
Abstract
The defining features of Alzheimer's disease (AD) include neurodegeneration, a decline in cognition, and tau and amyloid-β protein pathologies. Sleep problems affect many individuals with AD and could be an aggravating factor in the disease because it creates a barrier to the glymphatic system's ability to clear neurotoxic proteins, disrupt the plasticity of synapses, and increase neuroinflammation. Suvorexant, which works as a dual orexin receptor antagonist, has proven effective in the management of sleep problems by fine-tuning the orexin system, which regulates arousal. Preliminary studies indicate that, in addition to improving sleep, Suvorexant could potentially help in the reduction of amyloid and tau buildup, as well as the improvement of synaptic activity and reduction of neuroinflammation. Recent clinical studies show improvements in sleep quality among older adults, in addition to safety and efficacy, and suggest increasing cognitive functioning in mild cognitive impairment and early AD. This review summarizes the existing research on the potential of Suvorexant as a therapeutic to address the mechanisms of orexin signaling in AD, as well as the sleep-targeted interventions to address the symptoms and modify the disease to improve cognitive functioning. We also emphasize future research directions such as cognitive outcomes over extended periods, potential optimal dosing, and combinatory strategies with lifestyle and/or medication therapies. This review will discuss the current evidence regarding the therapeutic effects of suvorexant and orexin signaling in AD.
This is a visual representation of the abstract.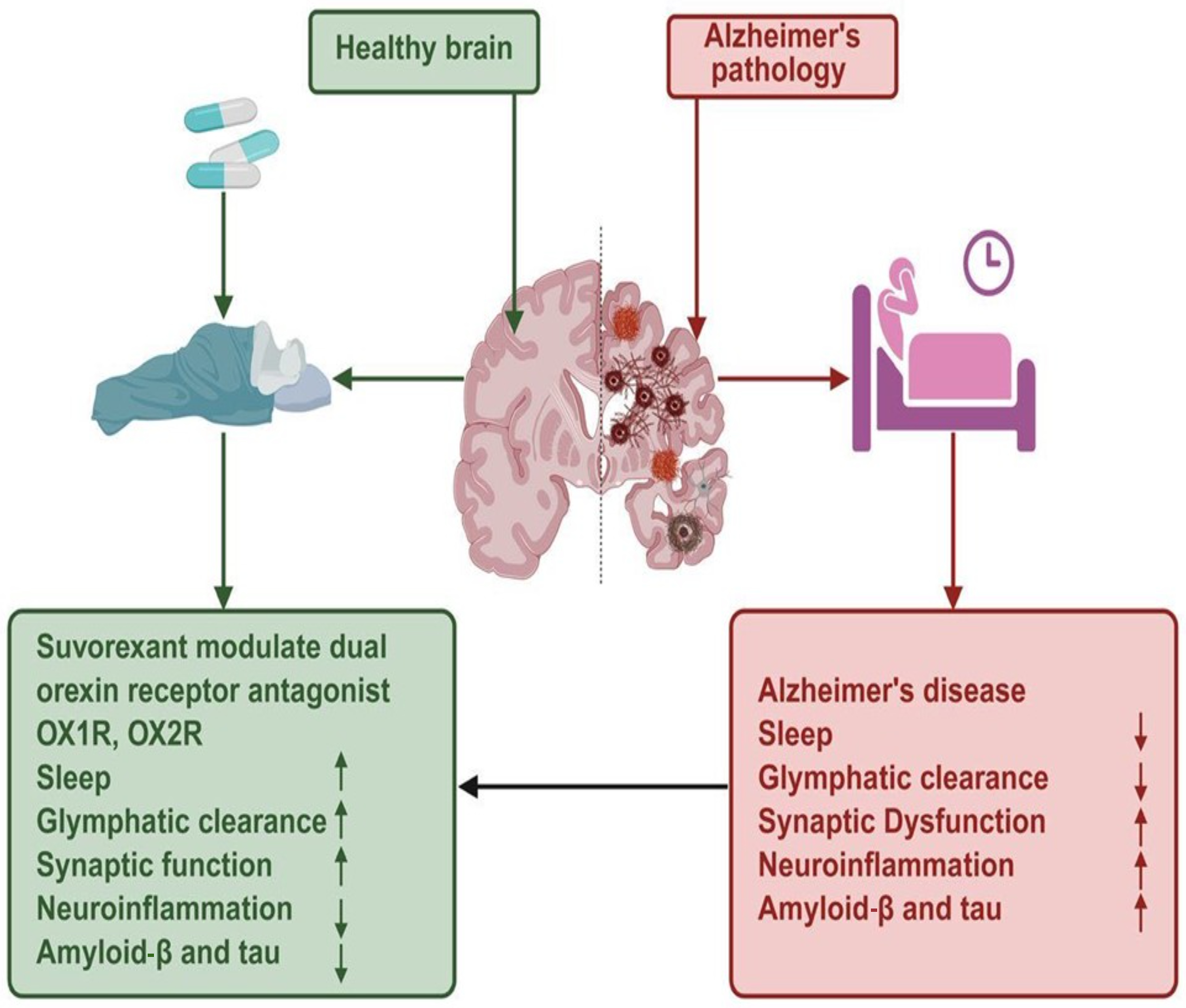
Keywords
Introduction
Alzheimer's disease (AD) is the most common type of dementia, and is a growing global health concern given the millions of elderly individuals that are impacted by this disease.1,2 The disease is associated with continuous and progressive decline in cognitive processes, including memory, executive functioning, orientation, and behaviors, culminating in severe impairment of independence, and ultimately, death.3,4 The pathological features of AD consist of the excessive extracellular presence of the amyloid-β (Aβ) peptide within the so-called senile plaques, while the intracellular inclusions consist of the aggregated hyperphosphorylated tau protein within the neurofibrillary tangles.5,6 These abnormal protein aggregates stimulate chronic neuroinflammation and cause the dysfunction and death of neurons, particularly in the hippocampus, entorhinal cortex, and other cortices, by disrupting inter-neuronal signaling.7,8 Cognitive decline associated with AD clinical progression is deeply intertwined with the widespread neurodegeneration and the synaptic loss 9 . 10 From the Aβ and tau pathologies, the clinical symptoms and neurodegeneration correlate more closely with tau. 9 However, Aβ pathology commonly develops before tau pathology. 11 These changes, both molecular and structural, begin decades in advance of an individual receiving an official clinical diagnosis because of the disease's long preclinical phase.12,13 The earliest non-cognitive symptoms of mild cognitive impairment (MCI) and AD that can be observed in clinical settings involve sleep disturbances. 14 Losing the ability to sleep soundly is one of the earliest and most common symptoms linked to MCI and AD.15,16 An estimated 40% to 80% patients with AD show sleep disturbances, which range from insomnia, disrupted sleep, increased nocturnal awakenings, daytime sleepiness, circadian rhythm disruptions, to altered sleep architecture.17,18 As the disease progresses, problems like these typically arise during the preclinical stage (e.g., MCI). 12 Several studies suggest a two-way interactive association between AD pathology and sleep disturbances.19,20 Sleep is vital for the clearance of metabolic byproducts in the brain through the glymphatic system, especially during deep non-rapid eye movement (NREM) sleep.21,22 The reduction of the clearances of Aβ and tau due to chronic sleep disruption is an example of the buildup of these proteins in the brain interstitial fluid, a phenomenon that may promote the pathology of AD.23,24 More Aβ and tau in critical brain regions disrupt the neuronal networks responsible for the regulation of sleep, perpetuating the problem of sleep disruption.25,26 Several longitudinal population-based studies report an association of chronic poor sleep, less slow wave sleep, sleep fragmentation, and disrupted circadian rhythms with an increased burden of Aβ in the brain and higher risk for cognitive decline and progression from MCI to AD.19,27 Orexin, also referred to as hypocretin, along with its system, peptidic neurotransmitters (orexin A, orexin B, OX1R, OX2R), and their receptors, OX1R and OX2R, is an example of a system that is to be synthesized by lateral hypothalamic neurons and is to participate in the cycle of sleep and wake regulation and control, arousal and energy homeostasis.28,29 Orexin is signaling in the brain to maintain stabilizing of the sleep-wake transitions and is signaling in the arousal centers in the brain to promote wakefulness and signaling in the brain to stimulate cognition centers.30,31 Recent studies indicate that dysregulation of the orexin system may occur with alterations in the hypothalamus in AD and may be linked to sleep problems and cognitive deficits.32,33 Increased orexin levels in the cerebrospinal fluid (CSF) of patients with mild to moderate AD are observed in correlation with decreased cognitive performance and are associated with poorer sleep efficiency and decreased rapid eye movement (REM) sleep.34,35 Increased orexin activity could indicate a compensatory mechanism in response to the neurodegenerative processes and/or dysregulation of the neurotransmitter systems involved in the regulation of the sleep-wake cycle.33,36
Moreover, clinical studies have reported that increased levels of orexin, sleep disturbance, and elevated AD biomarkers like total tau and Aβ are interrelated, which indicates that orexin signaling and sleep disturbance might be involved in the pathophysiology of AD. 34 There are, however, some neuropathological studies describing the loss of orexin neurons in the advanced stages of AD, suggesting that the orexinergic system might become dysfunctional during the progression of the disease.37,38 Even with such complexity, it seems orexin dysregulation relates to both sleep impairment and cognitive decline in AD, which justifies attempting to target this system therapeutically.32,39 This review seeks to explore mechanisms of the orexin system, sleep dysfunction, and AD pathology, and emerging evidence supporting suvorexant, a dual orexin receptor antagonist, as a potential treatment for AD. We aim to explore how modulation of orexin signaling due to suvorexant and potential improvements in sleep, disease-related biomarkers, cognitive trajectories, and alterations beyond symptomatic sleep improvement.
