
Abstract
Background
Newly diagnosed people with dementia and Alzheimer's disease may have varying levels of functional difficulties in which help is required. Little is known about how their needs are met, the associations of needs with care dyad background characteristics and how these characteristics are associated with each other.
Objective
We investigated the pathways between background characteristics, functional difficulties (need) and receipt of help.
Methods
The sample included 672 newly diagnosed people with dementia and their carers. Four activities of daily living (ADLs), three instrumental activities of daily living (IADLs) and receipt of help in these activities were used to define needs and unmet needs. Receipt of adequate support from health and social care services was also reported. Regression and path models explored the associations with background characteristics.
Results
Most people with dementia had at least one ADL (42%) or IADL (83%) difficulty. Among those who had a difficulty, 50% and 31% had at least one unmet ADL or IADL need, respectively. Support from health and social care services was reported as inadequate by 29%. Many background characteristics (age, gender, education, homeownership, urban-rural location, area deprivation) were associated with receipt of help through functional limitations and/or whether the carer was spouse or coresident.
Conclusions
Although people newly diagnosed with dementia had fewer ADL than IADL difficulties, unmet need was proportionally higher for ADLs than IADLs. The findings point to possible barriers to receiving help shaped by complex pathways through sociodemographic factors, current levels of functioning and carer characteristics.
Keywords
Introduction
People with dementia often experience care needs arising from difficulties managing daily life due to the condition. 1 Need for help with tasks related to memory, household chores and handling finances is often high. 2 Support which is needed is not always available resulting in unmet need or perceived inadequacy of support. The recent World Health Organization's global action plan for dementia 2017–2025 calls for addressing the wide divide between the needs and meeting the needs in people with dementia during the long-term care pathways. 3 The level and type of need and whether it is met may vary, depending on the progression of the disease, other health problems, and characteristics of the person with dementia and those caring for them.2,4,5 Because of the heterogeneity of studies (e.g., who had been studied, what factors have been taken into account and how they have been included in the models), the results show a mixed picture. In people newly diagnosed with dementia, little is known about how functional needs are met and shaped by the characteristics of the care dyads. The current study used path modeling to investigate the functional needs, how they are met, and how meeting those needs varies with the background of people newly diagnosed with dementia and their carers.
People with dementia often exhibit more need for help with instrumental activities of daily living (IADLs), such as household work, shopping and managing finances than in “basic” activities of daily living (ADLs), such as dressing, bathing, eating and using the toilet.6–10 This has been found in studies conducted in Western countries and including people at various stages of dementia. Previous research also shows that these needs are often not met in a consistent and timely way which may lead to unmet need and perceived inadequacy of support.6,7,9–12 Several reasons may contribute to this: the carer or person with dementia may not recognize the need, the person with dementia may refuse care, or the care provided is not of the quality or quantity required due to problems with communication, decreased ability to care for oneself and ineffective use of resources. 13 In addition to personal psychological and interpersonal barriers, there can be also lack of access to unpaid or formal care support because of situational (such as economic and functional barriers), structural (such as lack of information, awareness and provision of services) and cultural barriers (such as language, cultural stigma, faiths and belief systems). 14
To understand why unmet needs occur, the first step is to investigate the characteristics of the people with dementia and their immediate living environment. Andersen's behavioral model of health services use has grouped the characteristics associated with unmet needs to predisposing factors (e.g., gender, age, ethnicity), enabling factors (e.g., socioeconomic characteristics, having a carer/partner), and need for care factors (e.g., functional limitations, poor health). 15 Previous research has reported the associations of these factors with unmet need and inequalities in receiving help among people with dementia. The findings are however not conclusive, as we describe below (see also the description of the past studies in Supplemental Material 1).
The role of predisposing factors such as age, gender and ethnicity is not clear: they have not been found to be associated with unmet need in all studies, and when they have, the results are mixed. For instance, some studies have found more unmet need in men16,17 while some others in women18,19 with dementia. Similarly, in terms of age, some studies have found higher age of the person with dementia is associated with unmet need10,16 and faster increases in functional unmet needs, 19 while lower age has also been reported to be associated with unmet need. 20 Unmet need was also found to be associated with male gender 17 and younger age of carer.9,21 Ethnicity as a predictor of unmet need has been rarely included in the previous studies. Some studies have reported minority ethnicity being associated with unmet need.17,20,22 Ethnicity was sometimes described but not used in the model, 21 probably due to small sample size.
One of the most consistent findings in how well needs are met is related to enabling factors, such as socioeconomic status and availability of social support in the household. Several studies have reported associations between unmet need and lower socioeconomic status (lower levels of education, income, or wealth, not being homeowner, receipt of benefits, geographic area) of the person with dementia6,17,19,20,22–24 and carer's lower level of education.20,24 Some studies also show initial associations of several socioeconomic variables with unmet need of which only one or none eventually are significant,19,20,25 suggesting possible mediation through the correlated socioeconomic characteristics. For instance, higher educational level attained in early adulthood is often associated with later adulthood income and wealth but if these paths are not taken into account, only some of the correlated predictors turn out significant in the multivariable regression model.
Many studies show that the presence of spouse carer or not living alone is associated with how well needs are met.9,19–21,26,27 Better health status of the carer can also enable these needs to be met.9,17,28 However, in some studies these factors were not significant in the multivariable regression modeling,20,21 suggesting that there may be pathways between several enabling (and other) factors entered in the model.
The previous work on the role of need for care factors (often measured as functional limitations, severity of dementia and poorer health of person with dementia) show a complex picture. Some studies have reported more unmet need in those with milder functional impairments20,22 and in early stages of dementia, 5 while some reported more unmet need in those with higher levels of ADLs 29 and poorer health status. 24 The results reported within a study have been mixed: One study reported that a greater level of disability was associated with more unmet ADL needs, whereas for unmet IADL needs the pattern was the opposite showing fewer unmet IADL needs in those with more disability. 7 Another study reported higher unmet physical needs among people with dementia who had more severe functional impairment. 24 However, they also found unmet physical needs to be associated with milder cognitive impairment. Some studies have found either higher 9 or lower 20 dependency associated with higher unmet need, but this association disappeared when other characteristics were included in the model. The level of functional limitations has also been identified as an important mediator between sociodemographic and -economic characteristics and change in unmet need over four years in people with dementia. 19 Altogether, the studies point to the importance of exploring the pathways through need factors and separating the type of (unmet) need.
Past studies have rarely used path modeling. We are aware of two studies in England: one using longitudinal data focused on level and change of unmet need over four years 19 and another using cross-sectional data studied pathways to the outcomes of unmet need. 21 Both studies suggested mediation between the background characteristics (predisposing factors, enabling and need factors) but the included characteristics in the models were limited. Most previous studies have used multivariable regression models to identify factors that are associated with unmet need. In some studies, the initial associations of unmet need with background factors before multivariable modeling are mostly not significant.18,29 This may suggest that the studies use different definitions of unmet need and receipt of help 30 or there are differences in sample characteristics due to location and data collection. Different stages of disease also exhibit different needs: there may be variation by the type and stage of dementia between the studies, e.g., whether looking at early-onset dementia, newly diagnosed people living at home or those with severe dementia in institutions. Some studies find initial associations, but these associations disappear when more factors are adjusted in the stepwise models,17,20,31 suggesting possible presence of pathways (mediation) between factors. There may be cumulative influences of prior life circumstances on later-life health status, 32 and consequently on needs and receipt of help. When the time sequence of events, i.e., possible mediation in the pathways between the variables, is not been taken account, some potential predictors may turn out to be statistically significant and others not significant, although they may all be associated with the outcome in a chained pathway through mediation.
It is also important to consider the care dyad's characteristics, 28 as both the person with dementia and their carer contribute factors that enable or challenge the receipt of help and meeting needs. The care environment is shaped by the relationship between person with dementia and carer and various sociodemographic and socioeconomic characteristics of the household. Some studies have looked at the characteristics of the person with dementia and their carer.17,21,31 However, these and other studies, which have included various background factors from person with dementia only,6,16,18,20–22,24,25,29 have not investigated the pathways between the background characteristics, functional limitations, and receipt of help. To our knowledge, none have focused on people newly diagnosed with dementia.
