
Abstract
Background
Metabolic syndrome (MetS) serves as a precursor to Alzheimer's disease, a condition characterized by initial memory impairment and driven by dysregulated brain fluid dynamics. While time-restricted eating (TRE) improves memory in MetS, the mechanistic role of brain fluid dynamics in this process remains unclear.
Objective
To investigate whether a 1-month early TRE (eTRE) intervention enhances memory performance by improving brain fluid dynamics in individuals with MetS.
Methods
Twenty-eight men with MetS and 30 matched healthy male controls underwent MRI scans. Brain fluid dynamics was assessed using the diffusion tensor image analysis along the perivascular space (DTI-ALPS) index and global blood-oxygen-level-dependent-cerebrospinal fluid (gBOLD–CSF) coupling. In the MetS group, metabolic risk factors, cognitive and psychological status, and memory performance were evaluated pre- and post-eTRE. Relationships between imaging indices and memory scores were examined by correlation analysis.
Results
At baseline, men with MetS exhibited a lower DTI-ALPS index and higher gBOLD–CSF coupling than healthy controls (p < 0.05). After 1-month eTRE, the DTI-ALPS index increased (p < 0.001), while gBOLD–CSF coupling decreased (p = 0.027), approaching healthy control levels. Metabolic parameters and long-term memory performance also improved significantly (all p < 0.05). Changes in DTI-ALPS were positively correlated with delayed recall (r = 0.445, p < 0.05), whereas changes in gBOLD-CSF coupling were negatively correlated (r = -0.550, p < 0.05).
Conclusions
A 1-month eTRE intervention improved long-term memory and brain fluid dynamics in males with MetS, providing a promising non-pharmacological strategy to counteract metabolic-driven neurodegenerative diseases.
Trial registration
National Medical Research Registration and Filing Information System (https://www.medicalresearch.org.cn/), MR-61-24-042065.
Keywords
Introduction
Brain fluid dynamics, involving the continuous exchange between cerebrospinal fluid (CSF) and interstitial fluid (ISF), are critical for maintaining the central nervous system microenvironment. 1 This process is largely mediated by the glymphatic system, a structured pathway for metabolic waste clearance through aquaporin-4 (AQP4) channels in astrocytic endfeet. Through this pathway, CSF enters the brain parenchyma via periarterial routes, mixes with ISF, and then exits along perivenous spaces to eliminate neurotoxic metabolites.2,3 The system is primarily driven by arterial pulsations, becomes most active during sleep, and plays a central role in sustaining cerebral homeostasis.4,5 Sleep not only facilitates glymphatic transport but also supports memory consolidation, implying a functional association between these two processes. 6 In Alzheimer's disease (AD), impaired glymphatic clearance reduces the elimination of amyloid-β and tau, leading to their accumulation in memory-related structures such as the hippocampus and contributing to cognitive decline. 7 Even during normal aging, reduced glymphatic activity has been linked to hippocampal atrophy and memory deterioration, 8 underscoring the importance of maintaining glymphatic function for memory protection.
Metabolic syndrome (MetS) comprises several interrelated metabolic abnormalities, including central obesity, hypertension, insulin resistance, dyslipidemia, and hyperglycemia, that jointly elevate the risk of cardiovascular and metabolic disorders9–11. Growing evidence suggests that these metabolic disturbances may also compromise brain health. Emerging evidence suggests that the multifactorial pathology of MetS may collectively impair brain fluid dynamics, thereby increasing the risk of cognitive decline. Vascular stiffening and impaired endothelial function may dampen arterial pulsatility and weaken blood–brain barrier integrity 3 ; lipid dysregulation associated with obesity may alter glymphatic vessel contractility 12 ; and chronic hyperglycemia can induce microvascular inflammation and disrupt AQP4 polarization in astrocytic endfeet. 13 Collectively, these abnormalities are likely to hinder CSF–ISF exchange and the removal of metabolic waste. Such metabolic-driven impairment of brain clearance pathways identifies MetS as a major modifiable risk factor for AD.14,15 Epidemiological evidence further supports the link between MetS and cognitive impairment, with meta-analyses showing an approximately 30–40% higher risk compared with metabolically healthy individuals.16,17 Several population-based studies have reported poorer memory performance among individuals with MetS, 18 and one MRI-based cohort further suggested that this association may be more pronounced in men. 19 These findings highlight the importance of investigating the mechanisms linking MetS, brain fluid dynamics, and memory impairment.
An increasing number of studies suggest that cognitive deficits in MetS may result from inefficient removal of neurotoxic metabolites. 20 Among various lifestyle strategies, dietary interventions such as the Mediterranean, low-carbohydrate, and time-restricted eating (TRE) approaches have received increasing attention for improving metabolic health. 21 TRE, which aligns food intake with circadian rhythms without strict caloric restriction, has been shown to enhance insulin sensitivity, glycemic control, and inflammatory status.22,23 These metabolic improvements may, in turn, be relevant to brain fluid dynamics. Compared with traditional dietary interventions, TRE requires only modifications in meal timing rather than strict restrictions on food type or calorie intake, which contributes to its higher adherence. 24 Importantly, dietary patterns have been proposed as modifiable factors that may influence glymphatic activity indirectly through improvements in metabolic status. 25 Animal research further suggests that time-restricted feeding can counteract high-fat-diet-induced memory impairment, reduce amyloid-β deposition, and suppress neuroinflammation. 26 Despite preliminary evidence from animal experiments and small-scale clinical studies indicating that TRE might improve memory and influence brain fluid dynamics, the specific impact of early (eTRE) on brain fluid dynamics in males with MetS remains to be elucidated.
