
Abstract
Background
The Clinical Dementia Rating (CDR) scale is widely used for staging mild cognitive impairment (MCI) and dementia but suffers from lengthy administration time (45–60 min). The Montreal Cognitive Assessment (MoCA; 10–15 min) and Quick Dementia Rating System (QDRS; 3–5 min) are promising brief alternatives, although it remains unclear which tool performs better in discriminating between cognitive and functional impairment stages.
Objective
To compare the performance of the QDRS and MoCA in identifying MCI, dementia, and individuals eligible for disease modifying therapies and clinical trials (DMTT).
Methods
376 older adults (34.8% NCI, 33.0% MCI, 32.2% dementia) recruited from the memory clinic (n = 284, 75.5%) and community (n = 92, 24.5%) in Singapore completed the QDRS, MoCA, and CDR. No cognitive impairment (NCI), MCI, and dementia were staged as CDR-Global Scores (CDR-GS) of 0, 0.5, and ≥1, respectively. The DMTT subgroup was defined as CDR-GS of 0.5–1. Discriminative performance was determined by area under the curve (AUC) and compared using DeLong's test. Agreement with CDR classifications was determined on McNemar's test.
Results
Both QDRS and MoCA demonstrated fair-to-excellent discrimination across CDR-staged groups (MCI: AUC 0.79–0.84; Dementia: AUC 0.92–0.97; DMTT: AUC 0.85–0.91), with no significant differences in discrimination observed. The QDRS correctly identified a greater proportion of MCI (55.6% versus 19.4%; p < 0.001) and DMTT (58.9% versus 41.7%; p < 0.001) versus the MoCA.
Conclusions
The QDRS and MoCA are practical brief alternatives to the CDR. The QDRS was advantageous for identifying MCI and DMTT, whereas both were effective screening tools for dementia.
Keywords
Introduction
Dementia affects over 50 million people worldwide, with cases expected to double every 20 years.1,2 As the prevalence of dementia rises, there is a critical need to identify individuals with mild cognitive impairment (MCI)—a transitional stage preceding dementia characterized by mild cognitive and functional deficits with preserved independence in daily activities. 3 Timely detection of MCI supports earlier intervention, including disease-modifying therapies (DMTs) that target the underlying pathologies of dementia. The expansion of clinical trials for DMTs has increased the need for brief, cost-effective screening tools to enable efficient patient recruitment.4,5
Brief screening tools are routinely used in clinical settings (e.g., memory clinics and clinical trials) to detect and stage cognitive impairment (i.e., MCI and dementia), alongside confirmatory biomarker testing to determine underlying disease pathology.6,7 For instance, individuals who screen positive for MCI may undergo further investigations, such as an amyloid positron emission tomography (PET) scan, to confirm the presence of amyloid plaques, a hallmark of Alzheimer's disease (AD).8,9 Brief screening tools enable rapid triage and potentially reduce the need for more extensive assessments, thereby minimizing costs, and patient and clinician burden.
The Clinical Dementia Rating (CDR) scale, a staging tool for cognitive and functional decline, 10 is widely regarded as the gold standard in identifying MCI and dementia due to its high classification accuracy to established diagnostic criteria; and use in global datasets as a reliable indicator of symptom severity.10–13 However, the CDR is limited primarily by its lengthy administration time (45–60 min). 14 The Montreal Cognitive Assessment (MoCA) and Quick Dementia Rating System (QDRS) are promising alternatives in time-limited settings. The MoCA is a 10-min performance-based cognitive test, 15 whereas the QDRS is a 3–5 min informant-based measure of cognitive and functional decline. 16 Both screening tools have demonstrated high accuracy in identifying MCI and dementia against the CDR,16–18 with evidence supporting superior performance over other brief assessments such as the Mini-Mental State Examination (MMSE).19–21 However, it remains unclear how the QDRS and MoCA perform in discriminating between CDR-staged no cognitive impairment (NCI), MCI and dementia.
