
Abstract
We assessed cross-sectional lecanemab eligibility (January 2026) in 479 patients with mild cognitive impairment or dementia who underwent Alzheimer's disease (AD) biomarker testing at a tertiary memory clinic (2021–2025). Overall eligibility was 16%, with exclusions due to negative biomarkers (41%), advanced disease stage (31%), APOE ε4/ε4 homozygosity (6%), and other safety reasons (6%). In the 2025 subgroup (n = 100), eligibility increased to 32%, reflecting fewer exclusions for disease progression and a targeted evaluation of patients likely to meet criteria. These findings highlight a narrow post-diagnosis therapeutic window and suggest an upper eligibility limit under the current appropriate use recommendations for anti-amyloid therapies.
Introduction
Anti-amyloid monoclonal antibodies have emerged as the first disease modifying therapies capable of altering the biological trajectory of Alzheimer's disease (AD). Lecanemab is an IgG1 antibody targeting aggregated soluble and insoluble forms of amyloid-β and reduces amyloid-β plaques. In pivotal clinical trials it has demonstrated meaningful slowing of cognitive and functional decline in patients with mild cognitive impairment (MCI) or mild dementia due to AD.1,2 As regulatory approval and guideline adoption expand, accurate estimation of the number of eligible patients becomes increasingly important for healthcare systems. Real-world implementation of these therapies is constrained by the requirement for biomarker-confirmed amyloid pathology and by the need to align with the safety profile defined in clinical trials. These studies have shown that APOE ε4 homozygosity, use of anticoagulant therapy, relevant medical comorbidities, and significant cerebrovascular disease on neuroimaging, all increase the risk of amyloid-related imaging abnormalities (ARIA) which may lead to adverse clinical outcome.3–5 On the basis of these findings, appropriate use recommendations for anti-amyloid therapies, particularly for lecanemab, have been established to guide clinical practice in real-world settings. 6
Estimating the proportion of eligible patients for anti-amyloid therapy in clinical cohorts is essential for anticipating infrastructure needs, including infusion capacity, imaging and safety monitoring resources, and overall economic impact. Previous analyses in memory clinics have reported substantial variability in eligibility rates, reflecting differences in cohort characteristics, screening procedures, and the specific anti-amyloid therapy evaluated.7–16 In many settings, limited access to biomarker testing represents a major barrier, and few studies have focused on cohorts already enriched by biomarker assessment, in which eligibility might be expected to be higher.
In this study, we aimed to quantify eligibility for lecanemab in a biomarker-tested cohort of patients with MCI or mild dementia evaluated in a tertiary dementia clinic over a five-year period, with particular attention to temporal trends and the characteristics of patients evaluated more recently. Our key questions were how many patients in our cohort would be eligible for treatment at the present time, and, in the absence of the unavoidable delays that affected this cohort, how many patients in a more recently evaluated subset would be expected to be eligible under current clinical practice, where timely treatment is available.
Methods
We conducted a retrospective observational study including all patients evaluated at a tertiary dementia clinic (Fundación Jiménez Díaz, Madrid, Spain) between 2021 and 2025 who were diagnosed with MCI or mild dementia and had undergone AD biomarker assessment using either cerebrospinal fluid (CSF) biomarkers or amyloid positron emission tomography (PET). The primary objective was to estimate the number of patients within this biomarker-tested cohort who would be eligible for treatment with the recently approved lecanemab at the present time. A total of 479 patients were included, and eligibility criteria were assessed cross-sectionally in January 2026. In addition, a predefined subgroup analysis was conducted in patients evaluated in 2025 (n = 100) to explore potential changes in eligibility related to evolving diagnostic practices 6 and more recent case ascertainment. The study was approved by the Ethics Committee of Fundación Jiménez Díaz as part of an ongoing research project on biomarkers in neurodegenerative dementias.
CSF biomarker testing was performed in 95% of cases, including Aβ42, Aβ40, phosphorylated tau 181 (ptau181), and total tau, analyzed using Lumipulse G600II chemiluminescent immunoassay (Fujirebio Iberia, Barcelona, Spain). Biomarker positivity was defined as A + according to validated clinical thresholds for amyloidosis (Aβ42/Aβ40 ratio < 0.068), independently of ptau181 values. This includes all patients with cognitive symptoms across the amyloidosis spectrum, even those in the earliest stages who do not yet show biomarkers of neurodegeneration. Amyloid PET imaging with 18 F-flutemetamol (Vizamyl, GE Healthcare, Norway) was performed in 5% of cases and interpreted visually by experienced nuclear medicine specialists.
