
Abstract
Background
Hypertension (HTN) is a major modifiable risk factor associated with cognitive decline including Alzheimer's disease (AD), which continues to be the leading cause of dementia and death in the United States (U.S.). However, the national mortality burden of coexisting AD and HTN across demographic and geographic groups remains poorly defined.
Objective
We aimed to study these trends to provide insights for better prevention, management, and policy planning.
Methods
A retrospective analysis was conducted using the CDC WONDER Multiple Cause-of-Death database (1999–2023), focusing on adults aged ≥65 years with AD and HTN. Temporal trends were assessed using Joinpoint regression to estimate annual percent changes. Mortality patterns were examined by sex, race, region, urban-rural status, state, and place of death.
Results
Between 1999 and 2023, 504,360 deaths among U.S. adults aged ≥65 years listed both AD and HTN on death certificates, with age-adjusted mortality rates rising from 14.5 to 60.0 per 100,000. Women consistently experienced higher mortality than men (67.5 versus 48.1 per 100,000 in 2023). Non-Hispanic African American adults had the greatest overall burden (57.1) among races. Geographically, mortality was highest in non-metropolitan areas (48.7) and the West region (52.6), More than half of all deaths occurred in nursing homes or long-term care facilities.
Conclusions
Mortality for coexisting AD and HTN has quadrupled in the U.S. over the past two decades with substantial variations across groups, highlighting the substantial burden of deaths where AD and HTN coexist and the importance of effective HTN control and dementia care across the lifespan.
Keywords
Introduction
Alzheimer's disease (AD), a neurodegenerative disorder, is the most common cause of dementia in the elderly population, with about 10% of the United States (U.S.) population aged 65 and above suffering from it. 1 Similarly, hypertension (HTN) poses a considerable healthcare burden on the world economy. The U.S. national database reports an average yearly adjusted extra cost of $1920 for patients with HTN compared to their non-hypertensive counterparts, 2 and the American Heart Association estimates that the direct cost of HTN in the U.S. will exceed $200 billion by 2030. 3
The U.S. population is aging, and increasing AD deaths are noted every year, necessitating the urgent need to understand factors contributing to increased mortality among this vulnerable population. 4 HTN has been labelled as the most common modifiable risk factor for cognitive decline including AD, with studies suggesting it as the most significant as well.5–8 Mid-life HTN increases the risk of cognitive decline, stroke, vascular dementia and AD. Control of AD through BP management has been a topic for debate with conflicting opinions.5,7 However, several trials such as SPRINT-MIND have shown that blood pressure control reduced cognitive impairment, suggesting that optimum HTN management can influence cognitive outcomes.7,9 Several mechanisms have been proposed to explain the observed link between AD and HTN, including genetic links (pleiotropy), 1 altered molecular signalling, 10 and increased amyloid deposition and neurofibrillary tangling with HTN, both recognized as the pathological hallmarks of AD. 11
The association between these two highly prevalent diseases needs to be studied in more detail, particularly in the context of aging populations and increasing multimorbidity.7,12 Our study aims to analyze the CDC WONDERBASE data from the last two and a half decades to identify HTN as a common comorbidity contributing to mortality burden in people with AD, understand the emerging patterns of mortality trends, unravel the eluding mysteries of this complex relationship and provide insights for targeted interventions and improved management. This will provide epidemiologic insights relevant to prevention, surveillance and improving health policy.
Methods
Study setting and population
In this retrospective cohort study, data were extracted from the CDC WONDER (Centers for Disease Control and Prevention Wide-Ranging Online Data for Epidemiologic Research) Multiple Cause-of-Death database, which compiles information from U.S. death certificates across all 50 states and the District of Columbia. Death certificates with AD and HTN listed anywhere on the death certificate, either as the underlying cause of death or as contributing causes of death, in adults aged ≥65 years, were analyzed from 1999 to 2023 using the following International Statistical Classification of Diseases and Related Health Problems-10 Revision (ICD-10-CM) codes: G30 for AD and I10-I15 for HTN (Supplemental Table 1). The same ICD-10 codes have been used to identify AD13,14 and HTN15,16 in previous studies. This case definition identifies deaths in which AD and HTN co-occurred on the death certificate and does not represent a clinical cohort of patients with diagnosed AD. Accordingly, this analysis describes population-level mortality patterns rather than the individual-level effect of HTN on survival among patients with AD. This study was exempt from review by the local institutional review board because it utilized de-identified, publicly available data. Reporting followed STROBE (Strengthening and Reporting of Observational Studies in Epidemiology) guidelines.
Data abstraction
The abstracted dataset included information on state, year, region, population size, demographics, location of death and urban-rural status. Demographics consisted of race/ethnicity, sex, age, and site of death. The location of death was categorized into medical facilities (outpatient, emergency room, inpatient, death on arrival, or status unknown), home, hospice and nursing home/long-term care facility. Race and ethnicity were categorized using CDC WONDER classifications based on Office for Management and Budget standards as follows: non-Hispanic (NH) White, NH Black or African American, Hispanic/Latino, NH American Indian/Alaska Native (AIAN), and NH Asian/Pacific Islander. 17 Urban–rural status followed the 2013 National Center for Health Statistics classification, grouping counties into metropolitan (large central metro, large fringe metro, medium metro, small metro) and non-metropolitan (micropolitan, noncore regions). 18 Regional distribution was based on the U.S. Census Bureau divisions: Northeast, Midwest, South, and West. 19
Statistical analysis
Mortality rates were expressed as both crude mortality rates (CMRs) and age-adjusted mortality rates (AAMRs) per 100,000 individuals. Crude rates were obtained by dividing the annual number of relevant deaths by the mid-year U.S. population, while AAMRs were derived using the direct standardization method with the 2000 U.S. standard population as reference. 20 Rates were restricted to individuals aged ≥65 years and were calculated using the corresponding U.S. population as the denominator, rather than being limited to individuals with AD. To assess temporal variations, we applied the Joinpoint Regression Program (version 5.4.0, National Cancer Institute) to estimate annual percent changes (APCs) in mortality, along with their 95% confidence intervals (CIs). 21 This method detects significant inflection points where trends in AAMRs shift over time by fitting log-linear regression models. A change in mortality was considered statistically meaningful when the slope of the regression line differed significantly from zero, with statistical significance defined as p < 0.05.