Understanding of social care arrangements or lack of support after dementia diagnoses is important for the planning of personalized and integrated care. Early diagnosis makes possible early interventions 33 such as sufficient and timely care and support. Unmet need has been found to be associated with poorer general well-being and quality of life in cross-sectional studies,6,20,21,34–36 and faster functional decline 19 and need for institutional care 37 in longitudinal studies. Therefore, to support people to live well with dementia, it is important to identify the needs and possible pathways to meeting these needs early in the dementia pathway.
This study aims to investigate the level of functional difficulties (need), the extent of unmet needs and perceived inadequacy of support among people newly diagnosed with dementia and the role of sociodemographic characteristics of the person with dementia and their carer in the level of needs, receipt of help and unmet need.
Methods
Sample
We used a sample of 672 dyads of people with dementia and their carers who participated in the DETERMIND study. 38 People with dementia and their carers were recruited predominantly from Memory Assessment Services across three geographical and socially diverse areas of England (North-East, South London, and South-East). The people with dementia were newly diagnosed, within six months of their diagnosis, and had their baseline interview between March 2021 and March 2023.
Capacity to provide informed consent was assessed during a face-to-face consultation by a trained research assistant and a Personal Consultee was sought for those people with dementia who lacked capacity. Consent for the inclusion of a carer was sought from people with dementia with capacity and, for those people without capacity, consent was sought from the Personal Consultee. Questionnaire data were collected predominantly through face-to-face interviews with research assistants and typically lasted around two and a half hours at baseline. Ethics approvals were granted by the Health Research Authority Brighton and Sussex Research Ethics Committee (REC 19/LO/0528. IRAS 261263).
Measures
Functional limitations
Carer-reported functional difficulties were measured using the Bristol Activities of Daily Living Scale, 39 which was developed to assess activities of daily living in people with mild dementia living in the community. 40 The scale has 20 items each measured on a 4-point scale from 0 (no difficulties) to 3 (severe difficulties). The total score across 20 items of the BADL scale was calculated (range 0–60) to measure the overall level of functional limitations. The internal consistency of the score was good (Cronbach's alpha = 0.91).
Unmet ADL and IADL need
Unmet need was based on carer-reported functional limitations of the person with dementia for which no help was received. Four items for activities of daily living (ADLs; difficulty with eating, dressing, bathing/showering, using toilet) and three items for instrumental activities of daily living (IADLs; difficulty with housework, shopping, doing finances) were used to measure need, see Supplemental Table 1. If the person with dementia was reported to have a mild, moderate or severe difficulty conducting any of these activities but did not receive help for that activity, the item was coded as an unmet need (0 = received help for the respective need, 1 = did not receive help for the respective activity). 8 As seen in Supplemental Table 2, the count of unmet ADL and IADL needs was highly skewed. Therefore, binary variables for unmet ADL and unmet IADL needs were created when at least one unmet ADL or IADL item was identified. In terms of the final models, we carried out a sensitivity analysis using the count of unmet ADL and IADL need as the outcome. We also ran a model with three study sites as covariates to study the effect of the location.
Perceived inadequacy of support was a single, binary item asking the carer whether the person with dementia is receiving adequate support from the health and social services (0 = yes, 1 = no).
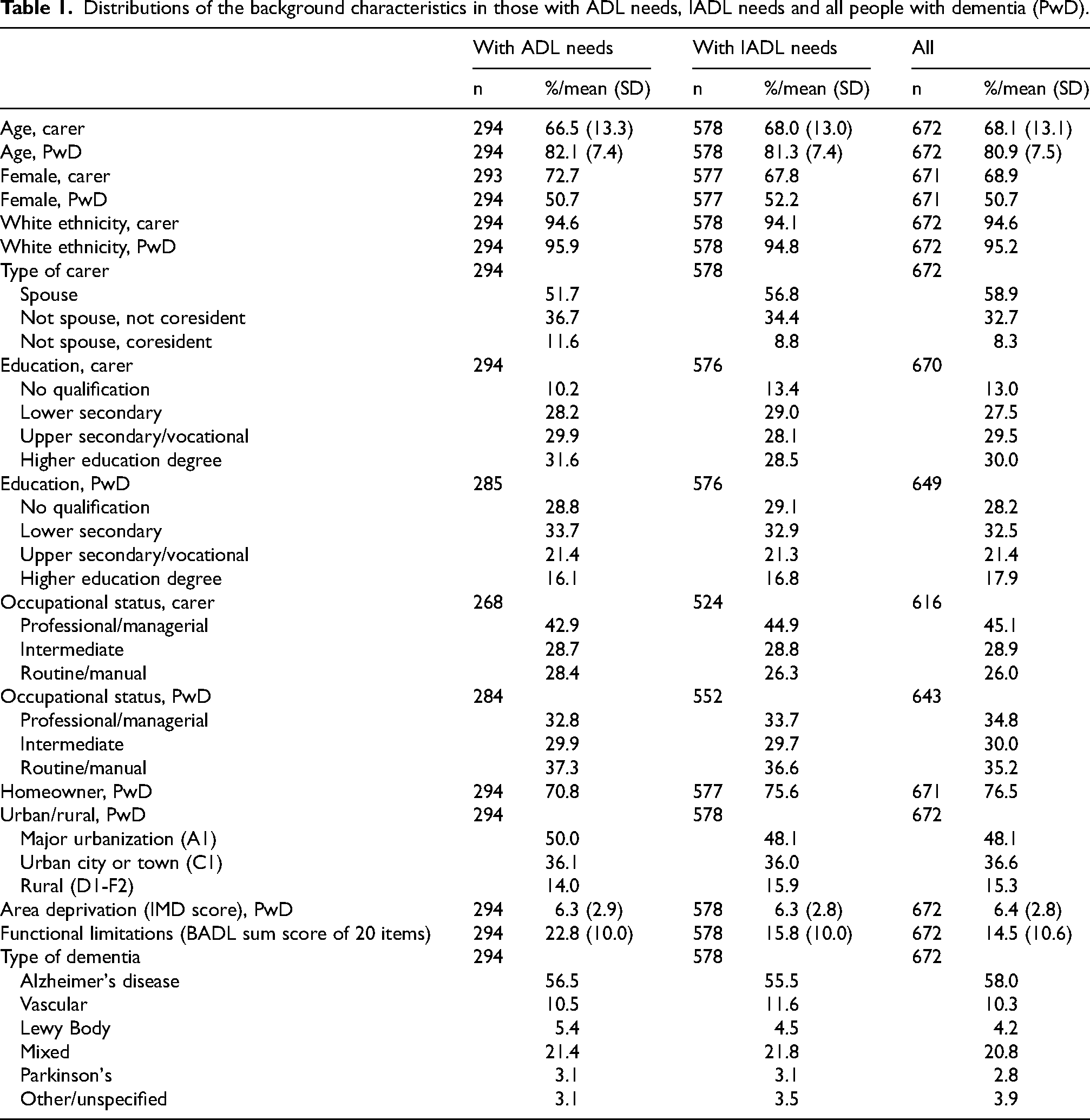
Several sociodemographic characteristics are known to be associated with receipt of help and unmet need among people with dementia and/or carers.19,20,25 Consequently, variables collected and incorporated within our analysis include: age, gender, ethnicity, education (level of qualifications attained) and occupational class based on the National Statistics Socio-economic Classification (NS-SEC) with three categories (higher managerial, administrative and professional or intermediate occupations; and routine and manual occupations 41 of the person with dementia and carer); home ownership (a binary measure, those owning their home outright or with a mortgage or shared-ownership, and those renting, living rent free, or squatting), urban-rural classification of postcode area 42 and deciles of the Index of Multiple Deprivation (IMD; range 1–10 where a lower decile indicates more deprivation) based on postcodes 43 for the person with dementia; and whether carer was spouse, not spouse and coresident, or not spouse and not coresident. Type of dementia was also controlled in the models. See the categories for the background characteristics in Table 1.
Distributions of the background characteristics in those with ADL needs, IADL needs and all people with dementia (PwD).
Analysis
Following descriptive analysis, logistic regression models were used to study the associations of unmet need and inadequacy of support with the background characteristics: gender, age, ethnicity, education and occupational status of the person with dementia and the carer; homeownership, area deprivation, urban-rural location and level of functional difficulties of the person with dementia; relationship of carer to person with dementia; and type of dementia. The correlations between the background factors were investigated to see whether associations between the factors may suggest mediation (Supplemental Table 3). A potential mediator is associated with both the primary exposure and the outcome and can be placed in the pathway between the primary exposure and the outcome. Factors associated with outcomes in bivariate models (p < 0.10) were further analyzed in a multivariable logistic regression.
