
Abstract
Background
Type 2 diabetes mellitus (T2DM) is a major risk factor for dementia, yet the prognostic value of early dynamic glycemic changes following glucose-lowering therapy remains underinvestigated.
Objective
To determine whether early glycated hemoglobin (HbA1c) trajectories after initiating sodium-glucose cotransporter 2 inhibitors (SGLT2i) predict long-term dementia and mortality risks.
Methods
This retrospective new-user cohort study utilized electronic health records from the TriNetX Global Network. Adults with T2DM initiating their first SGLT2i were included. To mitigate immortal-time bias, a 1-year landmark design was applied. Patients were stratified by baseline HbA1c and classified into improved, stable, or worsened trajectories based on values 91–455 days post-initiation. Propensity-score matching was performed within strata. The primary outcome was all-cause dementia.
Results
Among 172,050 matched patients, modest HbA1c worsening in those with Good baseline control (<7.0%) did not increase dementia risk (HR 0.93; 95% CI, 0.75–1.15). However, in patients with Fair baseline control (7.0–8.9%), worsening to Poor control significantly increased dementia (HR 1.39; 95% CI, 1.11–1.74) and mortality risks. Conversely, among those with Poor baseline control (≥9.0%), trajectory improvement conferred substantial neuroprotection, reducing the risk of dementia (HR 0.64; 95% CI, 0.51–0.79) and mortality (HR 0.71; 95% CI, 0.60–0.84). These findings provide clinically actionable evidence linking glycemic dynamics to neurodegenerative risk, particularly Alzheimer's disease and related dementias.
Conclusions
Dynamic HbA1c trajectories following SGLT2i initiation independently predict dementia risk. Integrating trajectory-based assessments into routine care provides an actionable, scalable biomarker to guide timely treatment intensification and mitigate diabetes-related neurocognitive decline.
Keywords
Introduction
Diabetes mellitus represents a rapidly growing global health challenge, with its prevalence projected to reach more than 1.3 billion adults worldwide by 2050. 1 Beyond its cardiovascular, renal, and metabolic complications, dementia has emerged as one of the most consequential long-term sequelae, both clinically and from a public health perspective.2–5 Globally, more than 55 million people are currently living with dementia, a figure expected to more than double by 2050. 6 Substantial epidemiologic evidence indicates that individuals with diabetes face a 40–60% higher risk of dementia compared with those without diabetes, with particularly strong associations for vascular dementia.2–5 Earlier age at diabetes onset, longer disease duration, poor glycemic control, and recurrent hypoglycemia further magnify this risk.3,7,8 These data underscore the intertwined epidemics of diabetes and dementia in aging societies and highlight the urgent need for strategies that extend beyond glycemic targets to encompass long-term neurocognitive outcomes.
Accumulating evidence links glycemic control with dementia risk in diabetes, yet most studies have relied on a single HbA1c measurement. Higher HbA1c levels, greater variability, and longer diabetes duration have each been associated with elevated risk of cognitive decline and dementia.2,4,7,9,10 However, a static value cannot capture treatment response or the dynamic course of glycemic control, nor does it account for hypoglycemia or glycemic instability, which are themselves risk factors.1,11 Indeed, recent cohort and meta-analytic data suggest that stable HbA1c trajectories within the moderate range confer the lowest dementia risk, whereas persistently high or highly variable values substantially increase risk.2,10 These findings underscore the need for more refined metrics, such as HbA1c trajectories, that reflect the quality and stability of glycemic control over time, and may more accurately predict long-term neurocognitive outcomes.4,7,9,10
Sodium–glucose cotransporter 2 inhibitors (SGLT2is) have become central in type 2 diabetes mellitus (T2DM) management, offering not only modest glucose-lowering (HbA1c reduction of ∼0.5–1.0%) but also robust cardiovascular and renal protection.12–16 Evidence now suggests potential neuroprotective effects, with population-based studies showing reduced risks of dementia and Parkinson's disease among SGLT2i users.14,17–19 Yet glycemic response to SGLT2i is heterogeneous: while some patients achieve marked HbA1c improvement, others show little change, despite accruing cardio-renal benefits.15,18 Importantly, there are no clear clinical guidelines on how to interpret post-treatment HbA1c trajectories to guide therapeutic intensification. This gap underscores the need to evaluate whether early HbA1c dynamics after SGLT2i initiation can serve as a prognostic marker for long-term neurocognitive outcomes.