Results
Overall mortality trends
A total of 2,936,795 AD-related deaths occurred between 1999 and 2023, among which 504,360 (17.2%) had HTN coded as an underlying or contributing cause. Annual descriptive analyses showed a steady rise in the proportion of AD deaths with coexisting HTN relative to AD deaths alone (from 6.45% in 1999 to 23.24% in 2023), consistent with an increasing burden of comorbidity over time (Supplemental Table 2, Supplemental Figure 1). The overall AAMR was 14.51 (95% CI: 14.10–14.91) per 100,000 population in 1999 and rose astonishingly to 60.00 (95% CI: 59.40–60.70) in 2023 (Figure 1, Supplemental Table 2). Trend analysis depicted that mortality rose sharply in the early years of the study period, increased more gradually through the mid-2000s, remained relatively stable until the mid-2010s, and then increased again through 2021 before a modest, non-significant decline through 2023 (Table 1, Figure 2, Supplemental Table 3).
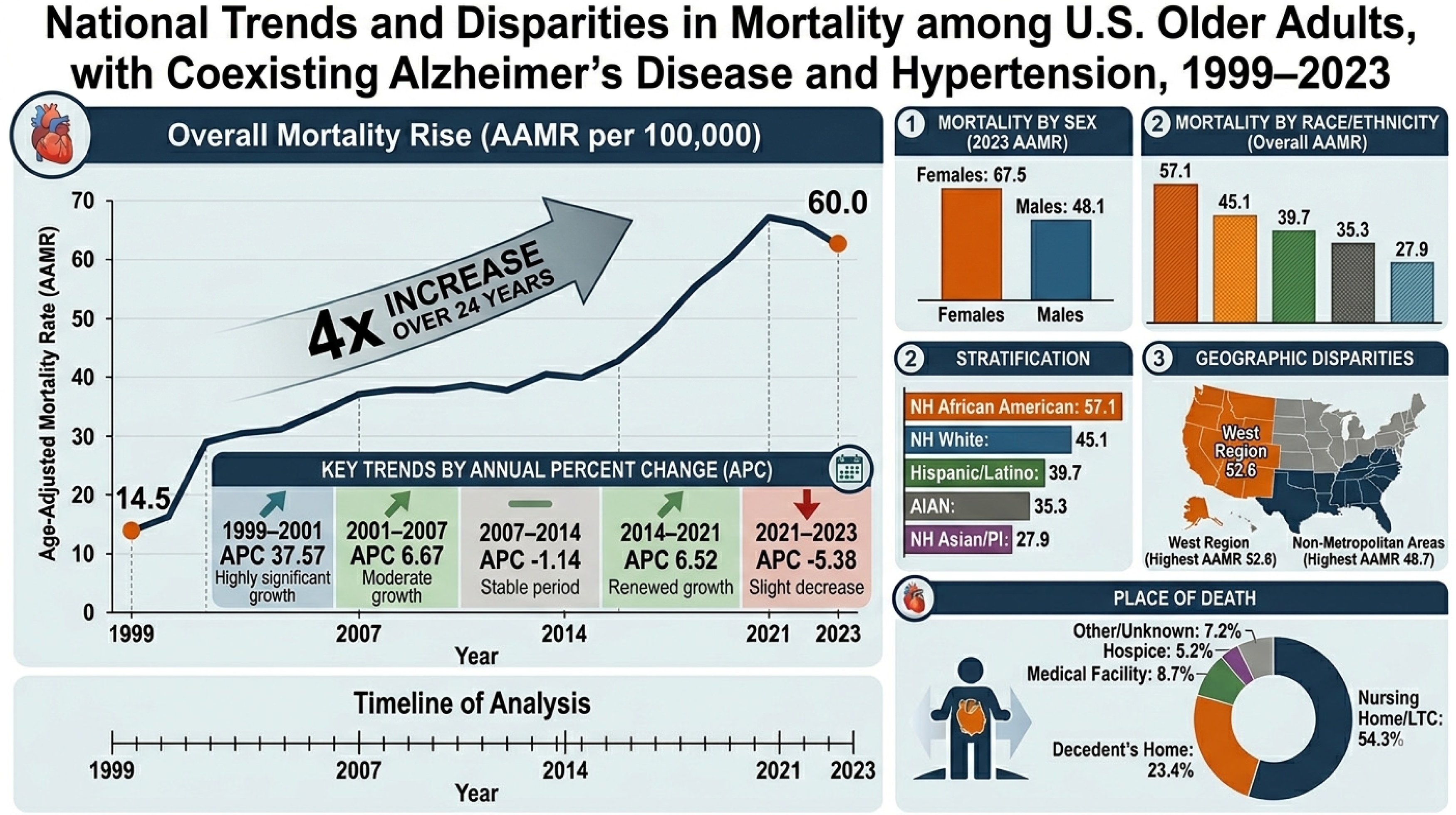
Graphical overview of national mortality trends and demographic disparities among older adults with coexisting Alzheimer's disease and hypertension, United States, 1999–2023.
