
Abstract
Background
Lecanemab is an anti-amyloid monoclonal antibody, approved for early Alzheimer's disease (AD), with evidence indicating greater benefit at earlier stages. Sensitive cognitive measures are needed to identify underlying amyloid pathology.
Objective
To investigate whether the Logical Memory (LM) subtest of the Wechsler Memory Scale-Revised (WMS-R) can help characterize amyloid positivity in lecanemab-eligible individuals.
Methods
We retrospectively analyzed 91 individuals who attended our center between December 2023 and March 2025; 45 met eligibility criteria (Mini-Mental State Examination ≥ 22, Clinical Dementia Rating 0.5 or 1.0, magnetic resonance imaging compatibility). Amyloid status was determined by positron emission tomography, classified as amyloid-positive (Aβ+, n = 35) or amyloid-negative (Aβ−, n = 10). All participants underwent neuropsychological assessment, including LM. Groups were compared, and LM Aβ status discrimination was evaluated using receiver operating characteristic analyses and multivariable logistic regression.
Results
Groups did not differ in age, sex, or education. LM immediate (LMIR) and delayed recall (LMDR) scores were lower in the Aβ+ group (LMIR median: 5.0 versus 9.0, p = 0.011; LMDR: 0.5 versus 3.0, p = 0.017). Receiver operating characteristic analyses identified cutoffs of 7.5 for LMIR (area under the curve [AUC]: 0.79, sensitivity: 79%, specificity: 77%) and 1.5 for LMDR (AUC: 0.76, sensitivity: 75%, specificity: 77%). Lower LM scores were associated with increasing amyloid positivity. Logistic regression showed significant associations for both LMIR and LMDR (odds ratio: 0.80 and 0.64, 95% confidence interval: 0.64–0.95 and 0.38–0.91, respectively).
Conclusions
WMS-R LM scores were significantly associated with amyloid-β accumulation in individuals with early AD meeting lecanemab eligibility criteria.
Introduction
Global dementia prevalence is steadily increasing, with Alzheimer's disease (AD) remaining its most common cause, 1 characterized by episodic memory loss. 2
Recently, anti-amyloid monoclonal antibodies such as lecanemab and donanemab have been approved for early-stage AD treatment. Although they slow cognitive decline, their clinical benefits are modest, and accumulating evidence suggests that patients with lower baseline amyloid-β (Aβ) derive greater benefit. This underscores the importance of early Aβ pathology identification in patients who are potential candidates for anti-amyloid therapy.3,4
Neuropsychological tests (NPTs) remain a cornerstone in AD diagnosis and monitoring. 5 The Logical Memory (LM) subtest of the Wechsler Memory Scale-Revised (WMS-R) 6 is a sensitive measure of episodic memory impairment, a hallmark of early AD; LM performance has been shown to decline early in the disease course. 7 Previous studies have reported associations between poorer LM performance and Aβ accumulation.8,9 However, its performance has not been systematically evaluated in cohorts rigorously selected based on eligibility criteria for anti-amyloid therapy and assessed using comprehensive NPTs.
In this study, we aimed to examine whether LM performance may provide additional clinical information to help triage patients who may benefit from confirmatory biomarker testing within a clinically selected cohort. We hypothesized that LM performance would be significantly lower in Aβ-positive (Aβ+) than in Aβ-negative (Aβ−) individuals, even after accounting for relevant demographic and cognitive factors.
Methods
Study design
This retrospective observational study was conducted at the lecanemab outpatient clinic of Kobe City Medical Center General Hospital. Participants were consecutively recruited between December 2023 and March 2025.
Participants
The screening process is summarized in Figure 1. The diagnostic workflow included an initial neurological examination; global cognitive assessment using the Mini-Mental State Examination (MMSE) 10 and Clinical Dementia Rating (CDR) 11 ; structural magnetic resonance imaging (MRI); comprehensive NPT battery; and amyloid positron emission tomography (PET). Inclusion criteria were based on Japanese lecanemab guidelines 12 and included a diagnosis of mild cognitive impairment due to AD or mild AD according to the 2012 criteria of the National Institute on Aging and the Alzheimer's Association, 13 an MMSE score of 22–30, and a CDR global score (CDR-GS) of 0.5 or 1.0. Participants were required to be MRI-compatible and capable of providing informed consent. Exclusion criteria included MRI findings such as > 5 cerebral microbleeds (≤ 10 mm) or a single macrohemorrhage > 10 mm. Through this screening process, participants for whom alternative causes of dementia were suspected were excluded. Only individuals who were clinically considered likely to have early AD underwent amyloid PET for the purpose of determining eligibility for anti-amyloid monoclonal antibody therapy.