Advances in MRI techniques have led to the development of diffusion tensor image analysis along the perivascular space (DTI-ALPS) 27and global cortical gray matter blood-oxygen-level-dependent (gBOLD)–CSF coupling as novel, 28 noninvasive proxies for assessing brain fluid dynamics. The DTI-ALPS index indirectly assesses perivascular fluid dynamics by quantifying water diffusivity along perivascular pathways, 29 thereby providing a surrogate measure related to the structural integrity of CSF–ISF exchange routes. However, it is confined to white matter regions near the lateral ventricles and does not directly capture CSF flow. 30 To complement this, we also incorporated gBOLD-CSF coupling, which reflects the relationship between neurovascular activity and CSF dynamics and is considered a functional indicator of waste clearance capacity. 31 Given the metabolic and vascular abnormalities in MetS, the combined use of these indices enables a multidimensional characterization of cerebral fluid movement in this population.
In this study, we hypothesized that a 1-month eTRE intervention would improve brain fluid dynamics and enhance long-term memory performance in males with MetS, with concomitant improvement in peripheral metabolism. Furthermore, we expected that changes in long-term memory performance would be closely associated with changes in these imaging markers of brain fluid dynamics.
Methods
Participants
This study enrolled 28 males with MetS (aged 26–51 years) and 30 healthy male controls (aged 24–52 years), recruited from the Endocrinology Outpatient Department of Xi’an Daxing Hospital, hospital announcements, and online advertisements. Written informed consent was obtained from all participants before enrollment. The study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of Xi’an Daxing Hospital (Approval Number: KY2024-025). Inclusion and exclusion criteria 23 were as follows:
Inclusion criteria. (1) Diagnosed with metabolic syndrome (i.e., more than 3 abnormal findings out of 5): a. Waist circumference ≥90 cm (men). b. Elevated triglycerides (TG) (use of medications for elevated TG is an alternate indicator) ≥ 150 mg/dL (1.7 mmol/L). c. Reduced high-density lipoprotein cholesterol (HDL-c) (use of medications for reduced HDL-c is an alternate indicator) < 40 mg/dL (1.0 mmol/L) in males < 50 mg/dL (1.3 mmol/L) in females. d. Elevated blood pressure (use of hypoglycemic medications is an alternate indicator). systolic blood pressure (SBP) ≥ 130 and/or diastolic blood pressure (DBP) ≥ 85 mmHg. e. Elevated fasting blood glucose (FBG) (used of hypoglycemic medications is an alternate indicator) ≥ 100 mg/dL (5.6 mmol/L). (2) Age from 25 to 55 years. (3) Stable weight (change ≤10% current body weight) for 3 months prior to the study. (4) If participants were on hypoglycemic medications, hypotensive medications, lipid-lowering medications or cardiovascular medications, dose adjustment was not permitted during the 3-month intervention.
Exclusion criteria. 1) Night shift workers. 2)MRI examination contraindications. 3) History of major diseases or related diseases, such as inflammatory disease, rheumatologic disease, adrenal disease, malignancy, type 1 diabetes, cirrhosis, chronic kidney disease, acquired immunodeficiency syndrome, eating disorder, uncontrolled psychiatric disorder and major adverse cardiovascular event. 4) Current participating in other weight-management program, current on a prescribed diet for special disease or current on any drugs that affect appetite. 5) History of weight-loss surgery. 6)Experienced 2 or more hypoglycemic events in the six months prior to screening, defined as blood glucose <2.8 mmol/L, or blood glucose not reaching <2.8 mmol/L but with evident hypoglycemic symptoms.
Study design
This study adopted a 1-month within-subject pre–post design to investigate the effects of eTRE in males with MetS. All participants were instructed to strictly restrict their daily eating window to 8 h (08:00–16:00). During the 8-h feeding window, participants were permitted to eat ad libitum without calorie counting or strict dietary restrictions, following protocols described by He et al. 23 and Zheng et al. 32 During the remaining 16-h fasting period, participants were allowed and encouraged to drink water freely to maintain normal physiological function. Adherence to the prescribed eating schedule was verified objectively using glucose pattern analysis based on continuous glucose monitoring (CGM; WeiTai Health Medical Technology Co., Ltd, Shanghai, China) and further supported by real-time activity and sleep tracking via a wearable smart band. Comprehensive data quality control and adherence verification procedures were implemented throughout the study. Detailed descriptions of the CGM configuration, spike detection algorithm, calibration procedures, and adherence feedback mechanisms are provided in the Supplemental Methods. All outcome measures, including cognitive assessments, laboratory biochemical indices, and neuroimaging data, were collected at baseline and after 1-month of intervention.
Clinical indicators assessments
At baseline, demographic and clinical characteristics were obtained, including sex, age, weight, height, education, and smoking and drinking history. Body weight and height were measured using the InBody 770 body composition analyzer (InBody, Seoul, Korea), which has a precision of ± 0.1 kg for weight and ± 0.5 cm for its integrated stadiometer. Participants were measured barefoot and in light clothing. Body mass index (BMI) was calculated as weight (kg)/height2 (m2), and assessed at baseline and after one month.
In the MetS group, all blood samples were drawn at the Clinical Laboratory of Xi’an Daxing Hospital between 07:40 and 09:00 h after an overnight fast (from 20:00 h) at baseline and 1 month later. Laboratory analyses included alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), γ-glutamyl transferase (GGT), leucine aminopeptidase (LAP), total bilirubin (TBIL), direct bilirubin (DBIL), indirect bilirubin (IBIL), total protein (TP), albumin (ALB), globulin (GLB), albumin/globulin ratio (A/G), total bile acid (TBA), AST/ALT ratio, urea (UREA), creatinine (CREA), uric acid (UA), carbon dioxide (CO2), TG, total cholesterol (TC), HDL-c, low-density lipoprotein cholesterol (LDL-c), amylase (AMY), FBG, and fasting insulin (FINS). Homeostatic model assessment of insulin resistance (HOMA-IR) and quantitative insulin sensitivity check index (QUICKI) were further calculated from FBG and FINS. Additionally, the following indices were calculated:


For the healthy control group, data on body weight, BMI, TG, TC, HDL-c, and LDL-c were obtained from physical examination reports within the recent 2–3 months, while FBG was measured by fingertip blood glucose testing.