Establishing which assessment is superior in detecting MCI and dementia can enable earlier detection, diagnoses and access to treatments, and better planning for future care, thereby improving patient outcomes. 22 This study aims to determine whether the QDRS or MoCA is more effective in identifying MCI, dementia, and individuals eligible for DMTs and clinical trials, as staged on the CDR-Global Score (CDR-GS). Although individuals with MCI remain functionally independent, subtle changes in complex, cognitively-demanding activities (e.g., managing finances, remembering appointments) may be present and detectable by close informants. 23 As the QDRS captures informant-reported changes across both cognitive and functional domains, it may be more sensitive to early changes than performance-based cognitive testing. Conversely, as dementia progresses and cognitive deficits become more pronounced, performance-based cognitive tools such as the MoCA may offer greater utility. Hence, we hypothesize that the QDRS will be superior for detecting MCI and DMT- and trial-eligible individuals, whereas the MoCA will be superior for detecting dementia.
Methods
Study sample
This cross-sectional study recruited participants recruited from two memory clinics in Singapore (National University Hospital and St Luke's Hospital) and the community between June 2020 and December 2024. Participants were aged 50 years or older, able to speak and write in English, Chinese, or Malay for neuropsychological assessments, and able to provide informed consent. Exclusion criteria were diagnoses of major psychiatric illness or substance abuse disorder, cognitive impairment caused by a history of traumatic brain injury, multiple sclerosis, tumor(s), epilepsy, systemic disease(s), and significant visual or auditory abnormalities. As a predominantly clinical cohort, individuals with neurological conditions associated with dementia, including cerebrovascular disease (e.g., stroke) and Parkinson's disease, were not excluded. 24 These conditions are recognized contributors to cognitive impairment and commonly co-exist with AD, particularly in Asian populations,25,26 and their inclusion enhances the generalizability of the findings to real-world clinical settings. Participants who did not have a reliable informant (i.e., ≥10 h a week of interaction with the participant) for QDRS and CDR assessments were excluded. Demographic data such as age, sex, race, and years of formal education were collected.
Ethics approval was obtained from the National Healthcare Group Domain-Specific Review Board, and the study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained in the preferred language of all participants by study coordinators prior to study recruitment.
Administration of the MoCA and QDRS
The MoCA is a 30-point test designed to detect dementia based on cognitive performance. 15 It assesses 6 key cognitive domains: memory recall, visuospatial ability, executive functioning, attention, language, and orientation. The MoCA was administered by a trained neuropsychological rater during study visits. MoCA assessment items were summed to produce a total score, ranging from 0–30, with lower scores indicative of worse cognition. 15 Previous literature has evidenced that MoCA scores are education-dependent, necessitating adjustment based on the educational level of the study population. 27 In this study, a locally-modified (Singaporean) version of the MoCA was employed to more accurately reflect the lower educational level of our cohort and older adults in Singapore. 19 This version adds one point to the total score for individuals with ≤6 years of education to correct for education effects, and has been used in Asian samples with a similar level of education, such as Hong Kong and Korea.28,29 This is in contrast to the adjustment threshold proposed in the original English MoCA (≤12 years of education), which was derived from a sample with higher educational attainment. 15
The QDRS is a 10-item informant-based questionnaire designed to stage cognitive impairment via evaluation of a participant's degree of change in cognitive and functional capacity. 16 Ten cognitive and functional areas are assessed: memory, orientation, judgement and problem solving, function outside the home, function at home and hobbies, basic self-care, behavior and personality, language and communication abilities, mood, and attention/concentration. 16 An informant with ≥10 h of interaction a week with their paired study participant completed the QDRS during study visits. In this study, informants comprised the participant's child (45%), spouse (44%), sibling (6%), extended family member (e.g., niece, uncle; 3%), or close acquaintance (2%). Questionnaire items are scored between 0, 0.5, 1, 2, and 3, corresponding to increases in symptom severity (e.g., for memory, 0 represents no obvious memory loss or inconsistent forgetfulness, 0.5 represents consistent mild forgetfulness, 1 represents mild-to-moderate memory loss, etc.). The QDRS total score is the sum of the 10 questionnaire items and ranges from 0 to 30, with higher scores reflecting worse cognitive and functional impairment. 16
