
Abstract
Background
Subjective cognitive decline (SCD) is a common early complaint in mild cognitive impairment (MCI). Evidence for the 21-item SCD-Questionnaire (SCD-Q21) to discriminate MCI from normal controls (NCs) is limited.
Objective
To investigate the discrimination performance of Chinese SCD-Q21 and compare it with SCD-Q9 for community-based MCI early detection, assess the added value of simple covariates, and determine an optimal SCD-Q21 cut-off.
Methods
294 NCs and 83 people with MCI were assessed and collected demographic and clinical data. Participants completed SCD-Q21, SCD-Q9, Hamilton Anxiety Scale (HAMA) and Hamilton Depression Scale (HAMD) scale; clinical adjudication used Montreal Cognitive Assessment-Basic, Clinical Dementia Rating, and Activities of Daily Living. Group comparison, logistic regression and ROC analyses were applied. Optimal cut-offs were derived using the Youden index and AUCs were compared using DeLong tests. Within-MCI analyses contrasted screen-positive versus screen-negative subgroups.
Results
Total SCD-Q21 scores were higher in MCI, although five items [question 1 (Q1), Q2, Q3, Q11, and Q17] did not differ between groups. In multivariable binary logistic regression models, lower education (OR = 0.786), higher body mass index (BMI) (OR = 17.874), and higher SCD-Q21 total scores (OR = 1.114) were independently associated with MCI, whereas SCD-Q9 was not. Standalone AUCs were 0.662 (SCD-Q21) and 0.640 (SCD-Q9). Combing age, sex, education, BMI, and HAMA/HAMD with SCD instrument yielded AUC ∼0.91. SCD-Q21 ≥ 7 gave 69.88% sensitivity and 62.93% specificity. Screen-negative MCI cases showed lower vascular/metabolic comorbidity and lower HAMA/HAMD scores.
Conclusions
SCD-Q21 provides independent information but modest stand-alone discrimination. As part of a brief multivariable triage including education, BMI, vascular risk review, and anxiety rating, it supports efficient case-finding in community settings.
Keywords
Introduction
Alzheimer's disease (AD) is the most common neurodegenerative disorder. It is characterized by progressive memory deterioration and is frequently accompanied by aphasia, agnosia, visuospatial impairments, deficits in reasoning and problem-solving, and changes in personality and behavior.1,2 Its complex etiology and insidious gradual progression pose major challenges for both research and clinical practice. 3
Early detection is critical, particularly during mild cognitive impairment (MCI), a transitional phase between normal aging and dementia. 4 Individuals with MCI are at a significantly elevated risk of progressing to dementia compared with cognitively normal individuals. 5 Accordingly, there is a pressing need for cognitive assessment tools that are sensitive and specific, easy to administer and cost-effective, 6 especially in primary care settings where most cognitive concerns are first raised.
Self-reported questionnaires assessing subjective cognitive decline (SCD) have emerged as promising tools for identifying early cognitive change.7,8 In 2015, Gifford et al. developed the 9-item Subjective Cognitive Decline-Questionnaire (SCD-Q9) using item response theory and computerized adaptive testing to down-select from a 57-item pool. In their study, SCD-Q9 demonstrated moderate discrimination for MCI (Cohen's d = 0.49). However, in our local implementation of the translated SCD-Q9, sensitivity was 68.8%, and nearly 10% of individuals with MCI scored zero, raising concern that the abbreviated instrument may omit content necessary for accurate detection in this context. The longer 21-item version (SCD-Q21) may retain more of this essential information. We translated the SCD-Q21 into Chinese and confirmed its reliability and validity,9,10 but its ability for distinguishing MCI from cognitively normal controls has not yet been systematically evaluated.
Accordingly, we aimed to (i) assess the discriminative performance of SCD-Q21 for identifying MCI and compare it with SCD-Q9; and (ii) evaluate whether integrating additional information can further strengthen simple screening in primary care for aging populations.
Methods
Ethics statement
The study was approved by the Medical Ethics Committee of XuanWu Hospital of Capital Medical University (Beijing, China). Written informed consent was obtained from all participants or their legally authorized surrogates.