We used structural equation modeling to examine the associations between the background characteristics and outcomes. A path model was built that included the variables correlated with the outcome. Path models enable investigation of mediation—the mechanisms that link the predictors to unmet need through indirect and direct associations. For assessing mediation, the contributing factors need to be organized in a sensible order. Although the current data were collected at one datapoint (baseline), it is possible to organize the factors in a timely order representing the pathways of lifetime circumstances. 32 For instance, demographic factors (date of birth, sex) are determined before socioeconomic factors in early adulthood (education), later adulthood (occupational status, homeownership, area characteristics) and current circumstances (functional limitations, relationship with carer). The associations between the background variables were organized in a timewise order (Supplemental Figure 1).
Analyses were carried out using Mplus 8. 44 The sociodemographic and other background variables were included as potential predictors of unmet need and the associations between the variables were added to the model if they were significant (p < 0.05). Paths that were not significant (p ≥ 0.05) were dropped from the model. Indirect effects were standardized to make it easier to compare the effect sizes. 45 Bootstrapping was used to calculate the bias-corrected 95 percent confidence intervals for the standardized indirect effects. 46
The fit of the model was assessed using chi-square analysis, but, because this index is sensitive to sample size, we also used the Comparative Fit Index (CFI) and Root Mean Square Error of approximation (RMSEA) as recommended by Hu and Bentler 47 and Kline. 48 A value at or below 0.08 for the RMSEA and SRMR and at or above 0.90 for the CFI was considered to indicate an adequate fit for the model. The weighted least squares means and variance (WLSMV) adjusted estimator with theta method was used, since it is suitable for categorical outcomes. 49 The associations for educational and occupational status and urban-rural location, variables which have more than two categories, appeared to be linear and were used as ordered categorical variables in the path analyses. Variable types used in the analysis are shown in Supplemental Table 4.
Missing data were handled using the full information maximum likelihood method (FIML). 50 This method makes it possible to estimate the likelihood function for all cases based on the information on the means and variances of the variables that are present in the dataset (see Table 1 for numbers in each background variable). Missingness was low (<5%) in all variables, except for carer's occupational status where 8% were missing. The current analysis uses only those dyads where functional limitations (need) of the person with dementia was available (n = 672). This excluded 26 dyads (3.7%) with no information on functional limitations. In dyads with missing information on functional limitations the carer was more often a spouse (76% versus 59%). There were no other significant differences in the background characteristics between dyads with missing and not missing functional limitations data (results not shown). The path models were also carried out including the 26 dyads with missing functional limitations. The results were very similar to the pathway models excluding the 26 dyads and the conclusions based on the models were the same (results not shown).
We also analyzed those who reported IADL item not applicable to understand the underlying characteristics of this group who were omitted from the main analysis (7%-15% of the sample). This was done by comparing the background characteristics of people with dementia who reported not applicable to an IADL item with those who reported that they had that IADL need and with those who reported that they did not have that IADL need.
Results
Descriptive data
Table 1 shows the distributions of the background variables. The average age was 68 years for carers and 81 years for people with dementia. The proportion of women was 51% for people with dementia and 69% for carers. White ethnicity was reported by 95%. Of the carers, 59% were a spouse, 33% were not a spouse and not coresident and 8% were not a spouse and coresident. Thirteen percent of carers and 28% of people with dementia reported no formal qualifications while a higher education degree was reported by 30% and 18%, respectively. A routine occupation as their last job was reported by 26% of carers and 35% of people with dementia while professional/managerial level job was reported by 45% of carers and 35% of people with dementia. Most people with dementia were homeowners (77%) and nearly half lived in a major urbanization area (48%). The average area deprivation score was 6.4 with standard deviation (sd) 2.8. The overall functional limitations score was 14.5 (sd = 10.6). The most common type of dementia was Alzheimer's disease (58%).
Most of the people with newly diagnosed dementia had at least one IADL difficulty (83%) while less than half (42%) had at least one ADL difficulty (Figure 1). Of those with functional difficulties, 50% had at least one unmet ADL need and 31% had at least one unmet IADL need. Of the carers, 29% reported that the support from the health and social care services for the person with dementia was not adequate. The distributions and counts of unmet need are shown in Supplemental Table 2. The most common of these needs were using bath/shower (24%) for ADLs and doing shopping (80%) for IADLs (Supplemental Table 1). No help was most often reported when there was a difficulty in using the toilet. Some ADL/IADL items were reported as not applicable: up to 2% of each ADL and 7%, 13% and 15% of the IADLs of housework/gardening, shopping and doing finances, respectively.
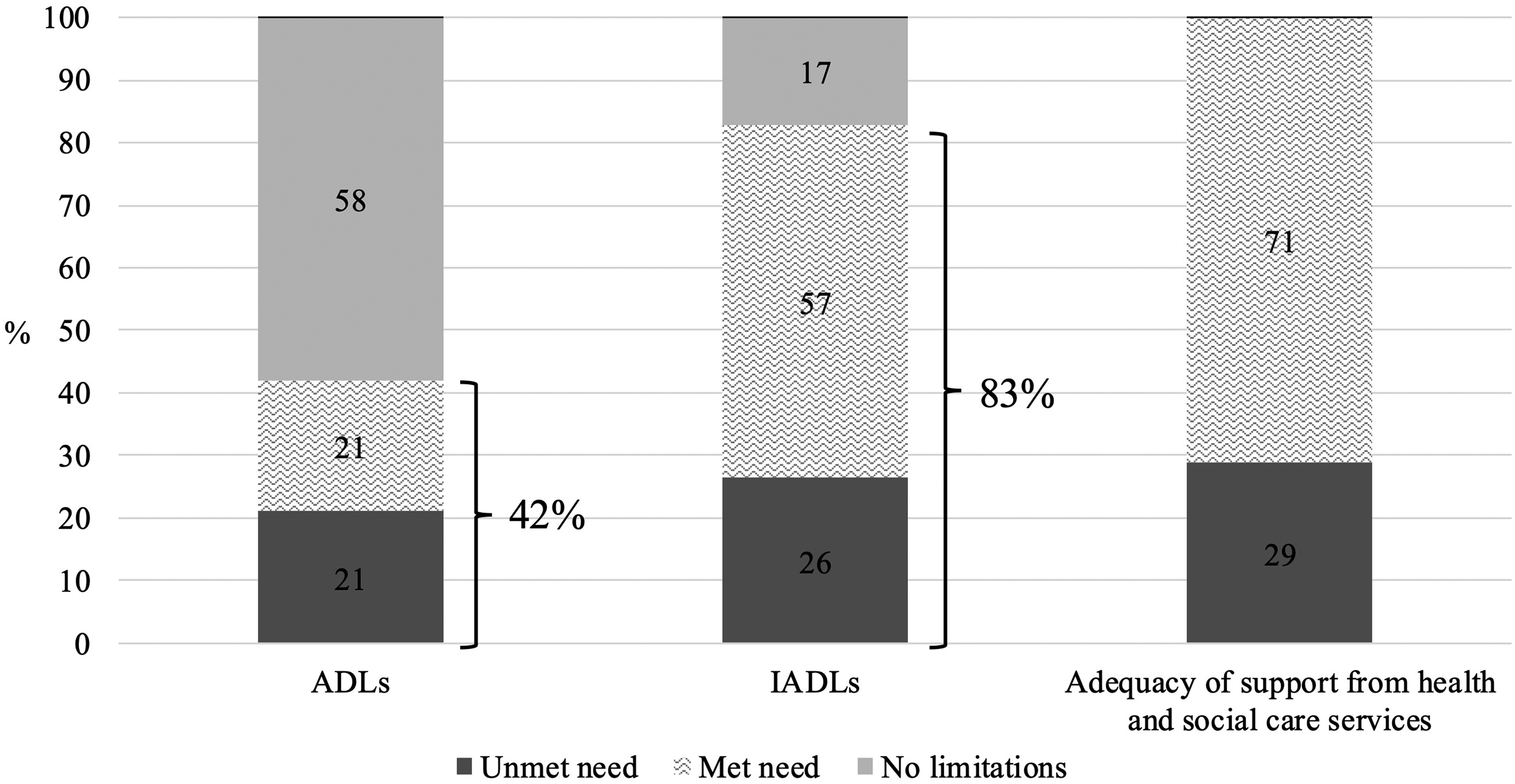
Distributions of activities of daily living (ADLs) and instrumental activities of daily living (IADLs) limitations and met and unmet need in ADLs, IADLs and adequacy of support from health and social care services in people newly diagnosed with dementia (n = 672).