Eligibility assessment followed current clinical guidelines for anti-amyloid therapy in early AD, based on the CLARITY AD trial criteria and appropriate use recommendations (Supplemental Table 1). 6 Exclusion criteria were applied sequentially in the following order: negative AD biomarkers; APOE ε4/ε4 homozygosity; age outside the approved therapeutic window; cognitive impairment beyond mild stage; anticoagulant treatment or significant comorbidities; significant cerebrovascular disease. This sequence was primarily chosen for efficiency and feasibility, prioritizing variables readily available in our databases (CSF biomarker status, APOE genotype, and age). Subsequently, medical records were reviewed for the remaining cases (half of the cohort) and current disease severity, anticoagulant therapy, and comorbidities, were reassessed in January 2026, at a single cross-sectional time point. If a patient met an exclusion criterion (e.g., moderate dementia), subsequent criteria were not evaluated. As a consequence of this stepwise approach, neuroimaging was ultimately assessed in 86 cases (18% of the initial cohort). The most recent available scans were reviewed, typically performed within the previous 18 months.
Cognitive stage was determined based on clinical evaluation supported by standard cognitive measures and by functional status using the Global Deterioration Scale (GDS). 17 GDS scores of 2–3 were considered MCI (corresponding to Clinical Dementia Rating [CDR] global score of 0.5) whereas a GDS score of 4 was classified as mild dementia (CDR 1). Significant cerebrovascular disease was defined as Fazekas grade 3 white-matter hyperintensities, multiple infarcts, including stroke involving a major vascular territory, more than four cerebral microbleeds, any macrohemorrhage greater than 10 mm in diameter, cortical superficial siderosis, or evidence of vasogenic edema. In addition, inflammatory amyloid-related vasculopathies, as well as other major intracranial pathologies with potential to cause cognitive impairment, were considered exclusionary. Neuroimaging assessment was based on magnetic resonance imaging (MRI), or computerized tomography (CT) scan when MRI was not available.
Descriptive statistics were used to quantify exclusion and eligibility proportions. Exclusion criteria were applied sequentially, and percentages were calculated relative to the initial cohort size.
Results
A total of 479 patients with MCI or mild dementia underwent AD biomarker testing between 2021 and 2025. The mean age of the cohort was 66.8 ± 9.4 years, and 54% were women.
Full 2021–2025 cohort (n = 479)
