
Abstract
Population aging is redefining the clinical reality of Alzheimer's disease and increasing the need for outcome measures that reflect the complexity of older adults. Although recent trials on putative disease-modifying drugs have moved beyond cognition-only endpoints and now include integrated cognitive-functional measures, frailty remains underrepresented in trial design. We discuss the demographic context of aging societies, the relevance of frailty to dementia expression, and the implications of recent amyloid-β-targeting antibody trials, which include substantial numbers of older adults. We propose that frailty can improve external validity, refine biomarker interpretation, and strengthen precision medicine approaches linking biological measures with functional outcomes
Keywords
Introduction
Population aging is transforming the clinical landscape of Alzheimer's disease (AD). In many countries, old age is no longer a future demographic scenario but a present reality. The proportion of individuals aged 65 years and older continues to grow, and the number of persons aged 80 years and older is rising even faster. 1 This change has profound implications for dementia care because the oldest age groups carry the greatest burden of disability, multimorbidity, dependency, and cognitive decline. In the United States, most people living with AD are older than 75 years, and prevalence rises sharply after age 85. 2 At the same time, aging research has increasingly shown that chronological age alone does not adequately describe health status in later life. Individuals of the same age may differ substantially in physiological reserve, resilience, mobility, autonomy, cognition, and vulnerability to stressors.3,4 Frailty has emerged to capture this heterogeneity because it describes vulnerability arising from reduced physiological reserve rather than chronological age alone. In AD, this distinction is important because cognitive symptoms, functional decline, multimorbidity, mobility impairment, and treatment burden often coexist in the same older person.
Frailty is not a single measurement strategy. It can be operationalized through related but distinct models, including the physical phenotype, the deficit accumulation approach, and global clinical judgment.4–6 These models should be introduced as complementary frameworks rather than interchangeable definitions, since each emphasizes a different dimension of vulnerability. This article discusses why this construct should be incorporated into the evaluation of AD disease-modifying therapies in older adults with biomarker-defined or clinically suspected disease.
Frailty as a clinical and biological construct
Frailty is now recognized as one of the most useful constructs in geriatric medicine because it translates biological aging into clinically observable vulnerability. 3 It identifies persons with reduced reserve across multiple systems who are less able to withstand disease, hospitalization, treatment toxicity, and environmental stressors.3,4 Frailty overlaps with age, disability, and comorbidity, but it is not synonymous with any of them. Its value lies in describing the global health state that influences how an older adult responds to a stressor.
The physical phenotype proposed by Fried and colleagues defines frailty through five measurable criteria: unintentional weight loss, exhaustion, weakness, slow walking speed, and low physical activity. 4 This model is intuitive, biologically plausible, and particularly informative when the research question concerns sarcopenia, mobility, energy expenditure, or physical reserve.
The deficit accumulation model proposed by Rockwood and Mitnitski takes a different approach. It defines frailty as the proportion of health deficits present in an individual across symptoms, diseases, disabilities, and laboratory or functional abnormalities. 5 This produces a continuous frailty index that captures graded vulnerability and is well suited to complex older populations. In AD, this feature is particularly attractive because biological burden, cognitive impairment, and functional loss also unfold along continua rather than as simple yes or no states.
The Clinical Frailty Scale further simplifies assessment by summarizing fitness and frailty through global clinical judgment. 6 It can be useful in pragmatic settings where a full frailty index is not feasible, although it provides less granular information than deficit accumulation measures. These three approaches are therefore complementary. The physical phenotype emphasizes mobility, strength, energy, and activity. The frailty index captures broader multisystem deficit burden. The Clinical Frailty Scale summarizes overall clinical vulnerability.
For AD trials, the choice of frailty model should follow the purpose of the assessment. If frailty is used as an effect modifier, the instrument should characterize physiological reserve without duplicating the primary cognitive or cognitive-functional endpoint. If frailty is used as an outcome, the analysis should clarify which components changed and whether the change reflects cognition, mobility, nutrition, comorbidity, disability, or other domains. This distinction is important because the relevance of frailty to dementia is increasingly clear. Frailty is associated with incident cognitive decline, dementia risk, and worse outcomes after the onset of cognitive impairment.7,8 These associations suggest that the clinical expression of neurodegeneration is partly shaped by the global health state of the individual rather than by neuropathology alone. Frailty may therefore help explain why similar biomarker profiles can lead to different clinical phenotypes and why equal amounts of neuropathology can be associated with different levels of disability.9,10 This observation is highly relevant at a time when the field is moving toward biomarker-defined AD 11 and toward disease-modifying therapies that aim to alter the underlying pathophysiology.