Participants
Recruitment and eligibility. From September to December 2023, community-dwelling older adults were recruited via local advertisements in residential communities in central urban Beijing. Interested residents and their informants completed structured, face-to-face interviews with trained physicians to obtain sociodemographic information (age, sex, years of education, ethnicity), social support, and medical history (hypertension, diabetes, cardiovascular disease, hyperlipidemia). Body mass index (BMI) was also calculated with the recorded height and weight by trained staff.
Inclusion criteria: age ≥ 60 years; Han ethnicity; residence in the community for ≥ 6 months.
Exclusion criteria: conditions likely to affect cognition or preclude valid assessment, including major neurological or psychiatric disorders, severe systemic illness, relevant metabolic disorders or toxic exposures, and significant sensory or language impairments. The details are provided in the Supplemental Methods.
Assessment and classification. Participant completed SCD-Q9, 11 SCD-Q21, 10 the Hamilton Depression Scale (HAMD), 12 and the Hamilton Anxiety Scale (HAMA). 13 A general neurological examination (sensory, motor, reflexes) was performed. Neuropsychological evaluation included the Montreal Cognitive Assessment-Basic (MoCA-B) with education-adjusted cut-offs 14 (illiterate or primary school, >19 points; middle school, >22 points; university, >24 points) to assess global cognition; the Clinical Dementia Rating (CDR) 15 to evaluate cognitive/functional performance, and the Activities of Daily Living (ADL) 16 scale to assess daily functioning. Final cognitive classifications were adjudicated by a panel of senior neurologists (assistant chief physicians or higher).
Two groups were defined as follows: normal controls (NC): no memory complaints, MoCA-B at or above the education-specific cut-off, CDR=0, and intact ADL (=20).
MCI: diagnosed per Petersen's criteria 17 ; memory complaints, MoCA-B below the education-specific cut-off, CDR =0.5, preserved ADL (=20), and not meeting criteria for dementia (CDR ≥ 1 score).
Statistical analysis
Analyses were conducted using SPSS v17.0 (SPSS Inc., Chicago, IL) and MedCalc v15.2.2 (MedCalc Software, Mariakerke, Belgium). Clinical characteristics and questionnaire scores were summarized as medians (continuous variables) or percentages (categorical variables). Group difference of SCD-Q9 and SCD-Q21 scores of NC versus MCI were tested using the Mann–Whitney U test (continuous) and chi-square test (categorical).
We also conducted exploratory, sex-stratified analyses by comparing SCD-Q21 item-level and total scores, and SCD-Q9 total scores between females and males using Mann-Whitney U tests (item-level p-values adjusted by Benjamini-Hochberg FDR).
To identify factors independently associated with MCI, we fitted binary logistic regression models with cognitive status (MCI versus NC) as the dependent variable and a priori predictors, including age, sex, years of education, BMI, SCD total scores (Q21 or Q9), HAMD and HAMA scores. Odds ratios (ORs) with 95% confidence intervals (CI) were reported. In a post-hoc analysis, we extended the primary logistic model with Q21 by additionally adjusting for comorbidities (hypertension, diabetes, cardiovascular disease, hyperlipidemia). Adjusted ORs were also reported. Two-sided p < 0.05 indicated statistical significance.
Receiver operating characteristic (ROC) analysis quantified discriminative performance for individual predictors and combinations. Area under the curve (AUC) was computed, and optimal cut-offs for SCD-Q9 and SCD-Q21 were determined using the Youden Index. AUCs were compared using the DeLong test. Sensitivity and specificity at the optimal cut-offs were reported.
Within the MCI group, we conducted an exploratory comparison of screen-positive versus screen-negative subgroups defined by the SCD-Q21 Youden cut-off using the Mann-Whitney U test or chi-square test, when approximate.
Results
Demographic and clinical characteristics
294 NC (MoCA-B scores: 25.7 ± 2.3) and 83 MCI (MoCA-B scores: 19.2 ± 3.3) participants were included, and MoCA-B scores were significantly lower in the MCI group than in the NC group (p < 0.001, Table 1). Compared with NC, the MCI group had fewer years of education (p < 0.001), higher BMI (p < 0.001) and higher HAMA scores (p < 0.05). There were no group differences in sex distribution, age, marital status, family history of dementia, HAMD scores, multimorbidity or social support (all p > 0.05). Sex-in sex distribution, marital status, family history of dementia, HAMD, multimorbidity or social support (all p > 0.005). Sex-stratified descriptives are provided in Supplemental Table 1.