Despite accumulating evidence linking glycemic control to dementia risk, nearly all prior studies have relied on single time-point HbA1c values, which cannot capture treatment response or dynamic change. Long-term high HbA1c levels (≥9%) are strongly associated with future dementia risk, whereas values maintained in the 6–8% range confer lower risk; greater variability and lower time in range are each linked to higher incidence of cognitive decline.9–11,20 Current ADA standards caution that intensive glycemic lowering (HbA1c < 6%) does not improve cognition and may increase hypoglycemia risk. 1 Although HbA1c trajectories have demonstrated prognostic value for cardiovascular and renal outcomes, their role as early markers of dementia risk has scarcely been investigated.9–11,20 In particular, whether glycemic response following therapy initiation can serve as an early indicator of long-term neurocognitive outcomes remains unknown.1,11,20–22 Against this backdrop, we designed the present study to evaluate whether one-year HbA1c trajectories after initiation of SGLT2i provide clinically meaningful information about subsequent dementia risk. Clarifying this association could establish a simple and scalable biomarker to inform timely treatment intensification and contribute to the prevention of diabetes-related dementia.
Methods
Data source and study design
We conducted a retrospective new-user cohort study within the TriNetX Global Collaborative Network, which aggregates irreversibly de-identified electronic health records from health-care organizations worldwide. The platform utilizes de-identified unique patient identifiers to integrate data into unified longitudinal records and deduplicate records across participating organizations.23,24 The study aimed to evaluate whether changes in glycated hemoglobin (HbA1c) from before to approximately one year after initiation of a SGLT2i predict subsequent risk of dementia among adults with T2DM.
Study population
Eligible patients were 18 to 90 years of age, had a diagnosis of T2DM (ICD-10-CM E11), and received their first prescription for an SGLT2i (ATC A10BK) between January 1, 2013, and July 25, 2025, ensuring restriction to the contemporary era of availability. The date of the first prescription defined the index date. To ensure a new-user design, patients with prior SGLT2i exposure during the preceding 12 months or any dementia diagnosis before the index date were excluded. Baseline characteristics of patients across HbA1c categories before and after propensity-score matching are summarized in Supplemental Table 1a and 1b.
Landmark, exposure windows, and risk-set entry
To minimize reverse causation and immortal-time bias, we applied a landmark design. Baseline HbA1c was defined as the value measured within the year preceding SGLT2i initiation that was closest to the index date. The follow-up HbA1c was defined as the value obtained within the first year after initiation that was closest to 365 days, with selection restricted to the window of 91 to 455 days after initiation to avoid peri-initiation instability; if two values were equidistant, the later value was used. Patients lacking HbA1c measurements during this window were excluded as their trajectories could not be ascertained. Patients who died or received a dementia diagnosis before this follow-up assessment were excluded. Follow-up began one year after the index date, when all patients were alive and dementia-free, and continued until dementia, death, loss to follow-up, or study end. Follow-up was defined by continuous activity within the network, and patients without subsequent healthcare encounters were censored at their last known activity date
HbA1c categories and trajectories
Baseline HbA1c was categorized as Good (<7.0%), Fair (7.0–8.9%), or Poor (≥9.0%). Within each baseline category, patients were classified according to whether their glycemic status at the follow-up assessment improved, remained stable, or worsened, based on transitions between categories. For parsimony, composite contrasts were also analyzed, such as “any worsening” among patients with good baseline control and “any improvement” among those with poor baseline control. The associations of HbA1c trajectories with risks of dementia and mortality are reported in Table 1.
Associations of HbA1c trajectories after SGLT2 inhibitor initiation with risks of all-cause dementia, dementia subtypes, and mortality.