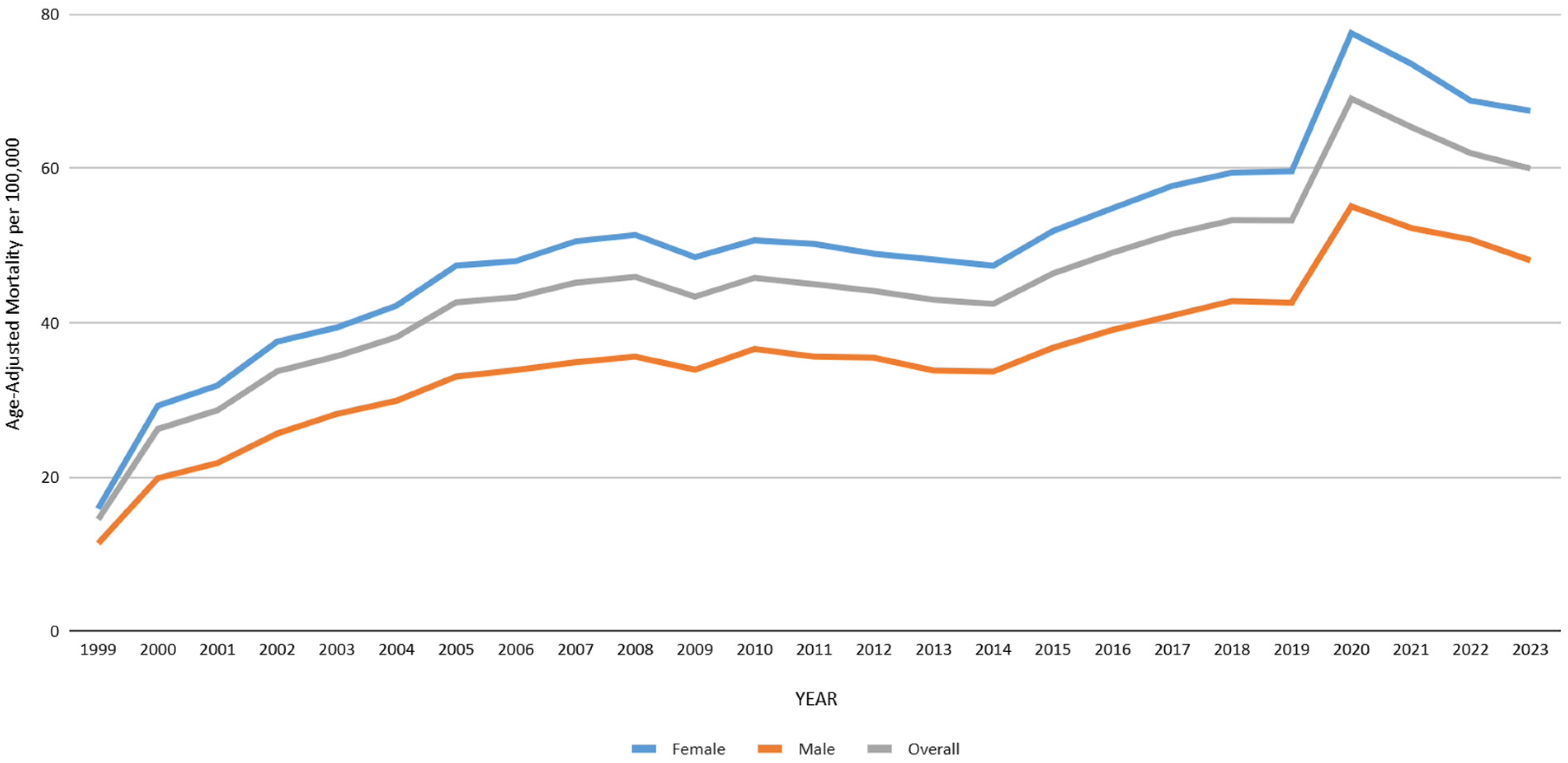
Overall and sex stratified hypertension and Alzheimer's disease-related AAMRs per 100,000 in the United States, 1999 to 2023, aged 65 years and above.
Annual percent change (APC) of hypertension and Alzheimer's disease-related age-adjusted mortality rates per 100,000 among adults aged 65 and above in the United States, 1999 to 2023.