Staging of cognitive impairment on the CDR
The CDR was used to stage cognitive and functional impairment, administered as semi-structured interviews with the participant and informant to obtain information regarding the participant's cognitive and daily functioning in six categories: memory, orientation, judgment and problem solving, community affairs, home and hobbies, and personal care. 11 Trained raters, blinded to the participant's MoCA and QDRS scores, administered the CDR. The same informant who completed the QDRS was interviewed for the CDR. Each category was scored on five levels of impairment (0 = none, 0.5 = questionable, 1 = mild, 2 = moderate, and 3 = severe) using information obtained from both participant and informant. Ratings were guided by standard CDR procedures, with greater weight given to informant-reported cognitive and functional decline. 30 In cases of uncertainty (e.g., discordant or ambiguous information from participant and informant reports), ratings were reviewed and resolved by study team consensus. The CDR-GS was derived from a synthesis of the individual ratings in each of the six categories. Based on CDR-GS, participants were categorized into three groups: NCI (CDR 0), MCI (CDR 0.5), and dementia (CDR 1–3). In addition, participants with CDR 0.5–1 were categorized into a DMT- and trial-eligible (DMTT) subgroup, representing individuals eligible for DMT intervention and clinical trial recruitment for AD.31,32 This operationalization has been used in previous studies. 32
Data collection
The MoCA, QDRS, and CDR were administered in the participant's preferred language (either English or Chinese). The Chinese version of the tests was translated by bilingual psychologists and was previously validated in Chinese samples.33–35 Data collected were obtained in a single study visit if both participant and informant were present (i.e., MoCA, QDRS, participant and informant input for CDR); otherwise, a separate session within 1–2 weeks of the participant's study visit was scheduled to retrieve informant data.
Statistical analysis
Group differences for categorical variables (sex and race) were analyzed using chi-squared tests. Normality of continuous variables (age, years of education, QDRS, and MoCA scores) was assessed using Shapiro–Wilk tests. All continuous variables were found to have non-normal distributions. Accordingly, group differences in continuous variables across CDR groups were analyzed using Kruskal–Wallis tests.
Binary logistic regression models were fit with age and years of education as covariates, with MoCA and QDRS included as predictors in separate and combined models. To avoid overfitting and inflated performance estimates, model training and evaluation were performed with five-fold cross-validation. Within each fold, models were fit on the training subset and applied to the held-out validation subset. Optimal classification cut-offs for each group were determined in the training data using Youden's index and applied to the validation data to estimate sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Performance metrics were averaged across folds to obtain cross-validated estimates.
ROC analyses
Univariate receiver-operating characteristic (ROC) analyses were used to assess ability of the QDRS and MoCA to discriminate between CDR-staged MCI and NCI (CDR 0.5 versus 0); dementia versus non-dementia (CDR≥1 versus ≤0.5); dementia versus MCI (CDR≥1 versus 0.5); DMTT versus NCI (CDR 0.5–1 versus 0); and advanced dementia versus DMTT (CDR≥2 versus 0.5–1). Using five-fold cross-validated models, univariate area under the ROC curves (AUCs) were generated to assess the discriminatory utility of each brief tool. Multivariate AUCs were generated from logistic regression models adjusted for age and educational attainment. AUCs were reported with 95% Confidence Intervals (CIs), and compared using DeLong's test. 36 AUC values were interpreted according to established thresholds. 37
Classification agreement with the CDR
Based on the optimal classification cut-offs, MoCA- and QDRS-staged groups (NCI, MCI, dementia, and DMTT) were generated. Agreement between these classifications and the CDR-staged classifications was assessed using cross-tabulations, which identified the proportion of participants with identical and different class assignments. Classification agreement between the MoCA- and QDRS-staged groups against CDR-staged groups was assessed on McNemar's test.