Memory was assessed using the Rey Auditory Verbal Learning Test (RAVLT). The protocol consisted of five immediate learning trials (Trials 1–5; total range 0–75 words), where List A (15 nouns) was read aloud at a rate of one word per second, followed by an interference trial (List B; range 0–15 words) and its immediate recall. After a 20-min interval filled with non-verbal distractor tasks (completing other assessment questionnaires), a long-delay recall trial (range 0–15 words) was performed to evaluate long-term memory retention. 33 To minimize practice effects in this longitudinal design, Form 1 (Rey, 1964) was used at baseline and Form 3 (Shapiro & Harrison, 1990) at follow-up, following the recommendations of Hawkins et al. 34 The RAVLT has been extensively validated, demonstrates high test–retest reliability, and shows minimal practice effects, making it a sensitive and reliable tool for detecting subtle memory changes. 35
To ensure the comprehensiveness and reliability of the study, and to provide a multi-dimensional assessment of the participants’ cognitive and psychological status, we also administered a battery of supplementary tests. Global cognitive function was assessed using the Montreal Cognitive Assessment (MoCA). To evaluate processing speed and executive function, the Symbol Digit Modalities Test (SDMT) and the Trail Making Test (TMT, Parts A and B) were employed. Additionally, sleep quality was monitored using the Pittsburgh Sleep Quality Index (PSQI).
Image acquisition
MRI data were acquired using a 3.0 T MRI system (SIEMENS MAGNETOM Prisma) with a 32-channel head coil. High-resolution T1-weighted anatomical images were obtained using a 3D MPRAGE sequence with the following parameters: scan time = 3 min 9 s, number of slices = 176, voxel size = 1.0 mm × 1.0 mm × 1.0 mm, repetition time (TR) = 1540 ms, echo time (TE) = 2.99 ms, flip angle (FA) = 9°, field of view (FOV) = 224 mm × 224 mm, and image resolution = 224 × 224. Resting-state functional MRI data were acquired using a standard echo-planar imaging (EPI) sequence without parallel imaging acceleration. The acquisition parameters were as follows: scan time = 10 min 10 s, number of slices = 72, voxel size = 2.0 mm × 2.0 mm × 2.0 mm, TR = 1000 ms, TE = 38 ms, FA = 52°, FOV = 208 mm × 208 mm, and image resolution = 104 × 104.
The DTI sequence with the following parameters was used for all scans: scan time = 10 min 42 s, number of slices = 64, voxel size = 2.0 mm × 2.0 mm × 2.0 mm, TR = 3800 ms, TE = 92 ms, FA = 52°, FOV = 220 mm × 220 mm, and image resolution = 110 × 110. b = 0 and 1000 s/mm2 with 30 directions.
DTI-ALPS index processing and calculation
The DTI data were processed with DSI studio software (version “Chen” build June 3, 2024, http://dsi-studio.labsolver.org). The main procedures included: The main preprocessing steps included correction for eddy current–induced distortions and head motion artifacts, followed by brain mask generation and tensor reconstruction using the standard DTI model. Regions of interest (ROIs) were manually placed in areas corresponding to projection fibers and association fibers adjacent to the left and right lateral ventricles, respectively. For each ROI, axial diffusivities along the x-, y-, and z-axes were extracted.27,36 The DTI calculations were performed using the following formula.

Where
fMRI preprocessing and gBOLD-CSF signal extraction
Resting-state fMRI data were preprocessed using the Data Processing Assistant for Resting-State fMRI (DPARSF, version 5.4, http://www.restfmri.net/forum/DPARSF), which is implemented on the SPM12 platform (SPM12, https://www.fil.ion.ucl.ac.uk/spm) The pipeline involved: (1) discarding the first 10 time points to allow for signal stabilization; (2) slice-timing correction and realignment to minimize timing and motion artifacts; (3) detrending to remove linear drifts, followed by spatial smoothing with a 4-mm full-width at half-maximum (FWHM) Gaussian kernel; and (4) temporal band-pass filtering (0.01–0.1 Hz) to isolate resting-state frequency components. The resulting preprocessed data were then used for gBOLD and CSF signal extraction.28,37
gBOLD signal was calculated as the mean time series within a gray matter mask derived from the Harvard–Oxford cortical and subcortical atlas, 38 with the cerebellum excluded. For CSF signal, ROIs were manually delineated on the bottom axial slices of the motion-corrected functional images, 39 guided by the corresponding high-intensity ventricular regions on the co-registered T1-weighted images, and the extracted signals were averaged within CSF ROIs. Finally, both CSF and gray matter signals were z-scored before coupling analyses.
Quantification of gBOLD-CSF coupling strength
The temporal interaction between global gray matter BOLD fluctuations and CSF signals was quantified via time-lagged cross-correlation within a ± 10 s window. In addition, the cross-correlation between the temporal derivative of the BOLD signal (dBOLD/dt) and CSF dynamics was computed, following hydrodynamic modeling frameworks.30,31
Statistical significance was determined through 10,000-permutation testing, in which gBOLD and CSF signals were randomly shuffled across subjects to generate a null distribution. The empirical p-value was defined as the proportion of permuted statistics exceeding the observed correlation. All computations were performed in MATLAB R2023b, utilizing parallel processing to accelerate computation.