Demographic and clinical characteristics of MCI and NC groups.
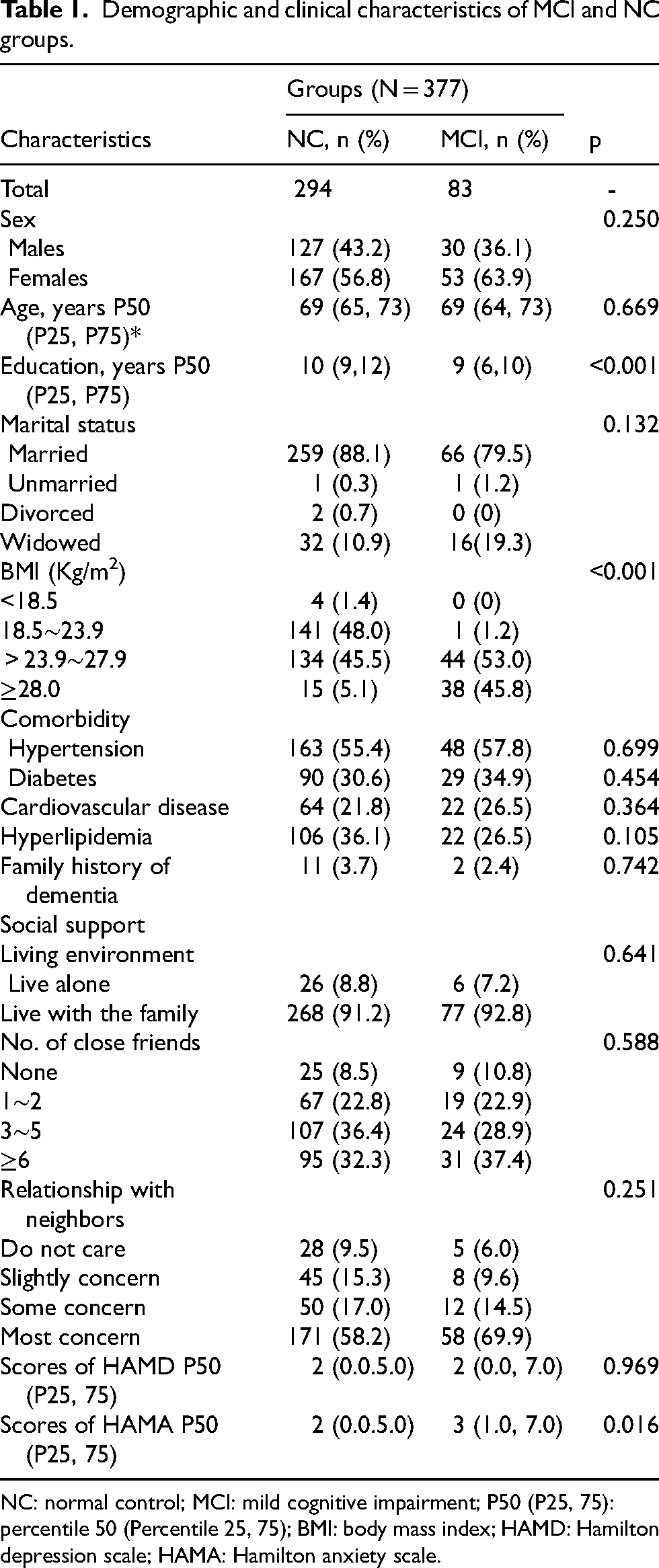
NC: normal control; MCI: mild cognitive impairment; P50 (P25, 75): percentile 50 (Percentile 25, 75); BMI: body mass index; HAMD: Hamilton depression scale; HAMA: Hamilton anxiety scale.
SCD-Q21 and SCD-Q9 scores
Total SCD-Q21 and SCD-Q9 scores were higher in MCI than NC (both p < 0.001). At the item-level, all the scores in MCI were significantly higher than NC except question 1 (Q1), Q2, Q3, Q11, and Q17 (Supplemental Tables 2 and 3).
In the sex-stratified exploratory analyses, female participants showed more pronounced SCD difference between MCI and NC than males, including higher SCD-Q21 total scores and several item-level effects (results are provided in Supplemental Tables 2 and 3).