The shift from cognition to meaningful clinical outcomes
The arrival of anti-amyloid monoclonal antibodies has changed the therapeutic perspective. The field is no longer discussing only symptomatic treatment. It is now discussing when to diagnose, whom to treat, how to monitor, and what counts as meaningful benefit. The first generation of disease-modifying trials already reflects an important conceptual evolution. The acetylcholinesterase inhibitor era was dominated by cognitive outcomes. By contrast, the pivotal trials of lecanemab and donanemab used global clinical outcomes that combine cognition and function, thereby acknowledging that patients and families do not experience AD as an isolated deficit in memory or executive performance.12,13 This shift is positive. It is in the direction of the World Health Organization framework of healthy aging, which places functional ability at the center of later life health rather than focusing on disease-specific impairment alone. 14
Even so, the current phase of therapeutic innovation remains incomplete. Cognitive and cognitive-functional endpoints represent progress, but they still do not fully capture the multidimensional vulnerability of older adults. In everyday practice, the patient who presents for evaluation of early AD is rarely defined only by biomarker positivity and a Clinical Dementia Rating Scale (CDR) score. That patient may have sarcopenia, impaired gait, polypharmacy, cardiovascular disease, sensory loss, social isolation, low physiological reserve, and fluctuating functional autonomy. These features influence treatment tolerance, adherence, monitoring burden, risk of complications, and real-world effectiveness.3,6 Yet they remain marginal in most trial designs and secondary in most discussions of treatment eligibility.
Older adults in anti-amyloid trials
The age composition of recent anti-amyloid trials makes this omission even more notable. Clarity AD enrolled participants aged 50 to 90 years. 12 TRAILBLAZER-ALZ 2 enrolled a population with early symptomatic AD that extended well into older age. 13 This matters because it contradicts the assumption that contemporary disease-modifying trials are restricted to unusually young and highly selected patients. Older adults were enrolled in meaningful numbers. Moreover, available analyses suggest that the benefit was not confined to younger participants. In Clarity AD, lecanemab slowed the decline in cognition and function in early AD across the trial population, 12 and exploratory analyses also suggested preservation of health-related quality of life and reduced increase in caregiver burden. 15 In TRAILBLAZER-ALZ 2, donanemab significantly slowed clinical progression on integrated and global outcomes. 13 A subsequent policy-oriented review argued that trial participants were broadly representative of Medicare populations in terms of comorbidities, concomitant medications, and treatment settings, and emphasized that donanemab produced meaningful health benefits with a manageable safety profile across diverse practice contexts. 16
These data are important for two reasons. First, they weaken the rationale for excluding older patients a priori from disease-modifying treatment discussions. Second, they reveal the need for a better language to characterize the older adults who are actually treated. Age alone is insufficient. A person aged 78 years who remains mobile, independent, socially engaged, and medically stable is not the same as a person aged 78 years with recurrent falls, exhaustion, impaired gait speed, malnutrition, polypharmacy, and dependence in instrumental activities. Yet current therapeutic discourse often places both individuals under the same age label. Frailty offers a way out of this simplification.
At the same time, frailty should not be presented as absent from the AD literature. Recent work has shown that frailty can provide prognostic information in biomarker-defined mild cognitive impairment due to AD, including associations with baseline cognition and subsequent decline. 17 The point is therefore not that frailty has never been studied in AD, but that it remains underrepresented in the design, reporting, and interpretation of AD disease-modifying therapy trials.
Why frailty should be integrated into Alzheimer's disease trials
Introducing frailty into AD trials would provide immediate conceptual and methodological advantages. These domains are summarized in Table 1. The first advantage is that frailty measures clinical benefit along a continuum of global health rather than within a single domain. Disease modification in AD should not be interpreted only as slower worsening of test scores. It should also be understood as preservation of the patient's capacity to remain active, autonomous, adaptable, and engaged in daily life. Frailty indices are well suited to capture such multidimensional change because they integrate mobility, comorbidity burden, symptoms, disability, and often social or functional deficits. A treatment that produces a modest effect on a cognitive-functional scale but also stabilizes the trajectory of frailty could have a larger real-world value than traditional analyses suggest.
Why frailty should be incorporated into Alzheimer's disease trials.