Post-hoc power analysis
A post hoc, simulation-based power analysis was conducted to assess sample size adequacy. For group comparisons, Monte Carlo simulations (1000 iterations per condition) were conducted to estimate power for Kruskal–Wallis tests using the observed distributions of QDRS and MoCA scores. Power was defined as the proportion of simulations with p < 0.05. Estimated power exceeded 0.99 for QDRS at a sample size of 10 per group; and power of 0.80 for the MoCA at 30 participants per group. A second Monte Carlo simulation (500 iterations per comparison) was conducted to estimate power for detecting differences in AUCs using DeLong's test, based on effect sizes derived from logistic regression models including age, education, QDRS, and MoCA. A minimum of 50 participants per group was sufficient to achieve ≥80% power, which was exceeded in the current cohort.
Assumptions of statistical tests
Assumptions for statistical analyses were assessed prior to testing. Assumptions for analysis of categorical variables (sex, race) on chi-squared tests were satisfied, with all expected cell counts ≥5. For logistic regression models, linearity of the logit was assessed using Box–Tidwell transformations (all p > 0.05), and assumptions were satisfied, including binary outcome specification and independent observations. Multicollinearity was examined using variance inflation factors, with all values <5, indicating no evidence of collinearity. Statistical analyses were conducted using SPSS v29.0 and R v4.3, and statistical significance was determined at p < 0.05 (2-tailed).
Results
Sample characteristics
Of the 477 older adults recruited between June 2020 and December 2024, 101 did not have an available informant and were subsequently excluded. A total of 376 eligible participants (284 [75.5%] from the memory clinic and 92 [24.5%] from the community) were included in the final analysis.