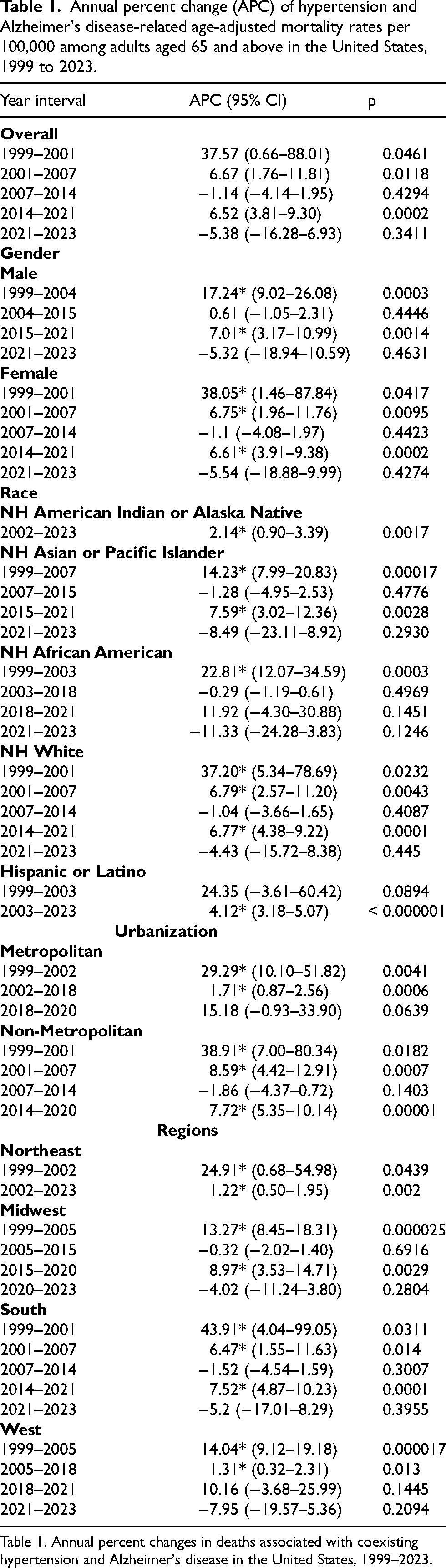
Table 1. Annual percent changes in deaths associated with coexisting hypertension and Alzheimer's disease in the United States, 1999–2023.
Stratification by sex
Females accounted for 354768 (70.33%) while male deaths were 149592 (29.67%). Female AAMR remained notably higher than males across the entire study period. In 1999, the AAMR was 15.88 (95% CI: 15.36–16.40) in women and 11.39 (95% CI: 10.77–12.00) in men; by 2023, these rates had increased to 67.5 (95% CI: 66.6–68.4) and 48.1 (95% CI: 47.1–49.1), respectively. Trend analyses demonstrated an overall significant increase in mortality for both sexes over time, with broadly similar temporal patterns. Females experienced a significant early rise (1999–2001) followed by a continued but more gradual increase through 2007, a plateau phase and a subsequent significant increase from 2015 to 2021, before a non-significant decline in recent years. Whereas, in males, a significant increase was observed during the early period (1999–2004), followed by a prolonged plateau and a renewed significant rise from 2015 to 2021, with a non-significant decline thereafter. Detailed segmented APC estimates, including non-significant intervals, are presented in Table 1, Figure 2, and Supplemental Table 4.
Stratification by race/ethnicity
Among races, NH Blacks had the highest AAMR of 57.14 (95% CI: 54.57–59.72) followed by NH Whites: AAMR 45.11 (95% CI: 44.42–45.81), Hispanics or Latinos: AAMR 39.69 (95% CI: 37.31–42.08) and AIAN: AAMR 35.28 (95% CI: 27.00–45.06) while the lowest mortality was exhibited by NH Asians or Pacific Islanders with an AAMR of 27.94 (95% CI: 25.19–30.75).
Trend analyses demonstrated overall increasing mortality across most racial/ethnic groups, with notable differences in magnitude and timing. NH Black and NH White populations showed significant early increases, followed by periods of relative stability, and renewed significant rises in more recent years, with non-significant declines observed after 2021. Among Hispanics/Latinos, mortality demonstrated a sustained and statistically significant increase especially 2003 onwards, representing one of the most consistent upward trends across groups. Similarly, AIAN populations exhibited a significant and continuous increase from the early 2000s onward. In NH Asians/Pacific Islanders, mortality rates significantly increased during earlier periods, followed by intervals of stability and later modest increases, with recent declines that were not statistically significant. Detailed segmented APC estimates, including non-significant intervals, are provided in Table 1, Figure 3, and Supplemental Table 5. AAMR estimates for AIAN populations during 1999–2001 were considered unreliable due to small counts (<20 deaths per year) and should therefore, be interpreted with caution.
