
Abstract
Background
Neuropsychiatric symptoms (NPS) affect most individuals with Alzheimer's disease (AD) and are among the most burdensome aspects of the condition, negatively influencing caregivers’ mental health, burden, and quality of care.
Objective
Given the scarcity of studies examining caregivers’ characteristics and NPS simultaneously, this study investigated how sociodemographic and clinical factors relate to different coping strategies, and whether NPS moderate these associations. Path analysis was used to capture direct and conditional effects.
Methods
A cross-sectional study of 176 caregiver–patient dyads assessed coping, burden, mood, and NPS. Path analysis examined the effects of caregiver education, burden, depressive symptoms, and sex on coping, with NPS as a moderator.
Results
Higher education predicted greater use of problem-focused (β = 0.43, p < 0.001) and dysfunctional coping (β = 0.22, p < 0.01). Burden was negatively linked to emotion-focused coping (β = −0.17, p < 0.05). NPS moderated the burden–problem-focused coping link (β = −0.16, p < 0.05).
Conclusions
Education plays a central role in shaping how caregivers cope with care demands. NPS moderated the relationship between caregiver burden and problem-focused coping, with limited influence on other strategies. These findings underscore the importance of considering both caregiver characteristics and patient-related factors when developing interventions, highlighting the need for personalized approaches to improve caregiver well-being and care outcomes.
Introduction
Neuropsychiatric symptoms (NPS) are among the most challenging aspects of Alzheimer's disease (AD), with significant consequences for quality of life and care management. 1 These symptoms include a wide range of disturbances affecting behavior, mood, personality, thought, perception, and basic functions. 2 They are associated with negative outcomes for both individuals with AD and their caregivers, including increased depression and caregiver burden. Caregiver burden is a multidimensional construct encompassing physical, emotional, psychological, social, and financial strain experienced by individuals providing care to patients with chronic and progressive conditions such as AD. 3 The NPS occur in 60–97% of individuals with AD, 4 and apathy and depression are among the most frequently reported manifestations.5–6
NPS are recognized as relevant factors for caregiver burden in AD, but their impact is not uniform.1–2,4–7 Symptoms such as agitation, aggression, and psychosis are often associated with greater stress and depression, whereas other manifestations, such as apathy or sleep disturbances, show less consistent effects across studies.4–7 As discussed in the review by van den Kieboom et al., 8 this heterogeneity likely reflects methodological differences as well as contextual factors such as caregivers’ education, social support, and coping resources.
Due to their high prevalence and persistence, NPS place considerable stress on caregivers. Their presence has been associated with elevated depression and greater difficulty in responding to the needs of the person with AD.9–11 In turn, caregiver burden can be understood as a proximal appraisal of caregiving stress that may influence the selection of coping strategies, consistent with stress and coping models in which perceived demands shape behavioral responses.3,8,10–14 This conceptual link supports the investigation of how caregiver characteristics and patient-related neuropsychiatric burden jointly relate to coping responses.
Coping refers to the cognitive and behavioral efforts used to manage demands perceived as exceeding the caregivers’ resources. These strategies may be adaptive, such as problem-focused coping, which involves solving practical issues, or emotion-focused coping, which includes religious practices, acceptance, and seeking emotional support. 15 In contrast, some caregivers resort to maladaptive strategies, such as denial, avoidance, or self-distraction, which are linked to greater distress and reduced caregiving effectiveness. 16 Recent studies support this distinction, Chen et al. 17 found that caregivers facing NPS often used emotion-focused strategies, while dysfunctional strategies like self-distraction were associated with increased distress. Likewise, Martyr et al. 18 analyzed data from the Improving the Experience of Dementia and Enhancing Active Life (IDEAL) cohort and reported that caregivers with greater resilience, often associated with adaptive coping, showed better psychological outcomes, especially in cases where the person with AD presented fewer neuropsychiatric and functional impairments.
A major limitation of the existing literature lies in the predominance of studies examining direct, bivariate associations, often overlooking moderating mechanisms and broader multivariate patterns that may explain variability in coping. Factors such as caregiver education, burden, depressive symptoms, and the severity of NPS have been examined individually, yet few studies have tested integrative multivariate models capable of capturing direct and conditional effects. In this context, education plays a potentially decisive role in how caregivers of people with dementia employ coping strategies, as it influences access to information, comprehension of medical guidance, and the adoption of more adaptive coping strategies, thereby shaping caregiver burden, anxiety, and depression. Higher educational levels are associated with the use of adaptive strategies and reduced burden, whereas lower levels tend to favor less effective strategies and greater stress in caregiving.3,8–11,15–16
Education represents a fundamental determinant of coping style and caregiver outcomes, with broader and more consistent implications than other sociodemographic factors.15–18 However, it remains unclear how sociodemographic profiles, particularly educational attainment, influence the use of these strategies in the presence of severe NPS, or whether specific coping approaches can buffer the effects of burden on caregivers’ mental health. 19 Furthermore, there is a clear need for models that move beyond identifying coping profiles to explain how and why specific strategies promote, or hinder, psychological adjustment in caregivers. Path analysis offers a comprehensive framework for examining these complex, multivariate relationships. Unlike basic correlation or regression models, it allows the simultaneous testing of direct and conditional effects within a theoretically grounded model. This makes it particularly suitable for research in dementia caregiving, where psychological and contextual variables often interact in intricate ways.
In this context, this study aims to (1) examine the associations between caregivers’ sociodemographic and clinical characteristics, including education, burden, and depressive symptoms, and their use of problem-focused, emotion-focused, and dysfunctional coping strategies; and (2) test whether NPS of people with AD moderate the relationships between these caregiver characteristics and coping strategies.
Based on prior evidence, we formulated the following hypotheses: H1. Higher caregiver education is positively associated with the use of problem-focused coping. H2. Even under higher burden, higher caregiver education is associated with lower use of dysfunctional coping strategies. H3. NPS moderate the association between caregiver burden and problem-focused coping, such that higher NPS strengthen the negative association between burden and problem-focused coping.
Methods
Study design
This is a cross-sectional observational study conducted in a clinical outpatient setting.