We analyzed whether the background characteristics of people with dementia who were reported to have a “not applicable” IADL item differed from those who were reported to have that IADL need and from those who were reported not to have that IADL need (Supplemental Tables 5–7). The results showed that for all three IADL items “not applicable” answers were more frequent when the person with dementia was older compared to those without need and when the person had more functional limitations compared to those with or without need. Those who were reported to have “not applicable” housework/gardening or shopping related need had more often a female carer and lived in a major urban location compared to those with or without the need in question. Moreover, those who were reported to have “not applicable” housework/gardening or shopping need were more often male than female compared to those with need. In addition, in those with “not applicable” housework/gardening need the carer was more often not the person with dementia's spouse, person with dementia had lower education and was not a homeowner compared to those without need. Among those who were reported to have “not applicable” need relating to shopping, the person with dementia more often had a routine occupation compared to those without need. Among those with “not applicable” need on finances, the person with dementia was more likely to be female, not a homeowner, have lower education, be in an intermediate occupation, and live in a rural location compared to those without need.
The associations of background characteristics with unmet need and inadequate support
Of the background characteristics, male gender of the person with dementia, having an extra-resident carer, higher education of the carer, not being a homeowner and having lower levels of functional limitations were associated with unmet ADL need (bivariate associations in Supplemental Table 8). Higher age of the person with dementia but lower age of the carer, male gender of the person with dementia, having a spouse carer, higher education of the carer, not being a homeowner, living in an urban and more deprived area, and having Alzheimer's disease compared to vascular dementia were associated with unmet IADL need (bivariate associations in Supplemental Table 9). A lower age and higher education of the carer, rural location and higher levels of functional limitations were associated with inadequate support from health and social care services (bivariate associations in Supplemental Table 10).
Some bivariate associations reduced when they were included simultaneously in the multivariable model (Supplemental Tables 8–10). This suggests potential impact of socioeconomic pathways through the current characteristics (mediation; see Supplemental Figure 1). The associations between the background characteristics are shown in Supplemental Table 3. Many of the background characteristics were associated with each other supporting possible mediation between them when they were both associated with the outcome. The associations were very similar for the subgroups of those with ADL or IADL need (results not shown).
Path models
Figure 2 shows the associations between background factors and unmet ADL need. Women with dementia, those with higher levels of functional limitations and those having a co-resident carer were less likely to have unmet ADL needs. Moreover, there were indirect associations so that part of the higher likelihood of women with dementia having their ADL needs met was due to their higher levels of functional limitations compared to men. On the other hand, there was competing mediation so that more women than men with dementia had a carer with a higher education who was not coresident, which was associated with a higher unmet ADL need. Higher education of the carer and the person with dementia not being a homeowner were both associated with a higher unmet ADL need, in both cases through the carer not being coresident. The magnitudes of the direct, indirect and total effects are shown in Supplemental Table 11.
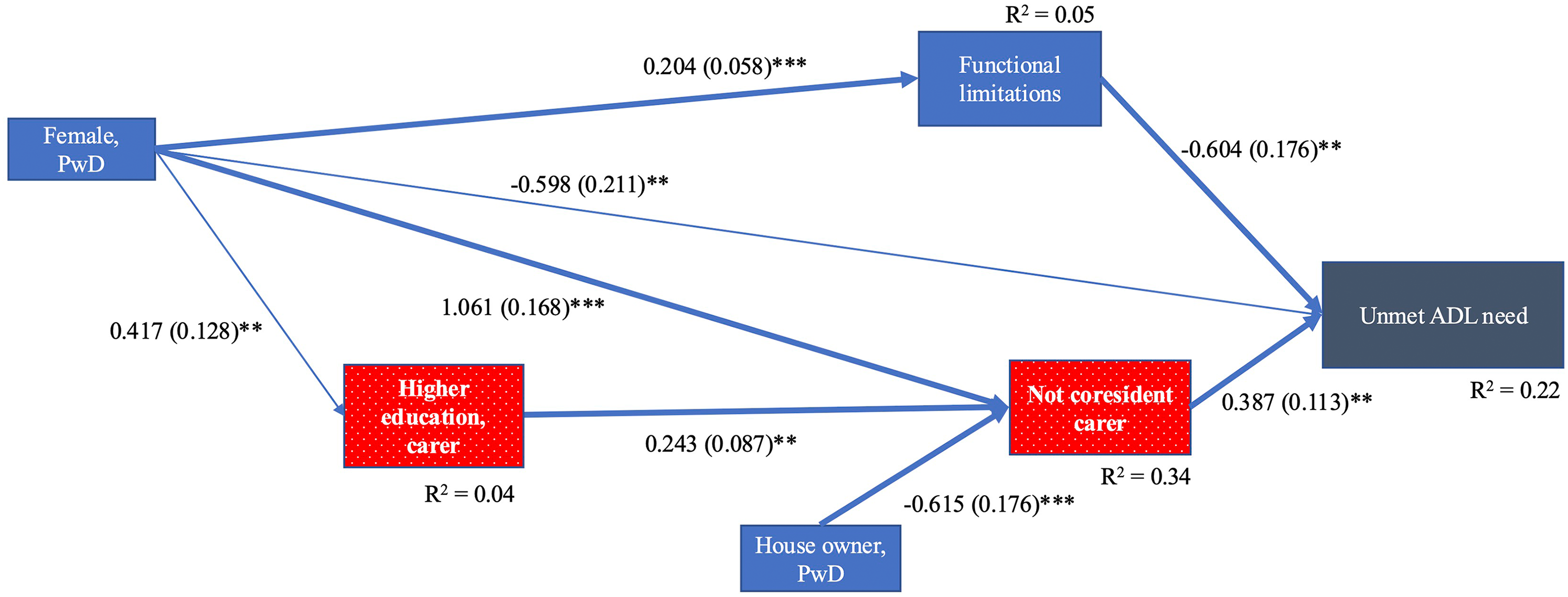
Path model for unmet need(s) in ADLs: people with dementia (PwD) and their carers (n = 294). Unstandardized estimates (standard error) are shown. * p < 0.05, ** p < 0.01, *** p < 0.001. Bold arrows illustrate mediation. χ2 < 5.45, df = 5, CFI = 0.99, RMSEA = 0.017. Note. Background characteristics in a dotted red box are associated with a higher unmet ADL need and in a blue box with a lower unmet ADL need. PwD = person with dementia (Color figure available online).
For unmet IADL need, there were many direct and indirect associations (Figure 3). Unmet IADL need was directly associated with lower levels of functional limitations, having a spouse carer, not being a homeowner and having Alzheimer's disease compared to vascular dementia. Older people with dementia were less likely to have an unmet IADL need due to higher levels of functional limitations and not having a spouse carer. Women with dementia were less likely than men to have unmet IADL need due to not having a spouse carer. Higher age and education of the carer were associated with higher likelihood of having unmet IADL need through carer being the person's spouse. However, both higher age and higher education of the carer were also associated with lower unmet IADL need (competing mediation) through socioeconomic and area characteristics (rural location, lower area deprivation and homeownership of the person with dementia). The magnitudes of the direct, indirect and total effects are shown in Supplemental Table 11.
