
Abstract
Background
While Alzheimer's disease (AD) is a known risk factor for falls, the association between falls and incident AD is a growing area of study.
Objective
The primary aim of this analysis was to examine associations between new-onset falls in older adults and neuroimaging and plasma biomarkers of AD. A secondary aim was to evaluate associations between new-onset falls and neuroimaging markers of motor dysfunction.
Methods
Data from the UK Biobank study was utilized. Participants were 70 years of age or older at the date of neuroimaging and had no reported history of falls at study enrollment. To determine falls status, participants self-reported data on falls history within the last year prior to neuroimaging.
Results
15,447 individuals were included in our analysis (No falls, N = 12,522; One fall, N = 2,199, Multiple falls, N = 726). Compared to individuals in the No falls group, individuals in the One fall and Multiple falls group had significantly higher volumes of white matter hyperintensities, while individuals in the Multiple falls group had significantly lower left and right hippocampal volumes. One or more fall was associated with higher plasma levels of pTau181, which did not remain significant after adjusting for multiple comparisons. Plasma amyloid-β 42/amyloid-β 40 ratio did not differ significantly between groups.
Conclusions
In a sample of older adults without history of falls at study enrollment, new-onset falls were associated with decreased hippocampal volumes, which is associated with prodromal AD, as well as an increased volume of white matter hyperintensities, which may also emerge secondary to AD pathology.
Introduction
Alzheimer's disease (AD) is a leading cause of morbidity and mortality worldwide. 1 In recent years, efforts have been made to characterize and treat neuropsychiatric symptoms (NPS), which occur almost universally in patients with dementia most often before the advent of severe cognitive decline. 2 However, less is known about other non-cognitive manifestations of AD, such as motor symptoms, which commonly include gait disturbance and falls. Motor symptoms in AD are not only associated with more severe NPS 3 and more rapid cognitive decline, 4 but are also known to decrease caregiver quality of life.5,6
Of these motor symptoms, falls are of particular interest, given their association with both frailty and mobility impairment. 7 AD and other dementias have been shown to be a risk factor for falls, 8 but the inverse relationship between falls and incident AD is a growing area of study. In a retrospective cohort study using electronic health record (EHR) data, falls were independently associated with an increased risk of all-cause dementia. 9 Additional research using the UK Biobank (UKB) study found that falls were associated with a higher risk of incident dementia, including AD and vascular dementia. 10
Physical activity is one domain by which motor symptoms, including falls, may impact cognitive outcomes in older age. Increased physical activity was associated with a lower risk of dementia in prior analyses,11,12 and in the form of structured exercise interventions may improve global cognitive function and functional independence in AD patients. 13 One hypothesis is that motor symptoms such as falls may hinder AD patients from benefiting from the protective effects of exercise on cognitive function, thereby precipitating more rapid clinical decline. 4
Together, past findings suggest that falls may help to identify a subpopulation of older adults at risk for incident AD or worse AD outcomes. However, less is known as to the mechanisms through which falls may contribute to AD risk and/or be a marker of early AD. More specifically, the relationship between falls during later life and neuroimaging and plasma markers of AD has yet to be studied, which may elucidate potential neurophysiological mechanisms through which falls may impact AD trajectory, with possible implications for intervention.
Using the UKB dataset, we selected a subgroup of older adults without history of falls at study enrollment, and examined the cross-sectional associations between new-onset falls within the year prior and plasma and neuroimaging markers of AD. In addition, we examined the association between new-onset falls and cortical and subcortical neuroimaging markers of motor dysfunction. An exploratory aim was to examine the relationship between new-onset falls and levels of physical activity measured via wrist-worn actigraphy. We hypothesized that falls would be associated with reduced hippocampal and temporal lobe volumes, reduced motor-related cortical and subcortical region volumes, and higher levels of AD-related plasma biomarkers, including a lower amyloid-β 42 (Aβ42)/amyloid-β 40 (Aβ40) ratio.
Methods
Study design and population
This cross-sectional analysis utilized data from the UKB study. Detailed study protocols are available on the UKB website (https://www.ukbiobank.ac.uk/). Briefly, between 2006–2010, over 500,000 individuals visited one of 22 assessment research centers across Scotland, England and Wales for study enrollment. 14 Our analysis primarily utilized data from a follow-up timepoint (“neuroimaging visit”) between 2015–2020, which included magnetic resonance imaging (MRI) scans, plasma biomarkers of AD and neurodegeneration, and cognitive performance tests. The UKB has research ethics approval from the Northwest Multi-Centre Research Ethics Committee as a research tissue bank.
Inclusion criteria
Inclusion criteria for this analysis are outlined in Figure 1, comprising a total 15,447 eligible participants. Participants were required to be 70 years of age or older at the date of neuroimaging and have available data for at least one neuroimaging outcome of interest. This age cutoff restricted the sample to individuals at high risk of AD onset and progression, consistent with prior analyses investigating AD risk. 15 In addition, participants were required to have complete data for the covariates of interest (see below).