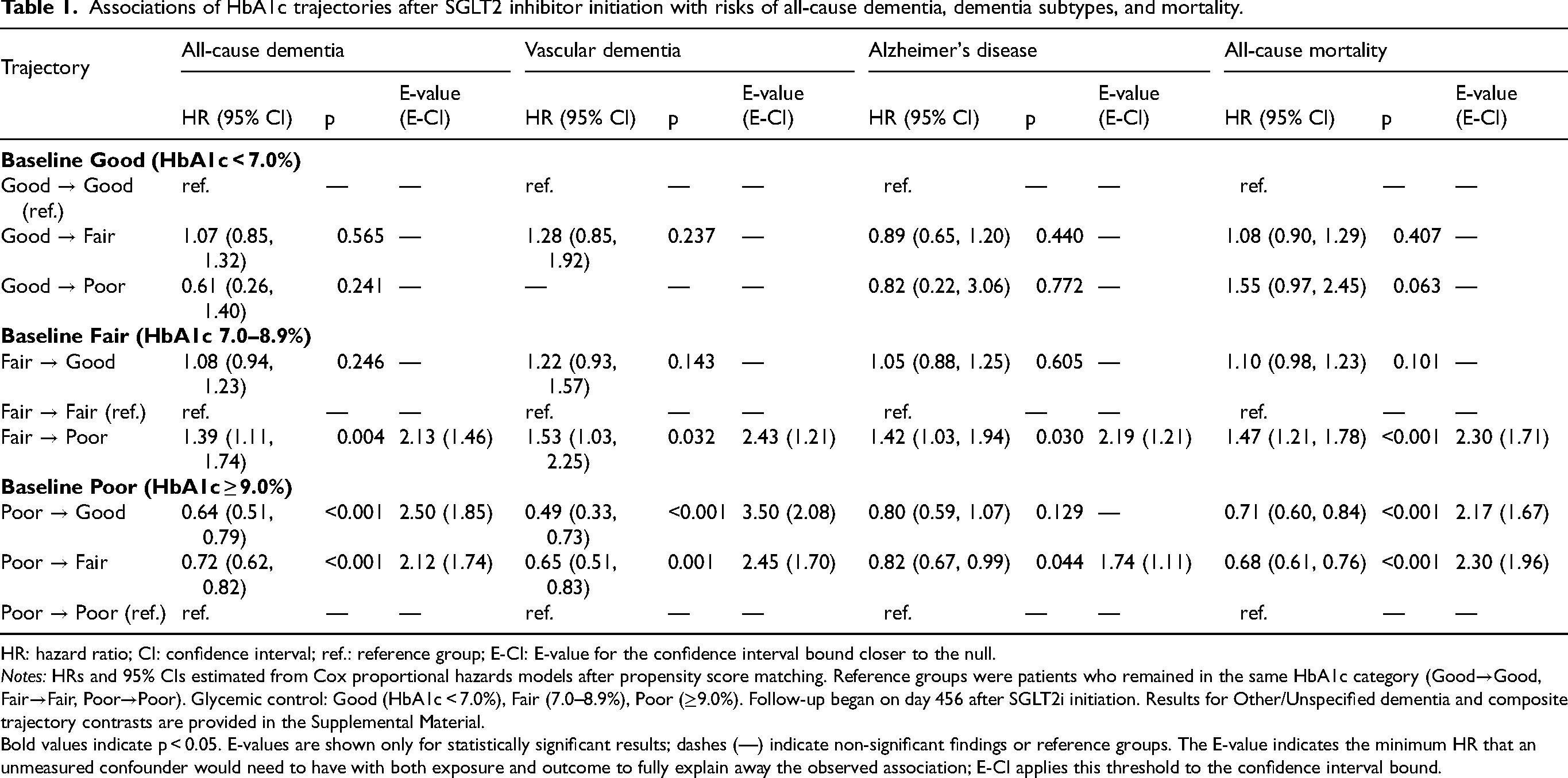
HR: hazard ratio; CI: confidence interval; ref.: reference group; E-CI: E-value for the confidence interval bound closer to the null.