Participants
A total of 176 dyads of individuals with AD and their caregivers were consecutively recruited during routine appointments at the AD outpatient clinic of the Institute of Psychiatry, Universidade Federal do Rio de Janeiro, Brazil. People with AD were diagnosed by psychiatrists following DSM-5 criteria. 20 People with mild to moderate AD, who were literate and met the criteria of the Clinical Dementia Rating (CDR) scale21–22 and Mini-Mental State Examination (MMSE) scores ranging from 12 to 26,23–24 were included in the study. Exclusion criteria for people with AD included psychiatric or neurological conditions such as aphasia, head trauma, alcohol abuse, and epilepsy, as specified by DSM-5. 20
For caregivers, inclusion criteria required them to be literate, provide care for the people with AD at least three times per week, and have an MMSE score of ≥ 28. Caregivers with a history of psychiatric or cognitive disorders were excluded based on current or previous assessments and medical records available at the outpatient clinic. All caregivers were over 18 years old, recognized as the main caregiver, and capable of providing detailed information about their family members with AD. Data was collected at a single time point using standardized assessments, ensuring ecological validity and capturing real-world caregiving conditions.
This study was approved by the Ethics Committee of the Institute of Psychiatry at the Federal University of Rio de Janeiro. At the outpatient clinic, all people with AD and their carers sign informed consent forms before the assessment, according to the Declaration of Helsinki. The consent process included a verbal explanation provided by the evaluator and the reading of the informed consent form by both the caregiver and the people with AD. For people with AD, we used simple, accessible language while ensuring that all relevant information was clearly communicated. Participation was voluntary, and their right to refuse was fully respected. When people with AD could not consent on their own, informed consent was obtained from a legal guardian or family member, following local regulations.
Caregiver's measurements
Coping
The Brief COPE Inventory includes 14 coping strategies, each with two items, totaling 28 statements aimed at evaluating the frequency with which individuals utilize various coping strategies in response to stressors.25–26 Participants rated their use of these strategies on a scale from 1 to 4, where 1 indicated “I haven’t been doing this at all” and 4 represented “I’ve been doing this a lot.” These strategies are categorized into three types: problem-focused (active coping, instrumental support, planning), emotion-focused (acceptance, emotional support, humor, positive reframing, religion), and dysfunctional-focused (behavioral disengagement, denial, self-distraction, self-blame, substance use, venting). The responses to each statement were analyzed separately, with higher scores (3 or 4) indicating greater engagement in specific coping strategies, and the result is represented as a profile based on the total score. The scale has broad international validation and the ability to capture a wide range of adaptive and maladaptive coping strategies, making it particularly suitable for examining the complex stressors faced by dementia caregivers. In the assessment of the scale, caregivers were asked to provide situational responses, corresponding to the state version, directly reflecting the strategies applied in the caregiving context.
Sociodemographic information
Caregivers provided sociodemographic information about themselves, including sex, age, education level, and their relationship with the people with AD.
Cognition
The Mini-Mental State Examination (MMSE) comprises 30 items designed to assess various cognitive domains, including orientation, memory, language, and basic motor skills. Scores range from 0 to 30, with lower scores reflecting more severe cognitive impairment.23–24
Burden
The Zarit Burden Interview (ZBI) is a caregiver self-report tool comprising 22 items designed to measure the impact of caregiving on the caregiver's life, focusing on functional and behavioral disabilities of the care recipient. Scores range from 0 to 88, with higher scores indicating greater caregiver burden.13–14
Resilience
The Resilience Scale includes 25 items that measure the ability to adapt positively to adverse life events. It assesses dimensions such as serenity, perseverance, self-confidence, life purpose, and self-sufficiency. Scores range from 25 to 175, with higher scores indicating greater resilience.27–28
Depression
The Beck Depression Inventory is a self-report scale that assesses symptoms of depression, including emotional symptoms such as hopelessness and irritability, cognitive symptoms like guilt, and physical symptoms such as fatigue and weight loss. Scores range from 0 to 63, with higher values indicating greater levels of depression.29–30
Anxiety
The Beck Anxiety Inventory is a brief self-report scale consisting of 21 multiple-choice questions that assess anxiety symptoms. Scores range from 0 to 68, with higher values indicating more severe anxiety.30–31
Caregivers’ perspectives about people with AD
Sociodemographic questions
Caregivers provided sociodemographic information about people with AD, including their sex, age, years of education, and marital status.
Neuropsychiatric symptoms
The Neuropsychiatric Inventory (NPI) evaluates the presence of various NPS, such as aberrant motor activity, agitation, anxiety, apathy, appetite changes, delusions, disinhibition, euphoria, hallucinations, irritability, and nighttime disturbances. Symptoms are rated for frequency (1 = absent, 4 = frequent) and intensity (1 = mild, 3 = severe), with total scores ranging from 0 to 144. Higher scores indicate greater severity of NPS.32–33 In line with the study objective of examining overall neuropsychiatric burden as a contextual factor, the total NPI score was used as an indicator of cumulative behavioral load.
Mood
The Cornell Scale for Depression in Dementia (CSDD) was used to assess mood symptoms, physical signs, circadian rhythms, and behavioral symptoms related to depression in people with AD. A score above 13 indicates the presence of depression.34–35
Severity of dementia
The CDR assesses the severity of dementia, with stages ranging from 0 (no dementia) to 3 (severe dementia), based on the extent of cognitive, behavioral, and activities of daily living (ADL) impairments.21–22
Functionality
The Pfeffer Functional Activities Questionnaire (PFAQ) is a caregiver-reported tool that evaluates people with AD ability to perform ADLs. Items are rated from 0 (normal) to 3 (dependent), with a maximum score of 30, where higher scores indicate more severe functional impairments.36–37
People with AD measurements
Cognition
The MMSE, as previously described, is used to assess various cognitive domains, including orientation, learning, short-term memory, language, and motor skills. The total score ranges from 0 to 30, with lower scores indicating greater cognitive impairment.23–24
Statistical analysis
All analyses were performed by thematic blocks, using SPSS software for Windows version 26.0. The variables were inspected for normality, using Kolmogorov-Smirnov, before analysis. The characteristics of the people with AD and their caregivers were evaluated using descriptive analyses of all variables observing the mean, standard deviation, and frequency (percentage) according to the type of variable studied.
We tested path analysis models in which the scores of the dimensions of the Cope instrument (Emotion, Problem, and Dysfunctional) were regressed onto the variables of caregiver sex, education, depression, and burden. Additionally, we included the total NPI score of the people with AD as a moderating variable to test whether overall neuropsychiatric burden influenced the associations between caregiver-related variables and coping strategies. For the path analysis model, we used the Maximum Likelihood Robust (MLR) estimator, which is robust to deviations from normality in continuous variables. All analyses were conducted in R software, version 4.4.1. Path analysis was performed using the lavaan package, version 0.6–18.
Statistical significance was set at p ≤ 0.05.