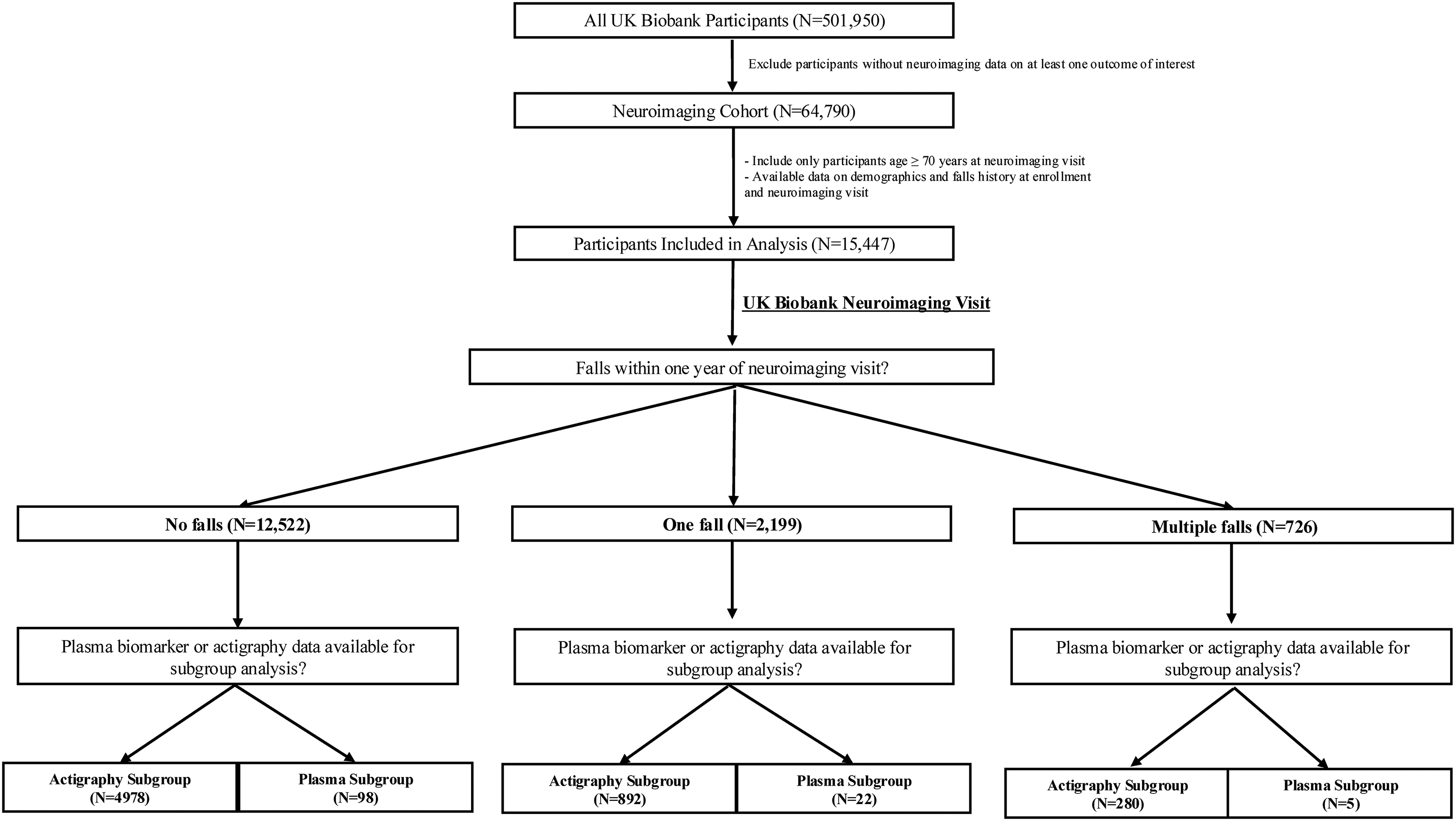
Inclusion criteria for participants (N = 15,447) included in this analysis. Major inclusion criteria included age ≥ 70 years at the neuroimaging timepoint and no history of falls at the enrollment timepoint.
To determine falls status, participants self-reported data on history of falls within the last year prior to the date of neuroimaging (UKB field ID #2296). Responses were categorized as follows: no falls within the last year (“No falls” group), only one fall within the last year (“One fall” group), and more than one fall within the last year (“Multiple falls” group). Participants with self-reported history of falls within the year prior to study enrollment (approximately 10 years prior to neuroimaging) were excluded from our analysis. This subgroup was isolated in efforts to capture a cohort of individuals with new-onset falls rather than a cohort with a chronic, recurrent history of falling.