Methods
From 2020 to 2026, a systematic review of the literature was carried out in databases such as PubMed, Scopus, Web of Science, and Embase, using the terms “suvorexant,” “orexin receptor antagonist,” “Alzheimer's disease,” “mild cognitive impairment,” “insomnia,” “sleep,” “amyloid,” “tau,” and “cognition.” Eligible studies encompassed clinical trials, observational studies, and preclinical studies analyzing the impact of suvorexant on sleep, cognitive function, AD related biomarkers, synaptic physiology, and neuroinflammation. Exclusion criteria included reviews, editorials, publications in languages other than English, and studies that did not include suvorexant or pertinent sleep interventions. Data extracted from each study included participant characteristics, details of the intervention (dose, duration, and combination therapies), primary and secondary outcomes, and safety profiles. The Cochrane Risk of Bias tool for clinical trials, Newcastle–Ottawa Scale for observational studies, and SYRCLE tool for animal studies were used to evaluate the studies’ methodological quality. The findings have been synthesized narratively with a focus on sleep outcomes, cognitive outcomes, modulation of biomarkers, and safety, while also addressing gaps in the literature and future research needs, including the cognitive outcomes of these interventions in the long-term, questions around the optimal dosage of these interventions, and the potential of these interventions in combination with lifestyle or pharmacological approaches.
Physiological basis: orexin signaling and Alzheimer's disease
The orexin system (or hypocretin system) consists of two neuropeptides (orexin A and orexin B) that are synthesized by a small population of neurons in the lateral hypothalamus.28,40 These neuropeptides function through two G protein-coupled receptors, orexin receptor 1 (OXR1) and orexin receptor 2 (OXR2).29,41 Orexin neurons have widespread projections to the locus coeruleus, basal forebrain, dorsal raphe nucleus, and tuberomammillary nucleus, all of which are involved in arousal, attention, and energy balance, thereby incorporating metabolic and circadian information to modulate networks that promote waking. 28 Orexin signaling helps stabilize consciousness during wakefulness by activating monoaminergic and cholinergic nuclei and blocking inappropriate shifts to sleep. 42 The loss of orexin neurons in humans or the genetic disruption of orexin or its receptors in animals causes narcolepsy, which is characterized by excessive sleepiness and disordered sleep-wake cycling, demonstrating the importance of orexin in sustaining wakefulness and arousal.30,42
Orexin in AD and sleep disruption
In AD, sleep difficulties for the affected individuals are associated with the dysregulation of the orexinergic system.32,36 Studies analyzing CSF in patients with AD have documented higher levels of orexins in patients with pronounced sleep fragmentation, decreased sleep efficiency, and reduced REM sleep. 34 Heightened orexin levels have corresponding cognitive deficits, and greater amounts of tau and amyloid biomarkers, indicating that orexin overactivity may worsen sleep disruption and further neurodegenerative processes in AD.34,35 In addition, excessive orexin activity may tilt the sleep-wake cycle toward increased wakefulness. 30 This, in turn, impairs the restorative functions of sleep and leads to further cognitive decline. 37 The findings corroborate that orexin dysregulation is not solely an outcome of AD pathology and, in fact, could be pathophysiologically involved in the worsening of sleep and cognitive deficits associated with the disease.32,33
Suvorexant: pharmacology and mechanism of action
Drug overview
The U.S. Food and Drug Administration (FDA) approved suvorexant in 2014 as a first-in-class dual orexin receptor antagonist (DORA) for the management of insomnia, specifically for patients experiencing difficulties related to sleep onset and/or sleep maintenance.43,44 As opposed to standard hypnotics working through central mechanisms involving wide-ranging neural regulation (e.g., GABA_A receptor modulators), suvorexant acts on the orexin (hypocretin) system, which plays a pivotal role in the management of alertness and arousal. 45 Suvorexant promotes the shifts and sustains the states of sleep by lowering wakefulness in individuals with insomnia through orexin signaling antagonism. 46 Given its distinct mechanisms and pharmacological properties, it is a valuable alternative treatment with a comparatively better profile of tolerability and safety than most traditional sleep medications. The medication is usually taken once nightly before sleep, and the dosage is adjusted based on clinical feedback and tolerability. 47
Mechanism
Suvorexant pharmacologically acts through reversible antagonism of orexin receptor 1 (OX1R) and orexin receptor 2 (OX2R), which, like most G-protein-coupled receptors, are activated by the endogenous neuropeptides orexin A and orexin B. 48 These receptors are present in the brain areas responsible for arousal, particularly the monoaminergic and cholinergic nuclei of the brainstem and hypothalamus. 49 Suvorexant facilitates the initiation and maintenance of sleep by lowering the sleep onset threshold and blocking the orexin-mediated activation of wakefulness circuits at both receptors.48,50 Suvorexant and other DORAs improve more than most conventional sleep-inducers (hypnotics) in the preservation of natural sleep architecture. They promote both NREM sleep and REM sleep, unlike GABAergic agents, which cause broad central nervous system (CNS) depression. The focused antagonism illustrates suvorexant's unique ability to center over sleep processes while having a lower likelihood of causing next day sedation, tolerance, and dependence in comparison to traditional sedative–hypnotics46,51
Additionally, orexin activity, which promotes wakefulness-related neuronal activity, may lead to heightened Aβ production and diminished clearance through the glymphatic system during sleep. 52 This correlates with the novel role of orexin pathways in neurodegeneration, through modulation of Aβ and tau pathology. 53 Suvorexant may reduce amyloid burden and indirectly alter tau phosphorylation by inhibiting OX1R and OX2R. Still, there is currently a lack of data supporting this claim, and most data come from small-scale preclinical and clinical studies. 54 While these findings suggest the possibility that suvorexant may play a disease-modifying role beyond sleep regulation, the evidence is still in its infancy, and further longitudinal studies involving large, adequately controlled samples are warranted54,55 (Figure 1).