Statistical analysis
The normality of continuous variables was assessed with the Shapiro–Wilk test. Depending on the distribution characteristics, paired t-tests (for normally distributed data) or paired Wilcoxon signed-rank tests (for non-normally distributed data) were applied to compare metabolic risk factors in MetS males before and after the intervention. The choice of statistical test was based on the assumptions of normality and homogeneity of variance. Independent samples t-tests (for normally distributed data) or Mann-Whitney U tests (for non-normally distributed data) were used to compare baseline characteristics and brain fluid dynamics indices (DTI-ALPS index and gBOLD–CSF coupling) between MetS patients and healthy controls. Paired t-tests were used to evaluate post- to pre-intervention changes in metabolic risk factors, brain fluid dynamics indices, neuropsychological performance (RAVLT, MoCA, SDMT, and TMT), and sleep quality (PSQI). Associations between intervention-induced changes in glymphatic indices and RAVLT performance were examined using Pearson correlation analyses. Statistical significance was set at two-tailed p < 0.05. All statistical analyses were performed using SPSS 26.0 (IBM Corp., Armonk, NY, USA)
Results
Demographic and clinical measurements
Table 1 presents the demographic characteristics of the participants, and effects of 1-month eTRE intervention in men with MetS. A total of 28 male patients with MetS and 30 male healthy controls were enrolled. The two groups did not differ significantly in age, years of education, or smoking status (all p > 0.05), and no heavy alcohol consumption was reported. As laboratory data for the control and MetS groups were obtained from different sources, only descriptive statistics were used for between-group comparisons. At the descriptive level, the MetS group showed higher baseline levels of TG, TC, LDL-C, and FBG, and lower HDL-C compared with healthy controls, while no significant differences were observed in baseline cognitive performance. Following the intervention, participants showed significant improvements in memory performance, including immediate recall (p < 0.001) and delayed recall (p = 0.005). Weight and BMI had decreased significantly (all p < 0.001). Regarding metabolic risk factors, significant reductions were observed in ALT, GGT, GLB, FBG, FINS, HOMA-IR, and TG, whereas QUICKI, TBIL, DBIL, CREA and AMY significantly increased (all p < 0.05). Despite a slight increase in the median ALT level, the overall paired data indicated a decreasing trend, as assessed using non-parametric analysis. No significant changes were observed in MoCA, SDMT, or TMT scores following the intervention (all p > 0.05).
Demographic and clinical characteristics of participants, and effects of 1-month eTRE intervention in men with MetS.
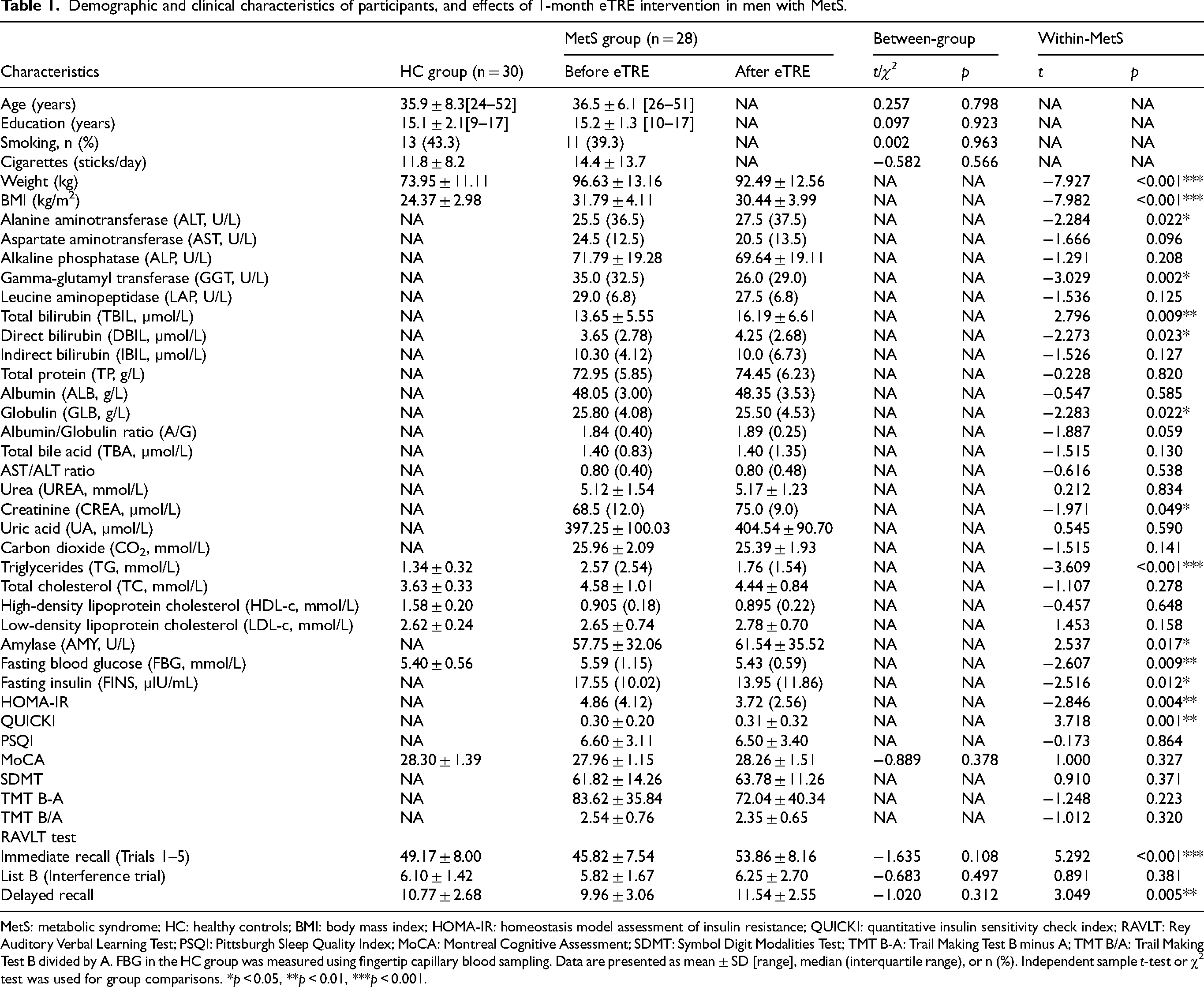
MetS: metabolic syndrome; HC: healthy controls; BMI: body mass index; HOMA-IR: homeostasis model assessment of insulin resistance; QUICKI: quantitative insulin sensitivity check index; RAVLT: Rey Auditory Verbal Learning Test; PSQI: Pittsburgh Sleep Quality Index; MoCA: Montreal Cognitive Assessment; SDMT: Symbol Digit Modalities Test; TMT B-A: Trail Making Test B minus A; TMT B/A: Trail Making Test B divided by A. FBG in the HC group was measured using fingertip capillary blood sampling. Data are presented as mean ± SD [range], median (interquartile range), or n (%). Independent sample t-test or χ2 test was used for group comparisons. *p < 0.05, **p < 0.01, ***p < 0.001.