Measures of neurocognition
To assess cognition at the neuroimaging visit, performance on a numerical and verbal reasoning test designed to test fluid intelligence (the capacity to solve problems that require logic and reasoning ability) was reported on when available (N = 13,679). 16 This UKB fluid intelligence test (UKB field ID: 20016) has been observed to be negatively associated with age and positively associated with validated tasks of working memory and non-verbal reasoning. 16 In addition, a numeric memory test (UKB field ID: 4282) was also reported on when available (N = 8,996), which has been shown to be strongly correlated with the validated Mini-Addenbrooke's Cognitive Examination (M-ACE). 17 Finally, performance on the UKB prospective (shape) memory task (UKB field ID: 20018) was reported on when available (N = 14,002), which was dichotomized as either correct or incorrect on the first attempt.16,18 This short battery of tasks was selected to capture domains of cognition, including executive function and working memory, that are known to be affected in mild cognitive impairment (MCI) and AD. 19 Lack of population norms on these tests of cognition prevented categorization of participants into stages of cognitive decline (i.e., normal cognition versus MCI) at the neuroimaging visit, and unfortunately only a small subset of individuals had EHR data on dementia diagnoses available at a later timepoint which was not reported on in this analysis.
Neuroimaging markers of Alzheimer's disease and motor dysfunction
The UKB imaging data were collected using a 3T Siemens scanner with a 32-channel head coil. T1-weighted structural brain MRI was collected on all individuals eligible for this analysis (N = 15,447). 20 Regional grey matter volumes were collected via FAST scans, processed and pre-calculated by the UKB. T2-weighted imaging was used to measure the total volume of white matter hyperintensities (WMH). Total WMH volume in the UKB was calculated automatically using FSL's BIANCA tool, which segments white-matter lesions primarily from T2 FLAIR images with T1 data as an additional input. 21
AD-related neuroimaging outcomes included: left and right total hippocampal volume (UKB Field IDs: 25019 & 25020), left and right grey matter temporal pole volume (UKB Field IDs: 25796 & 25797), and volume of total WMH (UKB Field ID: 25781). Hippocampal atrophy on MRI has emerged as a consistent biomarker of MCI and AD,22,23 while the temporal pole may display atrophy during early AD. 24 WMH may emerge secondary to AD pathology in addition to as a presumed biomarker of cerebrovascular disease. 25 Whole brain volume normalized for head size (UKB Field ID: 25009) was also included as a primary outcome measure given its association with progression to AD in older adults. 23
Neuroimaging variables related to motor dysfunction included left and right grey matter volumes of the caudate (UKB Field IDs: 25880 & 25881), putamen (UKB Field IDs: 25882 & 25883), precentral gyrus (UKB Field IDs: 25794 & 25795), and postcentral gyrus (UKB Field ID: 25814 & 25815). Grey matter volumes of the sensorimotor cortex (i.e., precentral and postcentral gyrus) and of subcortical structures (i.e., caudate) have been shown to be associated with motor performance and gait difficulty in older adults.26,27
Plasma markers of Alzheimer's disease and neurodegeneration
Plasma markers related to AD and neurodegeneration were collected on a subset of individuals at the neuroimaging visit (N = 125). EDTA plasma samples were sent to the University College London UKDRI Fluid Biomarker Lab for assay on a Quanterix Simoa HD-X Analyser. Plasma markers associated with neurodegenerative disease including neurofilament light (NFL), 28 glial fibrillary acidic protein (GFAP), 29 Aβ42/Aβ40 ratio, 30 and phosphorylated tau181 (pTau181) 31 were included (UKB Field IDs: 31040-31044).
Physical activity assessment
A subset of participants wore an Axivity AX3 wrist-worn triaxial accelerometer (N = 6,150) at 100 Hz, collected between 2013–2016. The UKB accelerometer working group processed and generated data on participants’ physical activity in 5 second periods, using the average vector magnitude in milligravities (mg) to estimate physical activity. For more detail on the classification of activity levels into categories of sedentary time (UKB Field ID: 40047), light activity (UKB Field ID: 40048), moderate-vigorous activity (UKB Field ID: 40049), and sleep time (UKB Field ID: 40046), see Walmsley et al. (2021). 32 A UKB-derived variable (yes/no) encoding for adequate quality and duration of wear time was used to ensure quality of data. Data was not imputed, and the data represent the averages of available data.
Statistical analyses
To assess differences in demographic characteristics between groups, logistic and linear regression were used for categorical (i.e., sex) and continuous (i.e., age at neuroimaging) variables, respectively. The No falls group was specified as the reference group, allowing for direct estimation of differences between each fall group and the reference group.
For primary analyses, multivariable linear regressions were conducted for all neuroimaging variables, with volume of brain region (in mm3) as the dependent variable, falls group as the independent variable (One fall/Multiple falls), and the No falls group as the reference group. Covariates known to be associated with brain volume and/or risk of AD were included in all analyses, including sex, 33 age at neuroimaging, 33 body mass index (BMI) at neuroimaging, 34 ethnicity (White versus Non-White), 35 years of education, 36 and AD polygenic risk score (PRS). 37
Multivariable linear regressions were also conducted for activity outcome variables measured via actigraphy with the same independent variables and covariates as above. For plasma biomarkers, which were also modeled as dependent variables in multivariable linear regressions, the falls variable was dichotomized (Falls/No falls) as the independent variable to maximize statistical power due to low sample size, with the same covariates as above.