Notes: HRs and 95% CIs estimated from Cox proportional hazards models after propensity score matching. Reference groups were patients who remained in the same HbA1c category (Good→Good, Fair→Fair, Poor→Poor). Glycemic control: Good (HbA1c < 7.0%), Fair (7.0–8.9%), Poor (≥9.0%). Follow-up began on day 456 after SGLT2i initiation. Results for Other/Unspecified dementia and composite trajectory contrasts are provided in the Supplemental Material.
Bold values indicate p < 0.05. E-values are shown only for statistically significant results; dashes (—) indicate non-significant findings or reference groups. The E-value indicates the minimum HR that an unmeasured confounder would need to have with both exposure and outcome to fully explain away the observed association; E-CI applies this threshold to the confidence interval bound.
Outcomes
The primary outcome was incident all-cause dementia identified by prespecified ICD-9-CM, ICD-10-CM, and UMLS codes, including Alzheimer's disease, vascular dementia, and other or unspecified dementias. All-cause mortality was a prespecified secondary outcome. Because patients with worsening HbA1c trajectories had higher mortality, the elevated dementia incidence observed in these groups is conservative, since early death would reduce opportunities for dementia diagnosis.
Covariates
Prespecified covariates included demographic factors (age, sex, and race or ethnic group), comorbidities spanning cardiometabolic, neurologic, renal, hepatic, pulmonary, and hematologic systems, baseline use of glucose-lowering, antihypertensive, lipid-lowering, antiplatelet or anticoagulant, corticosteroid, nonsteroidal anti-inflammatory, and psychotropic medications, as well as physiologic and laboratory measures (body-mass index, waist circumference, blood pressure, triglycerides, and low-density lipoprotein cholesterol). Health-care utilization during the year before the index date (hospitalizations and outpatient visits) and the index calendar year were included to account for detection intensity and secular trends (Supplemental Table 2). We also adjusted for the interval between the baseline HbA1c and index date, and incorporated the number of HbA1c tests in the baseline year to address potential measurement-density bias, with distributions summarized in Supplemental Tables. For baseline covariates, missingness was treated as an independent “unknown” category; multiple imputation was not performed to avoid additional model assumptions in the context of heterogeneous real-world data. 26
Propensity-score matching
Within each baseline HbA1c stratum, patients were compared using 1:1 nearest-neighbor propensity-score matching (PSM) without replacement, applying a caliper of 0.1 standard deviations of the logit of the propensity score. Propensity models included all prespecified covariates. Balance was assessed using absolute standardized mean differences (ASMDs), with values less than 0.10 indicating acceptable balance. Matching diagnostics are presented in Supplemental Table 1a and 1b.
Statistical analysis
Cumulative incidence was estimated with Kaplan–Meier methods, and hazard ratios (HRs) with 95% confidence intervals (CIs) were derived from cause-specific Cox proportional-hazards models fitted to the matched cohorts, to provide etiologic inference by estimating direct effects on individuals who remained event-free. 27 To complement these estimates with clinically interpretable absolute risk, we derived cumulative-incidence functions treating death as a competing risk, 28 as shown in Supplemental Figure 1. Hazard ratios for dementia associated with HbA1c trajectories across baseline strata are presented in Supplemental Tables 3–10.