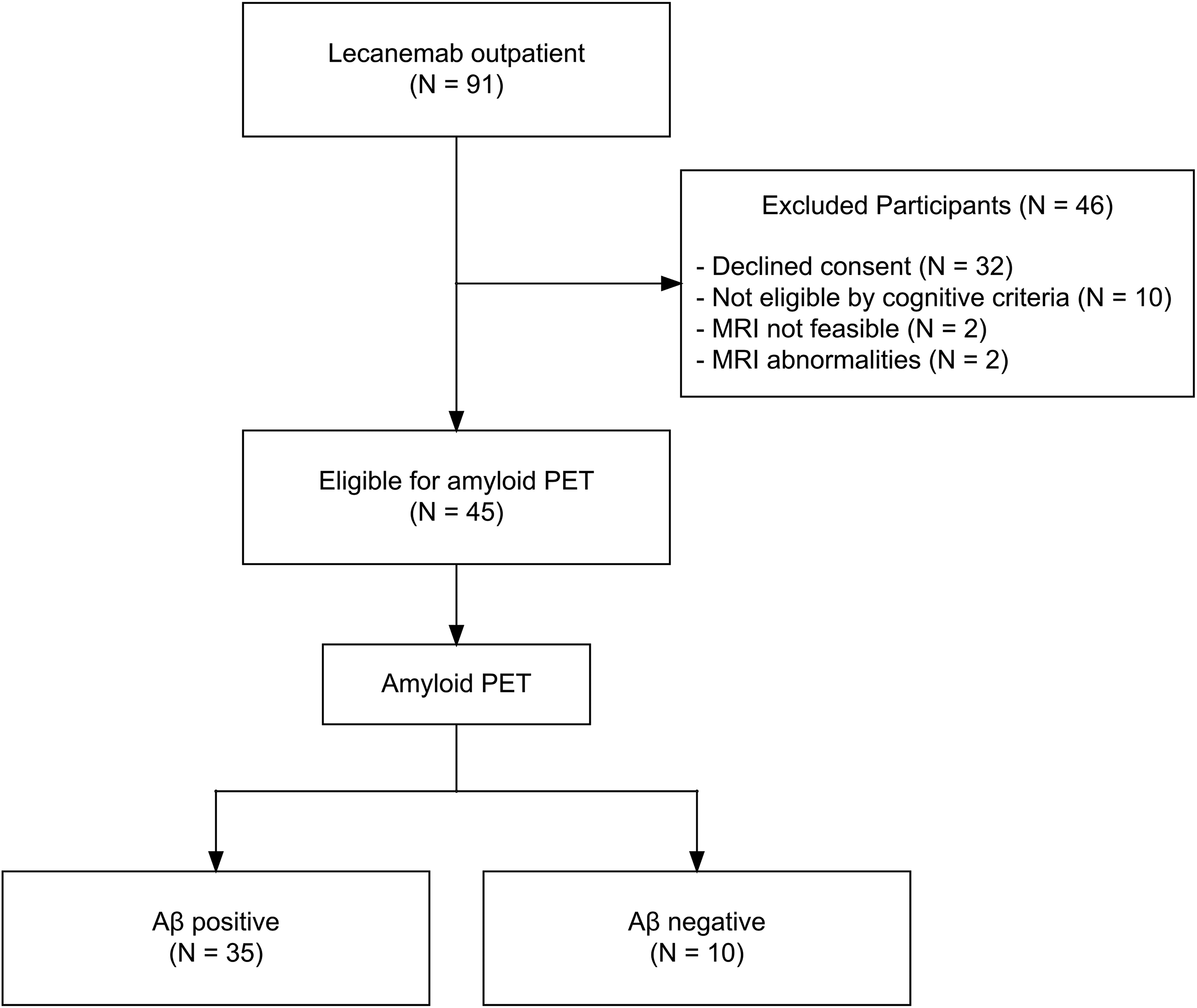
Flowchart of participant screening and eligibility assessment for lecanemab therapy.
Eligible participants underwent amyloid status classification and were categorized into Aβ+ and Aβ− groups for analysis. When clinically indicated, the cerebrospinal fluid (CSF) Aβ42/40 ratio was obtained with additional consent. With additional consent, apolipoprotein E (APOE) genotyping was conducted in a subset of Aβ+ individuals. The study was approved by the institutional review board of Kobe City Medical Center General Hospital (approval number: zn240711), and written informed consent was obtained from all participants or their legal guardians.