Multivariable associations with MCI
In models including age, sex, years of education, BMI, total SCD-Q21 score, HAMD, and HAMA scores, BMI (OR = 17.874, 95% CI: 8.728–36.603, p < 0.05), education (OR = 0.786, 95% CI: 0.710–0.869, p < 0.05), and total SCD-Q21 score (OR = 1.114, 95% CI: 1.029–1.205, p < 0.05) were independently associated with MCI (Table 2). Age, sex, HAMD, and HAMA were not significant (p > 0.05).
Logistic regression model of SCD-Q21/SCD-Q9 for MCI group.
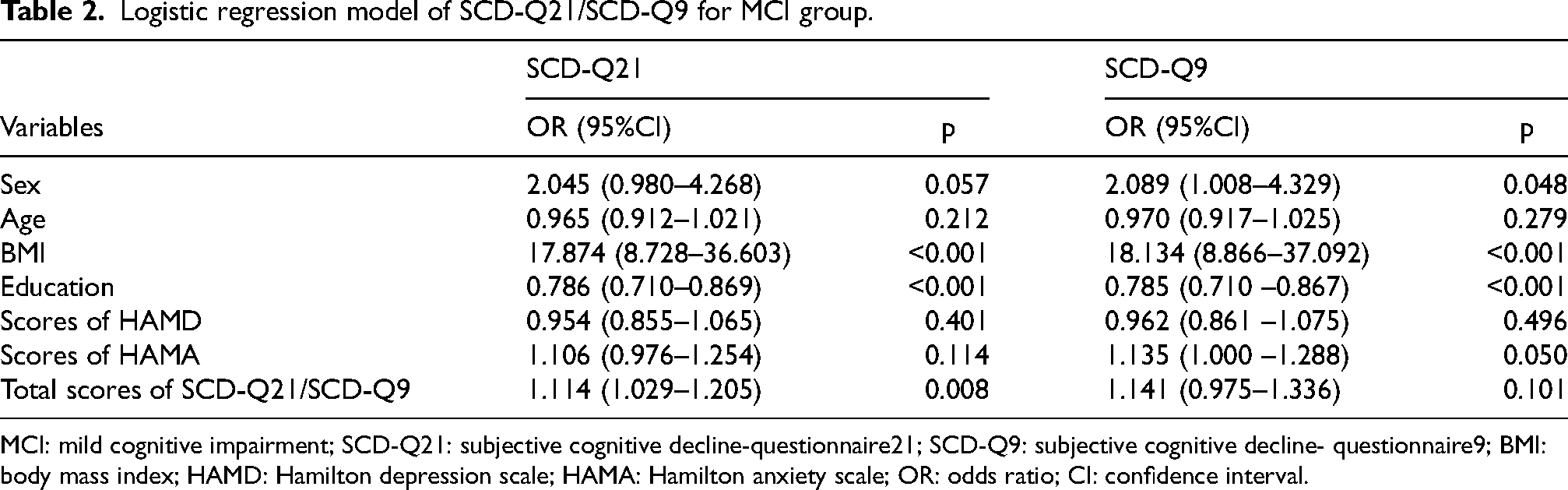
MCI: mild cognitive impairment; SCD-Q21: subjective cognitive decline-questionnaire21; SCD-Q9: subjective cognitive decline- questionnaire9; BMI: body mass index; HAMD: Hamilton depression scale; HAMA: Hamilton anxiety scale; OR: odds ratio; CI: confidence interval.
When SCD-Q21 was replaced by SCD-Q9 (also see Table 2), BMI (OR = 18.134, 95% CI: 8.866–37.092, p < 0.05) and education (OR = 0.785, 95% CI: 0.710–0.867, p < 0.05) remained significant, female was independently associated with MCI (OR = 2.089, 95%CI = 1.008–4.329, p = 0.048), whereas SCD-Q9 score was not (p = 0.101).
In the extended model that additionally included comorbidities, the BMI-MCI association remained strong (OR = 18.293, 95%CI = 8.819–37.943, p < 0.001), education remained protective, and female was independently associated with MCI (OR = 2.169, 95%CI = 1.027–4.581, p = 0.042). HAMA and HAMD were not associated, and individual comorbidities were not independently linked (Supplemental Table 4).