After sequentially applying the eligibility criteria, substantial attrition was observed at each exclusion step (Figure 1, left). The most frequent exclusion criterion was the absence of biomarker-confirmed AD pathology, resulting in the exclusion of 41% of patients. An additional 6% of the cohort was excluded due to APOE ε4/ε4 homozygosity. Cognitive stage constituted another major exclusion factor: 31% of the overall cohort was considered ineligible because they had progressed beyond the mild dementia stage (GDS > 4 or CDR > 1) over these few years from initial study.
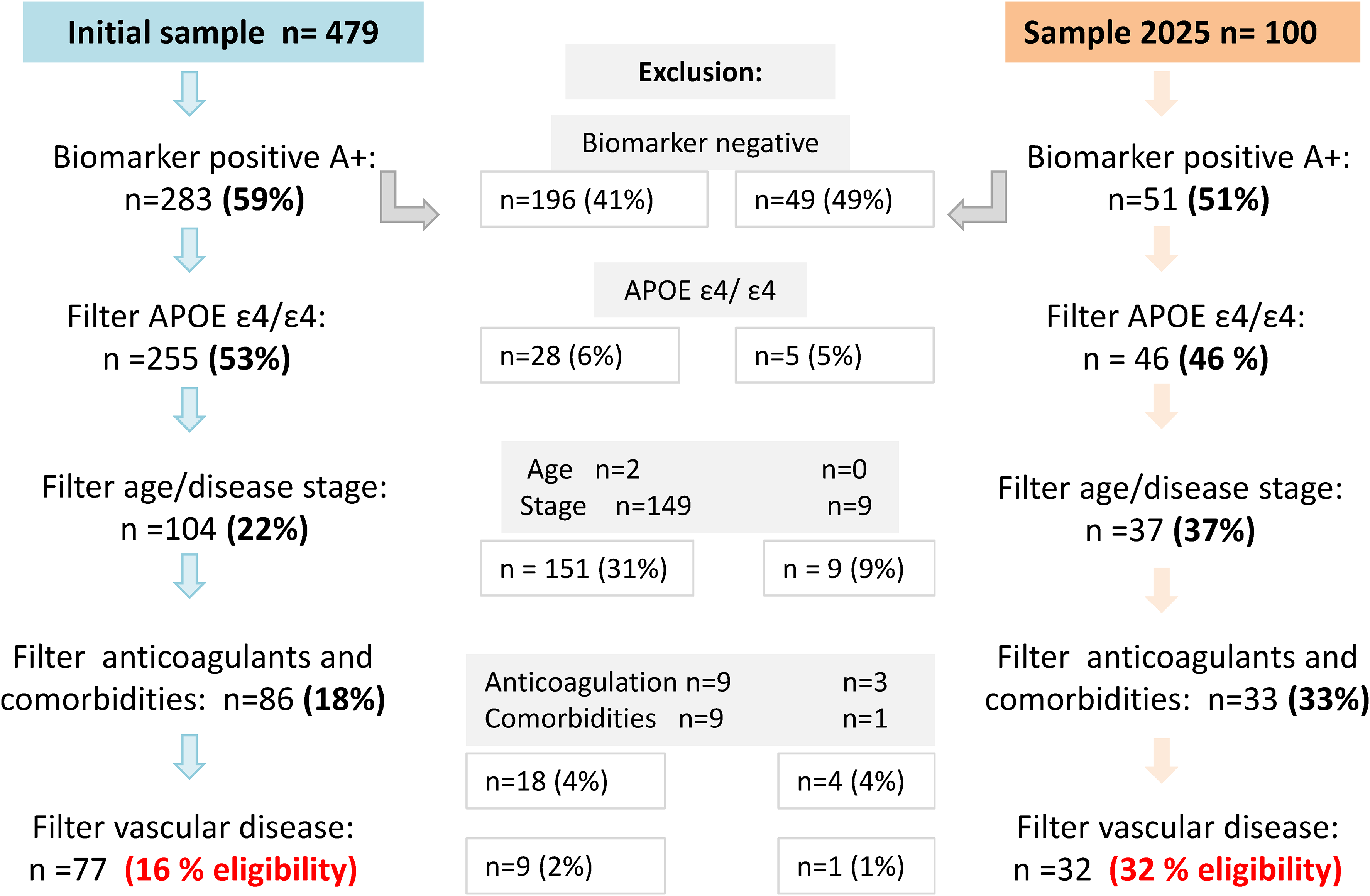
Assessment of potential eligibility for lecanemab treatment according to appropriate use recommendations 6 in patients studied with AD biomarkers. Left, full cohort (2021–2025). Right, subset of patients evaluated during 2025.
Safety-related criteria had a more limited impact on eligibility. Overall, 6% of patients were excluded due to ongoing anticoagulation, significant medical comorbidities, or high cerebrovascular burden. Cerebrovascular disease was assessed using CT instead of MRI in 27% of cases. After all exclusion criteria were applied, 16% of the initial cohort (approximately one in six patients) met full eligibility requirements.
2025 subgroup (n = 100)
In the subset of patients evaluated in 2025 (mean age 67 ± 6.4 years, 54% women), biomarker negativity again represented the most common exclusion factor, affecting 49% of patients (Figure 1, right). APOE ε4/ε4 status accounted for an additional 5% of exclusions. In contrast to the full cohort, progression to a moderate disease stage did not contribute substantially to exclusions. Importantly, this does not imply that patients diagnosed in 2025 were identified at an earlier stage than those diagnosed, for example, in 2023; rather, they simply had not yet had sufficient time to progress to a more advanced stage. Other safety-related exclusion factors, including ongoing anticoagulation, comorbidities, or cerebrovascular burden, accounted for 14% of cases. In this subgroup only 6% of the cases had neuroimaging evaluated with CT instead of MRI. Overall, 32% of patients evaluated in 2025 were eligible for treatment, representing a twofold increase compared to the full five-year cohort.
In summary, eligibility for lecanemab in our biomarker-tested cohort was predominantly limited by biomarker-negative status and disease stage, whereas safety-related exclusions accounted for a comparatively minor proportion of ineligible cases. The higher eligibility observed in 2025 was consistent with more recent-stage evaluation and reduced exclusion due to disease progression, together with a deliberate priorization of biomarker testing in patients more likely to fulfill the clinical criteria for eligibility.