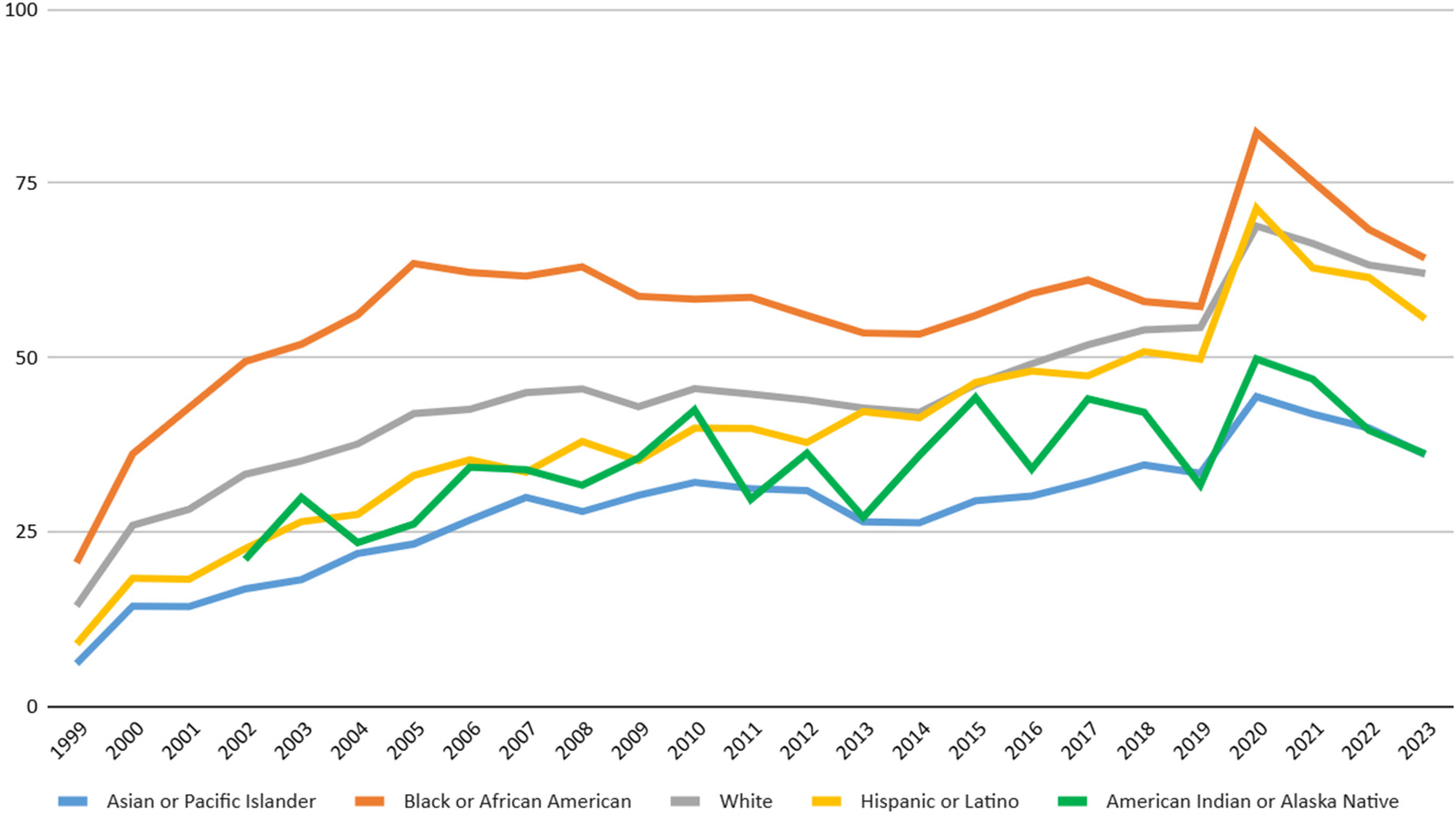
Race stratified hypertension and Alzheimer's disease-related AAMRs per 100,000 in the United States, 1999 to 2023, aged 65 years and above.
Stratification by urbanization
Non-metropolitan areas demonstrated a higher overall AAMR of 48.74 (95% CI: 47.18–50.29) in contrast to the Metropolitan areas with overall AAMR of 41.45 (95% CI: 40.78–42.13). Trend analysis revealed mortality increased over time in both settings, but the burden remained consistently greater in non-metropolitan counties (Table 1, Figure 4, Supplemental Table 6).
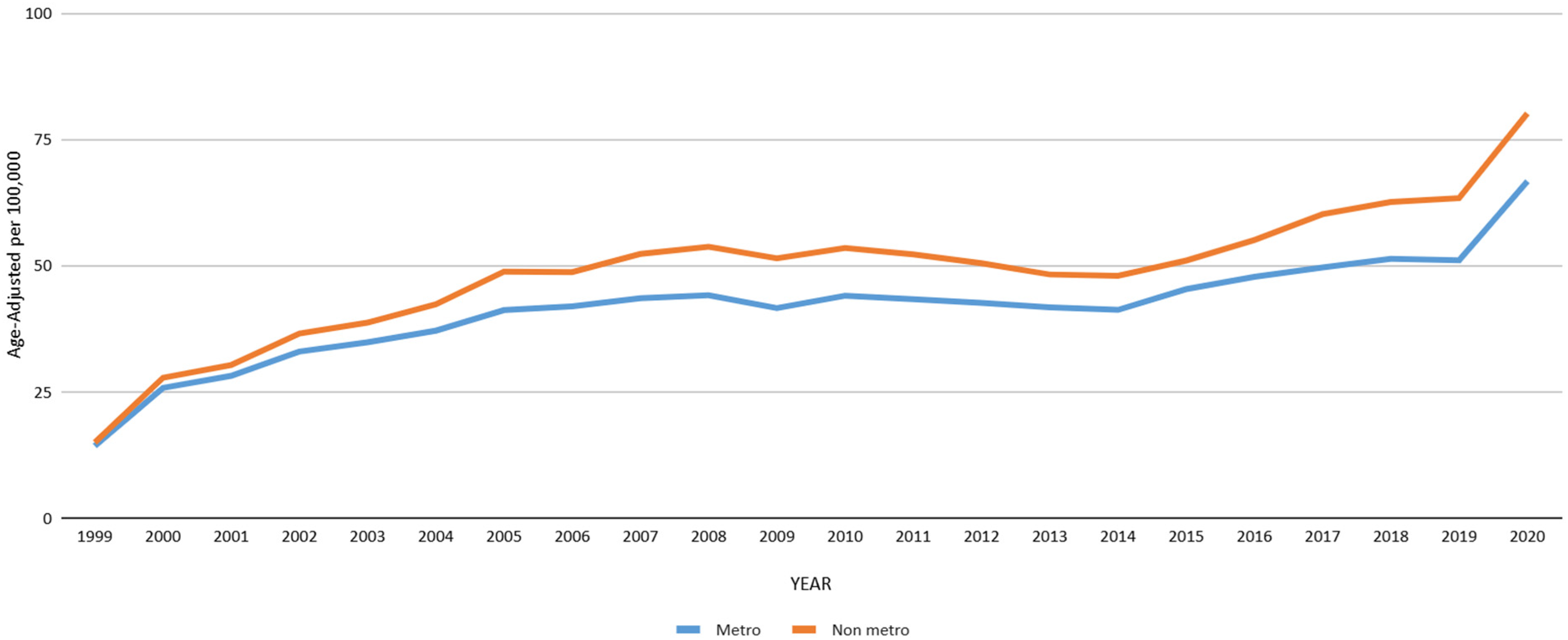
Urbanization stratified hypertension and Alzheimer's disease-related AAMRs per 100,000 in the United States, 1999 to 2020, aged 65 years and above.