ROC analysis for distinguishing MCI and NC groups
The standalone discriminative performance of SCD-Q21and SCD-Q9 for differentiating MCI from NC were modest, with AUC of 0.662 (95% CI: 0.611–0.709, p < 0.0001) for the former and 0.640 (95% CI: 0.590–0.689, p = 0.0001) for the latter. There was no statistically significant difference between the two AUCs (p = 0.1155). Education (AUC = 0.684, 95% CI: 0.634–0.731, p < 0.0001) and BMI (AUC = 0.831, 95% CI: 0.790–0.868, p < 0.0001) were predictive factors of MCI versus NC. Combining age, sex, education, BMI, and scores from the HAMD and HAMA with SCD-Q21 achieved AUC =0.909 (95% CI: 0.876–0.936, p < 0.0001), and with SCD-Q9 AUC = 0.905 (95% CI: 0.871–0.933, p < 0.0001). These two combined models in distinguishing MCI and NC showed no significant difference (p = 0.1909). Figure 1 displayed the ROC curves. The optimal cut-offs were ≥7.0 for SCD-Q21 (69.88% sensitivity, 62.93% specificity) and ≥5.0 for SCD-Q9 (48.19% sensitivity, 77.55% specificity) (Supplemental Tables 5 and 6).
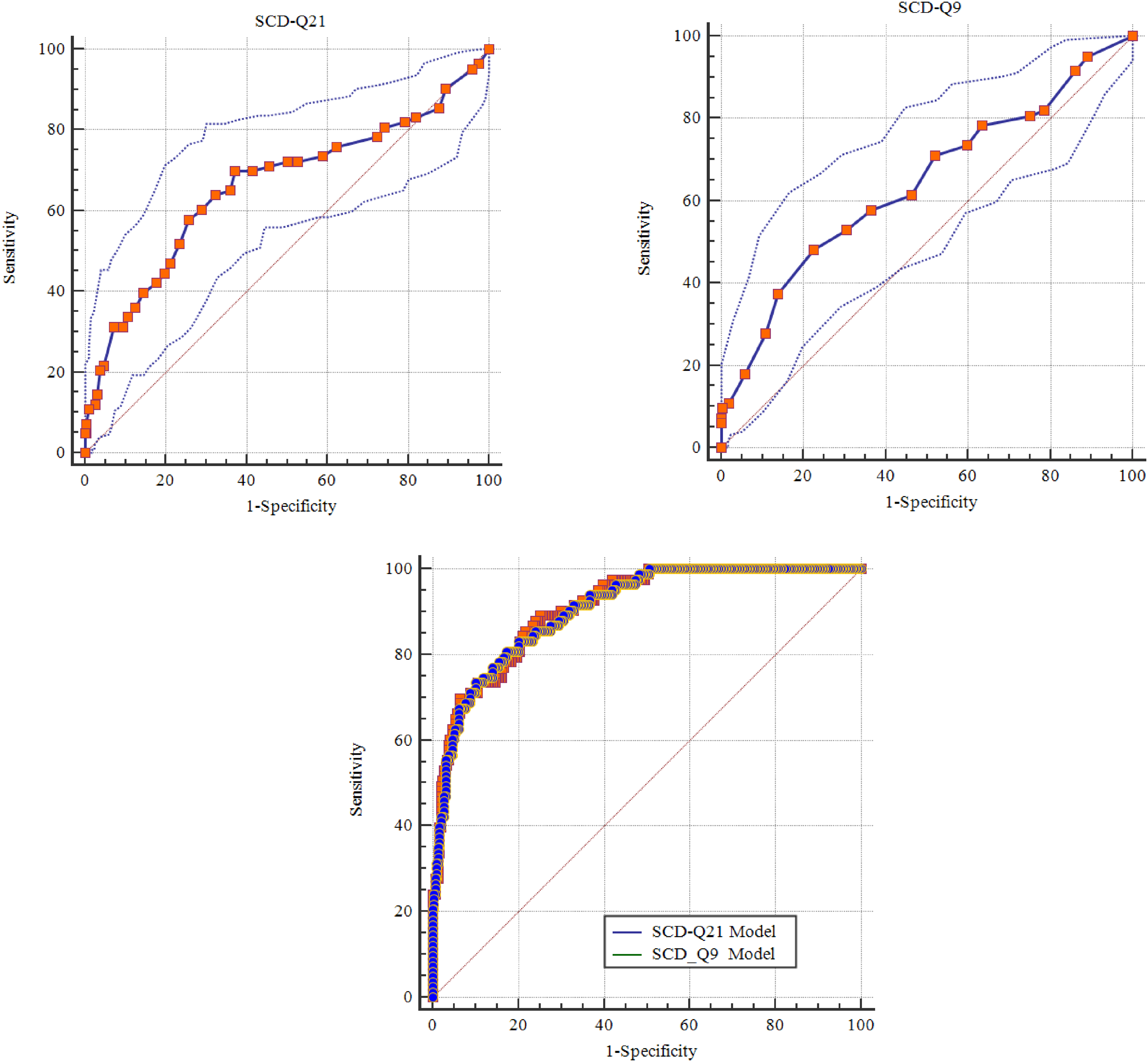
AUCs of MCI and NC groups. NC: normal control; MCI: mild cognitive impairment; AUC: area under the curve.