Amyloid status classification
Aβ positivity was determined through a multidisciplinary process. Amyloid PET scans were visually interpreted by board-certified nuclear medicine physicians following established clinical guidelines. 14 Findings were reviewed by multiple board-certified neurologists, integrating clinical data, MRI, cerebral blood flow single-photon emission computed tomography and CSF Aβ42/40 ratio (when available). In cases of discordance between amyloid PET and CSF Aβ42/40 ratio, PET findings were given precedence, as amyloid PET is performed under the Japanese national health insurance system and is considered the reference standard for eligibility assessment. Quantitative standardized uptake value ratios (SUVRs) and centiloid values were calculated for reference but were not used as diagnostic criteria.
Neuropsychological assessments
The comprehensive NPT battery was administered within 1 month of amyloid PET by trained examiners using standardized procedures. Assessed tests included multiple domains: immediate memory was assessed using WMS-R LM immediate recall (LMIR), delayed memory was assessed using WMS-R LM delayed recall (LMDR) and Rey–Osterrieth Complex Figure (ROCF) 15 delayed recall, attention and processing speed were assessed with the Trail Making Test Part A (TMT-A), 16 executive function was assessed with the Frontal Assessment Battery (FAB) 17 and Trail Making Test Part B (TMT-B), 16 language was assessed using letter fluency (LF), and visuospatial functioning was assessed using the ROCF copy. LM consisted of two brief stories read aloud by the examiner; LMIR assessed immediate recall, while LMDR evaluated delayed recall after 30 min. Verbatim scoring procedures were applied to LMIR and LMDR based on the WMS-R administration manual. 6 All other measures were scored according to standardized procedures.
Neuroimaging procedures
Amyloid PET imaging was performed using [18F]flutemetamol (Vizamyl®, 185 MBq; 90-min uptake) or [18F]florbetapir (Amyvid®, 370 MBq; 50-min uptake) on a Discovery IQ PET/computed tomography system (GE Healthcare, Chicago, IL, USA) with 3D ordered subset expectation maximization reconstruction (12 subsets, five iterations, 4-mm Gaussian filter). Images were spatially normalized to Montreal Neurological Institute space (DARTEL for flutemetamol, standard nonlinear normalization for florbetapir). SUVRs were calculated using the pons (flutemetamol) or whole cerebellum (florbetapir) as the reference region, and centiloid values were derived from SUVRs.18,19
MRI was acquired using a 1.5-T SIGNA Explorer scanner (GE HealthCare, Chicago, IL, USA) with an eight-channel phased-array head coil. The protocol included 3D T1-weighted gradient-echo (LAVA), fluid-attenuated inversion recovery, diffusion-weighted imaging, T2*, and magnetic resonance angiography sequences. Key acquisition parameters for 3D T1-weighted imaging were TR = 7.17 ms, TE = 4.44 ms, flip angle = 12°, slice thickness = 0.9 mm, and FOV = 256 × 256 mm. SPECT was performed using [123I]iodoamphetamine (111 MBq, IV), on dual-head gamma cameras (Discovery NM/CT 670 or Infinia Hawkeye 4, GE HealthCare, Chicago, IL, USA) with acquisition beginning 15 min post-injection. Images were normalized to Montreal Neurological Institute space using medi + FALCON (Version 1.4; Nippon Medi-Physics Co., Ltd, Tokyo, Japan), and Z-score maps were generated using the normal database method. All imaging was performed by experienced radiologic technologists and interpreted by board-certified nuclear medicine physicians.
Statistical analysis
Group comparisons of demographic and neuropsychological variables were performed using independent-sample t-tests or Wilcoxon rank-sum tests (continuous variables) or Fisher's exact tests (categorical variables). To evaluate the discriminative value of LM for Aβ status, receiver operating characteristic analyses were performed to estimate the area under the curve (AUC) and determine optimal cutoff scores. Trend analyses were performed using the Cochran–Armitage trend test to assess graded associations between LM scores and Aβ positivity rates. Multivariable logistic regression analyses were conducted to evaluate LMIR and LMDR as independent predictors of Aβ positivity, with adjustment for age and sex. Odds ratios (ORs), 95% confidence intervals (CIs), AUCs, and Akaike information criterion (AIC) were reported. Analyses examined the association between LM scores and centiloid values using Spearman's rank correlation and simple linear regression. Missing data were handled by listwise deletion. Statistical significance was set at p < 0.05. All analyses were performed using R (version 4.3.2; R Core Team, 2023).