Alterations in gBOLD–CSF coupling and DTI-ALPS index
Prior to the 1-month eTRE intervention, MetS patients exhibited a trend toward stronger gBOLD-CSF negative coupling compared to healthy controls, though this difference did not reach statistical significance (t = 1.867, p = 0.067). After a 1-month eTRE intervention, we observed a significant reduction in the gBOLD–CSF negative coupling (t = -2.341, p = 0.027) (Figure 1A). Specifically, the average cross-correlation between gBOLD and CSF signals exhibited a significant positive peak at a lag of −5 s (B = 0.242, p < 0.001, permutation test, n = 10,000), followed by a significant negative peak at a lag of +5 s (B = −0.227, p < 0.001, permutation test, n = 10,000) (Figure 1B). The negative peak at +5 s was selected as the primary index of coupling strength, and its absolute value was used for group-level statistical comparisons and visualization. Additionally, analysis of the first-order gBOLD derivative showed a pronounced positive peak at a lag of −1 s (Figure 1C).
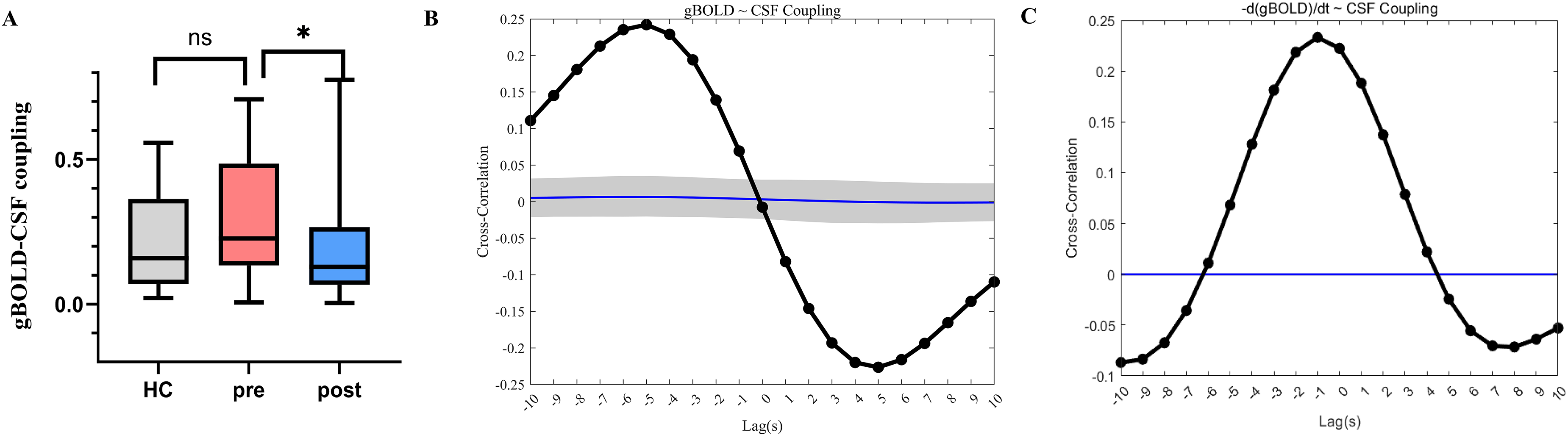
Coupling between gBOLD and CSF dynamics in men with MetS. (A) Box plot showing gBOLD–CSF coupling index across healthy controls (HC), MetS patients at baseline (pre), and MetS patients after 1-month eTRE intervention (post). (B) Group-averaged cross-correlation function between gBOLD and CSF signals across 28 MetS participants. (C) Cross-correlation function between the first-order derivative of the gBOLD signal and CSF fluctuations in patients with MetS. Thick line, mean curve of the participant group; thin line, mean curve of the null distribution from permutation tests. Shaded areas indicate 95% confidence intervals calculated from shuffled signals. gBOLD, global blood -oxygen -level–dependent; CSF, cerebrospinal fluid; MetS, metabolic syndrome. ns, not significant, *p < 0.05.
In addition, prior to intervention, MetS patients showed significantly lower bilateral ALPS indices than healthy controls (both p < 0.001). Following 1-month eTRE, A significant increase was found in the left side ALPS index (p<0.001, t = 3.809) (Figure 2A), whereas no significant change was observed on the right side (p = 0.085, t = 1.791) (Figure 2B).