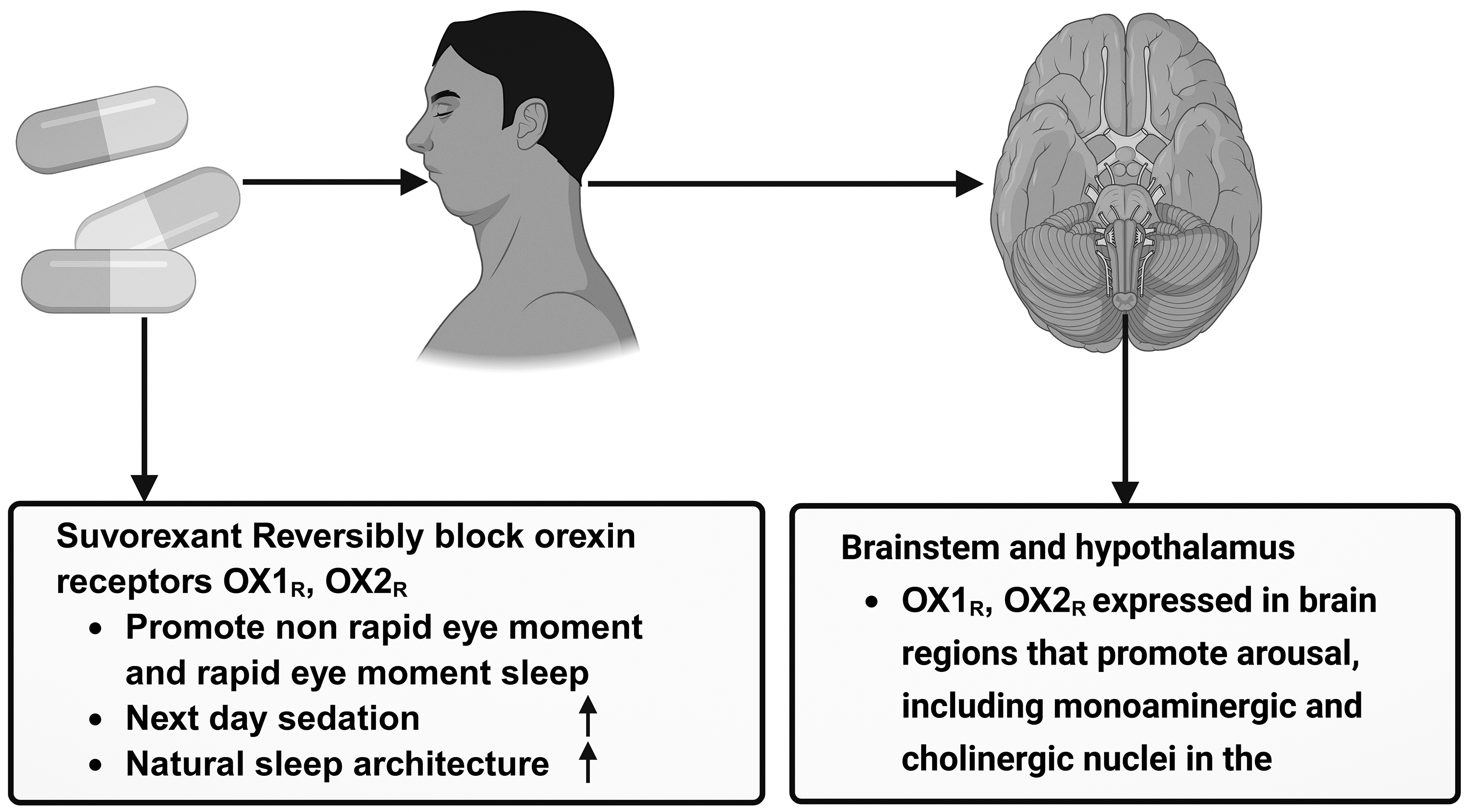
Mechanism of action of suvorexant on orexin signaling and sleep regulation. The depiction describes the main way in which suvorexant, a dual orexin receptor antagonist, facilitates sleep. Once suvorexant is taken orally, it is distributed to the brain where it reversibly inhibits the activity of the orexin receptor 1 (OX1R) and orexin receptor 2 (OX2R). These receptors are located in the arousal-promoting regions of the brainstem and hypothalamus, which include monoaminergic and cholinergic nuclei, and are involved in the promotion of alertness. Suvorexant lessens arousal signaling and promotes the initiation and maintenance of sleep by the inhibition of orexin A and orexin B-mediated excitation of circuits involved in the promotion of wakefulness. Notably, targeted antagonism of orexin A and B promotes non-rapid eye movement (NREM) and also rapid eye movement (REM) sleep while maintaining natural sleep architecture and reducing next-day residual sedation.