Model assumptions were visually evaluated using residuals-versus-fitted plots (see Supplemental Figure 1) to assess linearity and homoscedasticity, and Q–Q plots to assess normality of residuals. 38 Observed deviations from normality were modest and not considered sufficient to justify transformation of outcome variables. To further support inference in the presence of group imbalance and modest violations of normality, nonparametric bootstrapping with 5,000 resamples was performed for all primary and supplemental analyses. 39 Bias-corrected and accelerated (BCa) confidence intervals were calculated, and one-tailed p-values were derived from the empirical bootstrap distribution based on a priori directional hypotheses. The threshold for statistical significance was α = 0.05. Class imbalance correction methods were not applied, as prior evidence suggests that these methods may overestimate the probability of the minority class (i.e., individuals with falls) without improving the discrimination of individuals with and without the outcome of interest. 40
All analyses were restricted to participants with available data for the relevant outcome. To correct for multiple hypothesis testing, we applied the Benjamini–Hochberg (BH) procedure to control the false discovery rate (FDR) at 5% (FDR = 0.05) for all primary analyses, producing adjusted p-values (q-values). 41 Analyses were performed using R, version 4.4.1 (2024-06-14), 42 and RStudio version 2023.12.0. 43
Results
Demographic characteristics
15,447 individuals were included in our analysis. Mean [SD] age of all participants at recruitment was 62.5 [3.5] years and at neuroimaging was 73.8 [3.1] years, 8731 (56.5%) were male, and ethnic distribution was as follows: 15107 (97.8%) white, 49 (0.3%) Black, 158 (1.0%) Asian, and 133 (0.9%) Other/Unknown. Mean [SD] years of education was 16.0 [4.8], and mean [SD] BMI in kg/m2 was 26.2 [4.0]. 2,199 individuals had a self-reported history of one fall within one year of neuroimaging, while 726 individuals had a self-reported history of multiple falls within one year of neuroimaging. Demographic characteristics of study groups are reported in Table 1. Of note, mean performance on tasks of numeric memory and fluid intelligence, as well as proportion of correct responses on a prospective memory task, did not differ significantly between groups.
Demographic characteristics for participants (N = 15,447) included in this analysis.
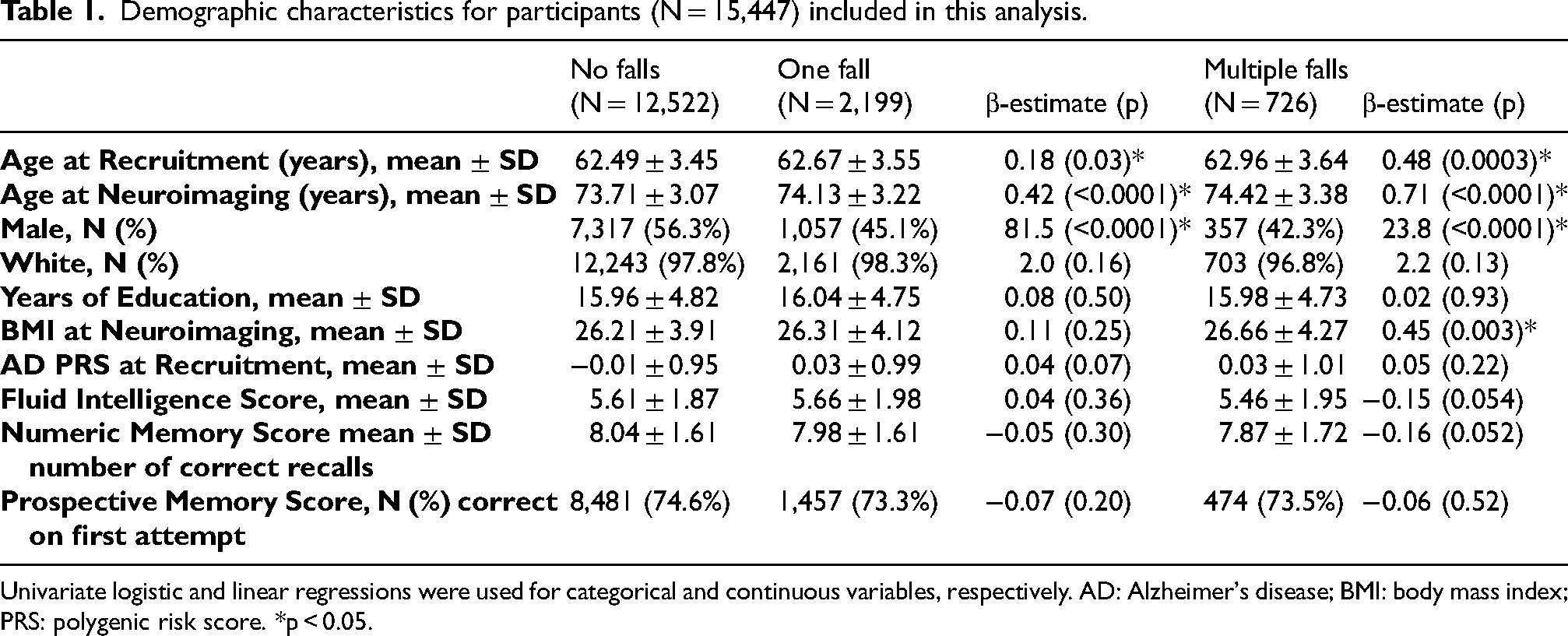
Univariate logistic and linear regressions were used for categorical and continuous variables, respectively. AD: Alzheimer's disease; BMI: body mass index; PRS: polygenic risk score. *p < 0.05.
