AD, ACE-1 activity was positively associated with AD pathology, particularly with Braak stages III-IV, in the temporal lobe. A study by the same group showed that ACE-2 activity was reduced and inversely correlated with parenchymal AD pathology. 6 Another recent small autopsy study by Ismael et al. 39 reported that in patients with AD diagnosis, ANGII was elevated in the hippocampus; however, no changes in levels of ACE-1 or ACE-2 were observed. In addition to autopsy studies, there are only a few studies evaluating changes in circulating RAS in AD. One cross-sectional study showed lower blood ACE-1 levels in AD participants when compared to cognitively unimpaired individuals. 27 Therefore, our study adds new information to the sparse literature.
This study has several advantages. First, our study included a large, well-characterized cohort of at-risk participants who were highly functioning, community-dwelling, and free from cognitive impairment at baseline, underwent rigorous evaluation, and followed for 15 years. These participants underwent a detailed cognitive assessment and provided blood samples, as blood analysis has been less studied to date. Second, the study examined at-risk participants for cognitive impairment, but who were free of cognitive impairment at baseline. Third, the study assessed markers of both the classical and regulatory RAS peptides and enzymes, whereas many earlier studies have focused solely on cRAS components.
The study limitations include the sample size and the fact that only a few participants developed cognitive impairment, which may result in limited power for some RAS measurements in our sample. Additionally, we do not have information on the underlying cause of the cognitive impairment (the type of dementia and mild cognitive impairment), which limits the application of our findings to the AD process. As this study primarily involved non-Hispanic whites, its findings may not be generalizable to other populations. Similarly, this study was conducted on samples from individuals with diabetes who were overweight or obese, which again potentially limits generalizability. However, participants who were included (compared to those excluded) were more likely to have lower weight, lower baseline HbA1c, lower SBP, lower serum creatinine, and lower diabetes medication use, which suggests a healthier population. A potentially healthier population might also explain the relatively small number of incident dementia cases.
In summary, our results provide preliminary evidence that circulating levels of RAS components, particularly ANG1-7 peptide, could be predictive of protection against cognitive impairment and function, and therefore, changes in circulatory RAS may be a helpful proxy marker of early stages of dementia. Further research, particularly follow-up longitudinal studies in larger, independent cohorts, with additional blood, cerebrospinal, and/or imaging biomarkers, is warranted to fully understand the relationship between brain and circulatory RAS and the onset of cognitive decline and disease pathogenesis in AD/ADRD.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261458824 - Supplemental material for Association between renin angiotensin system and cognitive outcomes over 15 years: The Look AHEAD study
Supplemental material, sj-docx-1-alz-10.1177_13872877261458824 for Association between renin angiotensin system and cognitive outcomes over 15 years: The Look AHEAD study by Sevil Yasar, Andrea Anderson, Kathleen M. Hayden, Owen T. Carmichael, Jeanne M. Clark, Michelle C. Carlson, Daniel J. Asby, Patrick G. Kehoe, Scott Miners and Mark A. Espeland in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of the Look AHEAD study participants.
ORCID iDs
Ethical considerations
The study was approved by the Johns Hopkins University Institutional Review Board (IRB) under protocol number #IRB00274756. The requirement for obtaining informed consent was waived as this was a secondary data analysis, and the dataset was anonymized.
Consent to participate
Informed consent to participate has been waived by the IRB because this was a secondary analysis of deidentified data.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by an ancillary study supported by the National Institute on Aging/National Institutes of Health (Grant No. 1R01AG074258). The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health, contributed stored blood samples to this ancillary study.
Two additional diversity supplements funded this research to the Action for Health in Diabetes Extension Study
The Action for Health in Diabetes is supported through the following cooperative agreements from the National Institutes of Health: DK57136, DK57149, DK56990, DK57177, DK57171, DK57151, DK57182, DK57131, DK57002, DK57078, DK57154, DK57178, DK57219, DK57008, DK57135, and DK56992.
The Look AHEAD Brain MRI ancillary study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Department of Health and Human Services: DK092237-01 and DK092237-02S2. The Look AHEAD Movement and Memory ancillary study was supported by the National Institute on Aging, National Institutes of Health, Department of Health and Human Services, R01AG03087-01. R01AG058571 funded the Look AHEAD Mind ancillary study.
The following federal agencies have contributed support: National Institute of Diabetes and Digestive and Kidney Diseases; National Heart, Lung, and Blood Institute; National Institute of Nursing Research; National Center on Minority Health and Health Disparities; Office of Research on Women's Health; the Centers for Disease Control and Prevention; and the Department of Veterans Affairs. This research was supported in part by the Intramural Research Program of the National Institute of Diabetes and Digestive and Kidney Diseases. The Indian Health Service (I.H.S.) provided personnel, medical oversight, and use of facilities. The opinions expressed in this paper are those of the authors and do not necessarily reflect the views of the I.H.S. or other funding sources.
Additional support was received from the University of Pittsburgh General Clinical Research Center (GCRC) (M01RR000056), the Clinical Translational Research Center (CTRC), funded by the Clinical & Translational Science Award (UL1 RR 024153), and NIH grant (DK 046204); Frederic C. Bartter General Clinical Research Center (M01RR01346); and the Wake Forest Alzheimer's Disease Core Center (P30AG049638-01A1).
The following organizations have made significant contributions to Look AHEAD: FedEx Corporation, Health Management Resources, LifeScan, Inc. (a Johnson & Johnson company), OPTIFAST of Nestle HealthCare Nutrition, Inc., Hoffmann-La Roche Inc., Abbott Nutrition, and Slim-Fast Brand of Unilever North America.
This manuscript is based on a subset of the Look AHEAD cohort, excluding participants from the Southwest Native American sites. The complete cohort has been described (The Look AHEAD Research Group. Baseline characteristics of the randomized cohort from the Look AHEAD (Action for Health in Diabetes) research study. Diabetes Vasc Dis Res 2006;3:202-215 NIH Registration: NIHMS81811). The analyses performed herein were not conducted at the Look AHEAD Data Coordinating Center. This does not represent the work of the Look AHEAD study group.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during the current study are stored at the Wake Forest University Coordinating Center of the Look AHEAD Study and are available from the corresponding author or Dr Mark Espeland on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.