Relevance to AD pathophysiology
The Suvorexant's relation to AD goes beyond a sleep aid because of its effects on sleep-related mechanisms that are affected by AD neuropathology that are relevant to AD. Improved glymphatic clearance. Sleep assists the glymphatic system of the brain that clears out the byproducts of brain metabolism, including interstitial Aβ and tau.54,56 Enhanced sleep duration and quality may improve glymphatic clearance of toxic proteins associated with AD that are eluded to by suvorexant, possibly decreasing pathological burden over time. Models of sleep and its improvements give rise to more efficient clearance of amyloid species and point to a mechanism whereby modulation of sleep may impact the rate of progression of the disease.54,57 There is new clinical evidence that Orexin–AD Biomarker Modulation suggests showing that suvorexant may interact with AD-related biomarkers without changes in sleep parameters.56,58 In a NIH-supported small proof-of-concept study, suvorexant at higher doses, in cognitively healthy adults, resulted in acute reductions of CSF levels of Aβ, and phosphorylated tau, both of which are critically involved in the AD pathogenesis. 59 These effects occurred in the absence of changes in sleep quantity on the night of administration, suggesting suvorexant may involve other mechanisms, besides sleep, that affect amyloid and tau processes. 60 Although the possible long-term effects of these sudden changes in biomarkers are still unclear, the findings are consistent with the prediction that, in AD pathology, orexin modulation could work at the molecular level.35,37 Taken together, the findings support suvorexant as a potential candidate for further researching the treatment of AD, both as a means to facilitate the sleep disruptions that commonly occur in this population, and as a possible agent that could act on the modulatory/ upstream pathways associated with the amyloid and tau pathologies.54,61
Preclinical evidence
Animal models
Transgenic mouse models of AD in preclinical studies have shown that modulation of the orexin system can affect cognition and related neuropathology.32,37 In the APP/PS1 transgenic mouse model, where the human amyloid precursor protein and presenilin 1 are overexpressed, resulting in substantial Aβ pathology, suvorexant, a dual orexin receptor antagonist, improved cognitive deficits and behavioral test performance related to learning and memory.54,62,63 Most notably, suvorexant diminished Aβ deposition in critical brain regions such as the hippocampus and cortex and restored synaptic plasticity. This indicates that orexin blockade may facilitate positive changes in behavior as well as reduce hallmark AD pathologies in this model.58,64 Moreover, suvorexant reinstated long-term hippocampal potentiation (LTP) and normalized circadian alteration of phosphorylated CREB, indicators of the maintenance of some mechanisms involved in synaptic plasticity, of which the correlates are learning and memory.65,66 These findings confirm that suvorexant's neuroprotective effects in animal models include AD core pathology beyond just sleep modulation.58,67 It should be noted that all the evidence mentioned above is based solely on animal models, especially transgenic mice that replicate certain aspects of AD pathology. 68 Though some models provide useful mechanistic details on amyloid deposition, synaptic plasticity, and orexin-related cognition, the intricate and heterogeneous aspects of human AD remain poorly understood. 69 Therefore, the preclinical data offers compelling support for a possible disease modifying impact for orexin receptor antagonism, however, the ability to apply preclinical data to humans is uncertain, and proof of principle in clinical human studies is needed to test the validity of the data. 69
Mechanistic findings
The positive impacts of orexin receptor antagonism in models of AD seem to involve several different mechanisms. 70 In APP/PS1 mice, suvorexant improved circadian rhythms and synaptic plasticity in the hippocampus. AD models show LTP improvements, and LTP suppression is associated with cognitive impairment.54,63 Given that pCREB expression in the hippocampus returned to baseline levels after treatment, the re-establishment of circadian signaling implies that orexin blockade could facilitate the molecular mechanisms underlying memory consolidation and the resilience of neurons.71,72 Additionally, decreases in Aβ plaque burden after suvorexant treatment show that changes in orexin signaling can affect amyloid metabolism and aggregation, perhaps by improved sleep-related clearance mechanisms or by decreased wake-related generation of toxic peptides.48,73 The preclinical studies, when considered collectively, underscore the possible benefits of targeting the orexin system in AD. This is because dual orexin receptor antagonists improve functional outcomes and influence the important neurobiological changes associated with the progression of the disease.54,57,67
Clinical evidence and therapeutic potential
Sleep outcomes in AD patients
The effectiveness of suvorexant in improving sleep outcomes for patients with mild to moderate AD dementia and insomnia is documented in clinical research. 74 Suvorexant was shown to increase total sleep time (TST) significantly more than placebo in a randomized, double blind, placebo-controlled, polysomnography-based phase 3 trial with 285 subjects aged 50–90 with probable AD dementia and insomnia.75,76 After 4 weeks of treatment, the suvorexant group showed a least squares mean improvement in TST from baseline of 73 min compared to 45 min in the placebo group (difference = 28 min; p < 0.01).75,77 Suvorexant also decreased wake after sleep onset (WASO), indicative of improvements in sleep maintenance throughout the night. Thus, suvorexant enhances sleep duration and continuity in AD patients with insomnia and no cognitive worsening associated with the treatment.50,78 The studies referenced here are human clinical research, mostly randomized controlled trials carried out on patients with clinical diagnoses of AD and comorbid insomnia. 79 The aforementioned studies provide relevant and direct evidence of the effectiveness and safety of suvorexant for improving sleep in this patient population. 80 It should, however, be noted that the main outcomes evaluated involve sleep-related parameters, and there is still a dearth of solid human studies on the long-term impact of disease progression, cognition, or the primary core AD neuropathology.81,82 Therefore, although clinical evidence strongly supports symptomatic benefits on sleep, additional longitudinal studies are warranted to assess whether these improvements may result in broader neuroprotective or disease-modifying effects in patients with AD. 83
FDA approval and clinical guidelines
In light of the recent positive results from clinical trials, the U.S. Food and Drug Administration (FDA) updated the prescribing information for the drug suvorexant (Belsomra) and incorporated a new indication for the treatment of insomnia in patients with mild to moderate AD.84,85 The phase 3 polysomnography findings illustrating AD patients’ TST and WASO improvements relative to placebo drove this regulatory decision.74,86 The revised labeling represents an advancement in suvorexant's sleep disturbance claim, specifically targeting the AD population who suffer most commonly and problematically from insomnia and fragmented sleep.56,87
Biomarker effects