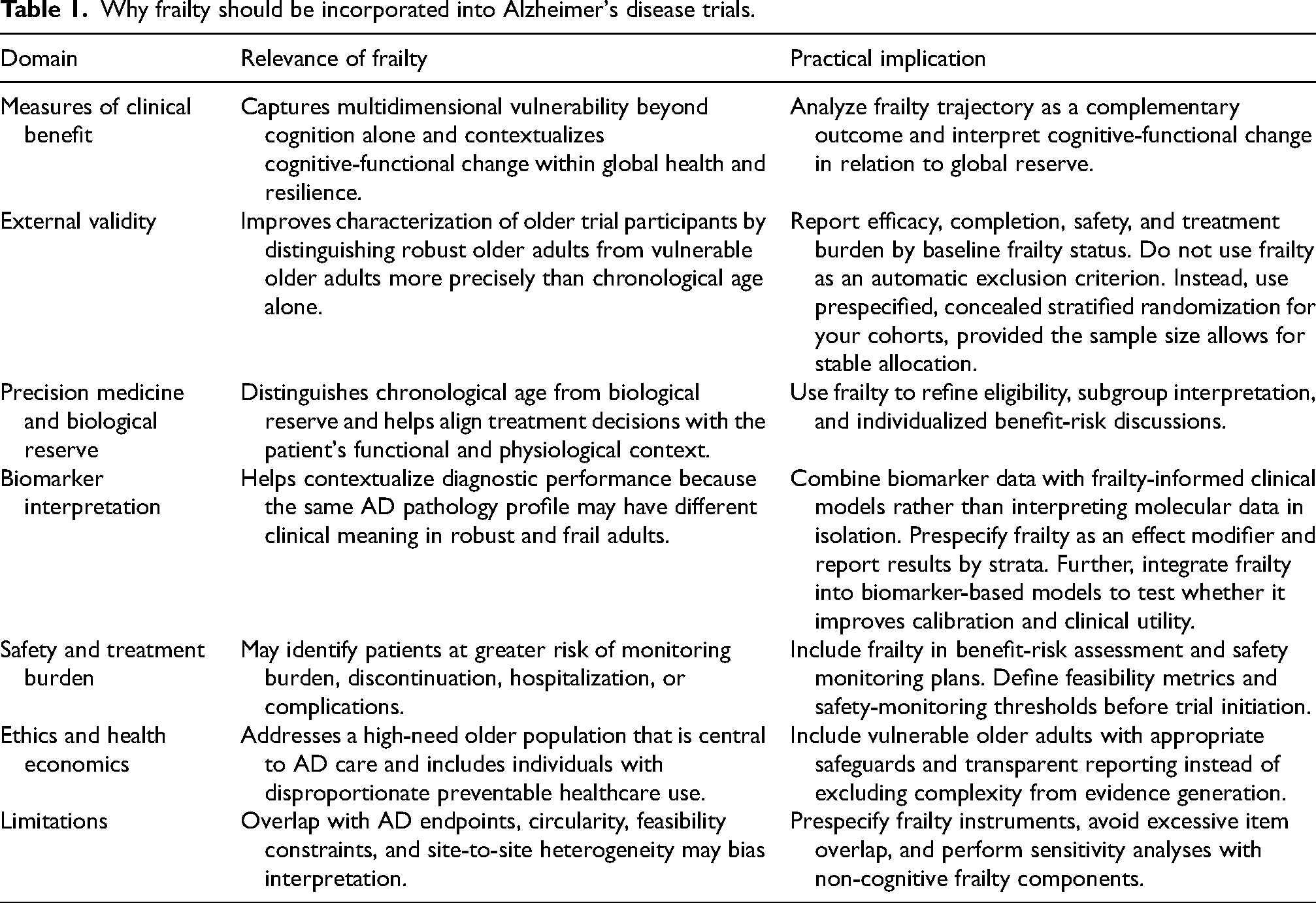
The second advantage concerns external validity. Trial populations are always selected. The relevant question is not whether selection exists but whether we can describe it more intelligently. Frailty assessment would help distinguish robust older participants from vulnerable older participants and would allow investigators to determine whether treatment effects differ according to physiological reserve rather than chronological age alone. This would produce more clinically relevant subgroup analyses and more honest estimates of who benefits most, who completes treatment, who develops complications, and who is likely to derive sustained functional advantage.
The third advantage concerns biomarker interpretation. The shift toward blood-based biomarkers is one of the most promising developments in the field. 18 However, biomarker performance is not independent of clinical context. In settings with a low pretest probability, false-positive results increase. In heterogeneous community populations, systemic illness, vascular disease, inflammation, renal function, and general biological aging may alter the interpretation of plasma signals. Frailty could serve as a bridge variable between biomarker data and clinical decision-making. A frailty-informed diagnostic model would be more precise than a biomarker-only model because it would acknowledge that the same molecular result may have different clinical meaning in a robust 68-year-old and in a frail 86-year-old with multisystem vulnerability.