Stratification by region and state
Among the 4 Census regions, the highest AAMR was observed in West: AAMR 52.59 (95% CI: 51.12–54.06) followed by South: AAMR 49.39 (95% CI: 48.28–50.49) and Midwest: AAMR 46.47 (95% CI: 45.14–47.80) while the Northeast had remarkably lower AAMR throughout with an overall AAMR of 28.11 (95% CI: 27.01–29.21) (Table 1, Figure 5, Supplemental Table 7).
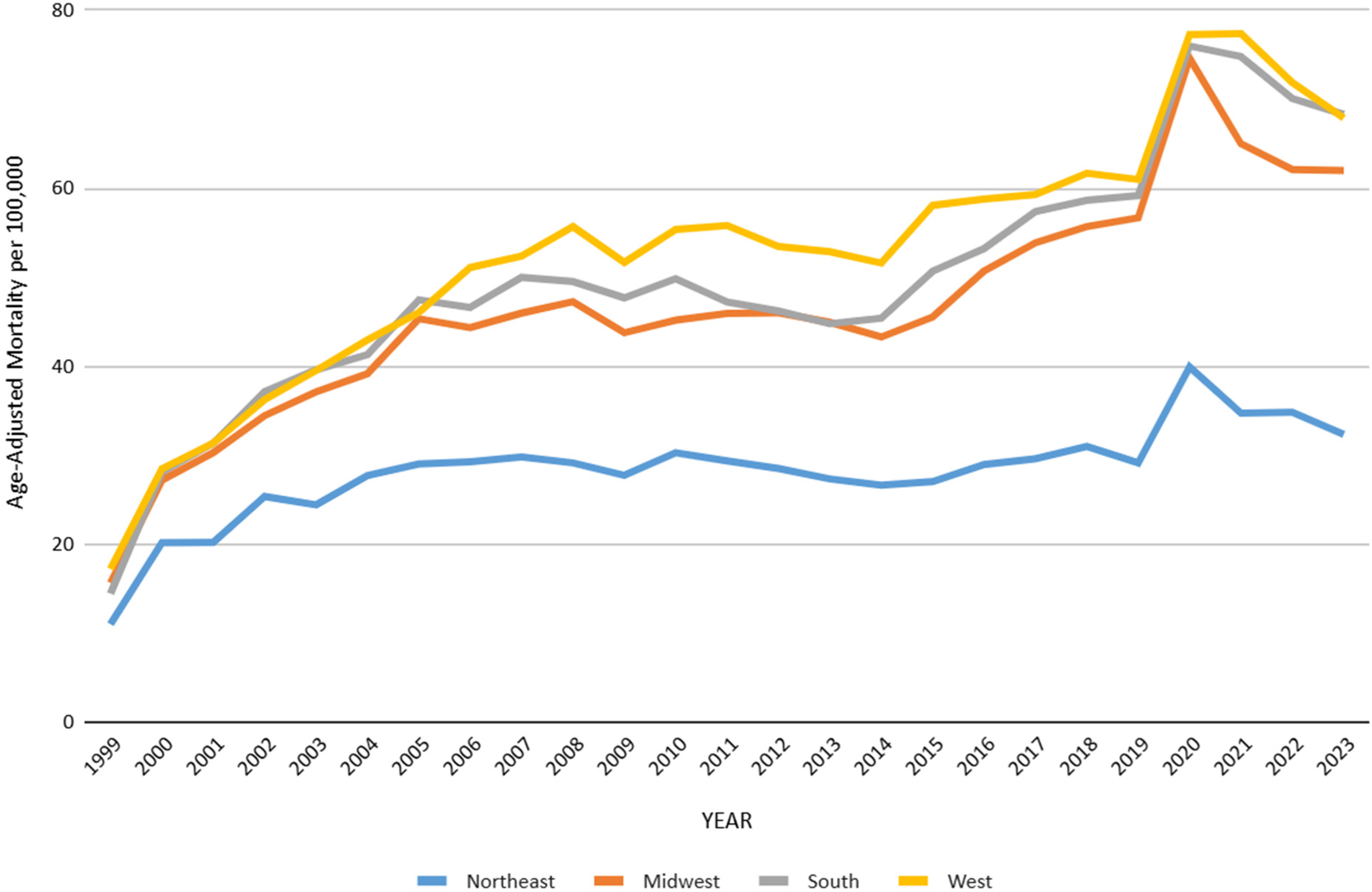
Region stratified hypertension and Alzheimer's disease-related AAMRs per 100,000 in the United Staes, 1999 to 2023, aged 65 years and above.