Discussion
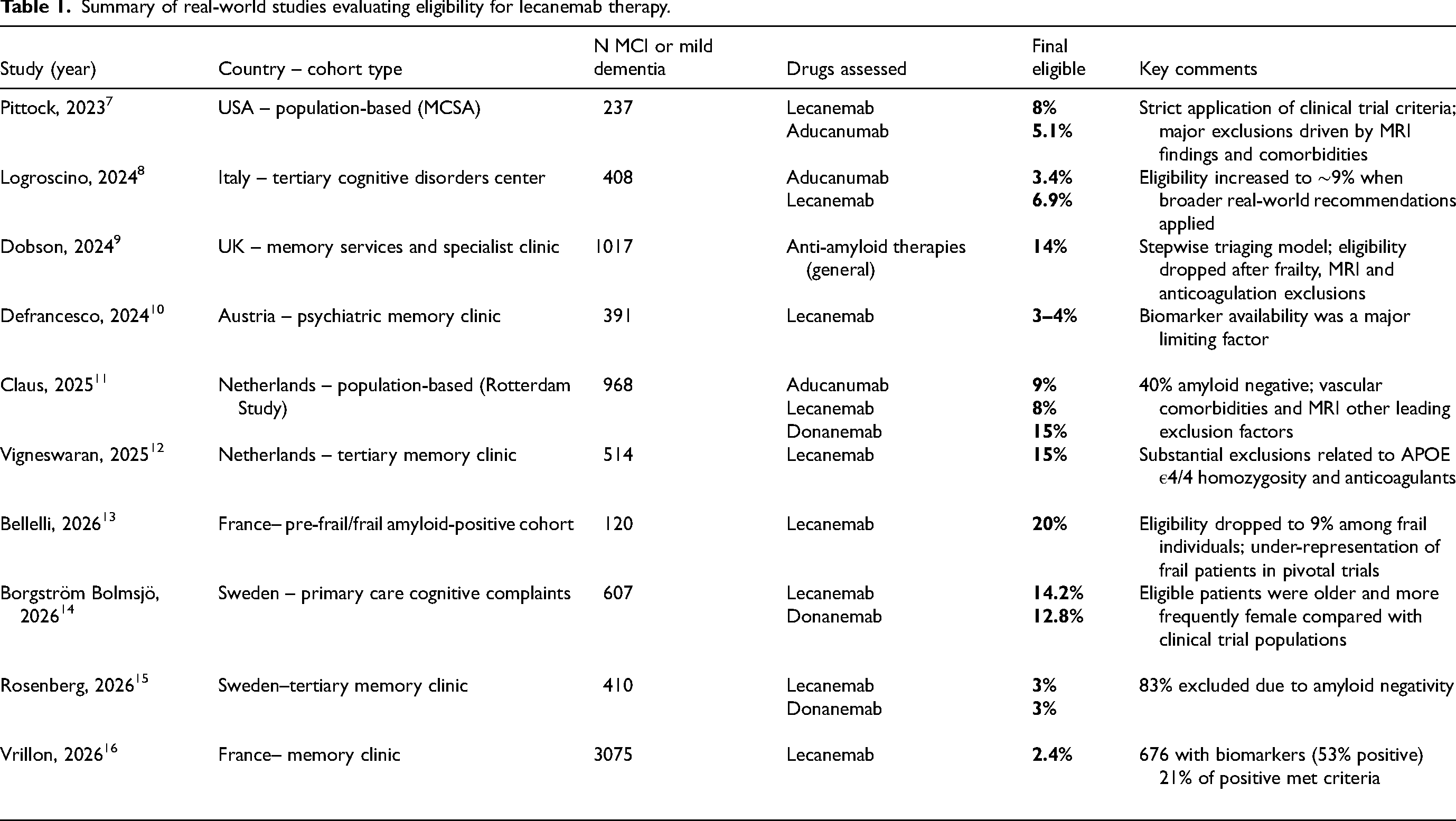
In this biomarker-enriched cohort of individuals evaluated for MCI or mild dementia suspected to be caused by AD pathology, only 16% ultimately met eligibility criteria for anti-amyloid therapy. This figure provides new data within the limited set of real-world estimates from diverse clinical settings, where eligibility proportions range from 5% to 15% (summary of studies in Table 1).7–16 Our estimate falls in the upper range because our initial sample, patients selected for biomarker assessment through lumbar puncture in our cohort, was already biased towards younger age, fewer medical comorbidities, and prior exclusion of cases in treatment with anticoagulants.
Summary of real-world studies evaluating eligibility for lecanemab therapy.