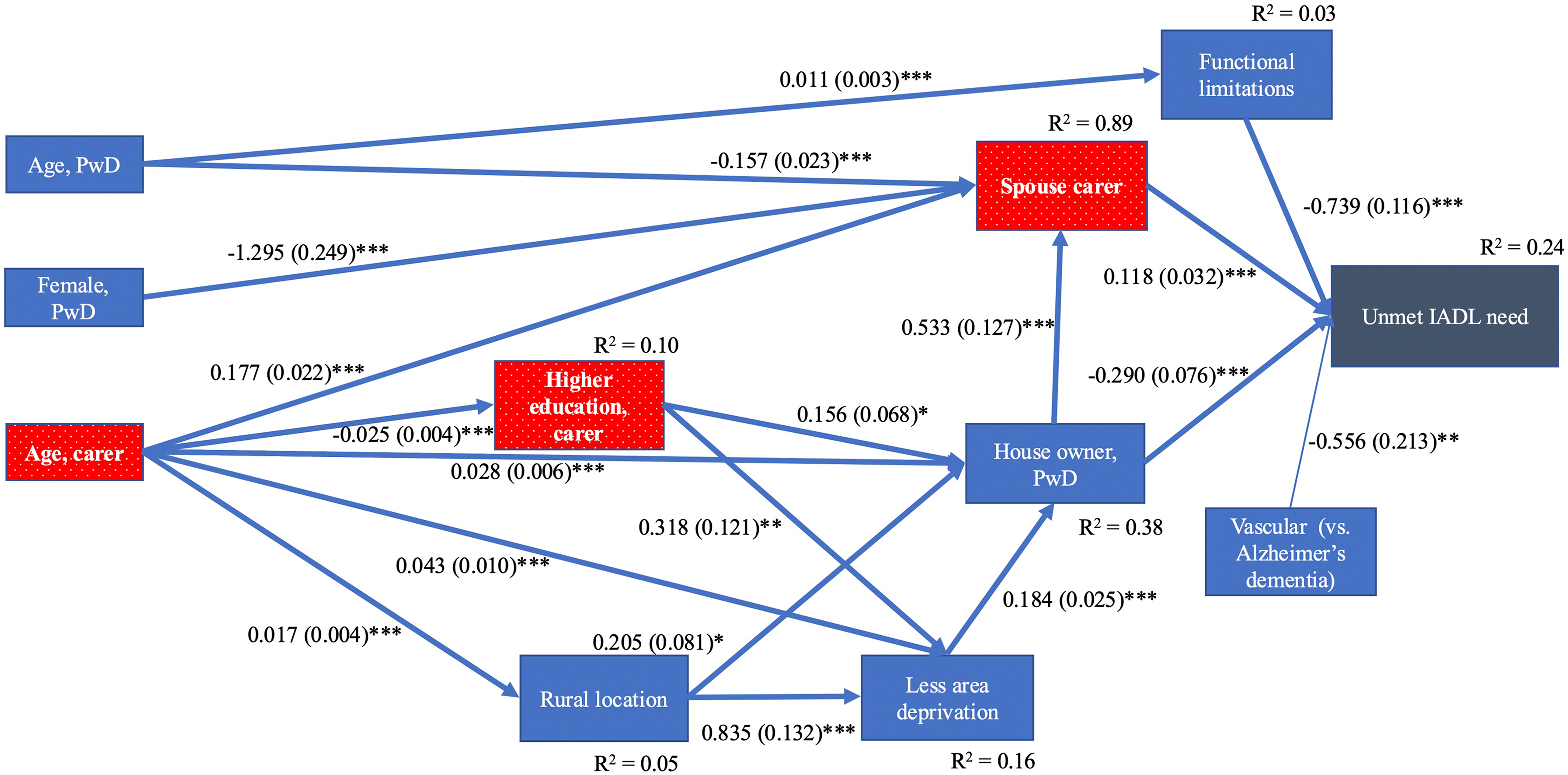
Path model for unmet need(s) in IADLs: people with dementia (PwD) and their carers (n = 578). Unstandardized estimates (standard error) are shown. * p < 0.05, ** p < 0.01, *** p < 0.001. Bold arrows illustrate mediation. χ2 = 97.45, df = 62, CFI = 0.94, RMSEA = 0.031. Note. Background characteristics in a dotted red box are associated with a higher unmet IADL need and in a blue box with a lower unmet IADL need. PwD=person with dementia (Color figure available online).
Figure 4 shows the associations with perceived inadequate support from health and social care services. There were direct associations between carer reported inadequate support from health and social care services and younger and higher educated carers, people with dementia with more functional limitations, living in rural locations and having mixed dementia compared to Alzheimer’ disease. Younger carers more frequently reporting inadequacy of support was partly due to the higher educational level of those carers. There was also competing mediation so that younger carers were more likely to care for someone in a more urban location, which was associated with more frequent report of adequate support. The magnitudes of the direct, indirect and total effects are shown in Supplemental Table 11.
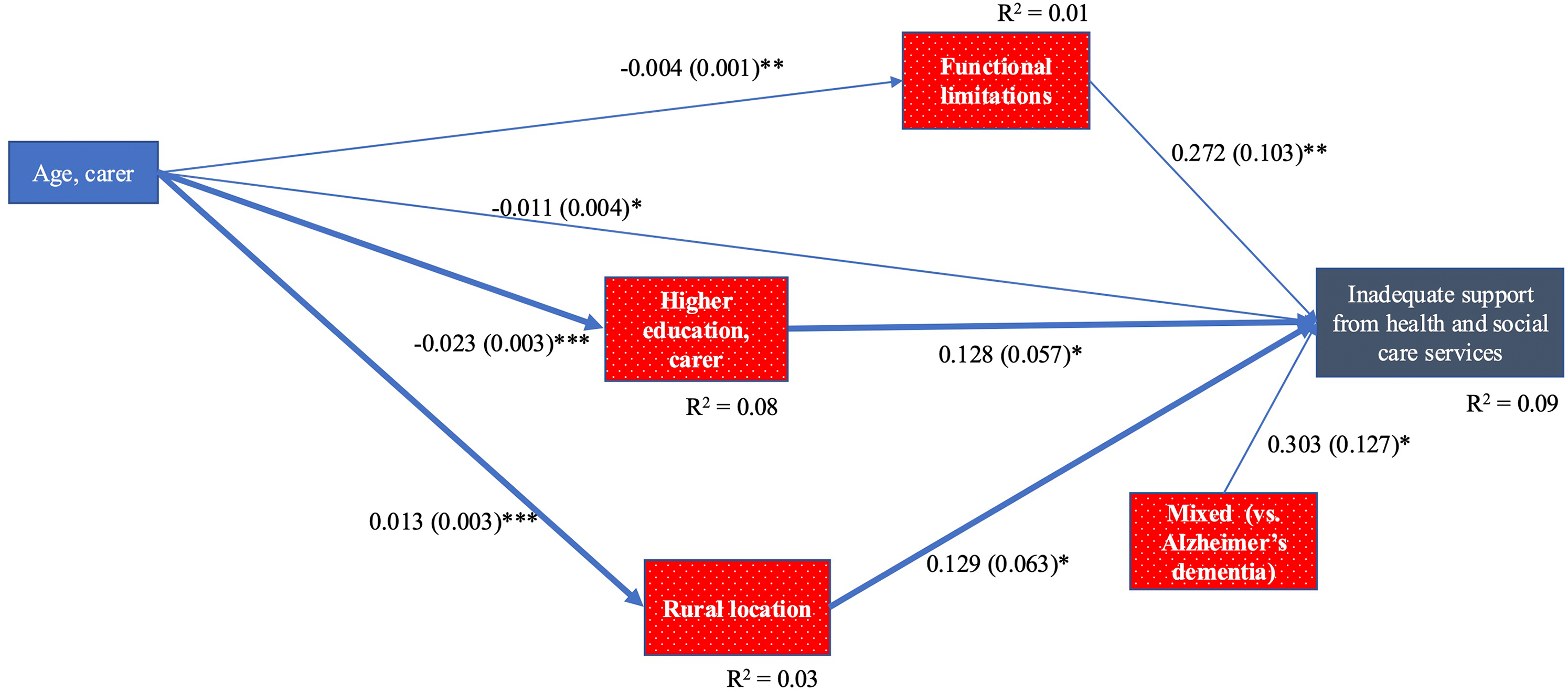
Path model for inadequate support from health and social care services: people with dementia (PwD) and their carers (n = 672). Unstandardized estimates (standard error) are shown. * p < 0.05, ** p < 0.01, *** p < 0.001. Bold arrows illustrate mediation. χ2 = 10.06, df = 7, CFI = 0.97, RMSEA = 0.026. Note. Background characteristics in a dotted red box are associated with higher perceived inadequacy of support from health and social care services and in a blue box with lower perceived inadequacy of support. PwD = person with dementia (Color figure available online).