Sensitivity and validation analyses
Robustness was assessed by repeating the analyses using an alternative post-index window (days 181–545) with risk-set entry on day 546 (Supplemental Table 1). HbA1c change was modeled through categorical transitions across Good, Fair, and Poor states (Supplemental Tables 3–10). Baseline measurement density was examined, showing similar HbA1c test frequency after matching (Supplemental Table 11a, b). Finally, we performed a systematic E-value analysis for statistically significant outcomes to quantify the strength of unmeasured confounding needed to nullify our findings. 29
Results
Study population and baseline balance
After the 1-year landmark, two propensity-matched comparisons were analyzed. In the Fair versus Good set, each arm included 52,858 patients, while in the Poor versus Good set, each arm included 33,167 patients. Baseline covariates were well balanced after matching (all ASMD <0.10). In the Fair versus Good set, the mean age was 63.60 versus 63.65 years, and women accounted for 43.59% versus 43.81% (Supplemental Table 1a). In the Poor versus Good set, the mean age was 59.77 versus 59.83 years, and women accounted for 43.19% versus 43.46% (Supplemental Table 1b). The number of HbA1c tests in the baseline year was well matched, approximately 2.3–2.5 per year across arms, minimizing concerns about measurement-density bias and potential selection bias from differential visit processes (Supplemental Table 11a, b). 30
Associations of HbA1c trajectories with dementia and mortality
For patients with good baseline HbA1c (<7.0%), neither transition to fair control (HR 1.07, 95% CI 0.85–1.32) nor pooled “any worsened” contrasts (HR 0.93, 95% CI 0.75–1.15) were associated with excess dementia risk (Table 1; Supplemental Tables 3–5; Supplemental Figure 1A–D); mortality estimates were similarly null (Table 1; Supplemental Tables 3–5; Supplemental Figure 1A–D, O). Subtype analyses (Supplemental Tables 4–6) confirmed no signal across Alzheimer's, vascular, or other/unspecified dementia. This suggests that modest HbA1c worsening from already well-controlled levels does not meaningfully alter near-term cognitive outcomes, supporting a strategy of clinical reassurance rather than escalation in this subgroup.
In contrast, among patients with fair baseline HbA1c (7.0–8.9%), deterioration to poor control markedly elevated dementia risk: all-cause dementia (HR 1.39, 95% CI 1.11–1.74), vascular dementia (HR 1.53, 95% CI 1.03–2.25), and other/unspecified dementia (HR 1.74, 95% CI 1.22–2.45) were all increased, alongside higher mortality (HR 1.47, 95% CI 1.21–1.78) (Supplemental Figure 1K, O). These data indicate that when patients in the “middle zone” worsen despite SGLT2i therapy, their neurocognitive and survival risks accelerate, underscoring the importance of early treatment intensification.
For patients starting with poor baseline control (≥9.0%), improvement yielded substantial benefit. Transition to good control reduced risks of all-cause dementia (HR 0.64, 95% CI 0.51–0.79), vascular dementia (HR 0.49, 95% CI 0.33–0.73), other/unspecified dementia (HR 0.51, 95% CI 0.35–0.73), and mortality (HR 0.71, 95% CI 0.60–0.84) (Supplemental Figure 1B–D, E–G, P). Improvement to fair control showed parallel reductions in all-cause dementia (HR 0.72, 95% CI 0.62–0.82), vascular dementia (HR 0.65, 95% CI 0.51–0.83), Alzheimer's dementia (HR 0.82, 95% CI 0.67–0.99), and mortality (HR 0.68, 95% CI 0.61–0.76) (Supplemental Figure 1I, L–N, Q). A pooled “any improvement” contrast confirmed protection for both dementia (HR 0.75, 95% CI 0.65–0.85) and mortality (HR 0.71, 95% CI 0.63–0.78) (Table 1; Supplemental Tables 8–10; Supplemental Figure 1B–D, E–G, I, L–N, P–R). These findings indicate that lowering HbA1c from ≥9% within the first year confers meaningful cognitive and survival advantages, supporting prompt intensification when early SGLT2i response is inadequate.