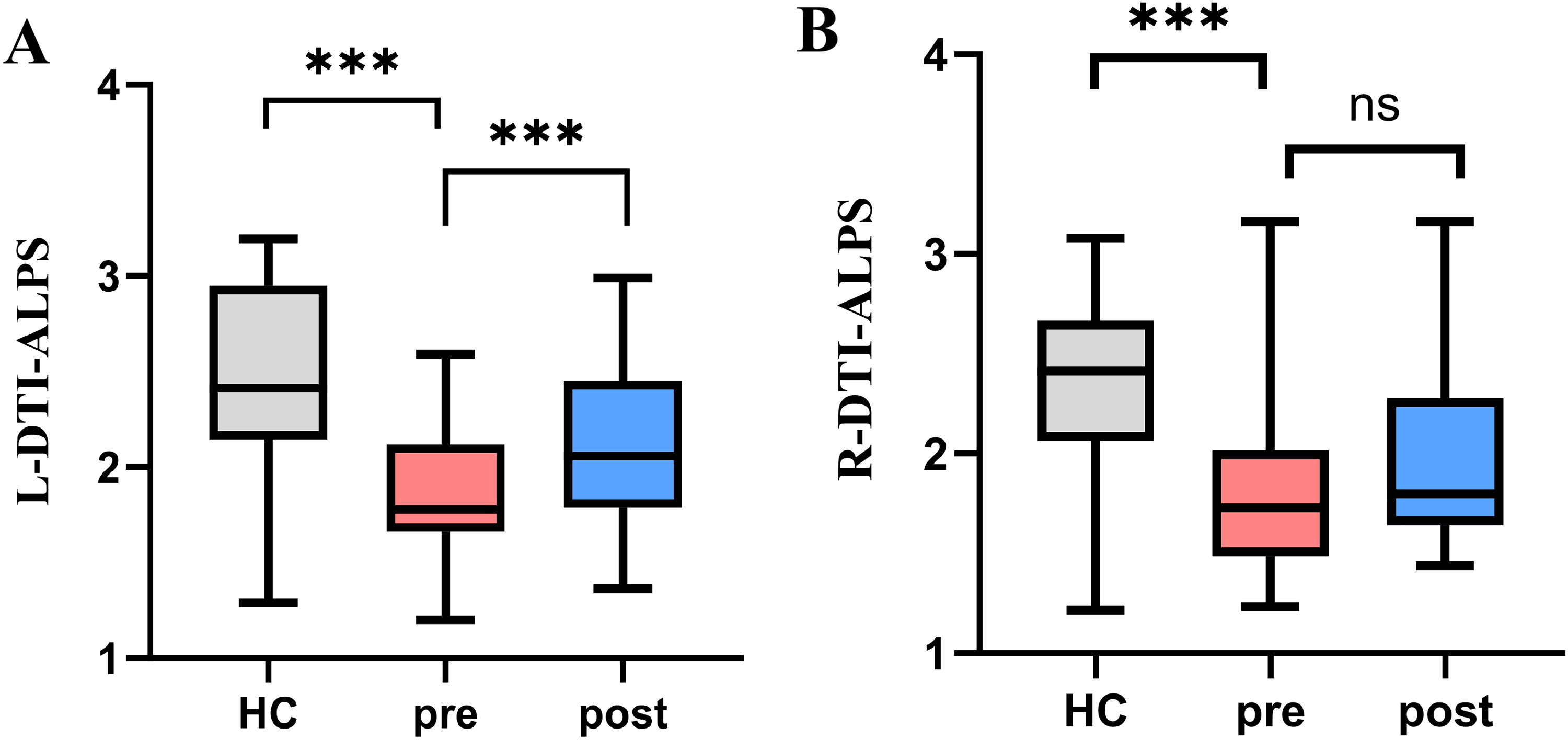
Box plot of left and right ALPS indices. (A) Changes in the left ALPS index. (B) Changes in the right ALPS index. HC, healthy controls; pre, MetS patients at baseline; post, MetS patients after 1-month eTRE intervention. L-DTI-ALPS, diffusion-tensor imaging analysis along perivascular space on the left side; R-DTI-ALPS, diffusion-tensor imaging analysis along perivascular space on the right side; MetS, metabolic syndrome; ns, not significant; ***p < 0.001.
Correlation between fluid dynamics and long-term memory performance
After 1-month of eTRE intervention, changes in gBOLD–CSF coupling were negatively correlated with improvements in Delayed RAVLT performance (r = –0.550, p = 0.002). Moreover, changes in the DTI-ALPS index were significantly and positively correlated with improvements in delayed recall scores (r = 0.445, p = 0.018) (Figure 3).