Improving sleep symptoms aside, suvorexant is now reported to have possible acute effects on certain AD-related biomarkers.74,88 In one such case, a small randomized controlled study, with cognitively unimpaired 25 participants aged 45 to 65 years, reported suvorexant at higher doses to be associated with reduced levels of CSF Aβ and phosphorylated tau proteins, both of which are central to the AD pathology. 59 Changes occurred within hours of administration and were not accompanied by measurable increases in sleep time. This suggests that orexin receptor antagonism may act on interim biomarker mechanisms or dynamics, beyond simple sleep extension. While these results are preliminary and derive from short-term dosing in healthy subjects, they are valuable proof of concept data for possible biomarker modulation by orexin antagonists that may impact AD pathophysiology.46,58,89 It is critical to note that the identified reductions in biomarkers were of an acute and short-term nature, occurring only in the specific time window following a single or short dosing regimen. 90 There is insufficient evidence to show whether these outcomes can be maintained following repeated use and whether long-term clinical advantages, such as a reduction in the rate of cognitive decline or the progression of the disease, are attainable. 91
Furthermore, the generalizability of these findings to individuals with AD is restricted by the small sample size and the inclusion of cognitively normal participants. Although the rapid modulation of Aβ and tau dynamics is intriguing, longitudinal studies are needed to assess the maintenance and the time-sustained therapeutic relevance of these acute biomarker changes, if any, in the context of neurodegenerative diseases. 92
Sleep architecture
Research on suvorexant and its effect on sleep architecture shows it increases total sleep time but does not significantly change the sleep stage architecture in patients with AD. 74 Polysomnography data is being processed from the same phase 3 AD sleep trial. Suvorexant increased TST by 28 min compared to placebo at the end of the treatment period, but did not result in meaningful changes in the amount of sleep in the REM, N1, N2, or N3 sleep stages.50,93 Likewise, there were no statistically significant changes regarding the time taken to reach REM sleep. The data indicating preserved architecture of sleep suggests that suvorexant improves sleep quantity while keeping the balance of the sleep stages intact. This sets suvorexant apart from many of the sedative-hypnotics that disrupt the microstructure of sleep.50,94
Safety and tolerability
Numerous clinical studies have established that suvorexant has a tolerable safety and tolerability profile with older individuals, including patients with AD. 48 In the phase 3 trial involving AD and insomnia, suvorexant was mostly well tolerated, and the most frequently occurring adverse event was sleepiness. 48 In both treatment groups, the overall incidence of sleepiness was low (≈4.2% in the suvorexant group and 1.4% in the placebo group), and no treatment group experienced adverse event-related withdrawals.48,75 There was no decline in neuropsychiatric symptoms and cognitive function during the trial period. 95 This is consistent with general clinical findings on suvorexant's use in general insomnia populations, where, for these patients, the most common, mild adverse events included dizziness, headaches, and excessive daytime sleepiness, and discontinuation due to side effects was rare. Suvorexant's side effect profile suggests that, in older patients with cognitive impairment, and with regular clinical monitoring, the drug can be used to provide relief from sleep disturbances.45,96 Suvorexant shows a good safety and tolerability profile even with long-term use and little evidence of tolerance development over the usual treatment period. 97 Long-term studies show a low occurrence of adverse events, and of those that do occur, most are mild and transitory, such as somnolence, dizziness, and headache. 98 Notably, during treatment, no major cognitive deterioration or aggravation of neuropsychiatric symptoms have been seen in older adults or in patients with AD. 99 However, an increased level of observation is warranted for elderly patients who are prescribed polypharmacy due to the various medication interactions and dosages that need to be managed. 100 Including extended follow-up periods in future studies will provide insight into the long-term safety, tolerability, and potential cumulative effects of suvorexant in susceptible patients. 101
Integrative mechanisms: beyond sleep
Glymphatic clearance
One of the mechanisms by which suvorexant may influence the pathology of AD is possible modulation of sleep-dependent glymphatic clearance that is enhanced with the removal of neurotoxic proteins. 54 The glymphatic system is a network system across the brain that consists of channels that are located perivascularly and remove interstitial solutes, including Aβ and tau, but are only active during slow-wave sleep.102,103 Suvorexant and similar dual orexin receptor antagonists may increase the efficiency of neurotoxic proteomics by clearance pathways, neurodegeneration, promoting the accumulation of toxic proteins, and by facilitating consolidated and extended sleep. 104 The mechanistic relationship between sleep modulation and the pathophysiology of AD was hypothesized and then demonstrated via experimental studies in rodent models that showed improved sleep duration and quality, enhanced glymphatic flux, and less amyloid deposition. 105
Direct modulation of pathological proteins
Apart from sleep-mediated clearance, orexin antagonism might also directly act on AD-related pathological proteins. 106 In early-stage human research, acute administration of suvorexant showed detectable decreases in CSF Aβ and phosphorylated tau, despite no notable differences in the total sleep time.54,107 Theoretically, orexin signaling may impact amyloid and tau metabolism via mechanisms that do not include orexin-enhanced sleep, and may include direct alterations to neuronal firing, synaptic release of amyloid precursor proteins, or modulation of the protein aggregation pathways. 36 It should also be noted that the studies referenced above examined changes in blood biomarkers in cognitively healthy individuals. 108 Therefore, the permeability biomarkers studied may be inapplicable in AD conditions, in which the pathology of amyloid deposition, tau aggregates, and neuron death is already present. 109 The translational relevance of these findings remains to be seen, as the disease-specific elements may influence the degree of response to orexin receptor antagonism. 39 Therefore, future studies within clinically confirmed AD populations are warranted to assess the possibility of similar effects on Aβ and tau, along with the therapeutic relevance of such effects within the context of AD-related neurodegeneration. 110
Immunomodulation and neuroinflammation
Prolonged neuroinflammation in AD is worsened by the disruption of orexin signaling, which is thought to engage in cross-talk with inflammatory processes in the CNS.37,111 Orexin antagonism may mitigate neuroinflammation by reducing prolonged wakefulness, which is linked to microglial activation and the release of inflammatory cytokines.36,37 In preclinical research, the mechanisms that promote sleep and the blockade of orexin have demonstrated a reduction in neuroinflammatory markers within the hippocampal and cortical areas. This suggests a possible pathway that aids in neuroprotection 36 (Figure 2). Orexin modulation and its corresponding effects on the immune system concerning AD have pathways that remain largely unexplored and, as such, require more mechanistic studies to understand how orexin-targeted therapies may work alongside other anti-inflammatory strategies. 112
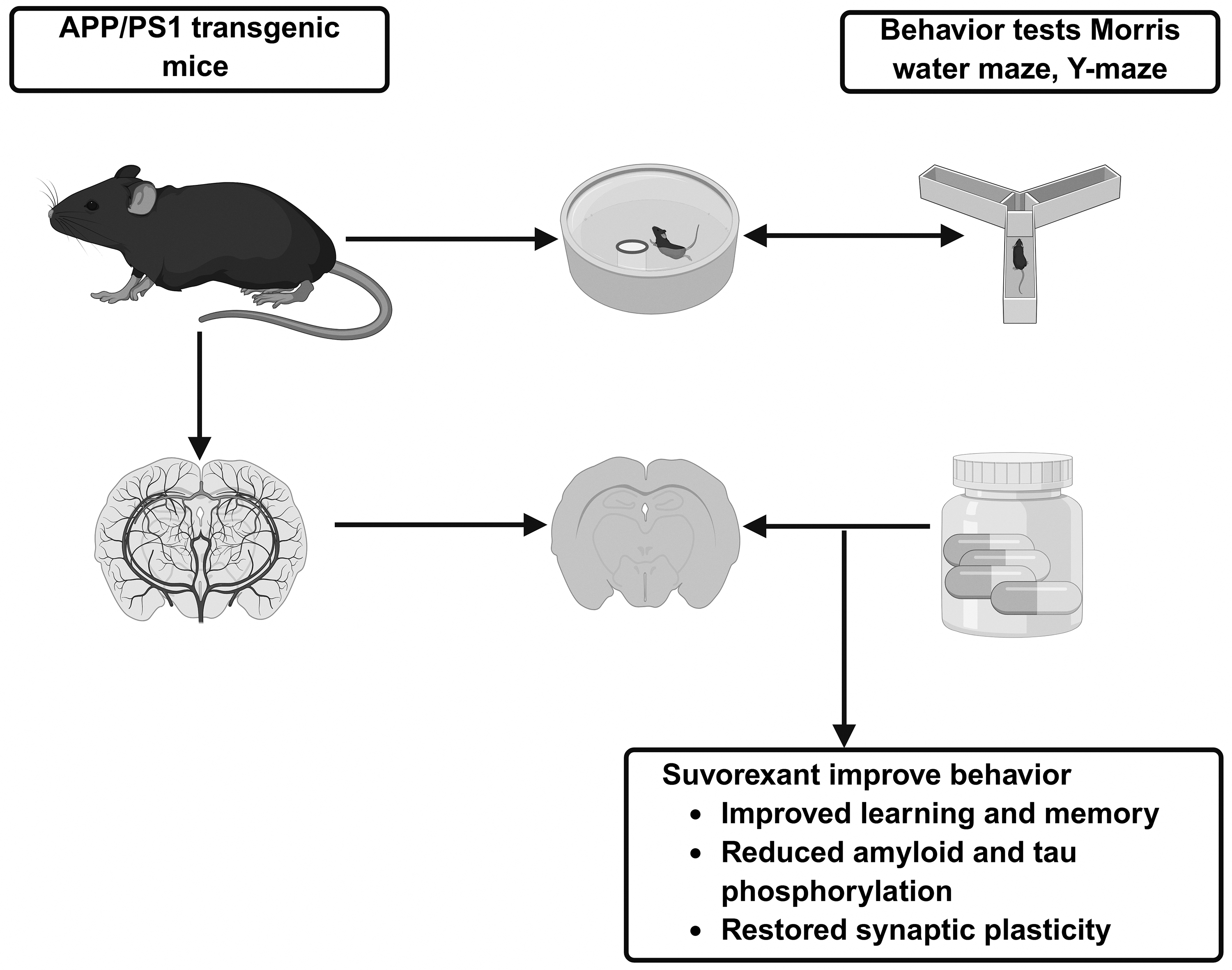
Suvorexant alleviates Alzheimer's-like phenotypes in APP/PS1 mice. Suvorexant, a dual orexin receptor antagonist, has been shown to improve cognitive function and reduce certain aspects of neuropathology in a mouse model of Alzheimer's disease (APP/PS1). Results from the Morris water maze and Y-maze tests suggest that chronic suvorexant administration enhances learning and memory, while also decreasing the amyloid-β burden, tau phosphorylation, and restoring expression of certain synaptic plasticity markers relative to vehicle-treated controls.