The theoretical model to be investigated in path analysis can be better visualized in Figure 1.
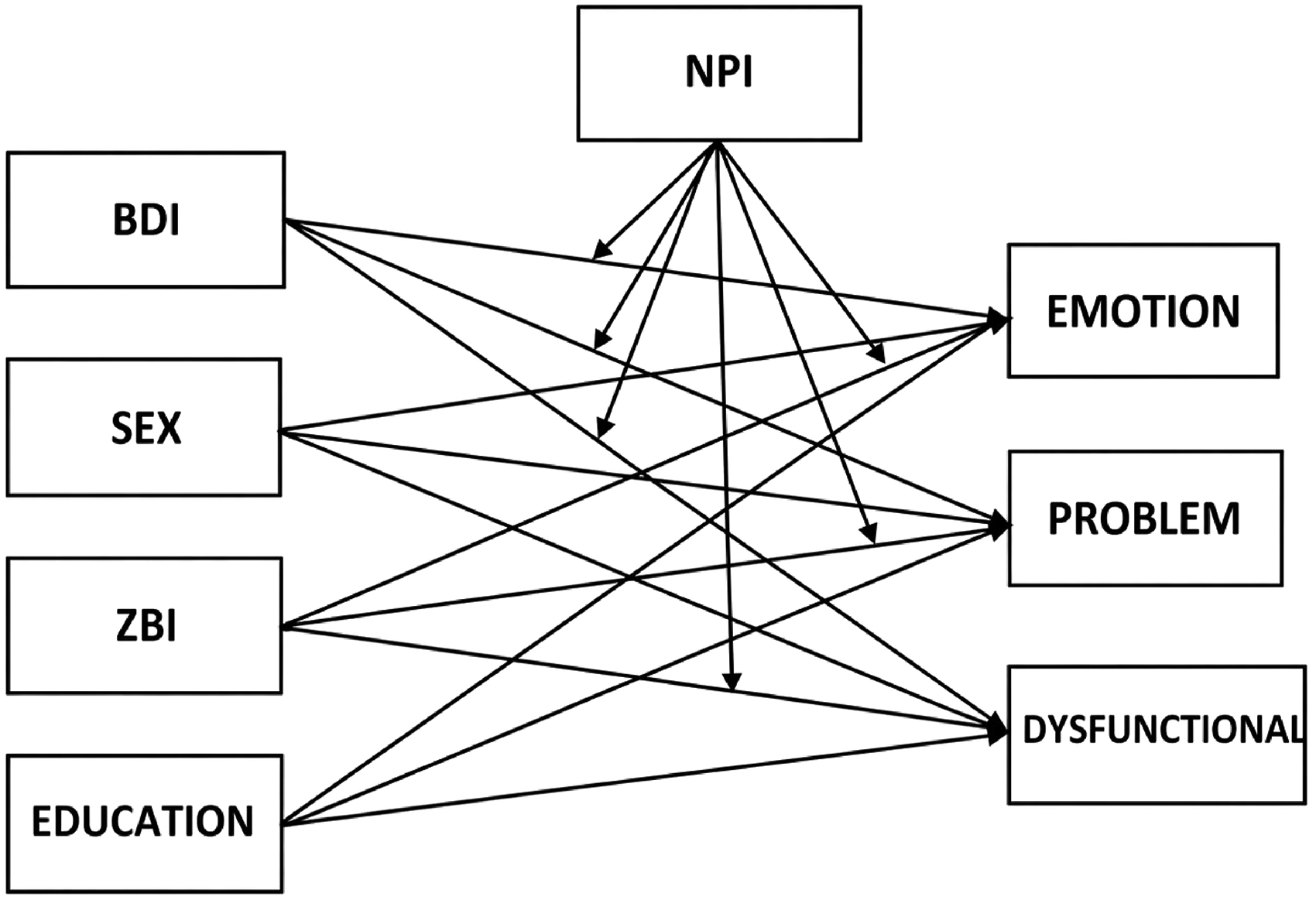
The theoretical model investigated in path analysis.
Results
Sociodemographic and clinical profile of people with AD
The sample comprised a total of 176 participants, with 66 males (37.5%) and 110 females (62.5%), reflecting a higher proportion of females in this cohort. The mean age range of the participants was 75.98 (SD = 9.4), indicating a relatively broad age range. In terms of education, the participants had an average of 8.7 (SD = 4.3) years of schooling. Regarding marital status, most participants are married (43.2%), followed by widowers (31.3%), divorced (16.5%), and single (9.1%). Clinical measures were also evaluated, focusing on cognitive and behavioral indicators. The mean score reflecting cognitive assessment was 17.73 (SD = 6.2), suggesting moderate cognitive impairment. The mean score of 19.10 (SD = 18.6), indicated significant NPS, commonly observed in AD participants. Additionally, the functional ability assessment demonstrated a mean score of 18.4 (SD = 9.02), reflecting a moderate level of impairment in daily activities. The assessment of depressive symptoms revealed a mean score of 8.4 (SD = 6.0), indicating mild depressive symptoms among the participants. Regarding dementia severity, 55.7% of participants were classified at stage 1 (mild dementia), 38.1% at stage 2 (moderate dementia), and 6.3% at stage 3 (severe dementia), suggesting a predominance of mild to moderate stages of AD within this sample. These findings provide a comprehensive overview of the sociodemographic and clinical profile of people with AD, reflecting common patterns in cognitive, functional, and emotional impairments associated with the disease.
The socio-demographic and clinical characteristics of people with AD are summarized in Table 1.
Sociodemographic and clinical characteristics of people with AD (n = 176).