Demographic information and QDRS and MoCA scores by CDR-staged groups are presented in Table 1. Post-hoc pairwise comparisons on Dunn's test revealed significant differences between all groups for most variables (all p < 0.05), except age, which did not differ between CDR-staged NCI and MCI (p = 0.11) following Bonferroni corrections. As cognitive and functional stage increased (i.e., NCI to MCI to dementia), participants were older; had fewer years of education; and had lower MoCA and higher QDRS scores (all p < 0.001). Group comparisons of DMTT to other cognitive and functional stages are presented in Supplemental Table 1.
Sample characteristics.
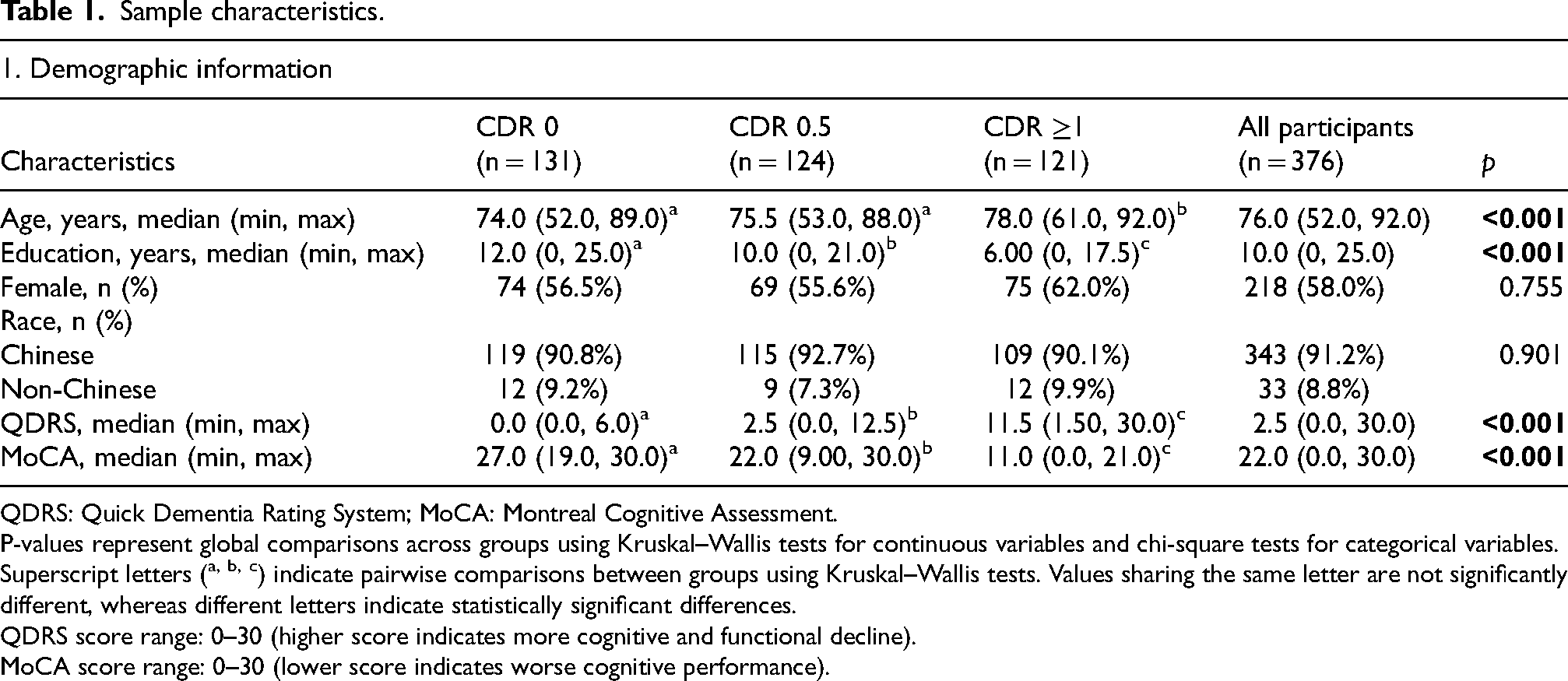
QDRS: Quick Dementia Rating System; MoCA: Montreal Cognitive Assessment.
P-values represent global comparisons across groups using Kruskal–Wallis tests for continuous variables and chi-square tests for categorical variables.
Superscript letters (a, b, c) indicate pairwise comparisons between groups using Kruskal–Wallis tests. Values sharing the same letter are not significantly different, whereas different letters indicate statistically significant differences.
QDRS score range: 0–30 (higher score indicates more cognitive and functional decline).
MoCA score range: 0–30 (lower score indicates worse cognitive performance).
Comparison of the QDRS and MoCA
Discriminatory performance of the QDRS and MoCA across cognitive and functional impairment groups is presented in Tables 2 to 4. Across all groups, no significant differences were observed between QDRS and MoCA in univariate analyses (M1 versus M2 in Tables 2 to 4; all p > 0.05). In multivariate analyses, differences between the two tools did not reach statistical significance after including demographics (age and years of education) as covariates (M4 versus M5 in Tables 2 to 4; all p > 0.05). Adding QDRS or MoCA to demographics (AUC 0.79–0.97; M4 and M5 in Tables 2 to 4), as well as combining both tools (AUC 0.87–0.98; M6 in Tables 2 to 4), significantly improved discrimination compared to demographics alone (AUC 0.60–0.77; M3 in Tables 2 to 4; all p < 0.001).
Univariate and multivariate AUCs for discriminating MCI from NCI.