Relationship between falls and neuroimaging and plasma markers of Alzheimer's disease (Aim 1)
Bootstrapped linear regression analyses of associations between new-onset falls and neuroimaging (N = 15,447) and plasma biomarkers (N = 125) of AD are presented in Table 2 and Table 3, respectively. Compared to the No falls group, the One fall group had a significantly higher volume of WMH. Compared to the No falls group, the Multiple falls group had significantly lower left and right hippocampal volumes and a significantly higher volume of WMH. The Multiple falls groups also had significantly lower whole brain and left grey matter temporal pole volumes compared to the No falls group, although these differences did not remain significant after adjusting for the FDR. Differences in whole brain and grey matter temporal pole volumes were not statistically significant between the One fall and No falls groups.
Associations between new-onset falls and Alzheimer's disease related magnetic resonance imaging (MRI) regional brain volumes.
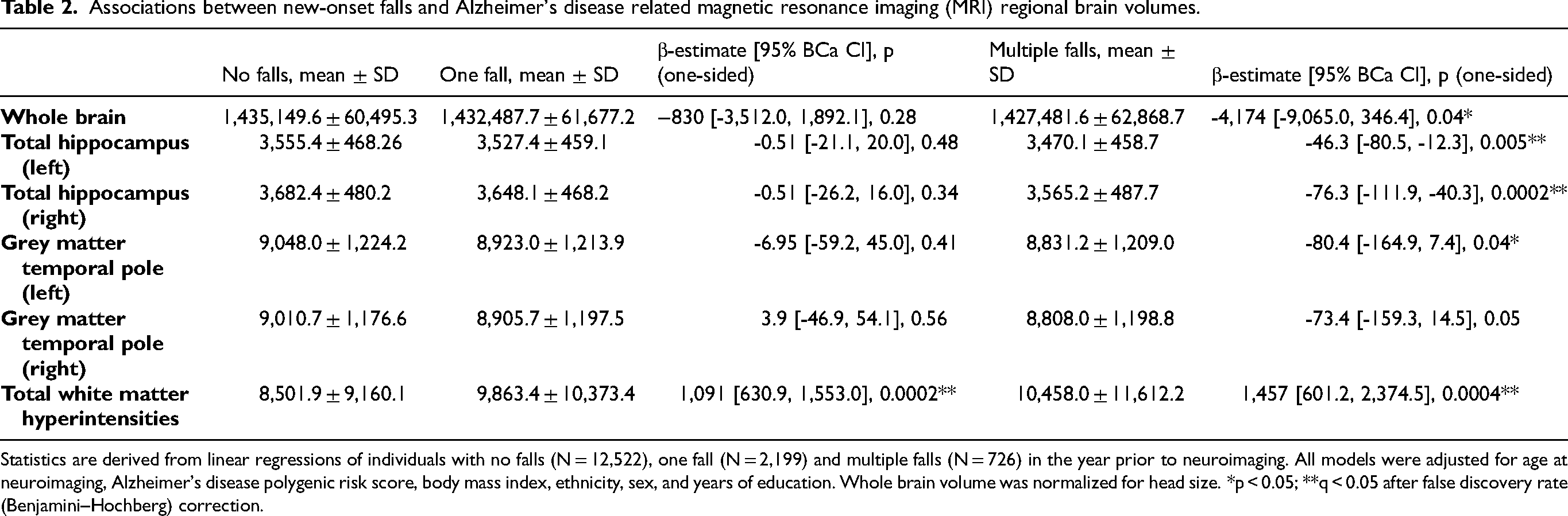
Statistics are derived from linear regressions of individuals with no falls (N = 12,522), one fall (N = 2,199) and multiple falls (N = 726) in the year prior to neuroimaging. All models were adjusted for age at neuroimaging, Alzheimer's disease polygenic risk score, body mass index, ethnicity, sex, and years of education. Whole brain volume was normalized for head size. *p < 0.05; **q < 0.05 after false discovery rate (Benjamini–Hochberg) correction.
Associations between new-onset falls and plasma biomarkers of Alzheimer's disease.