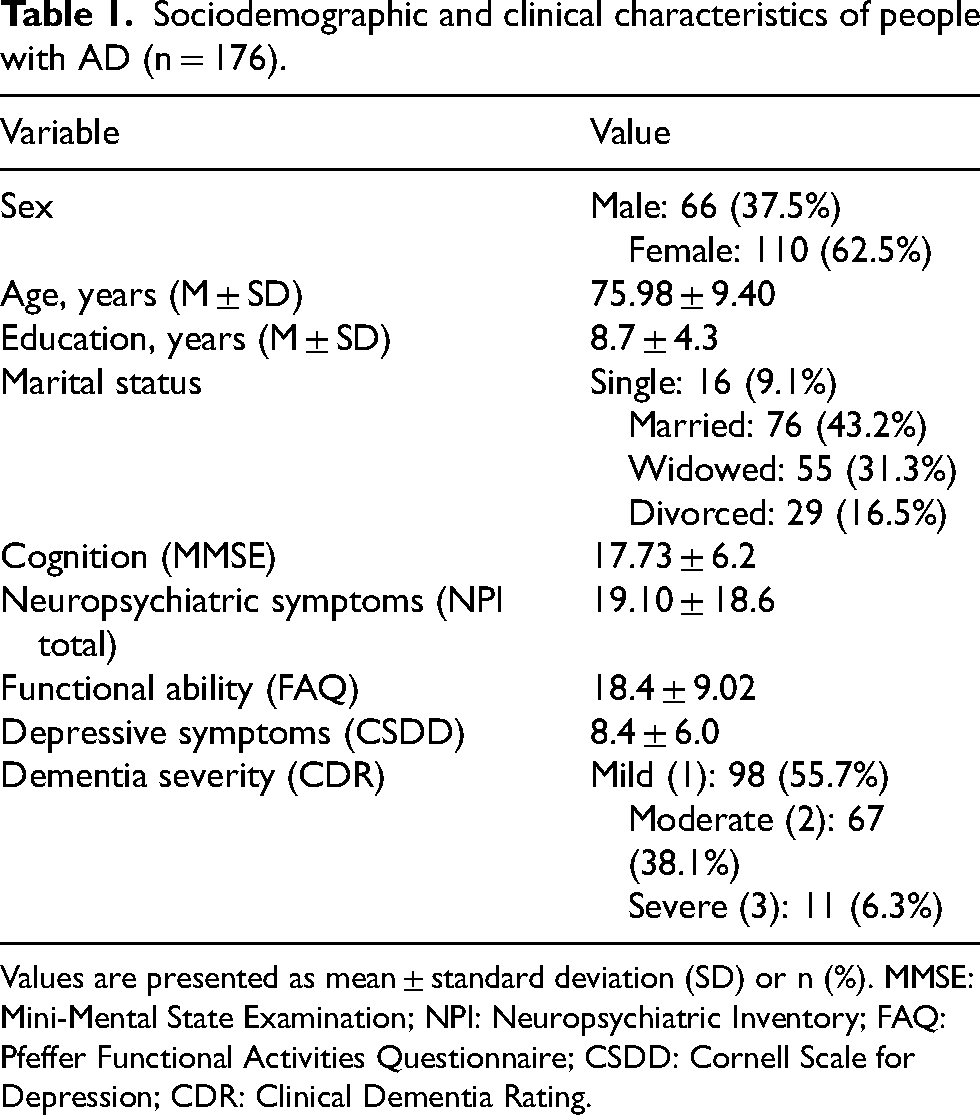
Values are presented as mean ± standard deviation (SD) or n (%). MMSE: Mini-Mental State Examination; NPI: Neuropsychiatric Inventory; FAQ: Pfeffer Functional Activities Questionnaire; CSDD: Cornell Scale for Depression; CDR: Clinical Dementia Rating.
Sociodemographic and clinical characteristics of caregivers
The caregiver sample consists of 176 individuals, with 30 males (17%) and 146 females (83%), indicating a significantly higher proportion of female caregivers. The average age of caregivers was 56.05 years (SD = 13.4), demonstrating a diverse age range within the group. In terms of education, caregivers had an average of 12.05 years of schooling (SD = 3.62), suggesting a generally moderate level of education.
Regarding the relationship with the person with AD, most caregivers were children (49%), followed by partners (35.2%) and siblings (9.1%), with a smaller portion of caregivers having other relationships.
Coping strategies utilized by caregivers yielded an average score of 65.7 (SD = 12.13), indicating a moderate ability to manage caregiving demands. The mean assessment of cognition was 28.34 (SD = 2.08), suggesting that caregivers generally maintained good cognitive health. The caregiver burden showed a mean score of 36.6 (SD = 17.93), reflecting a moderate level of burden. The resilience evaluation demonstrated an average score of 138.37 (SD = 8.35), indicating a moderate to high level of resilience. Anxiety levels among caregivers were mild, with a mean score of 7.8 (SD = 8.35). Similarly, depressive symptoms were mild, with a mean score of 8.85 (SD = 6.86). The differences in the clinical characteristics of caregivers of people with AD are summarized in Table 2.
Sociodemographic and clinical characteristics of caregivers (n = 176).
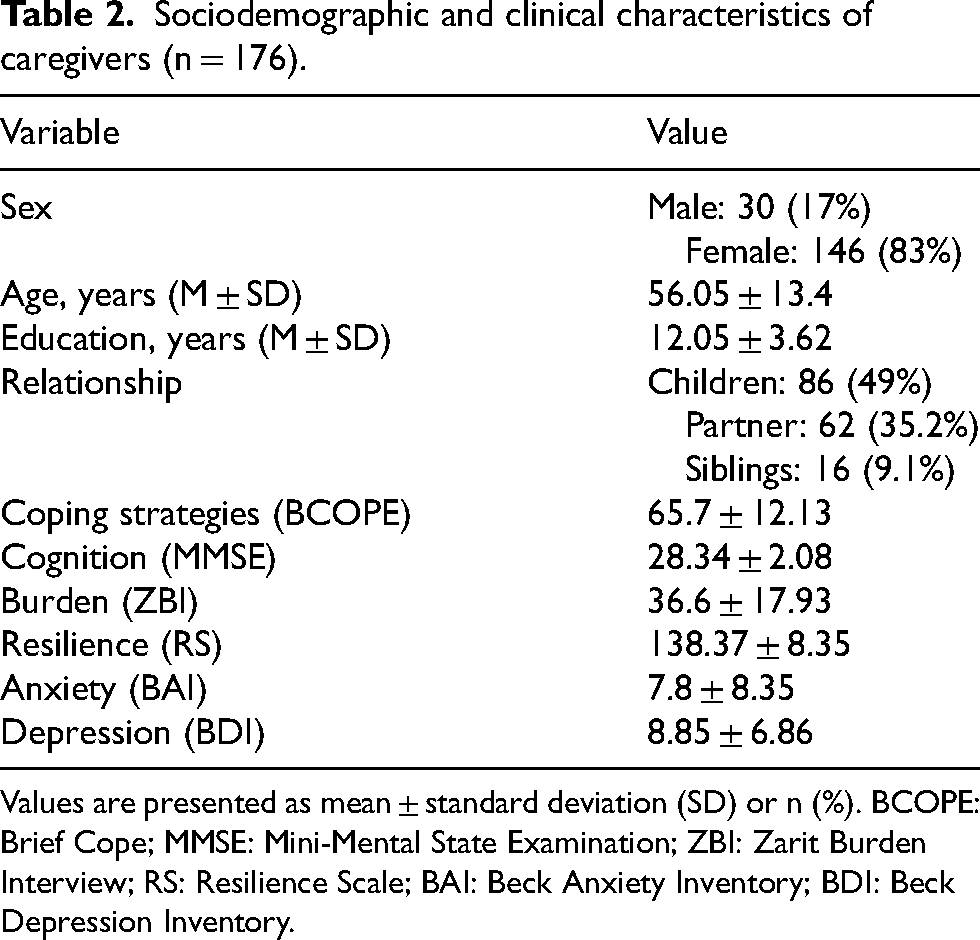
Values are presented as mean ± standard deviation (SD) or n (%). BCOPE: Brief Cope; MMSE: Mini-Mental State Examination; ZBI: Zarit Burden Interview; RS: Resilience Scale; BAI: Beck Anxiety Inventory; BDI: Beck Depression Inventory.