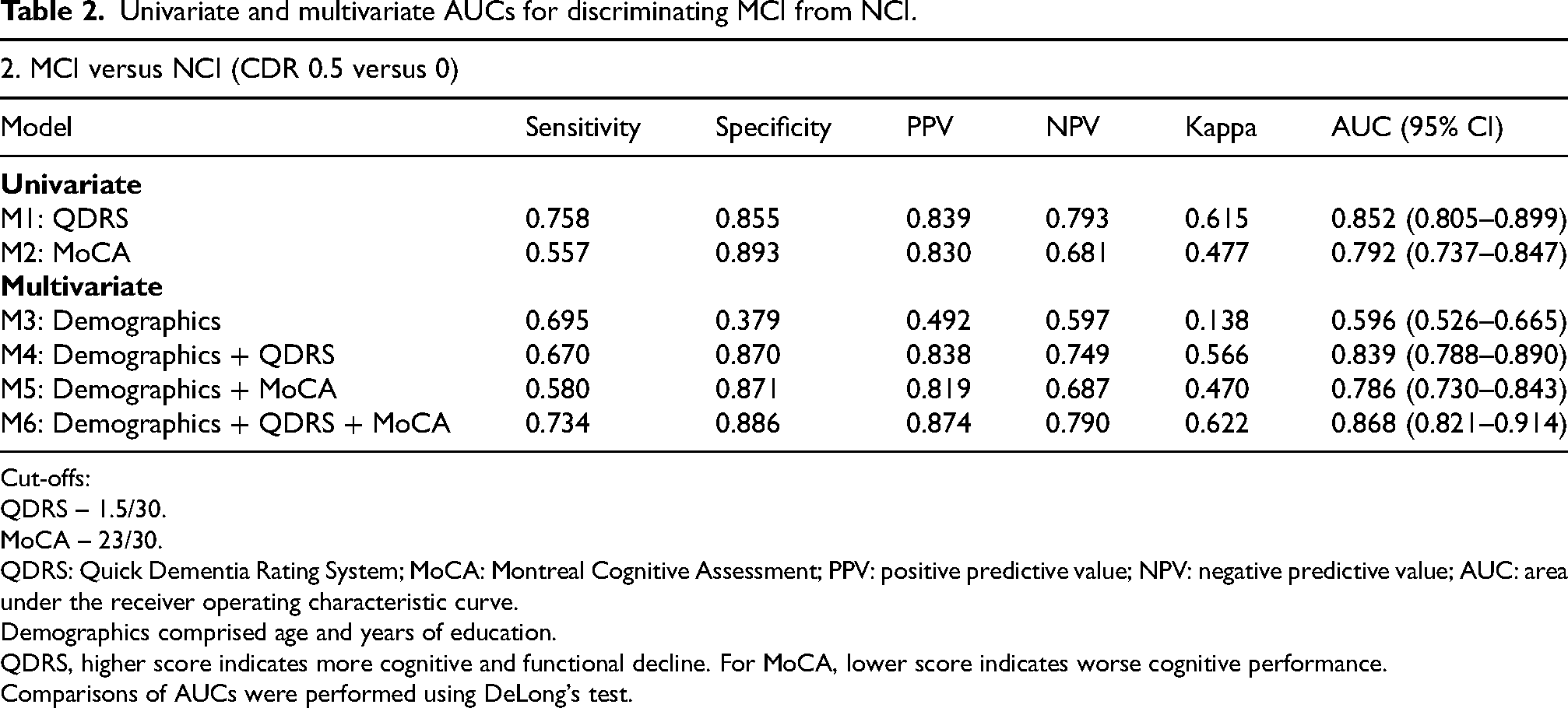
Cut-offs:
QDRS – 1.5/30.
MoCA – 23/30.
QDRS: Quick Dementia Rating System; MoCA: Montreal Cognitive Assessment; PPV: positive predictive value; NPV: negative predictive value; AUC: area under the receiver operating characteristic curve.
Demographics comprised age and years of education.
QDRS, higher score indicates more cognitive and functional decline. For MoCA, lower score indicates worse cognitive performance.
Comparisons of AUCs were performed using DeLong's test.