Results
Demographics and clinical characteristics
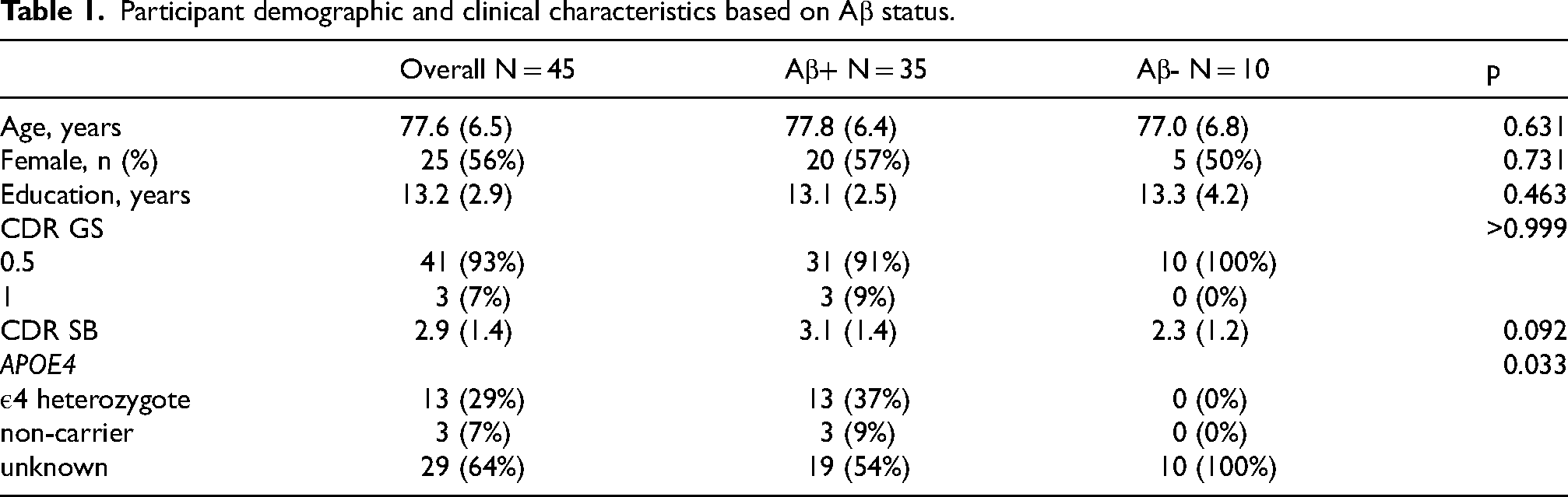
Demographic and clinical characteristics are summarized in Table 1. Of the 91 individuals initially recruited, 46 were excluded (32 declined consent, 10 did not meet cognitive eligibility criteria, 2 were unable to undergo MRI, and 2 had abnormal MRI findings). The remaining 45 participants underwent amyloid PET scanning, with 35 classified as Aβ+ and ten as Aβ−. There were no significant differences between groups in age (mean [standard deviation; SD]: 77.8 [6.4] versus 77.0 [6.8], p = 0.631), sex (male: 43% versus 50%, p = 0.731), or years of education (13.1 [2.5] versus 13.3 [4.2] years, p = 0.468). For CDR-GS, 91% and 9% of the Aβ+ group had scores of 0.5 and 1.0, respectively, compared with 100% and 0% of the Aβ− group. APOE4 genotype data were available for only a subset of Aβ+ participants, among whom 37% were heterozygotes and 9% were non-carriers.
Participant demographic and clinical characteristics based on Aβ status.
Neuropsychological performance
Detailed NPT results are presented in Table 2. All 45 participants (Aβ+ = 35, Aβ− = 10) completed the NPT battery. LMIR scores were significantly lower in the Aβ+ group compared with the Aβ− group (median [Q1–Q3]: 5.0 [3.0–7.0] versus 9.0 [8.0–13.0], p = 0.011). LMDR showed a similar trend (0.5 [0.0–1.5] versus 3.0 [2.0–5.0], p = 0.017). No significant between-group differences were observed for MMSE (p = 0.144), MMSE 3-word delayed recall (p = 0.283), FAB (p = 0.765), LF (p = 0.463), TMT-A (p = 0.682), TMT-B (p = 0.254), ROCF copy (p = 0.793), ROCF 3-min delayed recall (p = 0.366), or ROCF 30-min delayed recall (p = 0.774).
Neuropsychological test performance by Aβ status.