Path analysis with interaction effects predicting the emotion-focused, problem-focused, and dysfunctional coping dimensions
A path analysis model was estimated to examine the relationships between caregiver characteristics and coping dimensions. Emotion-focused, problem-focused, and dysfunctional coping scores from the COPE scale were specified as dependent variables. The total score of the NPI was included as a moderating variable to test whether NPS influenced the associations between caregiver-related variables (education, sex, burden, and depression) and coping strategies.
Interaction effects between NPI scores and caregiver variables were initially tested. However, high multicollinearity was observed between the interaction term (NPI × caregiver sex) and the NPI scores themselves (r = 0.96, p < 0.001). To ensure model stability and avoid biased estimates, this interaction term was excluded from the final model, while the remaining variables were retained according to the theoretical framework of the study.
The analysis revealed significant effects of caregiver education (β = 0.21, p < 0.01) and caregiver burden (β = −0.17, p < 0.05) on the emotion-focused coping dimension. However, NPI scores did not significantly moderate these relationships.
Regarding problem-focused coping, caregiver education had a strong positive effect (β = 0.43, p < 0.001). In addition, a significant interaction effect was found between caregiver burden and the NPI score (β = −0.16, p < 0.05), indicating that the level of NPS moderates the relationship between caregiver burden and the use of problem-focused coping strategies.
The direct association between caregiver burden and problem-focused coping was not statistically significant (β = −0.10, p = 0.10).
Finally, caregiver education was the only variable significantly associated with dysfunctional coping (β = 0.22, p < 0.01). The model estimates are summarized in Table 3.
Path Analysis with interaction effects predicting the scores of the Emotion, Problem, and Dysfunctional coping.
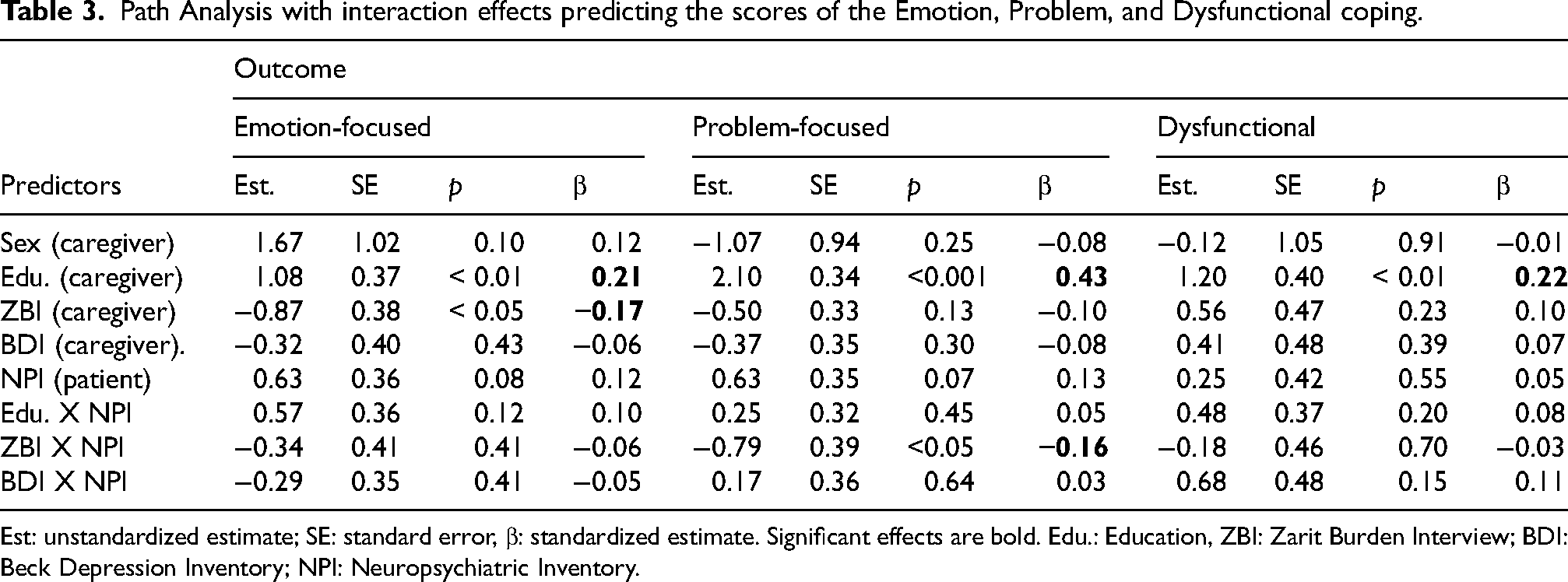
Est: unstandardized estimate; SE: standard error, β: standardized estimate. Significant effects are bold. Edu.: Education, ZBI: Zarit Burden Interview; BDI: Beck Depression Inventory; NPI: Neuropsychiatric Inventory.
Figure 2 illustrates the significant moderation effect observed for problem-focused coping.