Interstate data showed California had the highest number of deaths (15.05%) while Alaska had the lowest (0.05%). However, the highest AAMR was experienced in Oklahoma 116.36 (95% CI: 113.07–119.65), Mississippi 129.95 (95% CI: 125.35–134.55), South Carolina 91.92 (95% CI: 88.98–94.86), Minnesota 84.06 (95% CI: 81.50–86.62), and Texas 82.54 (95% CI: 81.22–83.86), while the lowest AAMR was seen in Massachusetts 21.54 (95% CI: 20.45–22.63), Connecticut 23.11 (95% CI: 21.65–24.57), New York 27.18 (95% CI: 26.45–27.91), Florida 27.53 (95% CI: 26.89–28.17), and New Hampshire 33.51 (95% CI: 30.56–36.46) (Supplemental Table 8, Supplemental Figure 2).
Stratification by place of death
Of the 504,360 deaths, the majority occurred in nursing homes/long-term care (54.34%), followed by decedent's homes (23.38%). Medical facilities, including inpatient, outpatient/ER, etc., accounted for 8.71% while other locations contributed 7.04%, hospice facilities 3.53%, and place of death was not known for 0.20% (Supplemental Table 3).
Discussion
We conducted a CDC WONDER analysis spanning across two and a half decades (1999 to 2023), which displayed several intriguing mortality patterns related to HTN and AD, reflecting an increased burden of cardiovascular and neurological conditions with major public health repercussions. We observed a dramatic increase in deaths attributed to these intertwined conditions with clear demographic and geographic disparities. The overall AAMR increased fourfold during this period identifying three distinct phases of swift elevation, stabilization and subsequent escalation. Sex-stratified temporal mortality trends revealed consistently higher deaths among women across the two decades. The analysis also exposed discrepancies across racial and ethnic groups, demonstrating the greatest mortality among NH Blacks followed by NH Whites and Hispanics, while the lowest mortality rates were observed among NH Asians or Pacific islanders. A closer look into geographic variations revealed non-metropolitan areas experiencing a higher mortality compared to metropolitan areas. Additionally, the South and West regions displayed the greatest AAMR across the U.S. while interstate data reflected high rates in Oklahoma and Mississippi and lower rates in Massachusetts and Connecticut.
Our study shows that overall AAMR for coexistent HTN and AD-related deaths increased significantly which is in line with several studies that show an increased burden of both HTN22–24 and AD25–27 during these time frames, especially during the earlier years,22,25 while other cardiovascular diseases (CVDs), such as heart failure and stroke mortality, both independently and in association with AD, declined or stabilised.22,28,29 A CDC database study on CVD-related AD mortality only observed a modest, insignificant increase in AAMR from 110.13 to 116.80 across 1999–2020 in contrast to a dramatic increase in AAMR from 14.51 to 60.00 in our study. 27 Another study finds that CVD-related AD AAMR decreased for all conditions like ischemic heart disease, heart failure, and stroke except for hypertensive disease (increased by 56.7%). 30 Taken together, these findings suggest that HTN remains a frequently documented and increasingly important comorbidity among older adults dying with AD, particularly in contrast to several other cardiovascular conditions whose associated mortality has stabilized or declined in recent years.28,31
Importantly, the increase in mortality should not be interpreted merely as evidence of a biologically worsening relationship between HTN and AD. Several non-mutually exclusive factors may contribute to this trend. First, the aging of the U.S. population, particularly growth in the old population, likely increases the absolute burden of AD-related mortality over time. 32 Second, AD has been underreported on the death certificates, notably in earlier years. Improved recognition and certification practices may partly inflate temporal increases.33,34 Similarly, awareness and documentation of HTN have evolved over time, which may increase the likelihood that both conditions are recorded together on death certificates. 35 Third, the disruptions of the COVID-19 era, especially in 2020–2021, may have influenced mortality, healthcare access and certification practices, all of which should be considered when interpreting late-period trends.
A wide array of mechanisms has been proposed to explain the frequent co-occurrence of dementia and HTN, including increased plaque deposition and neurofibrillary tangling, activation of glial cells and inflammatory mediators leading to neurological inflammation, hippocampal hypometabolism of glucose and cerebral vessels remodeling and oxidative injury which may partly help contextualize why HTN and AD frequently coexist in older adults and why this combination may contribute to a high mortality burden at the population level.36–40 Several studies have identified HTN as a modifiable risk factor for AD but with varying effectiveness of antihypertensives in its management. 40 This has long been a topic of debate with conflicting reports. While some trials and meta-analyses report improved cognitive outcomes and decreased incidence of AD with early management of HTN, notably during the Middle Ages,41–44 others report no single superior antihypertensive agent or no benefit, especially after AD has already been established.40,44–46 Thus, putting all of these together, the burgeoning cases of HTN-related AD fatalities can be attributed to the increased incidence of HTN and obesity, particularly among young adults, rendering them vulnerable to develop AD later in life; sedentary lifestyle, unhealthy eating patterns, variable efficacy of antihypertensives, an ageing population and increased awareness and reporting of AD as a cause of death on death-certificates.28,47
In our study, women maintained a higher AAMR than males throughout the study period. This is consistent with studies that show increased incidence of AD in females in contrast to males, mainly due to longer lifespan.25,48–50 Gilsanz et al. reported that females have a 65% increased risk of dementia with mid-life HTN compared to men, 50 while other literature reports the risk of HTN reverses after 65 years of age with a 13.6% increased risk in women, which is less likely to improve with pharmacotherapy compared to men (42.9% versus 57.9%), 51 possibly due to the hormonal changes after menopause. 52 Thus, these disparities in gender can be explained by difference in life expectancy, increased incidence of both HTN and AD in elderly women, variable interactions of sex chromosomes and hormones with neuronal degeneration; altered epigenetic regulation, metabolic pathways, molecular signaling and microbiome composition, prompting the need for improved awareness and better care in later stages of life, particularly for women.48–53
Analysis across different racial groups in our study demonstrates the highest AAMR in NH Blacks, which is consistent with a CDC analysis on HTN-related mortality reporting the highest mortality rate in this racial group. 23 Already established literature suggesting a higher prevalence, poor control and increased burden of HTN-related morbidity in NH Blacks can potentially explain this finding.54,55 Yet, these disparities should not be interpreted as reflecting innate biological difference alone. Rather, they also reflect the cumulative effects of structural inequities, differential access to specialty care, variation in treatment intensity, and broader social determinants of health that shape both vascular and neurodegenerative disease burden.54–56
Non-metropolitan populations had a higher mortality rate than metropolitan residents. These findings are coherent with a national study on mortality trends in obese patients with HTN. 57 Similarly, another CDC-based study on cardiovascular mortality in patients with AD reported the highest AAMR in the non-metropolitan population. 27 This difference in terms of urbanization status reflects the rural health disadvantage. Rural areas and small towns offer fewer specialty clinics, a relative lack of services, and a farther distance to access primary care. 56 These disparities highlight the need for adequate resource distribution and policies to address the barriers to specialty care.