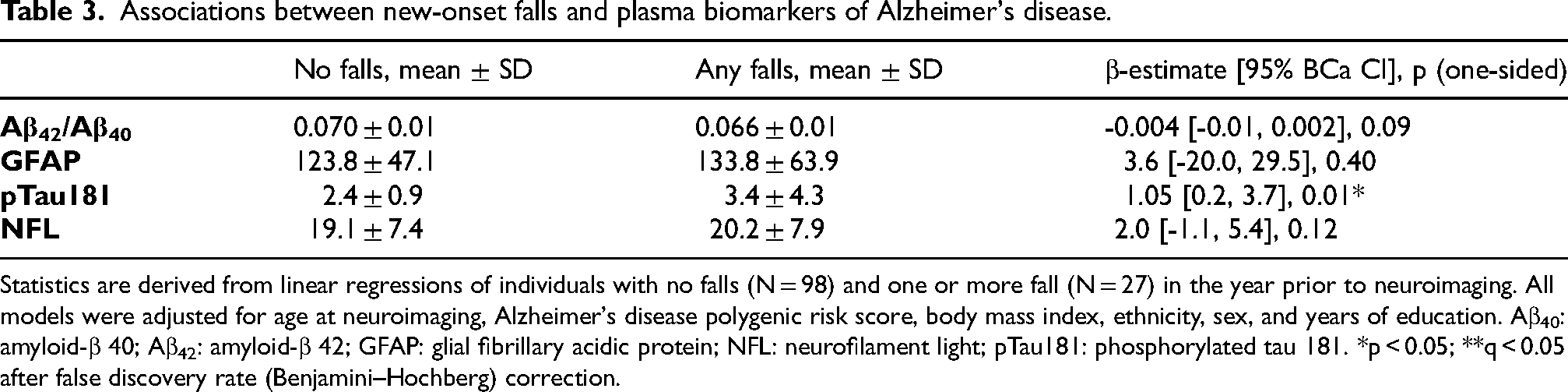
Statistics are derived from linear regressions of individuals with no falls (N = 98) and one or more fall (N = 27) in the year prior to neuroimaging. All models were adjusted for age at neuroimaging, Alzheimer's disease polygenic risk score, body mass index, ethnicity, sex, and years of education. Aβ40: amyloid-β 40; Aβ42: amyloid-β 42; GFAP: glial fibrillary acidic protein; NFL: neurofilament light; pTau181: phosphorylated tau 181. *p < 0.05; **q < 0.05 after false discovery rate (Benjamini–Hochberg) correction.
Compared to the No falls group, individuals with one or more fall had significantly higher plasma levels of pTau181, which did not remain significant after adjusting for the FDR. Groups did not differ significantly in plasma GFAP, NFL or Aβ42/Aβ40 ratio.
Relationship between falls and neuroimaging markers of motor dysfunction (Aim 2)
Bootstrapped linear regressions yielding associations between new-onset falls and neuroimaging markers of motor dysfunction (N = 15,447) are presented in Table 4. Contrary to our study hypotheses, the One Fall group had higher grey matter volumes in the left and right caudate and putamen and the Multiple falls group had higher grey matter volumes in the left and right caudate compared to the No falls group. Conversely, compared to the No falls group, the Multiple falls group had significantly lower grey matter volume in the right postcentral gyrus, while the One fall group had significantly lower grey matter volume in the right precentral gyrus
Associations between new-onset falls and motor dysfunction related magnetic resonance imaging (MRI) regional brain volumes.
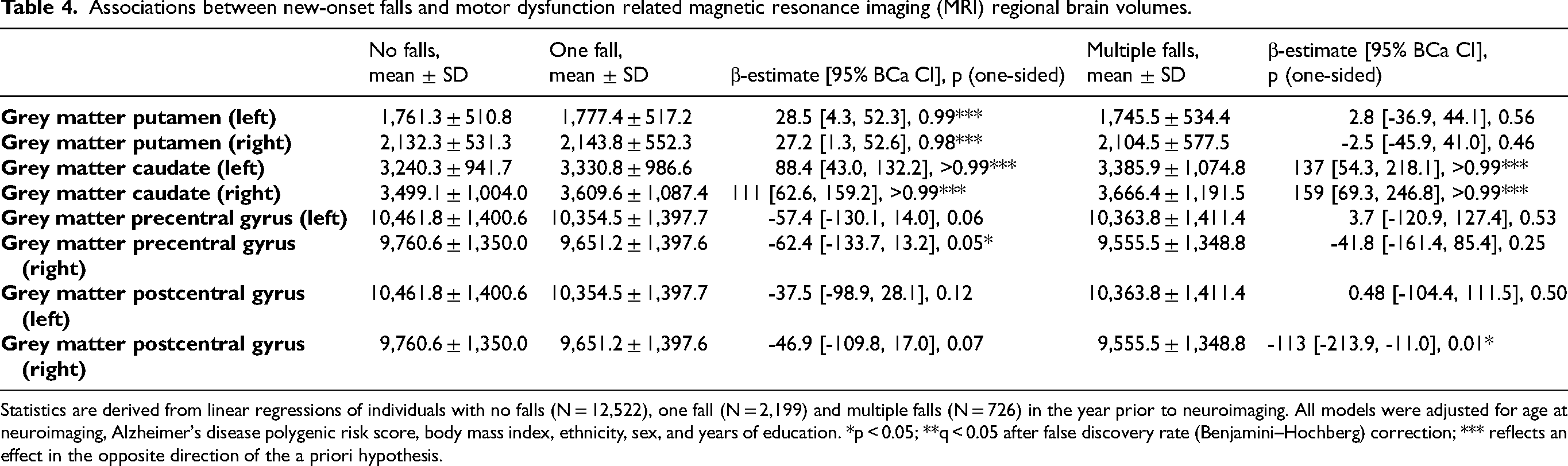
Statistics are derived from linear regressions of individuals with no falls (N = 12,522), one fall (N = 2,199) and multiple falls (N = 726) in the year prior to neuroimaging. All models were adjusted for age at neuroimaging, Alzheimer's disease polygenic risk score, body mass index, ethnicity, sex, and years of education. *p < 0.05; **q < 0.05 after false discovery rate (Benjamini–Hochberg) correction; *** reflects an effect in the opposite direction of the a priori hypothesis.