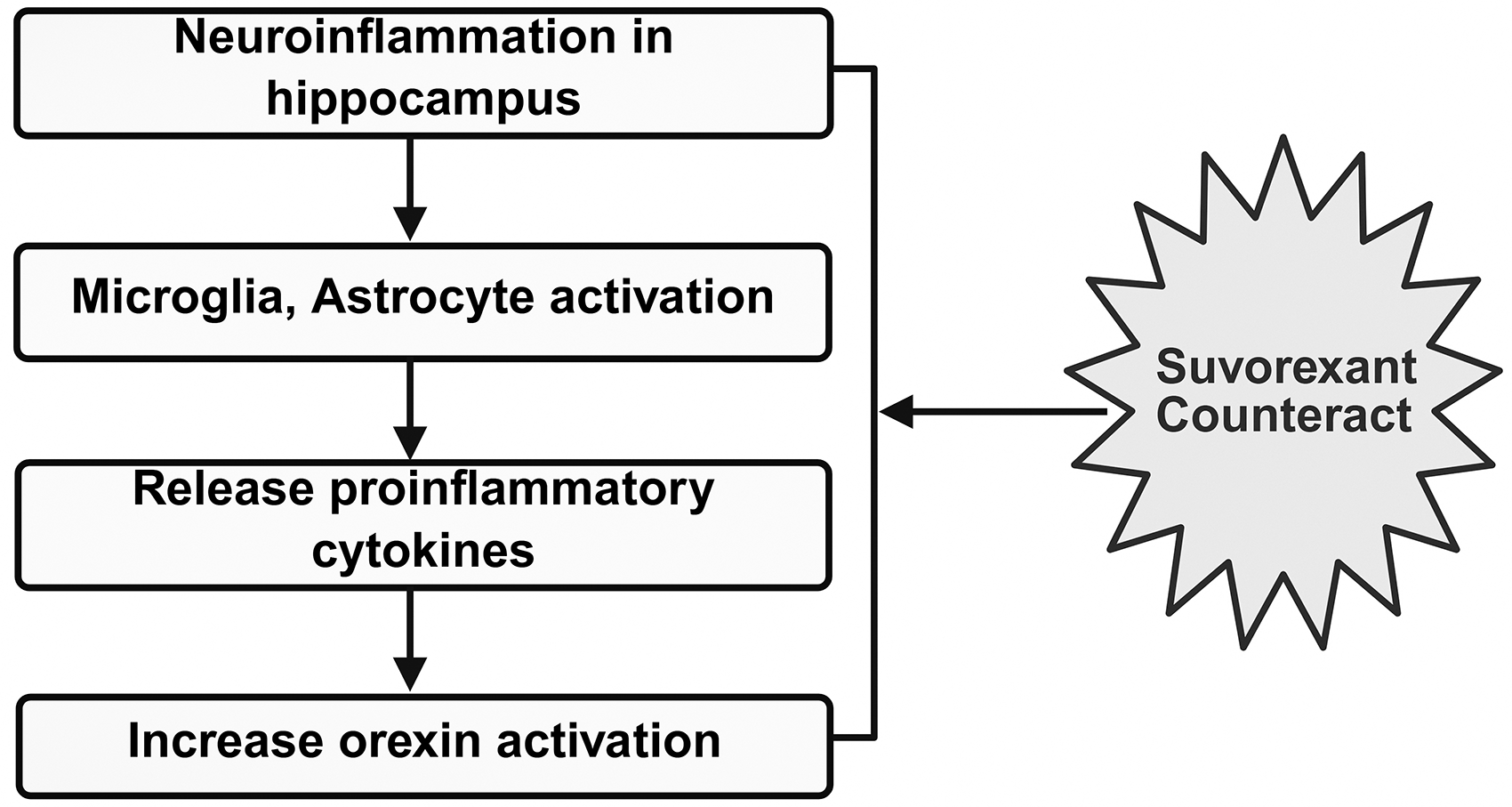
Suvorexant modulation of orexin-linked neuroinflammation. This is the proposed interaction between neuroinflammation in the hippocampi and orexin signaling, and the possible opposing action of suvorexant. In the case of Alzheimer's disease, neuroinflammation in the hippocampus triggers the activation of microglia and astrocytes, which, in turn, secrete proinflammatory cytokines. It has been demonstrated that these inflammatory mediators increase activity in the orexin system, resulting in a positive feedback loop that facilitates arousal, disrupts sleep, and stimulates additional neuroinflammatory activity. Suvorexant is a dual orexin receptor (OX1R and OX2R) antagonist that acts by suppressing orexin-mediated signaling. This would reverse the facilitating effect of orexin on inflammation-related hyperarousal. Accordingly, suvorexant would help to mitigate the neuroinflammatory burden and improve the regulation of sleep by reducing inflammation in the hippocampus.
Comparisons with other orexin receptor antagonists
Lemborexant and daridorexant
Along with suvorexant, lemborexant, and daridorexant, other DORAs are also studied for insomnia and possibly modulation of AD pathology.43,45 As with suvorexant, these agents antagonize both OX1R and OX2R, facilitating sleep onset and maintenance without causing global CNS depression (Figure 3).45,46 Lemborexant and daridorexant have been shown to improve sleep duration, decrease WASO, and preserve sleep architecture the same way suvorexant does. 113 Direct evidence in AD populations is still limited, but there is interest in the potential of the medications to improve sleep quality and glymphatic clearance of Aβ and tau. 114 Moreover, the pharmacokinetic profiles vary slightly: lemborexant has a quicker time to peak plasma concentration compared to daridorexant, whose half-life is shorter, possibly diminishing next-day residual effects.85,113 These factors may affect tolerability and treatment selection in the older demographic suffering from AD. 115
Selective orexin receptor antagonists
Selective orexin receptor antagonists (SORAs) are new pharmacological candidates that either selectively antagonize OX1R or OX2R (as opposed to both receptors).116,117 This selectivity could help refine the regulation of sleep-wake cycles, possibly having different effects on AD pathology compared to dual antagonists. 118 Preclinical studies indicate that while NREM (non-rapid eye movement) sleep is critical for glymphatic clearance, OX2R antagonism promotes sleep, and OX1R blockade may affect REM sleep and arousal circuits. 119 Targeting these receptors differentially is likely to be beneficial to maximize treatment efficacy and minimize treatment-related adverse effects, like excessive daytime sleepiness. 120 Even though there is only a limited amount of clinical data available on AD populations, future research hopes to determine if SORAs offer individualized adjustments on orexin dependent pathways with the possible benefits of adjusting biomarkers and/or improving cognitive functioning. This research furthers the potential of orexin-based therapies for sleep and neurodegenerative disorders. 46
Integrative mechanisms: beyond sleep
Aside from regulating sleep-wake patterns, new studies show that orexin signaling and its pharmacological modulation by suvorexant may affect several interrelated aspects of AD pathophysiology, including glymphatic clearance, neuroinflammation, and the metabolism of amyloid. 121 The glymphatic system, most active during slow-wave sleep, plays a critical role in the removal of Aβ and other neurotoxic proteins. The glymphatic system is a network of pathways around the brain's blood vessels. The glymphatic system is involved in the clearance of metabolic waste and plays a critical role in the removal of neurotoxic proteins. 122 Sleep disruption, especially reduced slow-wave sleep, is associated with glymphatic dysfunction and increased amyloid buildup. 22 By potentially improving the removal of pathological proteins, orexin antagonists may improve the efficiency of glymphatic clearance. 22 In parallel, neuroinflammation is a critical driver of AD progression, characterized by microglial activation and astrocyte reactivity, along with the secretion of pro-inflammatory cytokines. 123 The involvement of orexin signaling in the CNS's inflammatory response suggests that increased wakefulness and altered sleep patterns have a pro-inflammatory effect. 124 The pharmacological inhibition of orexin pathways may reduce neuroinflammatory signaling by directly or indirectly restoring sleep homeostasis/or directly modulating microglial activity, and/or altering cytokine levels. 39 While there is preclinical evidence that supports this association, clinical corroboration is still lacking and needs to be pursued further. 125