Furthermore, the elevated AAMR in the Southern and Western regions of the U.S. are consistent with a national synthesis on ischemic heart disease-associated mortality in patients with AD. 14 Similarly, Wen et al. reported the highest AAMR in the West in patients with cardiovascular diseases and AD. 27 The high prevalence of HTN in these regions and geographical disparities account for the clustering of deaths in these areas. 9 Our interstate analysis showed that Oklahoma had the highest AAMR for patients with HTN and AD, reflecting interstate disparities that call for special interventions and improved infrastructure, especially in the South and West, which is in line with previous research. 58 On the other hand, nearly half of the deaths occurred in nursing homes, indicating the need to effectively manage both HTN and AD. This finding is in conjunction with prior research showing that patients with advanced dementia frequently reside in institutional settings, 59 where cognitive decline and comorbidity burden contribute to mortality risk.
From a clinical and public health perspective, our findings underscore the importance of lifelong vascular risk reduction, equitable HTN detection and treatment, and integrated care for older adults with cognitive impairment. However, these data should not be interpreted as demonstrating that blood pressure control alone will directly reduce mortality among all individuals with established AD as such questions require prospective individual-level investigation. Future research should examine how HTN control, treatment timing, care setting and social determinants of health shape outcomes across the dementia continuum.
Limitations
Several limitations can be reported in our study. First, the reliance on death certificate data poses the biggest limitation in CDC analysis, as the recording of HTN and AD data can vary in accuracy across regions and care centers. Multiple studies report that AD is less likely to be reported as a cause of death on death-certificates.39,60 Second, our analysis identified deaths in which AD and HTN were co-listed on death certificates but could not determine whether HTN preceded AD, whether blood pressure was controlled, whether antihypertensive therapy was used, or whether HTN directly contributed to death in individual cases. Third, because this was a descriptive ecological analysis using administrative mortality data, causal inference was not possible, and no individual-level adjustment for potential confounders such as socioeconomic status, comorbidities, health behaviors, medication use, or access to care could be performed, nor can these results be generalized to individuals with HTN and AD. Moreover, data pertaining to race and ethnicity is subjected to several inaccuracies due to misclassification of individuals compromising the precision of subgroup estimates. This is particularly evident for smaller populations where several races are often under-represented rendering the AAMR values unreliable if the total number of deaths reported do not exceed 20 for that specific year. The observed geographic and demographic variabilities can be attributed to interstate differences in diagnostic practices, healthcare infrastructure, and access to specialized dementia care which limits the precision of reported mortality data. Another important limitation is while the study covers a long timeframe, it does not capture evolving clinical practices, including HTN management strategies and dementia care models, which may influence mortality trends but are not reflected in the dataset.
Conclusion
Mortality among U.S. adults aged ≥65 years in whom AD and HTN co-occurred on death certificates increased substantially between 1999 and 2023. This burden was disproportionately concentrated among women, non-Hispanic Black adults, non-metropolitan populations, and selected states and regions, with most deaths occurring in long-term care settings.
These findings describe a growing and unequally distributed mortality burden at the intersection of vascular and neurodegenerative disease in later life. They support the need for equitable HTN prevention and management across the lifespan, improved dementia care delivery, and more nuanced surveillance of multimorbidity in aging populations.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261461304 - Supplemental material for National trends and disparities in mortality among U.S. older adults, with coexisting Alzheimer's disease and hypertension, 1999-2023
Supplemental material, sj-docx-1-alz-10.1177_13872877261461304 for National trends and disparities in mortality among U.S. older adults, with coexisting Alzheimer's disease and hypertension, 1999-2023 by Muhammad Ibrahim Rashid, Muhammad Abbas, Ramesha Tahir, Taha Alam, Aliya Noor, Zaigham Ishrat, Muhammad Mudasir, Muhammad Ahsan Sarfraz, Umair Mehboob and Iman Osman Abufatima in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
ORCID iDs
Ethical considerations
This study was exempt from review by the local institutional review board because it utilized de-identified, publicly available data.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
All data are provided in the Supplemental Material and are fully reproducible as detailed in the Methods section.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.