The largest contributor to ineligibility in our sample was the absence of biomarker confirmed AD, consistent with reports indicating that up to 40–50% of patients evaluated for cognitive symptoms do not have underlying amyloid pathology, even in specialized settings.7,11,15,16,18 In certain memory clinics where patients are evaluated solely on the basis of memory complaints, up to 83% of cases have been found to have normal CSF Aβ42 levels. 15 These findings emphasize that AD is not the underlying etiology in a large proportion of cognitive complaints and reinforce the critical role of biomarker testing for diagnostic accuracy and for the rational allocation of disease-modifying therapies.
Disease stage constituted the second major determinant of ineligibility. Our approach—assessing how many patients in our cohort were currently eligible for treatment, rather than evaluating eligibility at the time of first clinical assessment as in other studies—revealed that a substantial proportion of patients progressed from mild to moderate dementia over three years of follow-up. Nearly one third of the cohort, including a substantial proportion of patients evaluated in 2021 and 2022, exhibited cognitive impairment beyond the mild stage by early 2026. This finding highlights the impact of delays between symptom onset, biomarker confirmation, and treatment consideration, which have previously been identified as major barriers to therapeutic access.3,16,19,20 From a clinical perspective, these results emphasize the importance of timely referral and early biomarker evaluation.
APOE ε4 homozygosity was present in 10% of cases with positive AD biomarkers and was associated with an approximate 6% reduction in eligibility within the initial sample. Additional safety-related exclusion factors, including comorbidities, anticoagulant therapy, and significant vascular burden, accounted for a smaller proportion of ineligible cases. This was largely attributable to a conservative approach to lumbar puncture in frail patients, based on multiple clinical considerations.
Notably, eligibility within the 2025 subgroup increased to 32%, approximately double the rate observed across the full five-year cohort. Two factors may explain this increase. First, biomarker assessment at our center became more deliberately targeted toward individuals considered potentially eligible for treatment, following the publication of the appropriate use recommendations for lecanemab. 6 Second, most patients in this subset were at an early stage of disease and had not yet had time to experience significant clinical deterioration. Importantly, even under these optimized conditions, eligibility did not exceed one third of the cohort, suggesting that this proportion may represent an approximate upper limit under current appropriate use recommendations for anti-amyloid therapies.
This study has several limitations. First, the cohort was preselected for biomarker testing in a tertiary memory clinic, which may limit the generalizability of the findings to broader clinical populations. Second, the retrospective design may have introduced misclassification or information bias. Third, cerebrovascular burden was not systematically assessed with MRI in all patients (27% in the full cohort and 6% in the 2025 subset were evaluated using CT), potentially leading to an underestimation of imaging-based exclusions. Patients with extensive white matter disease or multiple infarcts were excluded, but some cases with microhemorrhages or cortical siderosis may not have been detected in CT scans. Nevertheless, it is likely that many patients with a clinically significant cerebrovascular burden had already been excluded at earlier steps of the screening process, for example due to APOE ε4 homozygosity, a more advanced disease stage, or the use of anticoagulant therapy.
From a healthcare-planning perspective, these findings provide a pragmatic estimate of the potential demand associated with the implementation of anti-amyloid therapies. An eligibility rate of 15–30% may impose considerable burden on infusion capacity, neuroimaging monitoring, and interdisciplinary coordination. Accurate local estimates, such as those generated here, are essential for anticipating these requirements and to ensure the sustainable integration of disease-modifying therapies into clinical practice.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261466695 - Supplemental material for Eligibility for lecanemab therapy in a biomarker defined memory clinic cohort: A five-year analysis
Supplemental material, sj-docx-1-alz-10.1177_13872877261466695 for Eligibility for lecanemab therapy in a biomarker defined memory clinic cohort: A five-year analysis by Pablo Agüero-Rabes, Javier Roa-Escobar, Raquel Téllez, Verónica Mañanes and Estrella Gómez-Tortosa in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We thank A. Alvarez for the processing of biological samples in Fundación Jiménez Díaz.
Ethical considerations
The Ethics Committee of Fundación Jiménez Díaz approved this study as part of a long-term research project on clinical-genetic and biomarker correlations in neurodegenerative dementias (2014/46; 2021/46; 2023/ 21).
Consent to participate
All patients or their surrogates provided written informed consent for biomarker studies for clinical and research purposes.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has not received particular funding. EISAI company (Spain) has supported the Dementia Unit at Fundación Jiménez Díaz by contributing to the salary of a part-time lab technician. The company has not played any role in the design of the study or in the analysis and interpretation of data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Aggregate data (to preserve patient confidentiality) are available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.