Additionally, neuronal activity and the dynamics of the sleep-wake cycle appear to closely dictate the metabolism of amyloid. 26 While sleep aids in the clearance of Aβ, waking and the resultant synaptic activity boost its production. 126 Arousal-promoting orexin neurons have been demonstrated to modulate interstitial fluid levels of Aβ, and greater orexin activity has been associated with greater amyloid accumulation. 53 Mechanistic studies provide, for the first time, proof of concept for the association between orexin antagonism and Aβ homeostasis. It shows that orexin signaling suppression is associated with reduced Aβ accumulation. 70 The majority of existing evidence comes from short-term studies in humans and studies in animals. Therefore, the long-term effects of amyloid deposition and cognitive outcomes in AD are yet to be determined. 127 Together, these integrative mechanisms indicate that orexin receptor antagonists may have a therapeutic potential that goes beyond sleep symptom alleviation, and potentially, in AD, may impact fundamental underlying mechanisms. 32 The large majority of the current evidence base is of a preliminary nature and additional longitudinal and translational studies are warranted to ascertain possible disease modification targetable pathways. 128
Challenges and controversies
Heterogeneity of human biomarker data
In spite of the encouraging data from preclinical studies and the early stages of clinical studies, the research examining levels of orexin in CSF in patients with AD reports varied findings. 34 While some studies report increased levels of orexin in mild to moderate AD with association to sleep fragmentation and cognitive decline, others report no difference compared to age-matched controls. 58 The varied results may be attributed to methodological factors such as the time of sampling of the CSF, sensitivity of the assay, stage of the disease, and characteristics of the cohort. 129 Orexin dysregulation, sleep impairment, and AD pathology have unclear relationships, given that human biomarker data have substantial variability. This demonstrates that defining orexin as a biomarker requires standardization of measurement techniques and greater longitudinal studies. 35
Long-term cognitive outcomes
While suvorexant enhances certain sleep parameters in short-term studies, data regarding its impact on cognition and the progression of AD in the long-term are scarce. 60 The majority of clinical studies have centered on sleep outcomes within the 4–12 week timeframe, and thus far, there is insufficient data to ascertain if extended periods of orexin receptor antagonism have the potential to mitigate cognitive decline or diminish amyloid/tau burden in the human brain. 57 In addition to this, there is still much to clarify in terms of the effects of chronic use on circadian rhythm, daytime alertness, and the compensatory changes in orexin signaling. Knowledge gaps of this sort require longitudinal, placebo-controlled studies with clear cognitive and biomarker endpoints. 130
Optimal target populations
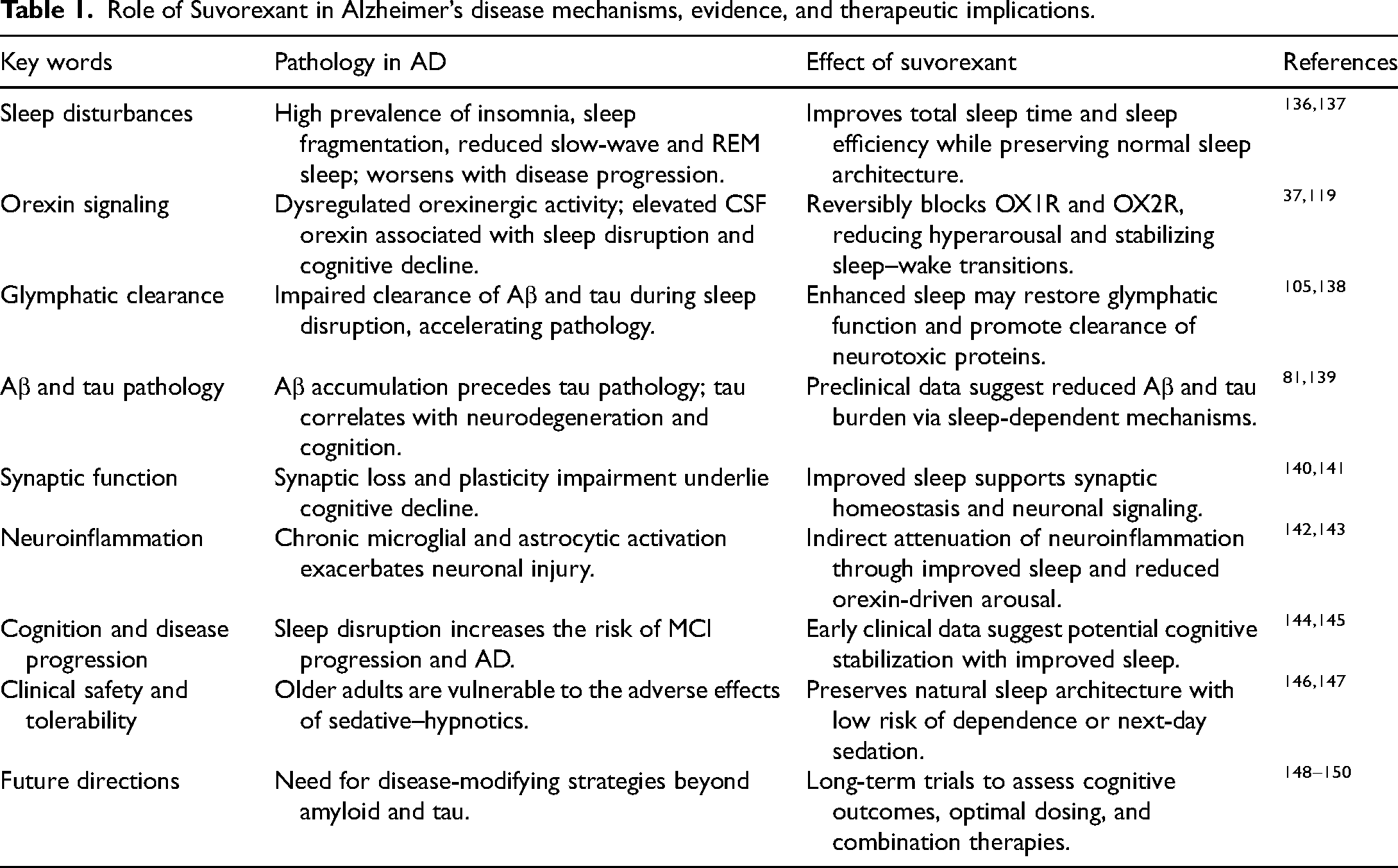
It remains unanswered regarding which specific subgroups of AD gain the highest advantages from suvorexant or other orexin-targeted treatments. 131 Factors like genetics, such as being an APOE4 carrier, the different stages of the disease (preclinical, MCI, or established AD), sleep quality before treatment, as well as comorbidities, may impact effectiveness and tolerability. 132 The therapeutic outcomes can be optimized, and the pathways for individualized treatment can be defined by the stratification of patients based on the articulated variables. Furthermore, the varying responses to DORAs as opposed to SORAs may help in further improving patient stratification.51,133 Future studies may identify response profiles using genetics, sleep phenotype, and biomarker data, which may inform targeted interventions.134,135 (Table 1)
Role of Suvorexant in Alzheimer’s disease mechanisms, evidence, and therapeutic implications.