Sensitivity analysis using unmet ADL and IADL need as a count in the final path model
The path estimates and model fit were very similar when using unmet ADL and IADL need as a binary versus a count outcome (see the comparisons of the path estimates and model fit in Supplemental Table 12). The only notable difference was that the path from functional limitations to unmet ADL need was stronger when the outcome was used as a binary versus a count measure (unstandardized path estimates −0.60 versus −0.21 for unmet ADL need; −0.74 versus −0.54 for unmet IADL need, respectively).
Sensitivity analysis adjusting for the study site
The three study sites (London, Sussex, and Northeast as a reference group) were added as covariates in the final model. The path estimates with and without adjusting for the study site were mostly similar (Supplemental Table 13). The only large difference was found for the paths related to urban-rural location which were not significant in the adjusted models for unmet IADL need and inadequate support for health and social care services as outcomes. The model fit, especially Comparative Fit Index, was poor when study site was added to these models. This suggests that there is an overlap between the measures as the locations systematically differ by their level of urbanization. In these models, the outcomes of unmet IADL need and inadequate support from the health and social care services differed by location, the former being lower and the latter higher in Sussex compared to Northeast.
Discussion
The aim was to investigate functional difficulties (need), unmet need and perceived inadequacy of support among newly diagnosed people with dementia and their association with care dyad's sociodemographic characteristics. First, there were differences in how well needs were met depending on whether the needs were related to ADLs, IADLs or perceived inadequacy of support from health and social care services. This suggests that not all needs are equal, and some are easier to pick up on and support than others. Second, the key mediation factors were the relationship with the carer (whether the carer was the spouse or coresident) and the level of functional limitations of the person with dementia. This finding suggests that both the living arrangements and the level of functional needs play a crucial role in determining whether sufficient help is received. Third, the results show complex direct and indirect pathways through several characteristics of the person with dementia and carer to unmet need and inadequate support from health and social care services. These associations have often been missed in the previous studies due to limited use of advanced analyses techniques. Our path analyses could pick up on some of the complexity and point to the need for further modeling with longitudinal data.
Differences in levels and proportions of unmet needs
Although the absolute levels of IADL needs and unmet IADL needs were higher compared to ADL needs and unmet needs, proportionally needs in ADLs were more often unmet (50%, compared to 31% for unmet IADL needs). The finding is in line with previous evidence. For instance, in people aged 65 + in England unmet ADL needs were proportionally higher (66% for dressing, 61% for bathing) compared to unmet IADL needs (12% for shopping, 24% for housework and garden work). 8 A similar finding was also reported in a subgroup of those with dementia in a general population sample of people aged 65+ in the United States: unmet ADL needs were higher compared to unmet IADL needs (18% versus 13%, respectively). 7 The difference between unmet ADL versus IADL needs became larger when people with dementia also had chronic conditions (29% versus 18%) and died (41% versus 6%). Similar to our results, the study found that the most common unmet need was related to using toilet in the subgroup of people with dementia.
The results above suggest greater barriers in getting help in ADL related tasks compared to IADL tasks in various old age populations, but especially those with dementia. This points to the reality that there are not enough resources to meet the needs, particularly when they are related to basic daily activities. In terms of dementia, this appears to be the case already at the early stages of dementia care pathway. Early-stage dementia related needs (such as specific ADL limitations) may be overlooked by the carer, difficult to meet if the carer is not available at the times help is needed (IADL needs are easier to postpone than ADL needs) or difficult to get professional help for if the needs are not severe enough to meet local authority eligibility criteria for publicly funded care. Carers may also prioritize some needs over others and choose to address those needs first. Further qualitative research on the topic is needed.
Support from health and social care services for the person with dementia was reported not adequate by 29% of the carers. A recent report by Alzheimer's Society in England found that 61% of people affected by dementia did not feel they or their loved ones had received enough support from local services to help manage dementia. 51 The higher proportion of insufficient support in this report compared to our finding may be due to the way the question was asked. The report included also support for people around the person with dementia. The question was asked from family members or carers and in some cases from people with dementia (8%). The sample was not restricted to those with new diagnosis. The ongoing follow-ups will reveal if the proportions of inadequate support increase over time in our sample of people with newly diagnosed dementia at baseline. Altogether, the results on the proportions of unmet need and inadequate support suggest that although many people newly diagnosed with dementia do not have substantial needs for care, those who do often go without help.
Key intermediary factors in unmet needs
The relationship with the carer
Our results point to the relevance of the relationship (whether a spouse) and co-residence (whether carers are around all the time or part-time) in how well needs are met. Previous work highlights the presence of spouse carer or not living alone as beneficial for meeting the needs of people with dementia.9,19,20,26,27 Although they have not separated the aspects of relationship and co-residence with carer as we have done in the present study, the results altogether suggest that the availability of apt help in the household enhances the chances of meeting the needs. Alternatively, carer's perception of needs and how they have been met may be less complete when they are not coresident or do not have a long history of living together. This may result in different reporting, e.g., over- or underestimation of the level of functioning and help received. For these reasons above, living arrangements could be one question post-diagnostic services could ask early in the care trajectory and direct people to relevant services.
Our analyses suggest that these carer characteristics (whether spouse/co-resident) may have a different effect depending on whether the unmet functional needs are related to ADLs or IADLs. Unmet needs related to ADLs compared to IADLs were more impacted by the presence of a carer. Compared to support for IADL needs, that for ADL needs is performed several times a day and cannot be easily postponed. Therefore, for meeting the ADL needs, availability of care within the household (carer coresident) was a key factor. This is in line with findings in other studies that found this factor to be relevant in meeting physical needs. 24 The need to have a carer present however may also be related to how mild, moderate and more severe needs are understood to affect everyday life. A person with slight problems may manage or be left to manage without help (note that the report of unmet need was from the carer). Person with dementia and/or their carer may not view these as an unmet need.
Unmet needs in IADLs seem to be related to whether the carer is the person's spouse or someone else. As there was also an association with the gender of the person with dementia, the finding may suggest possible gendered division of work and/or perception of what is help in household related IADL tasks (such as housework, gardening, shopping and doing finances) from earlier in the marriage/partnership. For instance, a carer who is the wife to the person with dementia may consider the tasks of preparing meals and shopping as not help as they have always done these tasks. Therefore, in these spousal care dyads no help may be reported and appear as unmet need for the husband. Conversely, husband carers may recognize the help they give in IADLs as an extra or new task they did not perform before and therefore will be reported and recoded as a met need. Although the role of gender in shaping the experiences of older men and women has been discussed previously,52–54 it is important to explore it further to understand its role in everyday activities in care dyads of people affected by dementia. The association with the older age of carer in spousal care dyads could also suggest that higher unmet need in IADLs may be due to poorer health and functioning of older spousal carers, compared to carers who were not a spouse and tended to be younger.
Neither spousal relationship nor co-residence with carer was a significant predictor of perceived inadequacy of support from health and social care services. This may reflect the universal nature of perceived support from services regardless of who and how much the carer is present. The lower proportion of overall variance (R2) explained by the model for inadequate support from health and social services further suggests that there are no large variations due to sociodemographic or other care dyad characteristics in how carers perceive the adequacy of help from formal services.
The level of functional limitations
Our results show that unmet ADL and IADL needs were more prominent at lower levels of these functional limitations. It has been suggested that when care needs increase with progression to more severe stages of dementia, the identification of any needs—related or unrelated to cognitive impairment—may become more urgent and this may enable access to the help required. 55 Some previous studies have shown that when there are low levels of functional difficulties in people with dementia 6 or no longstanding illness in older people in general26,27 unmet needs tend to be higher compared to unmet need among older people in general, which suggests that when needs are not expected they may go unnoticed and thus unmet. Moreover, some studies focusing only on people with dementia have reported more unmet needs in those with milder functional impairments20,22 and in early stages of dementia. 5 The stepwise regression modeling suggested that one of the key factors was that a higher proportion of those with milder functional impairment were living alone in which case help may not be available or the need not detected by others. 20
Unlike what we found for unmet ADL and IADL needs, functional limitations were higher in those people with dementia whose carers reported inadequate support from health and social care services. There may be different experiences and expectations of help depending on the level and type of functional limitations (e.g., if not typical for dementia) and various other user and service providers’ characteristics.14,56 Those with more needs were likely to have had more contacts with health and social services and experienced delays and difficulties in getting the services they need, a problem increasingly common in recent years,57,58 and therefore may have more often reported inadequacy of formal support.