The fourth advantage concerns safety. Frailty may identify participants who are more likely to experience treatment burden, monitoring difficulties, discontinuation, hospitalization, or complications. This is especially relevant for anti-amyloid therapies because treatment requires repeated imaging, infusion or injection logistics, management of concomitant drugs, and careful interpretation of adverse events.
The fifth advantage is ethical. The very population most affected by AD is also the population most often treated as methodologically inconvenient. Frail older adults account for a disproportionate share of potentially preventable Medicare spending and represent a group with high medical complexity and high unmet need. 19 Their underrepresentation in interventional research has consequences. It narrows the evidence base, encourages overly restrictive implementation, and leaves clinicians without guidance precisely where clinical uncertainty is highest. Excluding frailty from trial design may seem to simplify efficacy testing, but it ultimately transfers complexity from research to practice, where decisions must still be made.
These advantages should be balanced against limitations. Frailty assessment can overlap with AD outcomes, especially when cognitive or functional items are included in a frailty index. It can also increase assessment burden and may be difficult to standardize across international trial sites. These problems do not argue against frailty assessment, but they do require prespecified operational definitions, non-overlapping sensitivity analyses, and pragmatic instruments that can be implemented consistently.
Frailty, reversibility, and prevention
A frailty-oriented perspective also reshapes how we think about prevention and reversibility. Frailty is not always fixed. In many individuals, it is dynamic and at least partially modifiable. This is a crucial point for AD. The traditional separation between neurodegenerative disease and general health decline has probably been too rigid. Dementia prevention research already shows that vascular, metabolic, sensory, psychological, and social factors influence late-life cognitive trajectories. 20 Frailty gathers many of these dimensions into a clinically intelligible construct. In this sense, frailty is not merely a competing outcome. It may be part of the causal terrain on which AD pathology becomes clinically manifest. Intervening on frailty may therefore complement biomarker-directed therapies rather than distract from them.
A framework for frailty-informed therapeutic development
For future trials, the goal should not be to replace established AD outcomes but to enrich them. Core biomarker and clinical end points should remain. What is needed is an additional layer of phenotyping that reflects real aging. Table 2 translates this proposal into a practical trial-development framework. At enrollment, participants should undergo structured frailty assessment using validated approaches based on deficit accumulation, physical phenotype, or global clinical judgment. Longitudinal analyses could test whether baseline frailty modifies treatment efficacy, whether treatment changes frailty trajectories, and whether frailty mediates the relationship between biomarker change and functional outcome. Safety analyses could examine whether frailty predicts treatment discontinuation, burden of monitoring, hospitalization, or complications. Such designs would move the field closer to precision medicine in its proper sense, which is not simply molecular selection, but alignment of therapy with the biological and functional reality of the person.
Key research questions for a frailty-informed Alzheimer's disease trial agenda.
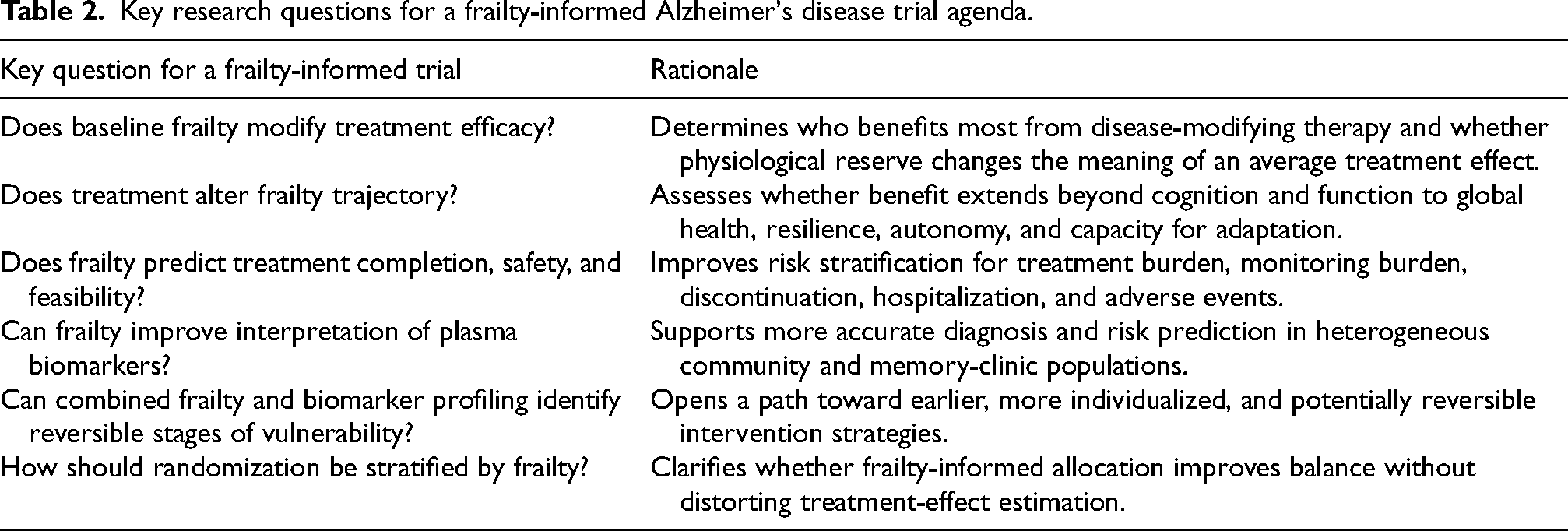
Stratification by frailty should be interpreted carefully. Prespecified stratified randomization does not inherently skew trial results if allocation remains concealed and treatment arms are balanced within each frailty stratum. Instead, it can protect internal validity by preventing unequal distribution of robust and frail participants between groups. The risk arises when frailty strata are introduced after randomization, used to exclude patients without justification, or analyzed with insufficient statistical power.