Sensitivity and validation analyses
Using a later landmark (days 181–545, entry day 546) yielded qualitatively identical results: Fair→Poor remained harmful (all-cause dementia HR 1.60, 95% CI 1.27–2.01), whereas Poor→Good (HR 0.78, 95% CI 0.62–0.98) and Poor→Fair (HR 0.74, 95% CI 0.64–0.87) remained protective (Supplemental Table 1). HbA1c test counts were well balanced after matching (Supplemental Table 11a, b)
Discussion
In this large, propensity-matched cohort of patients initiating SGLT2is, we found that one-year HbA1c trajectories strongly predicted subsequent dementia risk, fully consistent with our a priori hypothesis. Patients with Good baseline control (<7.0%) showed no excess risk when HbA1c worsened modestly, with hazard ratios for all-cause and subtype-specific dementia remaining null (Table 1; Supplemental Tables 4–6; Supplemental Figure 1A–D, O). By contrast, among patients with intermediate (Fair, 7.0–8.9%) baseline control, worsening to Poor control was consistently associated with increased incidence of dementia—including vascular and other dementia subtypes—and elevated mortality (HR for all-cause dementia, 1.39; 95% CI, 1.11–1.74) (Table 1; Supplemental Table 7; Supplemental Figure 1K, O). For patients with Poor baseline control (≥9.0%), improvement to Fair or Good categories was strongly protective, reducing risks of all-cause, vascular, and other dementias as well as mortality (HR for all-cause dementia, 0.64; 95% CI, 0.51–0.79 for Poor→Good; HR 0.72; 95% CI, 0.62–0.82 for Poor→Fair) (Table 1; Supplemental Tables 8–10; Supplemental Figure 1B–D, E–G, I, L–N, P–R). These findings provide clinically actionable evidence linking glycemic dynamics to neurodegenerative risk, particularly Alzheimer's disease and related dementias. These findings highlight a clinically actionable gradient: failure to maintain or improve control when baseline HbA1c is ≥7.0% identifies patients at heightened neurocognitive risk, whereas marked improvement from ≥9.0% confers substantial benefit. Current ADA/EASD consensus guidelines recommend timely pharmacologic intensification when glycemia remains above target despite SGLT2i therapy, including GLP-1 receptor agonists such as semaglutide or tirzepatide, additional oral agents, or insulin when indicated.31–33 Our results provide empirical support for these recommendations, underscoring that persistent or worsening hyperglycemia after SGLT2i initiation should not be viewed as benign but instead as a call for prompt escalation to mitigate both dementia and survival risks. Our systematic E-value analysis further confirms that substantial unmeasured confounding would be required to fully explain the observed associations, with point estimates ranging from 2.12 to 3.50, and the strongest robustness observed for the protective effect of glycemic improvement on vascular dementia risk. 29 Furthermore, the use of unified records and standardized mapping within TriNetX minimized biases from fragmented care across institutions.23,24,34 Additionally, our dual statistical approach using cause-specific hazards and cumulative incidence functions ensured both robust etiologic inference and accurate absolute risk estimation in the presence of competing mortality.27,28
Prior studies have consistently linked glycemic control with dementia risk, but most have relied on single HbA1c values rather than dynamic trajectories. Large cohort studies from the UK and Sweden have shown that chronic hyperglycemia is associated with elevated dementia risk, particularly of the vascular subtype,4,9 and decades-long follow-up in JAMA Neurology demonstrated that higher cumulative HbA1c exposure predicted dementia incidence. 