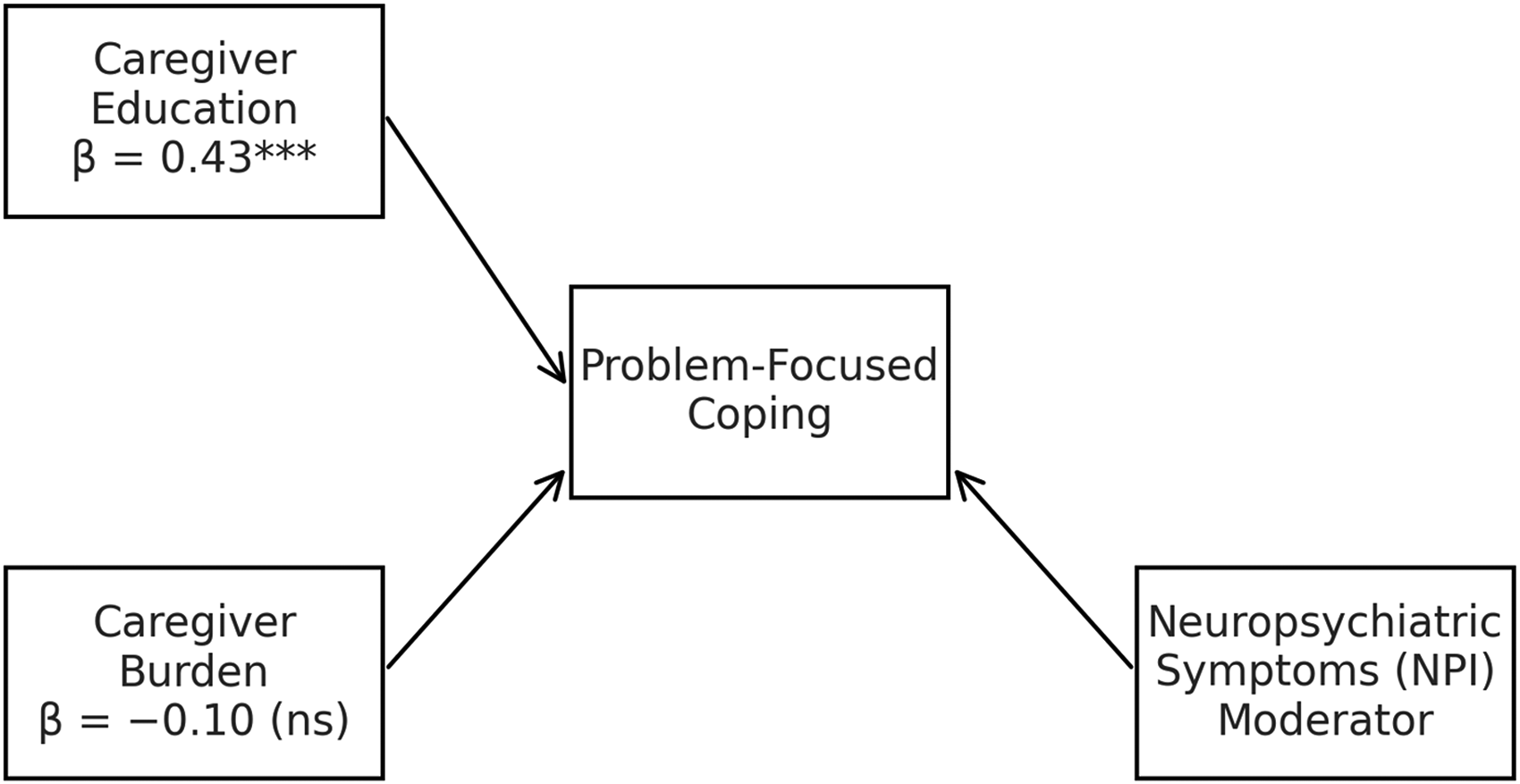
Moderating effect for Problem-focused dimension.
Figure 3 presents the estimated effects for emotion-focused coping.
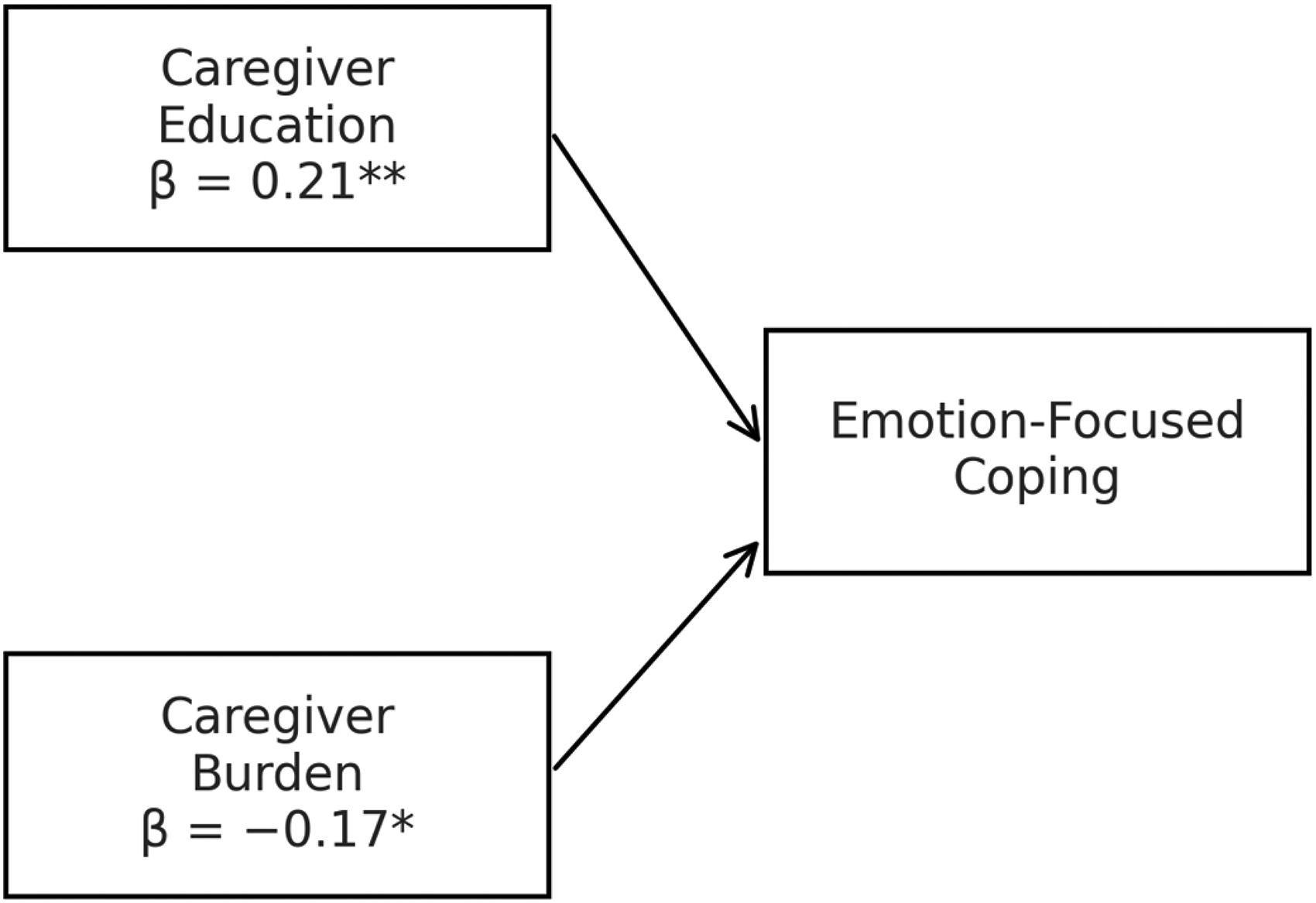
Moderating effects for emotion-focused strategy.