Relationship between falls and levels of physical activity measured via actigraphy (Exploratory aim)
Finally, bootstrapped linear regressions yielding associations between falls and daily averages of activity data (N = 6,150) during the study period are presented in Supplemental Table 1. Compared to the No falls group, the Multiple falls group had significantly decreased daily average of sedentary time. Otherwise, overall daily averages of sedentary time, light activity, moderate-vigorous activity, and sleep time were not found to be significantly different between groups.
Discussion
In a sample of individuals 70 years of age or older without history of falls at study enrollment, new-onset falls were associated with decreased hippocampal volumes, which is associated with prodromal AD, as well as increased volume of WMH, which is a marker of cerebrovascular disease but may also emerge secondary to AD pathology. In subgroup analyses, new-onset falls were also associated with elevated levels of plasma pTau181, which is a biomarker known to be associated with AD pathology independent of underlying cognition, 44 although this finding did not remain significant after adjusting for multiple comparisons. Our findings suggest that new-onset falls, particularly recurrent falls, may be associated with AD-related neuroimaging changes and may be used by clinicians to screen for those at risk of subsequent cognitive decline.
Our study expands on past work observing a relationship between falls and risk of incident dementia 10 by considering history of falls beyond a year prior to the date of study and utilizing neuroimaging modalities to measure burden of disease. Neuroimaging changes may precede clinical diagnoses of AD and provide valuable information related to the mechanism of associations. In our analysis, we selected a sample of individuals who reported no history of falls at enrollment (approximately 10 years prior to neuroimaging), allowing for more direct ascertainment of the relationship between new-onset falls and AD pathological processes. We also included a subset of cognitive tests related to executive functioning and memory, which did not differ significantly between groups, suggesting that in our sample falls might represent a marker of early AD prior to significant cognitive decline.
Our analysis also separated individuals into three groups (No falls/One fall/Multiple falls), rather than simply creating a dichotomized falls variable combining all individuals with one or more fall. Existing literature suggests that individuals with more than one fall within a year represent a high-risk subset of individuals who experience falls 45 ; while one fall may reflect an isolated event, individuals with recurrent falls are more likely to sustain serious injuries, 46 have distinct risk factors (more severe gait/balance disturbances),47,48 and be at increased risk of functional decline 49 compared to individuals with a single fall event. Our findings supported the idea that individuals with recurrent falls, rather than one fall, are most at risk of poor cognitive outcomes, as hippocampal volumes were only decreased in the Multiple falls group relative to the No falls group.
Our finding that multiple falls were associated with lower hippocampal volumes, which has been identified as an early marker of incident cognitive decline and AD,22,50 replicate those of a much smaller cohort (N = 83) of cognitively normal individuals. 51 Our analysis also identified a graded increase in volume of WMH among the One fall and Multiple falls group, sequentially. While WMH are presumed to be a marker of age-related microvascular changes, a recent study found that WMH were associated with longitudinal increases in positron emission tomography (PET) amyloid uptake and decreased hippocampal volumes on MRI among cognitively normal individuals, suggesting that WMH may also be a marker of early AD-related clinical decline. 52 Burden of WMH has also been found to be associated with an increased incident fall risk over a 12-month period, 53 which highlights the uncertain temporal relationship between falls and neuroimaging changes in our study population.
Beyond neuroimaging markers of disease, we also examined the association between new-onset falls and plasma biomarkers of AD in a subgroup of UKB participants. We observed an association between new-onset falls and levels of plasma pTau181, which did not survive adjustment for the FDR. However, given the limited sample size of available plasma data, this finding warrants further consideration and/or investigation. Our analysis did not observe an association between new-onset falls and plasma Aβ42/Aβ40 ratio, in contrast to prior research observing elevated amyloid burden on PET in patients with slow gait speed 54 as well as elevated cerebrospinal fluid levels of Aβ42 in hip fracture patients without dementia. 55
Our analysis also identified associations between new-onset falls and volumes of brain regions related to motor dysfunction, although these findings did not support our original study hypotheses. Grey matter volume of subcortical regions such as the caudate and putamen were found to be increased or not significantly different, rather than decreased, in individuals with falls. Sparing of neurodegeneration of subcortical regions such as the putamen decreases the likelihood that falls in this sample were consistent with parkinsonian features related to dopaminergic dysfunction and rather may be more reflective of general cortical atrophy/neurodegeneration. Neurodegeneration in the precentral gyrus, indicated by cortical thickness, was previously associated with slower walking speed among individuals with normal cognition, MCI, and AD, 56 supporting the observed association between falls and decreased left precentral gyrus volume in our analysis.