10 More recent work has emphasized the role of long-term stability and time in range, with HbA1c variability and instability associated with higher risk of cognitive decline.20,35 However, none of these studies directly evaluated whether treatment response to a specific class of glucose-lowering therapy could itself serve as a prognostic marker. Our study is the first to show that HbA1c trajectories in the year after SGLT2i initiation carry independent prognostic value. We demonstrate that when baseline HbA1c is ≥7.0%, failure to achieve stability or improvement is not benign but instead portends substantially higher risks of dementia and mortality (Table 1; Supplemental Tables 7–10; Supplemental Figure 1). Conversely, improvement from very poor control (≥9.0%) was associated with pronounced reductions in all-cause, vascular, and other dementias as well as mortality, establishing treatment response itself as a clinically relevant marker of neurocognitive outcomes. This represents a shift from interpreting HbA1c as a static target to recognizing dynamic change, particularly early response to therapy, as central to dementia risk stratification. These findings also align with and extend existing literature. The particularly strong association between worsening control and vascular dementia observed in our data (Supplemental Tables 3–10) is consistent with prior evidence that diabetes accelerates cerebrovascular pathology, which in turn drives vascular cognitive impairment.21,22 The novelty lies in showing that within the setting of SGLT2i therapy, early glycemic deterioration despite treatment should be interpreted as an early warning signal for adverse neurocognitive and survival outcomes. This perspective underscores that it is not prescription of the drug alone, but the patient's treatment response, that holds prognostic meaning. This perspective reinforces our clinical hypothesis that failure to improve HbA1c after SGLT2i initiation should not be regarded as benign but rather as a signal to intensify therapy.31–33
Our findings suggest that HbA1c trajectories should be interpreted as actionable early warning signals rather than passive observational markers. For patients with baseline HbA1c between 7.0 and 8.9%, deterioration to poor control despite SGLT2i therapy consistently predicted higher risks of dementia and mortality (Table 1; Supplemental Table 7; Supplemental Figure 1K, O). In such cases, continuing SGLT2i monotherapy is unlikely to be sufficient, and treatment intensification with additional agents is warranted.31–33 For patients starting with HbA1c ≥ 9.0%, achieving improvement within the first year markedly reduced the risks of all-cause, vascular, and other dementias, as well as mortality (Table 1; Supplemental Tables 8–10; Supplemental Figure 1B–D, E–G, I, L–N, P–R), reinforcing the value of early, aggressive control. These trajectories thus provide a practical trigger point for therapy adjustment, ensuring timely intervention and avoiding missed opportunities for neurocognitive protection.
The biological plausibility of our findings is supported by established mechanisms linking hyperglycemia to neurocognitive decline. Worsening HbA1c reflects sustained metabolic stress, which accelerates cerebrovascular injury, promotes white matter hyperintensity progression and subcortical infarcts, and disrupts blood–brain barrier function, thereby impairing amyloid-β clearance.36–38 Chronic hyperglycemia also induces systemic and neuroinflammation, a pathway strongly implicated in vascular and mixed dementias. Conversely, improvement in HbA1c may mitigate these processes by reducing cerebrovascular burden, enhancing insulin sensitivity, and lowering the incidence of vascular events. Long-term stability of HbA1c has consistently been associated with lower dementia risk,1,2,9–11 and our data extend this evidence by showing that patients with very poor baseline control (≥9%) derive substantial cognitive and survival benefits when HbA1c improves. In contrast, patients with baseline HbA1c < 7% did not experience excess dementia risk with modest worsening, suggesting that fluctuations within this low range may remain below the threshold required to trigger significant neuropathology. 20 This gradient helps explain why trajectories carried prognostic value only when baseline HbA1c was ≥7%. Taken together, these mechanistic insights reinforce our central hypothesis: HbA1c trajectories after SGLT2i initiation capture not only glycemic control but also the underlying pathophysiologic processes that drive dementia risk.