The role of functional limitations in unmet need is not consistent across the various studies,7,9,24,29 see a summary in Supplemental Material 1. However, together with longitudinal findings, 19 they point to the importance of identifying and supporting people with dementia with unmet needs early on, especially when the needs are not typical for dementia. This could be done during the diagnostic process to actively signpost according to needs. On the other hand, those with more needs and poorer functioning, typically later in the dementia pathway, may struggle to get help, especially formal care. Easier access to post-diagnostic services could help to reduce unmet needs when needs are high. In addition to directly addressing the needs of the person with dementia, better support to their carers is essential so they can provide adequate support for the person with dementia they care for.
The predictors and pathways to unmet ADL/IADL need and perceived inadequacy of health and social services
The current study finds several sociodemographic and other background characteristics of both the person with dementia and carer to be associated with unmet need and inadequacy of support. The evidence from previous research is mixed: the associations of the care dyad characteristics with unmet need vary from one study to another. The current study shows that background characteristics varied between the three outcomes of unmet need and inadequate support. Moreover, it showed chains of associations between the different factors which may help to understand the inconsistencies found when pathways and mediation through the characteristics have not been taken into account.
Characteristics of the person with dementia
Previous studies report mixed findings on the role of age and gender of the person with dementia on unmet need. Some studies have found more unmet need in men16,17 while some others in women18,19 with dementia. In terms of age, some studies have found higher age of the person with dementia is associated with unmet need10,16 and faster increases in functional unmet needs. 19 However, lower age has also been reported to be associated with unmet need. 20 The current study showed that compared to women, men had more unmet ADL and IADL needs while unmet IADL needs were higher in younger compared to older people with dementia. The path analysis showed that age and gender effects were often associated with the outcome through other characteristics in the model which we discuss further below.
Ethnicity as a predictor of unmet need has been rarely included in the previous studies. Two studies in the United States found non-white ethnicity to be associated with unmet need in people with dementia.20,22 In a study from Brazil, black/brown ethnicity was initially associated with unmet need in people with dementia but ceased to be significant when adjusted for the level of needs. 17 Our study did not show an association between ethnicity and unmet need or inadequacy of support. In the current study the group of those not white was small and heterogeneous which may impact comparisons.
One of the most consistent findings across the different studies appear to be that higher socioeconomic status of the person with dementia is associated with how well needs are met.6,17,19,20,22–24 This was also the case in the current study in terms of homeowners having less unmet ADL and IADL needs. Homeownership may allow better environment for caring and opportunity to adjust for needs. For instance, our results illustrate that people with dementia who were house owners were more likely to have a coresident carer which helped to meet ADL needs. In terms of IADL needs, homeownership was a strong predictor of met IADL needs. However, the benefit of being homeowner was to some extent reduced because the carer was likely to be spouse. As already discussed, performing and/or reporting help with IADL tasks such as housework and doing finances may differ between the spouses in the same household which may impact how needs are reported to be met.
Characteristics of the carer
Several previous studies have identified the relationships of carer characteristics, such as male gender, 17 younger age and not being a spouse,9,21 and carer having poorer health with unmet needs.9,17,28 The studies that have included several characteristics of people with dementia and their carers have found that often carer factors are stronger predictors of unmet needs than the characteristics of the people with dementia.9,31 Our results point to a similar pattern but suggest sequential pathways between the characteristics in the care dyads so that the current needs and living arrangements of the person with dementia which have been shaped by the age and gender as well as carer's characteristics create circumstances where needs are more or less likely to be met.
The associations could illustrate some of the complexities and findings that may appear against the odds of what is generally expected. For instance, that certain carer characteristics such as higher education, a characteristic usually associated with a higher chance of needs being met, 20 is associated with less likelihood of receiving help in ADL and IADL needs. The current models suggested that this happened because a higher educated carer is less likely to live with the person with dementia (for unmet ADLs) or is a spouse (for unmet IADLs, through homeownership and lower area deprivation). These pathways may help to understand that even though some sociodemographic factors, such as higher education is often beneficial in terms of receiving help, they may also cluster with factors such as living arrangements which may not support meeting needs. Alternatively, there may be different interpretations of needs and whether help should be provided depending on social strata and how much the carer is present. Further qualitative work may help to understand the reasons behind the found pathways.
Another notable factor showing a complex association with unmet need through mediation was age of the carer. Older carer age was associated with more unmet IADL needs among people with dementia, a finding not in line with some other studies.9,21 The different results may be due to measuring unmet need differently (these two studies used the CANE instrument to measure unmet need). The inclusion of the pathways between a wider range of background characteristics in our path models made it possible to identify why the older age of the carer was associated with unmet IADL need: an older carer was more likely to be a spouse which turned out to be an important factor in how well IADL needs were met, possibly related to poorer health and functioning in spousal carer due to age. Moreover, the association with the gender of the carer suggested gendered division of housework in spousal care dyads which may affect how needs and help are perceived and reported, as discussed above.
However, when using another receipt of help outcome—inadequacy of support from health and social care services—younger age of the carer was associated with reporting inadequate support, partly because they had a higher level of education and cared for a person with dementia with more functional difficulties. These two mediators may have contributed to the carer experiencing more contacts or attempted contacts with formal services and possible problems accessing them and /or disappointment with their quality, as discussed above. The carer's expectations of the access to and/or quality of care may be higher when their educational level is higher. However, younger carers were less likely to care for someone in a rural location where perceived adequacy of support was more negative. Previous studies have discussed that the association of younger carer age with unmet needs could be related to the carer's circumstances, e.g., competing demands related to the carer's own family and work. 9 The pathways in the current study bring up an interesting additional angle that this association can also be shaped by the type of help in question (meeting IADL needs, support from formal services) and characteristics of both carer (education, whether spouse or someone else) and person with dementia (level of functional limitations, rural location). Future research would benefit from exploring these associations in more detail.
Complex pathways between the characteristics of carer and person with dementia
The current study identifies several routes and interplay of various personal and environmental characteristics through which help is received. While it may be difficult to grasp the meaning of competing mediations in a complex model, it may be useful in understanding in practical terms that mediation can, through some mediators, have positive and some other mediators negative association with the outcome, hence reducing or canceling out the overall total effect. The competing mediation could be seen especially in the pathways for age and gender in how needs are met. For instance, although women had less unmet ADL needs compared to men, partly due to having more functional limitations which were more likely to be met, some of the gender advantage in meeting these needs was reduced for women as their carer was less likely to live with them, compared to carers for men with dementia who were more likely to be coresident.
Similarly, unmet IADL needs were associated with having an older carer who was a spouse. However, older age of the carer was also associated with homeownership and living in a rural, less deprived living area —all conditions that supported meeting the IADL needs—which to some extent reversed the negative impact of having an older carer. These observations from the path models point to the importance of investigating the role of the factors both independently and organizing them together in a path model. Whether the factors such as age and gender are beneficial or not depends on their associations with other characteristics, i.e., there is no straight forward way to label sociodemographic characteristics as positive or negative. This highlights the need for thorough and complex modeling.
The inspection of the underlying characteristics of the group of those who reported IADLs as “not applicable” can help to understand who were excluded from or included in the model, potentially impacting the results. The findings suggest that reporting IADLs as not applicable may reflect potential gender differences in household chores 54 so that some tasks may be considered inapplicable for women because they were conducted by men (e.g., managing finances), or inapplicable for men because they were conducted by women (e.g., housework). The results also suggest that tasks may be rated as not relevant when the living environment and daily living requirements might have been adjusted for more severe limitations (the associations of not applicable with higher number of functional limitations, older age of person with dementia, living in major urban location, not homeowner). When the care dyads providing “not applicable” -answers are omitted, (unmet) needs among those at the early stages of disease may appear to be more frequent than in those at later stages of the disease. People may not need to do things when they have more functional limitations, 7 e.g., housework and shopping may be reported as “not applicable” if the person is bedbound or live in an accommodation where all the services are provided.
Strengths and limitations
Our sample included nearly 700 dyads of people with newly diagnosed dementia and their carers with detailed information on their sociodemographic and socioeconomic characteristics. This is an important group to study to identify those more likely to experience lack of support soon after the diagnosis of dementia, which have policy implications for delivery of post-diagnostic support.