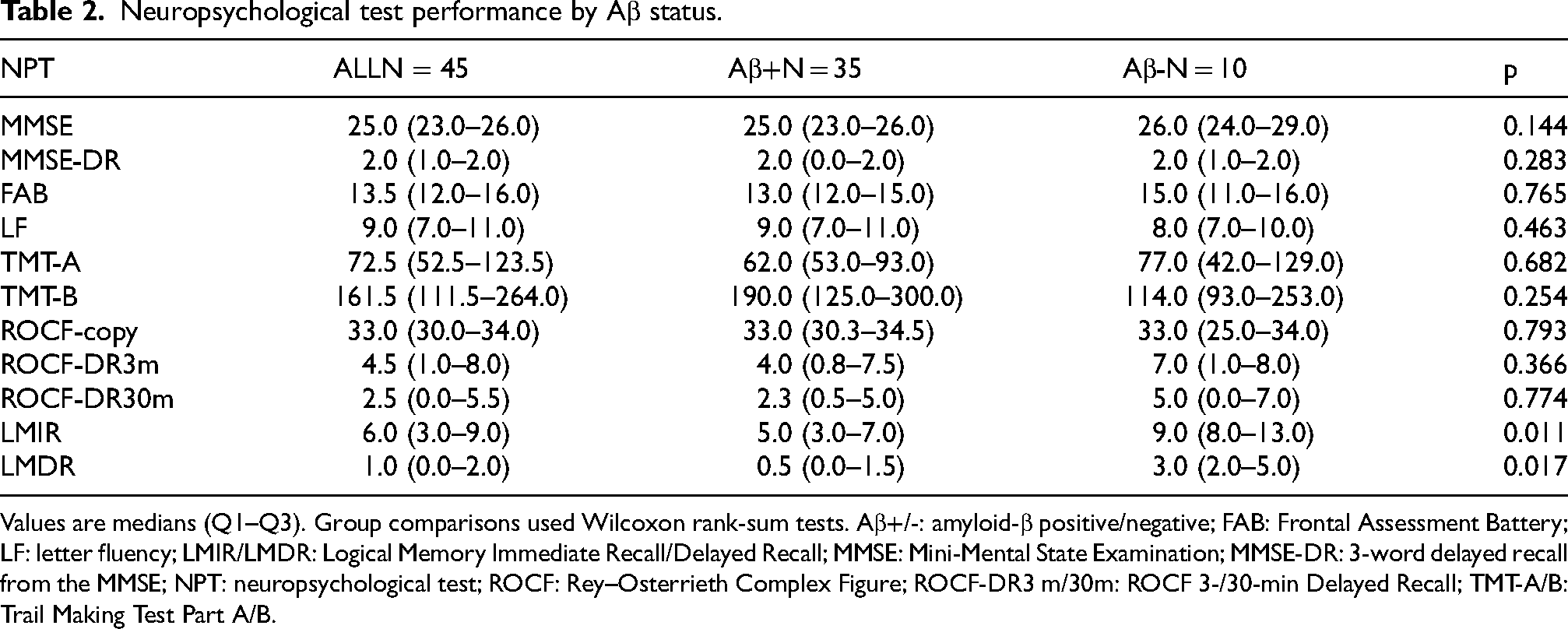
Values are medians (Q1–Q3). Group comparisons used Wilcoxon rank-sum tests. Aβ+/-: amyloid-β positive/negative; FAB: Frontal Assessment Battery; LF: letter fluency; LMIR/LMDR: Logical Memory Immediate Recall/Delayed Recall; MMSE: Mini-Mental State Examination; MMSE-DR: 3-word delayed recall from the MMSE; NPT: neuropsychological test; ROCF: Rey–Osterrieth Complex Figure; ROCF-DR3 m/30m: ROCF 3-/30-min Delayed Recall; TMT-A/B: Trail Making Test Part A/B.
Association of LMIR and LMDR with Aβ positivity
Detailed results are provided in Table 3 and Figure 2. Receiver operating characteristic analyses demonstrated that LMIR had an AUC of 0.79 (95% CI: 0.61–0.97) with a cutoff of 7.5 (sensitivity: 79%, specificity: 77%, PPV: 90%, NPV: 58%). LMDR yielded an AUC of 0.76 (95% CI: 0.55–0.97) with a cutoff of 1.5 (sensitivity: 75%, specificity: 77%, PPV: 90%, NPV: 54%). The Cochran–Armitage trend test showed a significant linear relationship between LMIR scores and Aβ positivity (p = 0.01); a similar significant trend was observed for LMDR scores (p = 0.02). Lower LMIR scores were significantly associated with Aβ positivity (OR: 0.80, 95% CI: 0.64–0.95, p = 0.020), with an AIC of 36.0 and an AUC of 0.79. In the adjusted model, the association between LMIR and Aβ positivity remained significant (OR: 0.81, 95% CI: 0.63–0.96, p = 0.037), with an AIC of 39.6 and an AUC of 0.81. Lower LMDR scores were also significantly associated with Aβ positivity (OR: 0.64, 95% CI: 0.38–0.91, p = 0.048), with an AIC of 35.0 and an AUC of 0.76. In the adjusted model, the association between LMDR and Aβ positivity remained significant (OR: 0.62, 95% CI: 0.37–0.91, p = 0.040), with an AIC of 38.1 and an AUC of 0.81. For comparison, a baseline model including age and sex alone demonstrated poor discrimination (AUC: 0.54; AIC: 53.5).