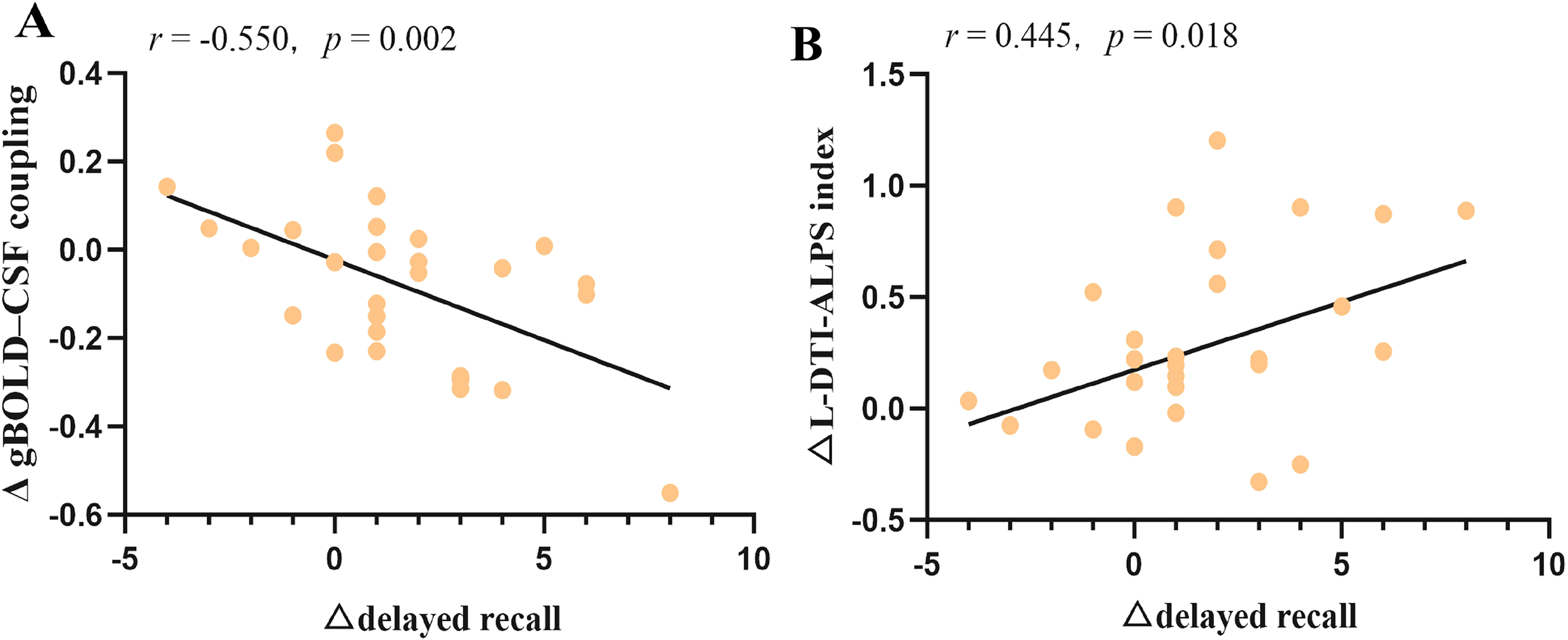
Correlation analysis of DTI-ALPS index with gBOLD–CSF coupling strength in men with MetS after a 1-month eTRE intervention.
Discussion
This study found that after a 1-month eTRE intervention, male participants with MetS exhibited improved brain fluid dynamics (increased DTI-ALPS index and decreased gBOLD–CSF coupling) and significantly enhanced long-term memory performance, with concomitant improvement in peripheral metabolism. Changes in brain fluid dynamics indices were significantly correlated with changes in long-term memory performance. These findings suggest that eTRE, as a lifestyle intervention, may offer potential clinical value for metabolic-driven neurodegenerative diseases.
A significant increase in the left-sided ALPS index was observed, approaching levels observed in healthy controls, whereas no significant change occurred on the right. This lateralized difference might reflect vascular asymmetry or inter-individual variation in perivascular architecture. 40 Although the ALPS index was initially proposed as a marker of perivascular diffusivity, 41 emerging evidence suggests that it is also shaped by white matter microstructural properties, such as fiber crossings, axonal undulations, and dispersion patterns. 42 Recent comparative studies indicate that ALPS changes may not directly reflect CSF-ISF exchange per se, but rather altered tissue water mobility or white matter integrity. 43 Thus, the observed increase indicates region-specific improvements in white matter microstructure following the 1-month eTRE intervention, potentially facilitating perivascular fluid dynamics. Ketone bodies generated during TRE may serve as an alternative fuel source for white matter, supporting energy metabolism, attenuating axonal injury, and restoring microstructural integrity. 44 Experimental work indicates that intermittent fasting drives astrocyte-specific remodeling and region-specific alterations in astrocytic structure, 45 processes that may influence the cellular architecture surrounding perivascular spaces. AQP4 localization and astrocytic integrity were critical for maintaining interstitial fluid homeostasis and perivascular exchange.46,47 Moreover, TRE ameliorates arterial compliance and diminishes rigidity, 2 and these metabolic and vascular improvements may collectively promote neurovascular coupling and brain fluid dynamics, providing a multifactorial mechanistic basis for the elevated ALPS index.
Following the intervention, the gBOLD–CSF coupling was significantly reduced. This temporal profile differed from most previous analyses, 48 which may partly relate to the shorter TR used in our study (1 s). This finding may appear paradoxical, as reduced gBOLD–CSF coupling has generally been associated with pathological burden or cognitive impairment in neurodegenerative and other disease states.31,49,50 However, the biological significance of this metric may be context-dependent rather than strictly linear. For instance, recent longitudinal evidence has demonstrated that increased coupling values, reflecting weakened synchronization, are associated with greater amyloid-β burden and cognitive decline. 51 In addition, coupling alterations under physiological stress, such as sleep deprivation, may reflect compensatory rather than purely pathological processes. 48 Therefore, the reduction observed in our study does not necessarily indicate functional worsening, but may instead reflect normalization of an altered baseline state, particularly given its concurrence with increased DTI-ALPS index and improved long-term memory. This pattern suggests that the physiological significance of altered coupling differs across disease stages, and that, during the early or preclinical stage of metabolic dysfunction, it may reflect a compensatory physiological state. Potential contributors include metabolic regulation, 52 circadian and sleep-related mechanisms,53,54 and neurovascular processes.55,56 Nevertheless, these interpretations remain preliminary, and further mechanistic and longitudinal studies are warranted to clarify the physiological basis and long-term significance of these coupling changes.