The current analyses add understanding of the pathways between the factors associated with unmet needs. While Andersen's behavioral model of health services helps to theoretically cluster the characteristics associated with unmet needs into thematic sub-groups (predisposing, enabling, and need factors), 15 it does not tell how these factors should be organized and whether some of them are associated with each other and create a chain of associations (mediation). Past studies have rarely used path modeling, and if they have, the included background characteristics have been limited.19,21 Most studies carry out multivariable regression models to identify factors that are associated with unmet need.
Multivariable regression assumes that the adjusting factors are independent variables or confounders and not on the causal path between the primary exposure and outcome. Sometimes factors that are initially significant in bivariate analyses are insignificant when adjusted for other sociodemographic factors in multivariable models, e.g., living arrangements or functional limitations of the person with dementia.9,20 If they are added to a stepwise regression in the later steps without inspecting the initial associations with the outcome, 17 their role may not be discovered because potential mediation has not been taken into account. Our results from the multivariable regression and path models show this. If we had relied only on the results of multiple regression, we would have concluded that the characteristics of the person with dementia, the carer's education and the relationship with carer had little impact. Some studies explicitly mention the correlations between the covariates, for instance that education of the carer correlates with carer stress, IADL/ADL difficulties and education of the person with dementia, and therefore education of the carer was excluded from the regression analysis. 31 Some have not included functional limitations. 10
Regression analysis cannot identify chains of influence as can be done in a pathway model. 59 The paths between these factors can shape the receipt of help and whether needs are met. Understanding which factors are involved and how can help to develop person-centered care and inform how to target responding to dementia needs. 60 Pathway modeling helps to understand the chained associations between the background characteristics, current circumstances (e.g., level of functional difficulties) and receipt of help. It gives a more nuanced picture of the associations between various background factors which may not be apparent in multivariable regression analysis which cannot handle mediation.
However, the study has some limitations. Although the organization of the background characteristics in the path and mediation models can be justified by the temporal order of the events, the data collection was cross-sectional and based on retrospective reporting which may be influenced by participants’ current state. This could have more impact on recalling events in the distant past, e.g., reporting education or occupation but likely less on demographic variables such as gender and age. Some variables were not asked directly, e.g., urban-rural location and area deprivation were created based on the post codes. The order of the events may not also reflect the reality for all participants. Some associations may be bidirectional or even reversed, therefore reflecting a network or “clusters” of items (e.g., the association of the educational level of carer and person with dementia or the living context of person with dementia including urban-rural location, area deprivation and homeownership).
Although incomplete data were handled with missing data methods, the characteristics of those who did not participate at baseline are not known and can affect the initial sample characteristics and the results. A selection of ADL and IADL items was used to create the unmet need variables. Some areas of functioning that may be of interest are not considered, e.g., spiritual needs that are often high and not assessed or taken into account in care 61 or psychosocial needs such as meeting family and friends. 62 Although we analyzed unmet needs for ADLs and IADLs separately, a more detailed understanding of each need within each of these two functional categories may be necessary, e.g., what are the adverse consequences. 63
There may also be alternative ways to construct and use unmet need variables. The comparison of the models for unmet ADL and IADL need as a binary or count measure showed little difference. This could be expected as in this group of people recently diagnosed with dementia very few had more than one unmet need. An outcome measure that takes into account the number or severity of unmet needs may however be needed when following up people over time with increasing severity of dementia and (unmet) needs. The score of the functional limitations included some of the same items that were used for creating unmet ADL and IADL need variables (i.e., a selection of functional limitations were used to establish ADL or IADL need and a second variable measuring receipt of help was used to identify whether the ADL or IADL need in question was met). The use of partly overlapping information may contribute to shared measurement between functional limitation and unmet ADL and IADL need outcome. This is important to take into account when interpreting the models. Adjusting for functional levels is however a usual practice and not doing so may also alter the interpretation (see the summary of variables used and associations found in the previous studies in Supplemental Table 1).
Needs and whether they were met were reported by carers and therefore represent a carer's point of view. Moreover, carer characteristics can affect perception and reporting of functional limitations and unmet needs person with dementia has, e.g., related to how much the carer is present (co-resident or not) or information processing skills which may vary by educational level. Carer's view is likely to be different from how people with dementia perceive the situation. Previous studies suggest that people with dementia report fewer (unmet) needs than their carers. 36 A qualitative analysis suggested, however, that people with dementia may experience more significant limitations than some of their ratings may imply. 64 There may be variability in needs and distress related to unmet needs that may determine how people with dementia perceive their circumstances. 65 This may justify for relying on carers’ assessments of levels of need and whether they are met although carers too are likely to experience distress related to unmet needs of the PwD. In the future studies, it is important to include the view of people with dementia on whether they recognize these as needs or unmet needs. Regardless of their cognitive limitations their perception and agency should be considered.
The dataset covers some locations in England and includes dyads of carer and person with newly diagnosed dementia. The results are not necessarily generalizable to other contexts, places or to people whose dementia was not newly diagnosed. Our future analyses over time will provide a more detailed longitudinal account of needs and unmet needs and how they may change. Further work is also needed on the study location differences which we noticed in the sensitivity analysis. Some sociodemographic variables, such as urban-rural classification, were picking up the location differences. However, some location differences in unmet need were evident despite the information on the individual and area sociodemographic characteristics in the models. These differences need more investigation, e.g., to understand care provision and organizational characteristics in each location. The associations in the pathways were modest to moderate and there may be other factors not included in our study that should be considered for future research.
Conclusions
Half of the people newly diagnosed with dementia had at least one unmet ADL need while 31% had at least one unmet IADL need and 29% reported inadequate support from the health and social care services. Our study identified relationship and living arrangements with carer and functional limitations of person with dementia as key mediators while there were numerous other important pathways, sometimes resulting in a competing effect. The modeling of the pathways between the characteristics of the people with dementia and their carers on unmet need can help to identify and potentially improve care dyad's care strategies and engagement. Overall, the results point to the importance of recognizing unmet need at the early stages of dementia, especially when needs are not typically related to dementia, and to making sure that there is also adequate formal support when needs are higher.
Although there are some direct pathways from socioeconomic disadvantages to unmet needs, majority of these pathways to unmet need run through levels of functional limitations and relationship with carer. Both are potentially modifiable pathways. While it is not necessarily possible to change the intermediate factors, it may be possible to limit the potentially adverse impact by modifying the wider support networks and making living environment more dementia-friendly. 3 Leaving people without help they need at the start of the care pathway can have devastating effects.3,51 It may directly impact the wider health and care system while the lack of consistent support means people with dementia and their carers are at greater risk of crisis and reduced wellbeing. Longitudinal analyses exploring the unique context of people affected by dementia and the wider support systems are needed to develop tailored interventions that work for individuals, their families and are deliverable for services.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261459015 - Supplemental material for Functional difficulties, receipt of help, and unmet needs among people with newly diagnosed dementia: Results from the DETERMIND project
Supplemental material, sj-docx-1-alz-10.1177_13872877261459015 for Functional difficulties, receipt of help, and unmet needs among people with newly diagnosed dementia: Results from the DETERMIND project by Sanna Read, Nicola Brimblecombe, Ben Hicks, Bo Hu, Derek King and Raphael Wittenberg in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We are grateful to the researchers who collected the data and the participants who gave up their time free of charge to contribute to the research.
Ethical considerations
Ethics approvals were granted by the Health Research Authority Brighton and Sussex Research Ethics Committee (REC 19/LO/0528. IRAS 261263).
Consent to participate
Written informed consent was obtained from all participants involved in the study. In cases when person with dementia did not have capacity, a written signed Consultee Declaration form was obtained for them.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The DETERMIND study was supported by the Economic and Social Research Council (UK) and the National Institute for Health Research (UK) through grant number ES/S010351/1 “Determinants of quality of life, care and costs, and consequences of inequalities in people with dementia and their carers” (Investigators: S. Banerjee, K. Baxter, Y. Birks, C. Brayne, M. Dangoor, J. Dixon, P. Harris, B. Hu, M. Knapp, S. Read, L. Robinson, J. Rusted, R. Stewart, A. Thomas, R. Wittenberg).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Direct access will be granted to authorized representatives from the Sponsor and host institution or via request to the study CI Professor Sube Banerjee (sube.banerjee@nottingham.ac.uk). Following the end of the study in January 2027, anonymized data will be uploaded to the UK Data Archive online repository. Access to data will be limited to authorized researchers who agree to the End User License (![]() ).
).
Supplemental material
Supplemental material for this article is available online.