Figure 4 presents the estimated effects for dysfunctional coping.
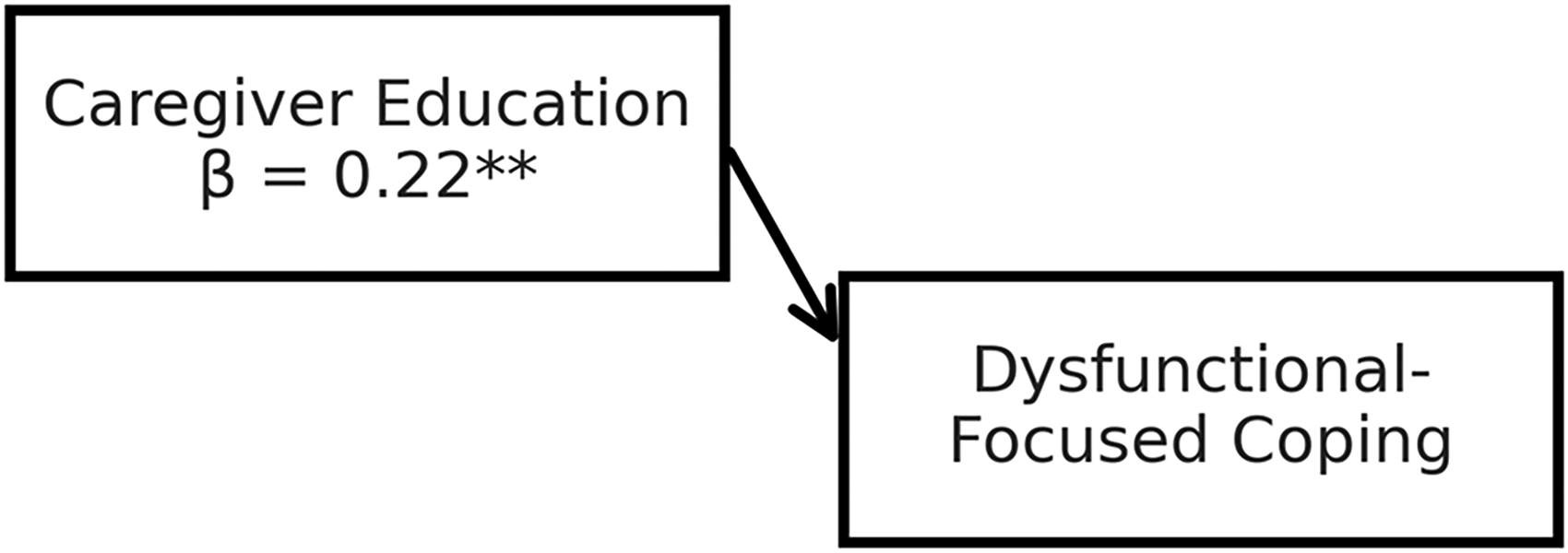
Moderating effects for dysfunctional coping.
Discussion
The present study investigated the relationships between caregivers’ sociodemographic and clinical characteristics and the use of different coping strategies in the context of AD, while also examining whether NPS moderated these associations. Three main findings emerged from the analysis. First, caregiver education was consistently associated with greater use of problem-focused coping strategies. Second, caregiver burden influenced emotion-focused coping and interacted with NPS to shape the use of problem-focused coping. Third, higher education was unexpectedly associated not only with adaptive coping strategies but also with greater use of dysfunctional coping. Together, these findings suggest that coping responses among caregivers are shaped by a complex interplay between caregiver resources, perceived caregiving demands, and the NPS presented by individuals with AD.
The characteristics of the caregiver sample provide important context for interpreting these findings. Caregivers were predominantly women, mostly middle-aged, and frequently children or spouses of individuals with AD, reflecting the well-established family-centered nature of dementia caregiving. This sociodemographic profile is consistent with previous research showing that women often assume the primary caregiving role in chronic neurodegenerative conditions. 38 Although caregivers demonstrated moderate levels of burden and generally mild symptoms of anxiety and depression, the caregiving context remained demanding, particularly given that care recipients presented mild to moderate dementia, reduced functional ability, and depressive symptoms which characterizes a demanding and multifaceted caregiving context. These factors likely contribute to the psychological demands placed on caregivers and may influence the coping strategies mobilized in response to caregiving stress.
Against this clinical background, we examined whether patient-related neuropsychiatric burden altered the relationships between caregiver characteristics and coping strategies. Interactions between NPS and caregiver education, sex, burden, and depression were tested. More specifically, caregiver education and burden were associated with emotion-focused coping, although NPS did not significantly moderate these relationships. The hypothesis that using the total NPI score may conceal the impact of specific dimensions on emotion-focused coping is rooted in the complexity of caregiver burden. 39 While the total score aggregates various NPS, it may mask the distinct effects that individual dimensions, such as agitation, depression, or apathy, can have on emotional resilience and coping mechanisms. These dimensions could interact differently with caregivers’ stress levels or coping strategies, either amplifying or mitigating their burden. For instance, dimensions like aggression might exacerbate emotional strain, while apathy could lead to feelings of detachment and reduced engagement. 40 In addition, the presence of mild-to-moderate depressive symptoms among care recipients, as measured by the CSDD, may further contribute to emotional strain. Depressive features such as apathy, withdrawal, and reduced initiative can subtly alter relational dynamics, potentially increasing caregivers’ feelings of helplessness and influencing their coping responses. This broader interpretation may help explain why the overall NPI score did not emerge as a significant moderator for emotion-focused coping.