The robustness of our findings was reinforced through multiple sensitivity strategies. First, a landmark design was applied to minimize immortal-time bias, with follow-up anchored after post-index HbA1c ascertainment; effect estimates remained consistent across alternative landmark windows (days 181–545; Supplemental Table 1). Second, HbA1c change was modeled categorically, and results were directionally stable across dementia subtypes and mortality endpoints (Table 1; Supplemental Tables 3–10), demonstrating consistency across outcomes, an important criterion for causal inference. Third, the measurement density of HbA1c testing was balanced after matching, and additional adjustment for test frequency and outpatient visits did not materially alter risk estimates (Supplemental Table 11a, b), reducing concern for detection bias or differential surveillance. Finally, dose–response plausibility was evident: trajectory slope analyses showed that greater upward drift in HbA1c was associated with progressively higher risks of dementia and mortality, satisfying the Bradford Hill criterion of biological gradient. Taken together, these analyses strengthen the internal validity of our study, fulfilling key causal criteria: temporality (trajectory change precedes dementia onset), consistency (effects reproducible across subtypes and mortality), biological gradient (risk increases with worsening HbA1c slope), and robustness to confounding (stable after adjustment for health-care utilization). While residual confounding cannot be fully excluded, the convergence of evidence across multiple analytic approaches enhances confidence that early HbA1c deterioration after SGLT2i initiation represents a true risk signal rather than an artifact of study design. Specifically, our approach of treating missingness as an unknown category while balancing measurement density ensures that trajectory differences reflect clinical outcomes rather than data granularity.26,30
Our results suggest that among patients with baseline HbA1c ≥ 7.0%, one-year HbA1c trajectories should be used as a trigger for treatment escalation rather than passive observation. Patients whose HbA1c worsens after SGLT2i initiation should not remain on monotherapy but should receive timely intensification with complementary agents such as GLP-1 receptor agonists, DPP-4 inhibitors, or insulin when indicated, in accordance with current ADA recommendations.39,40 Conversely, patients with HbA1c ≥ 9.0% who achieve improvement within the first year experienced substantially lower dementia and mortality risks, underscoring the prognostic value of early stabilization. From a public health perspective, HbA1c trajectory is a low-cost, scalable biomarker that can be readily implemented for risk stratification and early intervention in diabetes populations.41,42 Because HbA1c monitoring is already embedded in standard diabetes care,39,40 its dynamic use offers a practical way to identify high-risk individuals and prevent missed opportunities for intervention. From a health economics standpoint, leveraging HbA1c trajectories represents a low-cost, high-yield strategy for population-level dementia prevention, maximizing impact without adding new resource burdens. We therefore call for future clinical trials to incorporate trajectory-based decision rules, testing whether embedding early treatment response into algorithms improves both cognitive and survival outcomes. Such an approach would move beyond static HbA1c thresholds toward precision diabetes management and dementia prevention.
Several limitations merit consideration. First, as an observational analysis, residual confounding cannot be excluded despite robust matching and sensitivity checks. Second, dementia diagnoses were based on ICD codes, which may undercapture early or mild cases and introduce outcome misclassification. Third, our findings derive from routine care data and thus require replication across diverse populations and treatment settings to ensure generalizability. Finally, future work should integrate HbA1c trajectories with complementary biomarkers, including cognitive testing and neuroimaging, to refine risk stratification and elucidate underlying mechanisms.
In summary, this study is the first to demonstrate that dynamic HbA1c change after SGLT2i initiation provides a simple, feasible tool for predicting dementia risk, and it should be directly considered in clinical decision-making.
Conclusions
Our study demonstrates that dynamic HbA1c trajectories after SGLT2i initiation are not merely descriptive but prognostic: worsening control in patients with baseline HbA1c ≥ 7.0% signals elevated dementia and mortality risk, whereas improvement from ≥9.0% confers substantial protection. By transforming a routine biomarker into a treatment trigger, these findings move beyond static thresholds and establish a simple, scalable approach with the potential to change clinical practice and inform precision strategies for dementia prevention.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261462927 - Supplemental material for HbA1c trajectories after SGLT2 inhibitor initiation and the risk of dementia
Supplemental material, sj-docx-1-alz-10.1177_13872877261462927 for HbA1c trajectories after SGLT2 inhibitor initiation and the risk of dementia by Jiaqiang Zhang, Yangyang Wang, Zhongyuan Lu, Yitian Yang, Jiao Wang, Liang Zhao, Fangfang Li, Mengrong Miao, Wan-Ming Chen, Szu-Yuan Wu and Mingyang Sun in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We thank the TriNetX Global Collaborative Network for providing the data infrastructure.
Ethical considerations
This study utilized the TriNetX platform, which exclusively provides de-identified and aggregated electronic health record data.
Consent to participate
In accordance with HIPAA rules, research conducted using this platform is exempt from IRB oversight and does not require informed consent.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Henan Province Clinical Research-Oriented Physician Training Program (Funding Number: HNCRD202409) and Lo-Hsu Medical Foundation, Lotung Poh-Ai Hospital (Funding Numbers: 11403 and 11404).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data were obtained from TriNetX and are available through their global research network.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.