True-positive versus false-negative MCI cases
Applying SCD-Q21 ≥ 7 to the MCI group, true positives had higher rates of hypertension, cardiovascular disease, and hyperlipidemia, and higher HAMA/HAMD scores than false negatives (all p < 0.05), with no differences in sex, age, education, marital status, BMI, family history of dementia, diabetes, or social support (all p > 0.05; Supplemental Table 7).
Discussion
In this community-dwelling cohort of older Chinese adults, we evaluated the Chinese SCD-Q21 for identifying MCI and directly compared it with the shorter SCD-Q9. Building on prior work establishing reliability and validity of the Chinese SCD-Q21 9 and the localization and application of SCD-Q9 in Chinese settings,8,11 we found modest standalone discrimination for SCD-Q21 (AUC = 0.662). Crucially, SCD-Q21 remained independently associated with MCI after adjustment for age, sex, education, BMI and mood symptoms, whereas SCD-Q9 did not. When SCD scores were combined with simple clinical and demographic variables, classification improved markedly (AUC ≈ 0.91 for models including either SCD-Q21 or SCD-Q9).
This level of discrimination aligns with prior evidence: brief SCD instruments typically show only moderate separation from MCI when used alone. 6 The SCD-Q9 development study likewise reported a moderate case–control difference (Cohen's d ≈ 0.49). 7 Our results therefore reinforce the view that low-burden, multidomain screening outperforms any single questionnaire in community settings.
Although overall ROC performance was similar, SCD-Q21 demonstrated stronger independent associations with MCI in adjusted models compared with SCD-Q9. Item-level contrasts and prior construct-validity work indicate that SCD-Q21 samples broader domains: global memory and temporal comparison, everyday activities, self/peer comparison, and memory for important dates and numbers, beyond the content retained in SCD-Q9. 9 These observations accord with evidence that SCD questionnaires are multidimensional rather than unitary and show invariance across age groups, 18 and with findings that executive- and language-focused SCD complaints discriminate preclinical Alzheimer's disease from normal aging. 19 This wider coverage likely explains SCD-Q21's incremental signal in multivariable models even when overall AUCs appear comparable.
In the present sample, five items (Q1, Q2, Q3, Q11, and Q17) did not significantly differentiate MCI from normal controls. These questions primarily reflect global self-evaluation of memory or highly prevalent everyday lapses (e.g., general perception of memory problems or losing objects), which are common in normal aging and may therefore show limited specificity for MCI in community populations. In contrast, items that showed stronger discrimination tended to involve more concrete, functionally anchored, or socially observable difficulties, such as repetition or word-finding problems. This pattern may indicate that some SCD-Q21 items capture generalized cognitive concern rather than disease-specific decline. Future work could explore whether differential item weighting or refinement improves discrimination.
Affective symptoms intersect tightly with subjective cognition, with anxiety particularly salient early in impairment. Human studies show that anxiety and depression often co-occur in later life,20,21 yet anxiety displays stronger and bidirectional links with cognitive performance, monitoring, and progression risk in many cohorts.22–24 In our sample, HAMA scores were higher in MCI than controls, whereas HAMD scores did not differ; within MCI, individuals above the SCD-Q21 cut-off (≥7) also had higher HAMA/HAMD scores and more vascular/metabolic comorbidity than screen-negative peers. Together, these data support a model in which anxiety may amplify subjective monitoring, vigilance and help-seeking, increasing SCD signal, while low affective burden contributes to false-negative self-report. Practically, pairing SCD tools with a brief anxiety screen (for example, HAMA) and a quick vascular risk review may improve case-finding and triage in primary care.