Within this broader literature, Delfino et al. 41 used path analysis to explore the links between caregiver characteristics and NPS in AD participants. They found a direct relationship between NPS, caregiver burden, and the use of criticism management strategies. Additionally, caregiver burden and criticism management strategies influenced these symptoms indirectly, with caregiver burden acting as a mediating factor. While both studies emphasize the central role of caregiver burden in shaping coping responses, our findings diverge from those of Delfino et al. 41 regarding the role of NPS. In our model, NPS did not moderate the relationship between caregiver factors and emotion-focused or dysfunctional coping strategies, suggesting that other variables may mediate or moderate this complex interaction.
Conversely, the interaction analysis revealed that the NPS moderated the relationship between caregiver burden and problem-focused coping. Interestingly, under higher levels of NPS, greater burden was associated with fewer reported problem-focused strategies, suggesting that in highly demanding care contexts, the use of active coping may be inhibited. Given that most care recipients were in the mild to moderate stages of dementia, problem-focused coping may still be perceived as viable under lower neuropsychiatric burden. However, as symptom severity increases, particularly in more functionally impaired individuals, caregivers may experience diminished perceived controllability, limiting the use of active coping strategies. In contrast, when NPI levels were lower, the association between burden and problem-focused coping was negligible. Our findings are in line with González-Fraile's 15 study, which demonstrated the greater effectiveness of problem-focused coping in caregivers of people with moderate dementia, while emotional coping was more suitable for those dealing with mild dementia.
Consistent with our first hypothesis, higher caregiver education was positively associated with greater use of problem-focused coping. This finding aligns with previous research suggesting that education may enhance access to knowledge, problem-solving skills, and health literacy, thereby enabling caregivers to mobilize more adaptive responses when facing caregiving demands.15,42 Education may also facilitate the interpretation of behavioral changes in the person with AD, reducing uncertainty and enabling more structured coping strategies. Our findings align with Balasubramanian et al., 43 who describe coping as a complex process shaped by the appraisal of stressors and by the resources available to the caregiver. Taken together, these findings reinforce caregiver education as a consistent correlate across the coping dimensions examined in this study.
Unexpectedly, however, higher education was also associated with greater use of dysfunctional coping, contradicting our second hypothesis. There are several potential explanations. More educated caregivers may exhibit higher self-expectations and greater awareness of caregiving inadequacies, which could translate into increased self-blame or self-criticism—key components of dysfunctional coping subscales. 16 Alternatively, education may not uniformly protect against stress; highly educated caregivers may experience greater role conflict or perceive caregiving as more disruptive to personal or professional goals. These possibilities highlight the importance of examining coping not as a linear continuum but as a multidimensional configuration that may vary across educational or sociocultural contexts.
Taken together, the results suggest that coping in the context of AD caregiving cannot be understood solely through direct associations. Instead, multivariate patterns highlight the interplay between caregiver resources (e.g., education), stressors (e.g., burden, NPS), and psychological responses. The moderation effect identified supports contemporary models of coping flexibility, which posits that the effectiveness of a coping strategy depends on alignment between perceived controllability of stressors and strategy type 39 ]. Under high NPS severity, caregivers may perceive situations as less controllable, making problem-focused strategies less viable.
Strengths and limitations
The sample of 176 participants, predominantly women (83%) and family caregivers (49% being children), may not fully represent all caregiver populations, limiting the generalizability of the findings. Important contextual factors such as social support, caregiving experience, cultural background, and financial resources were not analyzed, even though economic conditions may be correlated with educational attainment and access to formal assistance. Likewise, we did not examine whether caregiver age and education were correlated in this sample, which may partly influence the interpretation of education-related effects. The models also did not adjust for potentially relevant covariates such as caregiver age, sex, or severity of cognitive impairment in the person with AD; in particular, including a direct indicator of cognitive severity alongside NPS may help disentangle distinct clinical contributions in future studies. Self-reported data from caregivers and people with AD may have introduced bias, as some participants might have exaggerated or minimized challenges, affecting the accuracy of the results. Since this is a cross-sectional study, it provides only a snapshot of associations and cannot establish cause-and-effect relationships. Longitudinal studies are needed to better understand how caregiver and patient characteristics influence coping strategies over time. Key clinical factors, such as comorbidities and treatments, were not considered, which could impact the severity of symptoms and, consequently, coping strategies. The study also did not address geographical and cultural diversity among caregivers, reducing its ability to reflect a broad range of caregiving experiences. While NPS were examined, their categorization lacked sufficient detail, which may have diminished the precision of the findings. These limitations highlight areas for future research to improve interventions and provide better support for caregivers of people with AD.
Clinically, our findings have important implications for caregiver support programs. The consistent association between caregivers’ level of education and coping patterns suggests that educational attainment may shape how caregivers interpret and manage care demands. Interventions that aim to promote coping efficacy should therefore consider integrating educational components, such as caregivers training programs focused on emotional regulation, problem-solving, and disease management. Moreover, considering that caregivers with lower education levels may be more vulnerable to maladaptive coping, targeted interventions that are culturally appropriate and accessible regardless of formal education level become especially important. Psychoeducational approaches, peer support, and simplified resource materials may help bridge this gap and empower a broader range of caregivers.
Conclusion
In conclusion, this study underscores the role of caregivers’ educational level in shaping coping patterns, particularly in the emotion-focused and problem-focused dimensions, while also revealing an unexpected positive association with dysfunctional coping. Although NPS moderated the relationship between caregiver burden and problem-focused coping, their influence on the other coping dimensions was limited. These findings emphasize the importance of considering both caregiver characteristics and patient-related factors when designing interventions aimed at improving caregivers’ well-being. Additionally, the moderating effect of NPS on caregivers’ burden, particularly in more severe cases, offers important insights for tailoring support strategies. Ultimately, this study contributes to the growing body of research advocating for the incorporation of caregiver education and a personalized approach to managing NPS to enhance the overall caregiving experience and improve patient outcomes. Future research should continue to explore these dynamics, particularly in larger and more diverse caregiver samples, to further inform effective caregiving interventions.
Footnotes
Acknowledgements
The authors acknowledge the financial support provided by Brazilian funding agencies: Alexandre Magno Frota Monteiro received support from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES); Marcela Moreira Lima Nogueira and Tatiana Belfort Almeida dos Santos received support from the Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ); and Márcia Cristina Nascimento Dourado is a Researcher of the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and also received support from FAPERJ.
Ethical considerations
This study was approved by the Ethics Committee of the Institute of Psychiatry at the Federal University of Rio de Janeiro and was conducted in accordance with the Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from all caregivers and from the people with AD or, when applicable, from their legal guardians/family representatives.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received support from CAPES, FAPERJ, and CNPq, as detailed in the Acknowledgments section.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Marcia Cristina Nascimento Dourado is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.