While new-onset falls were not associated with levels of light or moderate-vigorous activity on wrist-worn actigraphy, several limitations should be considered. Firstly, in some participants, actigraphy data was collected several years prior to neuroimaging, at which time motor dysfunction may have not originated in individuals with falls. In addition, these data capture only a discrete period, and thus, may not be representative of overall activity trends over months to years. Finally, it is possible that in some individuals (i.e., One fall group), falls do not capture motor dysfunction but rather represent an isolated event.
Limitations
The observational nature of UKB data prevents definitive understanding of the temporal relationship between falls and AD-related neuroimaging markers. In this light, it is possible that participants with recurrent falls may have experienced AD or other dementia-related cognitive changes prior to the study period, precipitating new-onset falls. However, the finding that tasks of numeric and prospective memory as well as fluid intelligence, which is associated with preclinical AD, 57 did not differ significantly between groups at the neuroimaging visit decreases the likelihood that advanced AD precipitated participant falls. Nevertheless, it is possible that the neuropsychological tests used were insufficiently sensitive to detect subtle cognitive impairments, and the lack of standardized tests such as the Mini Mental State Examination and Montreal Cognitive Assessment is a limitation of our analysis.
Several limitations relate to the self-report assessment of participant falls history. First, while participants with falls in the year preceding study enrollment (approximately 10 years prior to neuroimaging) were excluded, history of falls between the enrollment and neuroimaging timepoints were not assessed. Moreover, because falls were self-reported over a one-year period, there was potential for recall bias or inaccurate reporting by study participants. In addition, our sample may have been biased toward older adults who were healthy enough to attend study visits and undergo MRI, which may partially account for the lower prevalence of falls observed compared with other population estimates in older adults. 58 Sample size was also limited with respect to plasma biomarkers, and lack of associations between new-onset falls and plasma biomarkers of AD may reflect limited statistical power rather than the true absence of biomarker differences. The high proportion of white individuals limits the generalizability of our findings and necessitated collapsing non-white ethnicities when controlling for covariates to maximize statistical power. Finally, we limited our outcomes of interest to neuroimaging regions most associated with AD and motor dysfunction; thus, associations between new-onset falls and other neuroimaging markers of disease may not have been captured.
Conclusions and future directions
The findings of our analysis suggest that new-onset falls captured via a one-item self-report question are associated with AD-related neuroimaging markers, included decreased left and right hippocampal volumes. In addition, these findings support existing literature that among all individuals who fall, individuals with recurrent falls within a one-year period may be at most risk for poor cognitive outcomes. Finally, while the exact stage of AD diagnosis in our cohort cannot be deciphered by the current data, lack of significant differences in tasks of fluid intelligence and memory suggest that in our sample, recurrent falls may represent a marker of early AD prior to the onset of severe cognitive decline.
We suggest several potential areas for future research. Firstly, although new-onset falls were not associated with levels of physical activity measured via actigraphy in our analysis, future analyses assessing the relationship between levels of physical activity and risk of incident AD among individuals with falls would help to clarify whether structured exercise interventions may be beneficial for individuals in this high-risk cohort. Additionally, longitudinal follow-up of participants with recurrent falls over several years will help to understand their trajectories of cognitive decline and risk of AD clinical diagnoses. Finally, prospective clinical trials investigating the association between new-onset recurrent falls in later life and neuroimaging and plasma biomarkers of AD with larger sample sizes of plasma samples would strengthen the validity of our findings. Nevertheless, our findings help to encourage the implementation of routine screening for falls and other forms of motor dysfunction in older adults, as well as more frequent follow-up among participants who screen positive to identify incident cognitive decline.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261462930 - Supplemental material for Relationship between new-onset falls and neuroimaging markers of Alzheimer's disease in the UK Biobank
Supplemental material, sj-docx-1-alz-10.1177_13872877261462930 for Relationship between new-onset falls and neuroimaging markers of Alzheimer's disease in the UK Biobank by Jacob S. Shaw, Michael J.C. Bray, Haris I. Sair, Licia P. Luna, Katherine J. Hunzinger, Esther S. Oh, Paul B. Rosenberg and Matthew E. Peters in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
This research has been conducted using the UK Biobank Resource under application number 760913. We gratefully acknowledge the individuals who participated in the UK Biobank study and the investigatory teams who made this work possible.
Ethical considerations
The UKB has research ethics approval from the Northwest Multi-Centre Research Ethics Committee as a research tissue bank.
Consent to participate
All participants provided written informed consent.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PBR has received research grants from the National Institutes of Aging, Alzheimer's Clinical Trials Consortium, Richman Family Precision Medicine Center of Excellence on Alzheimer's Disease, Eisai, Functional Neuromodulation, and Lilly; honoraria from Lilly, GLG, Leerink, Medalink, Novo Nordisk, Noble Insights, TwoLabs, Otsuka, MedaCorp, ExpertConnect, HMP Global, Worldwide Clinical Trials, Medscape, and Neurology Week. PBR has received grant support from National Institute on Aging including AGR01054771, AGR01050515, AGR01046543, and AGR01071522.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study can be made available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.