We also confirmed two well-described epidemiological patterns. Higher educational attainment was protective against MCI, consistent with cognitive-reserve accounts and population-based evidence.25,26 In contrast, higher BMI showed an independent positive association with MCI. Although the BMI-cognition relation is debated: midlife adiposity generally increases dementia risk,27–29 whereas some later-life analyses suggest an ‘obesity paradox’.27,30 Our cross-sectional findings, together with Chinese data emphasizing lifestyle/activity as modifiers, 31 support considering adiposity in risk stratification. In adjusted models including comorbidities, BMI remained significant, whereas individual comorbidities were not (Supplemental Table 4). Post-hoc correlations were small but consistent for SCD-Q21 totals with BMI, cardiovascular disease and hyperlipidemia, but not diabetes, and there was no BMI × diabetes interaction (Supplemental Tables 8–12). In addition, within MCI, false-negative cases had lower vascular/metabolic comorbidity than true-positive cases (Supplemental Table 7). Taken together, these observations suggest that education, BMI and vascular-risk indices are useful for MCI triage, although item-level effects are small.
For clinical application, given SCD-Q21's modest stand-alone discrimination and the similar performance of combined models built with either SCD-Q21 or SCD-Q9, we do not recommend using SCD instrument as a sole screening test. Instead, SCD questionnaires should function as one component of a brief, multivariable triage that also incorporates easily collected clinical features, including years of education, BMI, and a brief mood/anxiety rating, which materially improve discrimination in our cohort. When time permits or a slightly richer clinical signal is desirable, SCD-Q21 is reasonable given its broader construct coverage and independent association with MCI after adjustment. For SCD-Q21, a working cut-off of ≥7 balanced sensitivity (∼70%) and specificity (∼63%); positive triage should prompt confirmatory neuropsychological testing and, where feasible, biomarker-informed evaluation. A negative SCD result does not exclude MCI, approximately one-third of MCI cases fell below the SCD-Q21 cut-off, so reassessment, informant report, and vascular risk review are advisable when clinical concern persists.
Limitations warrant consideration. The sample comprised Han Chinese, community-dwelling older adults and may not generalize to other cultural or clinical contexts. Cross-sectional data preclude inference about progression, and diagnoses were not biomarker-confirmed. Lifestyle behaviors (diet, physical activity, sleep) and socioeconomic circumstances (income, education quality, household composition, access to care) were not comprehensively captured and may confound associations, particularly those involving BMI and subjective complaints, in ways that vary across settings. Self-report is influenced by mood, education and insight; meta-analytic work indicates that self-awareness in MCI is variably affected and may not differ from normal cognition across all domains. 32 We also observed sex-related differences in demographics and SCD patterns. Future work should evaluate sex-specific thresholds and factor-weighted scoring, incorporate informant-report to enhance accuracy,7,33 and apply longitudinal follow-up to establish prognostic utility.
In conclusion, the SCD-Q21 is a feasible patient-reported instrument that provides independent information regarding MCI beyond demographic, anthropometric, and mood measures. While its standalone discrimination is modest, integration with simple clinical variables substantially improves classification performance, supporting its use within brief multivariable triage approaches in primary care and community settings.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261463667 - Supplemental material for An application study: 21-item Subjective Cognitive Decline Questionnaire in detecting mild cognitive impairment
Supplemental material, sj-docx-1-alz-10.1177_13872877261463667 for An application study: 21-item Subjective Cognitive Decline Questionnaire in detecting mild cognitive impairment by Lixiao Hao, Yue Xing and Ying Han in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We would like to thank the patients and families that participated in this research, without which this research would not be possible.
Ethical considerations
This study was approved by the Medical Ethics Committee of Xuanwu Hospital, Capital Medical University, Beijing, China, and conducted in accordance with the Declaration of Helsinki (1975).
Consent to participate
Written informed consent was obtained from all participants or their legally authorized representatives prior to study participation.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by the National Natural Science Foundation of China (Grant 61633018, 82020108013) and Capital Medical University Natural Science Foundation (Grant PYZ23057).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.