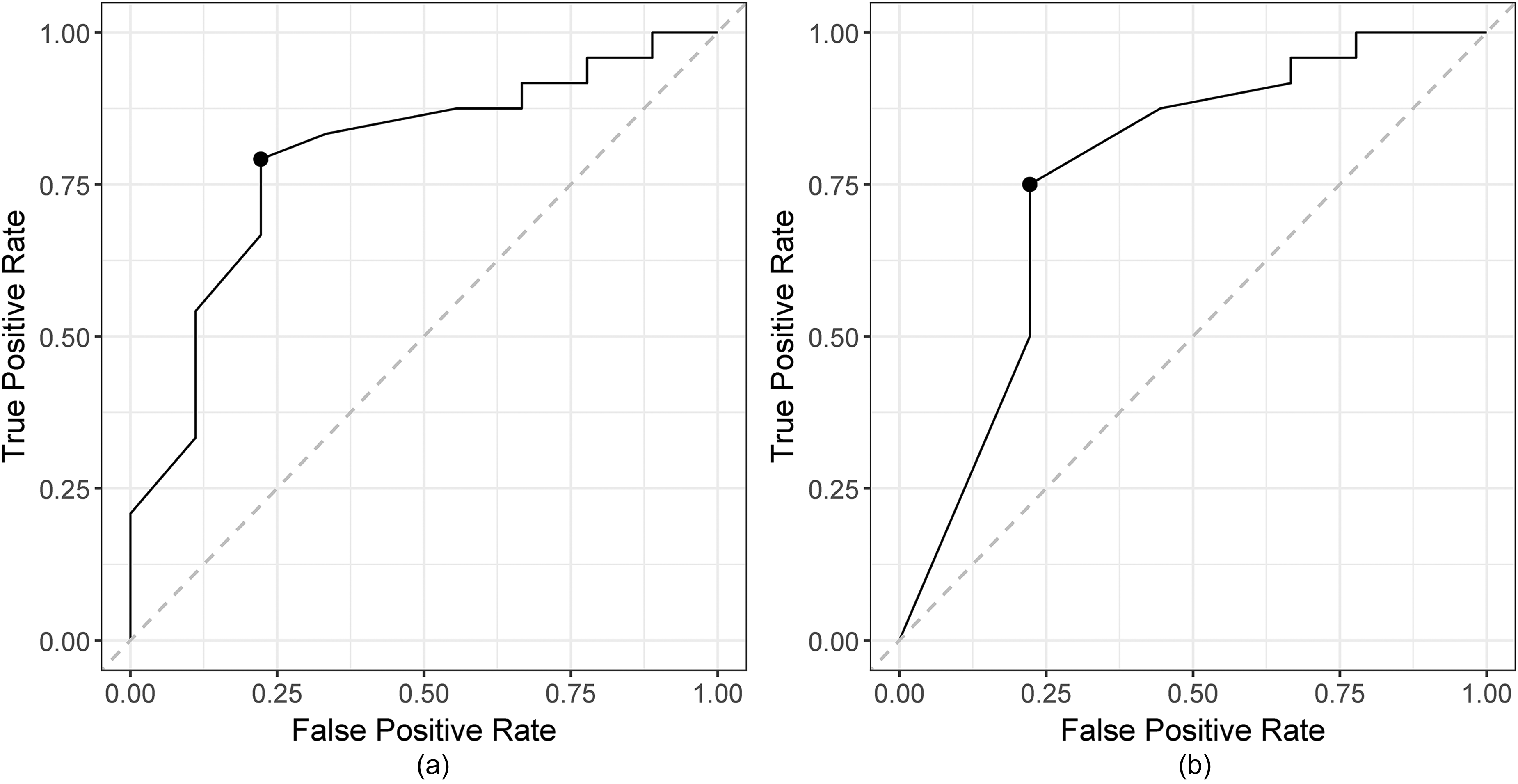
Receiver operating characteristic curves for predicting Aβ positivity using LMIR and LMDR.