This approach may also help resolve a tension that has accompanied the anti-amyloid era. Much debate has focused on whether the magnitude of benefit is large enough to justify treatment burden. This question is legitimate, but it cannot be answered in the abstract. The meaning of a given treatment effect depends on the patient's baseline vulnerability and remaining reserve. Slowing decline by a modest amount may be highly meaningful in a person at the threshold of losing independent function. Conversely, the same average effect may be less compelling in a patient whose overall health trajectory is dominated by advanced frailty. Frailty assessment would therefore not only refine eligibility. It would also refine the interpretation of benefit.
To minimize circularity, trials should distinguish the role of frailty before analysis begins. If frailty is used as an effect modifier, the instrument should avoid the same cognitive-functional items that define the primary endpoint. If frailty is used as an outcome, analyses should clearly report which components changed and whether changes were driven by cognition, mobility, nutrition, comorbidity, or disability. This distinction is essential because frailty can otherwise become a different label for the same clinical decline that AD trials already measure.
From disease-centered outcomes to person-centered aging
AD research has long excelled at measuring pathology and cognition. It must now become equally skilled at measuring resilience and global function. The most relevant clinical question in an aging society is no longer whether we can preserve a single function in isolation. It is whether we can help an older person maintain the capacity to live, decide, move, relate, and adapt despite neurodegenerative disease. Frailty speaks directly to that question. It is a translational measure of aging biology, a clinical measure of vulnerability, and a pragmatic measure of what matters in later life.
The therapeutic future of AD will almost certainly be combinatorial. Biomarker-based diagnosis will become more accessible. Disease-modifying therapies will expand. Preventive strategies will continue to target vascular and lifestyle risk. In that future, frailty should not remain an afterthought. It should become a central organizing variable that links biology to function and trial efficacy to real-world meaning. The field has already taken an important step by moving beyond cognition-only endpoints. The next step is to recognize that the success of treatment in older adults cannot be judged fully without understanding the gradient of frailty on which AD unfolds.
Conclusions
Frailty remains an underrepresented dimension in AD disease-modifying therapy trials. Its integration into clinical trials would improve the characterization of older participants, strengthen external validity, refine interpretation of biomarker data, inform safety monitoring, and provide a more meaningful assessment of therapeutic benefit. In an aging world, the central aim of treatment cannot be limited to slowing decline on a scale. It must include preserving the broader capacity to function. Frailty offers a framework for connecting disease-modifying therapy with the lived reality of older adults and should become a standard dimension of future AD therapeutic development.
Footnotes
Acknowledgements
The authors thank all investigators and participants of the original clinical studies mentioned in this article.
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Vincenzo Solfrizzi is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
Dr Bruno P. Imbimbo is an employee of Chiesi Farmaceutici S.p.A. and inventor on company patents related to anti-Alzheimer compounds.
Data availability statement
All data mentioned are derived from publicly accessible published sources cited in the References section.