These changes in brain fluid dynamics are likely to have functional consequences for memory processing. Participants exhibited modest improvements in both immediate and delayed recall, whereas other cognitive domains, including global cognition (MoCA), processing speed (SDMT), and executive function (TMT), remained unchanged. This pattern may reflect a ceiling effect, given the largely normal baseline cognitive performance. The selective improvement in memory may be related to the particular vulnerability of hippocampal–hypothalamic circuits to metabolic disturbances. The hypothalamus is highly responsive to peripheral metabolic signals, 57 while the hippocampus is particularly sensitive to insulin resistance and metabolic dysregulation, 58 both of which are closely linked to memory function. Importantly, such metabolically sensitive circuits may also retain a greater capacity for functional recovery following metabolic interventions. 59 Beyond regional vulnerability, evidence suggests that TRE can directly modulate hippocampal function and cognitive performance, potentially through improvements in metabolic efficiency, circadian regulation, and synaptic plasticity.26,60,61 Taken together, these findings suggest that a one-month eTRE intervention may improve memory performance in males with MetS. However, the clinical significance of these changes should be interpreted with caution. Given that midlife MetS is a strong predictor of late-life cognitive decline,62,63 even modest improvements during this stage may have potential prognostic relevance. Further longitudinal studies are warranted to determine their long-term effects.
Furthermore, delayed recall performance was positively correlated with the ALPS index but negatively correlated with gBOLD—CSF coupling, indicating a close link between brain fluid dynamics and hippocampal-dependent memory. Previous studies have shown that the ALPS index is associated with early Aβ uptake in the hippocampus and parahippocampal gyrus 64 and is positively correlated with hippocampal volume, 65 indicating that higher ALPS values reflect hippocampal structural and functional integrity. In contrast, increased gBOLD–CSF coupling in AD has been linked to memory impairment and greater accumulation of Aβ and tau pathology. 31 As large-scale gBOLD fluctuations are related to the default mode network, which is closely connected to the hippocampus,66,67 the reduced gBOLD–CSF coupling observed here may reflect normalization of brain fluid dynamics and improved hippocampal metabolic homeostasis, consistent with the observed enhancement in long-term memory. These associations may be partly mediated by metabolic improvements induced by eTRE, as insulin resistance and dyslipidemia impair neurovascular coupling and glymphatic clearance, whereas improved insulin sensitivity may optimize cerebral blood flow–fluid coordination.68,69
Consistent with previous studies,70,71 the 1-month eTRE significantly improved body weight, insulin resistance, lipid profile and liver function. In addition, our study further demonstrated significant increases in serum TBIL, IBIL, and CREA levels after the intervention. Although previous eTRE studies rarely examined these parameters, both animal experiments involving 48-h fasting 72 and human studies with 24-h fasting 73 reported increased bilirubin levels following prolonged fasting, consistent with our findings. These changes may reflect transient metabolic adaptations to short-term energy restriction and could be related to potential nephroprotective effects. 74 Moreover, low serum AMY has been associated with increased MetS risk, suggesting a link between exocrine and endocrine pancreatic function. 75 thus, the observed increase in AMY may indicate a modulatory effect of eTRE on pancreatic function. The mechanisms underlying the increase in GLB remain unclear and warrant further investigation. Notably, HDL-C decreased while LDL-C increased following the intervention. Such findings may reflect transient or variable lipid responses to short-term TRE, influenced by dietary composition and intervention duration.22,76
Several limitations should be acknowledged. First, although rigorous quality control procedures were implemented, the relatively small sample size and inclusion of only male participants may restrict the interpretability and generalizability of the findings. In addition, the control and MetS data were obtained from different sources, which may introduce site-related variability and limit direct comparability. Future research involving larger and more heterogeneous cohorts is needed to confirm and extend these observations. Second, the DTI-ALPS index and gBOLD-CSF coupling are indirect proxies for brain fluid dynamics and do not capture the full complexity of cerebral fluid movement; therefore, their interpretation should be approached with caution. Third, the use of a single neuropsychological battery may not capture the full spectrum of memory domains affected by metabolic shifts. Fourth, while eTRE yielded brain-related improvements, the potential confounding effect of concomitant caloric restriction cannot be entirely ruled out. Future research should strictly monitor energy intake to isolate time-dependent effects. Finally, the short follow-up period limits our ability to draw conclusions regarding the long-term durability and clinical significance of the observed cognitive changes. Longer-term longitudinal studies are needed to determine whether these changes persist over time and translate into clinically meaningful cognitive benefits in individuals with MetS.
In summary, this study provides preliminary evidence that a 1-month eTRE intervention enhances long-term memory in males with MetS, changes associated with improved brain fluid dynamics. These findings highlight a potential mechanistic link between metabolic status, brain fluid dynamics, and long-term memory function. Given its simplicity and effectiveness, eTRE represents a promising lifestyle strategy for delaying AD-related neurodegeneration in men with metabolic syndrome.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261465674 - Supplemental material for One-month early time-restricted eating enhances long-term memory by modulating brain fluid dynamics in males with metabolic syndrome: Evidence from perivascular diffusion and global blood-oxygen-level-dependent-cerebrospinal fluid coupling
Supplemental material, sj-docx-1-alz-10.1177_13872877261465674 for One-month early time-restricted eating enhances long-term memory by modulating brain fluid dynamics in males with metabolic syndrome: Evidence from perivascular diffusion and global blood-oxygen-level-dependent-cerebrospinal fluid coupling by Linshuang Feng, Xin Jin, Xiaoshi Li, Tingting Qu, Hui Guo, Zirui Wang, Yazhou Quan, Liwei Chen, Lei Wang and Yarong Wang in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
ORCID iDs
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of Xi’an Daxing Hospital (Approval Number: KY2024-025).
Consent to participate
Written informed consent was obtained from all participants before enrollment.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.