Multivariate logistic regression results with AUC.
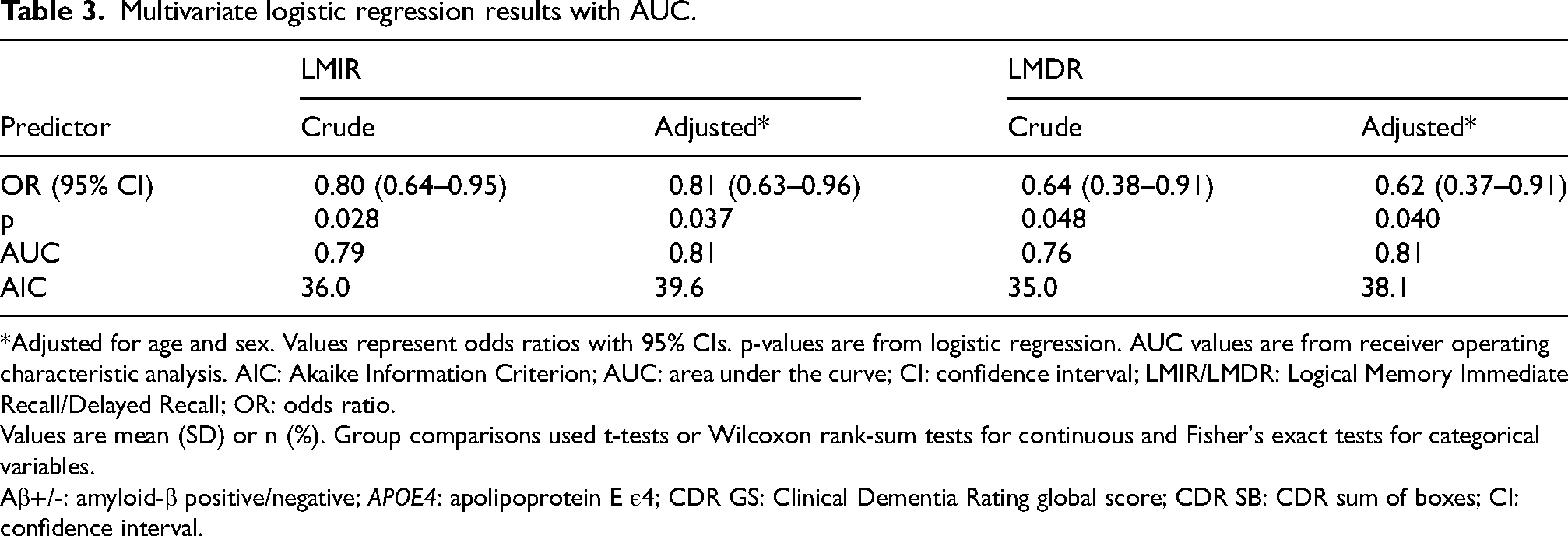
*Adjusted for age and sex. Values represent odds ratios with 95% CIs. p-values are from logistic regression. AUC values are from receiver operating characteristic analysis. AIC: Akaike Information Criterion; AUC: area under the curve; CI: confidence interval; LMIR/LMDR: Logical Memory Immediate Recall/Delayed Recall; OR: odds ratio.
Values are mean (SD) or n (%). Group comparisons used t-tests or Wilcoxon rank-sum tests for continuous and Fisher's exact tests for categorical variables.
Aβ+/-: amyloid-β positive/negative; APOE4: apolipoprotein E ε4; CDR GS: Clinical Dementia Rating global score; CDR SB: CDR sum of boxes; CI: confidence interval.
Spearman's rank correlation showed a negative association between LMIR and centiloid values (ρ = −0.51, p = 0.002), and a weaker but still significant negative association for LMDR (ρ = −0.38, p = 0.027). Simple linear regression analyses yielded similar findings. LMIR scores were significantly associated with centiloid values (β = −3.97, 95% CI: −6.62 to −1.32, p = 0.005), and LMDR scores also showed a significant association (β = −4.69, 95% CI: −8.37 to −1.02, p = 0.014, R2 = 0.18). Residuals from both models did not violate the normality assumption (Shapiro-Wilk p > 0.4).