Future directions and research priorities
Large-scale randomized controlled trials
Although short-term trials show that suvorexant enhances sleep for patients with mild-to-moderate AD, no long-term data address the cognitive impacts and/or disease-modifying potential of suvorexant. 54 Suvorexant warrants large-scale, multi-center randomized controlled trials (RCTs) with clinical (cognition, function) and biomarker data (Aβ, tau, and neuroinflammation), as cognitive and functional outcomes remain unknown. 132 extended follow-up periods that are longer than 12 months will be essential in establishing whether long-term antagonism of orexin receptors will be able to halt cognitive decline, pathological burden, or the progression of MCI to AD dementia, as suvorexant may be the first chronic orexin receptor antagonist to be tested. 121 If positive, it will likely confirm suvorexant's therapeutic effect as a disease-modifying treatment (beyond the symptomatic treatment of insomnia), providing evidence that targeting the orexin system can influence core pathological processes such as Aβ accumulation, tau pathology, and neuroinflammation, rather than solely improving sleep-related symptoms. 54
Mechanistic studies
Although there is growing evidence connecting orexin signaling and the pathology of AD, some significant mechanistic inquiries still require an effort to be addressed. 54 Future research should investigate orexin's role in neuroinflammation, glymphatic clearance, plasticity of the synapses, and the aggregation of proteins, preferably in human and preclinical model studies. 57 Application of advanced imaging methods, including PET tracers for amyloid and tau, coupled with biomarker analysis in CSF and blood, may help to specify whether orexin antagonists influence the dynamics of pathological proteins directly, or through the facilitation of sleep. 57 Moreover, studies should investigate the potential influence of circadian rhythm shifts and their relationships with cognition, as this may help to delineate the activity of orexin antagonists in the context of chronotherapy. 54
Combination therapies
Synergistic strategies that integrate pharmacologic and non-pharmacologic methods may maximize the outcomes of treating AD. 151 Examples of such methods are the combination of suvorexant and lifestyle interventions, such as sleep hygiene, exercise, and light therapy, that have been shown to enhance circadian stability and glymphatic function. 22 Also, the combination with disease-modifying therapies (e.g., anti-amyloid or anti-tau monoclonal antibodies) may have additive or synergistic effects as they may enhance sleep-dependent clearance of toxic proteins while directly addressing some of the pathologies. 62 For interventions such as suvorexant, lifestyle changes, and other pharmacological treatments to work synergistically to improve sleep, enhance glymphatic clearance, reduce neuroinflammation, and ultimately improve cognitive function in people who have AD, optimal clinical assessment will be critical in determining the best combination of timing, dosing, and patient selection to maximize the potential benefits and minimize the risks associated with these combination strategies. 152 Furthermore, a broader range of strategies for addressing sleep disturbances in AD should be considered. 81 Pharmacologic options such as melatonin and trazodone may improve sleep quality and regulate the circadian rhythm. Their impact may be limited by efficacy side effects and inconsistent results. 153 Due to their safety and broader positive effects on circadian and behavioral regulation, non-pharmacologic interventions such as cognitive behavioral therapy for insomnia, structured light exposure, increased physical activity, and improved sleep hygiene are important first-line approaches. 154 Moreover, other DORAs, such as lemborexant and daridorexant, have shown similar or even better sleep outcome results. However, new data have shown possible variations in pharmacokinetics, receptor selectivity, and next-day residual effects. 45 Still, the existing debate on these alternatives fails to engage deeply, and contrasting the effectiveness, safety, and relevance of these alternatives as applicable to AD populations, would allow for a more robust assessment of the therapeutic approaches to sleep disturbance problems within this framework. 155
Recommended dosing of Suvorexant (10–40 mg) in adults
Suvorexant is a DORA that is approved for use in the treatment of insomnia. Currently, it is being studied for potential use in sleep disturbances related to AD. 121 Clinical trials and prescribing data show that the therapeutic dose range for adult patients is 10–40 mg, taken orally before sleep. 156 The selection of dose is guided by balancing efficacy in facilitating sleep against safety and tolerability. 156 The recommended initial dose for most patients is 10 mg at bedtime. 157 This dosage has been shown to have a positive effect on sleep onset and maintenance in adults, while reducing next-day somnolence, impaired alertness, and other CNS adverse reactions. 158 Ten milligrams is viewed as safe and effective for initiation for older patients (≥65 years) and patients with liver impairment. 97 For persistent sleep disturbances after a week at a dose of 10 mg, clinicians may choose to increase the dosage to 15 mg or 20 mg. 159 Clinical trials involving adults with insomnia have shown that within this dosage range, there is a marked improvement in TST and a reduction in WASO, accompanied by a favorable tolerability profile.47,160 When considering a medication that aids sleep initiation and maintenance, if a concern about substantial next-day sedation, an intermediate dose is often enough. 30–40 mg doses have been used for instances of severe, refractory insomnia. Higher doses have been shown to of sleep continuity, especially for patients that experience frequent awakening throughout the night, shift sleep periods. 160 Nonetheless, such doses carry a greater likelihood of adverse effects, such as drowsiness, light-headedness, and the possible development of complex sleep-related disorders (e.g., sleepwalking). 161 Older adults and those with comorbidities or on polypharmacy should exercise caution. 100 Suvorexant is rapidly absorbed, with peak plasma concentrations occurring within about 2 h. It has a half-life of about 12 h which not only supports its effects throughout the night but also requires thoughtful dose selection to avoid next-day sedation 48 . Hepatic impairment may increase plasma exposure, and therefore lower starting doses and slower titration may be justified. For patients who have MCI or early-stage AD, optimal dosing should be tailored. 162 Doses of 10–15 mg are less likely to induce falls, confusion, excessive sedation, etc., and may be enough to induce sleep and, in turn, promote glymphatic clearance of Aβ and tau. In research and long studies targeting AD pathology, it becomes necessary to properly titrate and monitor cognitive and functional outcomes to ensure safety and efficacy are properly balanced.54,163
Conclusion
Suvorexant holds some promise for treating insomnia in AD and might also impact the pathology of AD via modulation of the orexin system. Transgenic mouse model preclinical studies show that dual orexin receptor antagonism results in improved sleep and circadian rhythmicity, and also enhances some forms of synaptic plasticity and reduces Aβ. Early studies with humans showed some sleep continuity improvements with some hypothesized acute decreases in amyloid and tau levels in the CSF. Regardless of the positive discoveries, the existing proof base continues to be limited, with small-scale and short-term studies, varied biomarker information, and sparse long-term cognitive results. Thus, comprehensive longitudinal studies, driven by biomarkers, are necessary to determine whether suvorexant will provide AD patients relief from insomnia along with disease-modifying benefits, and to ascertain which patient subsets will gain the most from orexin-targeted treatments.
Footnotes
Acknowledgements
The authors gratefully acknowledge the Center of Advanced Scientific Research and Publication (CASRP) for English language editing.
Language-editing tools were used to improve clarity and consistency. All scientific content, interpretation, and final responsibility rest with the authors.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.