Discussion
This study demonstrated that the WMS-R LM subtest is significantly associated with Aβ accumulation in individuals with early AD. In a cohort selected according to lecanemab eligibility, LM consistently distinguished Aβ+ from Aβ− individuals. Lower LM immediate and delayed recall scores were associated with increased amyloid burden, supporting a robust association between LM performance and Aβ accumulation.
The association between Aβ deposition and cognitive decline has long been debated.20,21 Braak staging has emphasized tau pathology as the major correlate of cognitive impairment, but amyloid PET has enabled in vivo visualization of Aβ accumulation and has provided evidence that Aβ deposition often precedes overt cognitive decline.22,23 Aβ deposition begins in the precuneus, posterior cingulate cortex, and medial and lateral orbitofrontal regions (stage 1), and progressively spreads. Longitudinal studies have shown that more than half of stage 1 individuals progress to stages 2–3 (mild cognitive impairment-equivalent) within 2 years, with memory decline beginning during stage 2. 22 Notably, prior PET studies have demonstrated a spatial overlap between Aβ deposition and regions of the default-mode network (DMN), particularly in the precuneus and posterior cingulate cortex, and have further reported a correlation between regional aerobic glycolysis in young adults and later Aβ accumulation. 24 These findings suggest that intrinsic metabolic characteristics of DMN regions may confer vulnerability to Aβ pathology. Our findings align with these data, suggesting that LM decline captures the earliest stage of clinically meaningful cognitive change related to Aβ pathology. However, these findings should be considered hypothesis-generating and require further investigation for validation, as the observed associations do not establish a causal relationship between LM decline, DMN dysfunction, and Aβ deposition.
LM, but not ROCF delayed recall, or MMSE 3-word recall, distinguished Aβ+ from Aβ− participants, which may reflect the neural networks each task engages. LM tasks strongly depend on DMN, including the posterior cingulate cortex, precuneus, medial prefrontal cortex, and hippocampal formation, which are vulnerable to early Aβ deposition.22,25–28 DMN disruption impairs narrative encoding and contextual integration, processes critical for LM performance.29,30 In contrast, ROCF primarily relies on visuospatial construction, and MMSE recall relies on rote memory, which are less dependent on DMN integrity. Although the present study was cross-sectional and does not establish a direct neural mechanism, the pattern of associations observed across tasks is broadly consistent with current neurobiological models.
This study had some limitations. First, it was conducted at a single center with a relatively small and imbalanced sample, which limits statistical power and the stability of effect estimates and restricts the number of covariates that could be included in multivariable models. Accordingly, the discriminative analyses should be regarded as exploratory, and validation in larger multicenter cohorts is warranted. Second, as this was a cross-sectional study conducted in a clinically preselected cohort, the observed association between the LM subtest and Aβ accumulation should be interpreted with caution. Further studies are needed to clarify the potential causal relationships among LM performance, amyloid accumulation, and DMN disruption. Third, although participants were clinically screened and amyloid PET was used to confirm eligibility for anti-amyloid therapy, the inclusion of individuals who may not progress to AD or who have non-AD pathology cannot be fully excluded. This heterogeneity may influence the observed association between LM performance and Aβ accumulation. Therefore, our findings should be interpreted within a clinically defined, amyloid-positive population, and they do not indicate that LM can differentiate underlying pathologies. Finally, LM was administered to participants aged ≥ 75 years, exceeding the original standardized age range of the WMS-R; this approach was adopted because supplementary normative references for older adults have been reported.31,32 However, given the limited availability of formally standardized normative data for individuals aged ≥ 75 years, LM scores in this age group should be interpreted with caution.
In conclusion, in a cohort clinically preselected as having early AD according to lecanemab eligibility criteria, the LM subtest was significantly associated with amyloid-β accumulation.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to Kohei Hayase, Yurina Nishio, and Manami Deguchi, speech-language pathologists from the Department of Rehabilitation, Kobe City Medical Center General Hospital, for their cooperation in conducting neuropsychological assessments and collecting data. We also extend our appreciation to Koyama Hiroyuki and Keiji Shimizu, and radiological technologists in the Department of Radiation Technology of the same institution, for their contributions to neuroimaging acquisition and data processing.
Ethical considerations
The study was approved by the institutional review board of Kobe City Medical Center General Hospital (approval number: zn240711).
Consent to participate
Written informed consent was obtained from all participants or their legal guardians.
Consent for publication
Not applicable
Author contributions
Please replace this text with the Manuscript Author Contributions sent in the Manuscript metadata/information from Sage Track.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was supported by a research grant from Astellas Foundation for Research on Metabolic Disorders (Grant Number 2024A4025).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated or analyzed during the current study are not publicly available due to ethical and privacy restrictions.