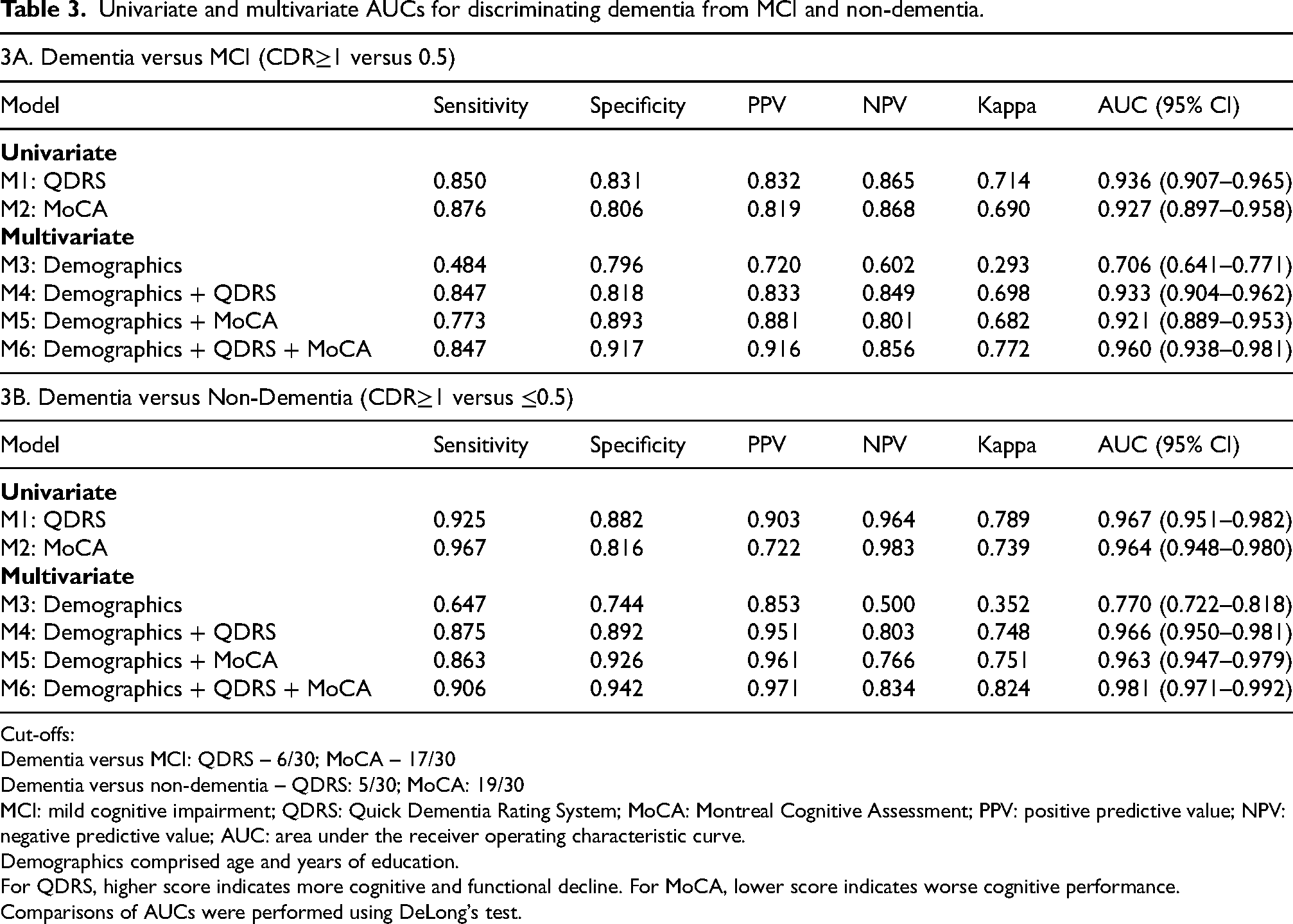
Univariate and multivariate AUCs for discriminating dementia from MCI and non-dementia.
Cut-offs:
Dementia versus MCI: QDRS – 6/30; MoCA – 17/30
Dementia versus non-dementia – QDRS: 5/30; MoCA: 19/30
MCI: mild cognitive impairment; QDRS: Quick Dementia Rating System; MoCA: Montreal Cognitive Assessment; PPV: positive predictive value; NPV: negative predictive value; AUC: area under the receiver operating characteristic curve.
Demographics comprised age and years of education.
For QDRS, higher score indicates more cognitive and functional decline. For MoCA, lower score indicates worse cognitive performance.
Comparisons of AUCs were performed using DeLong's test.
Univariate and multivariate AUCs for discriminating DMTT from NCI and advanced dementia.
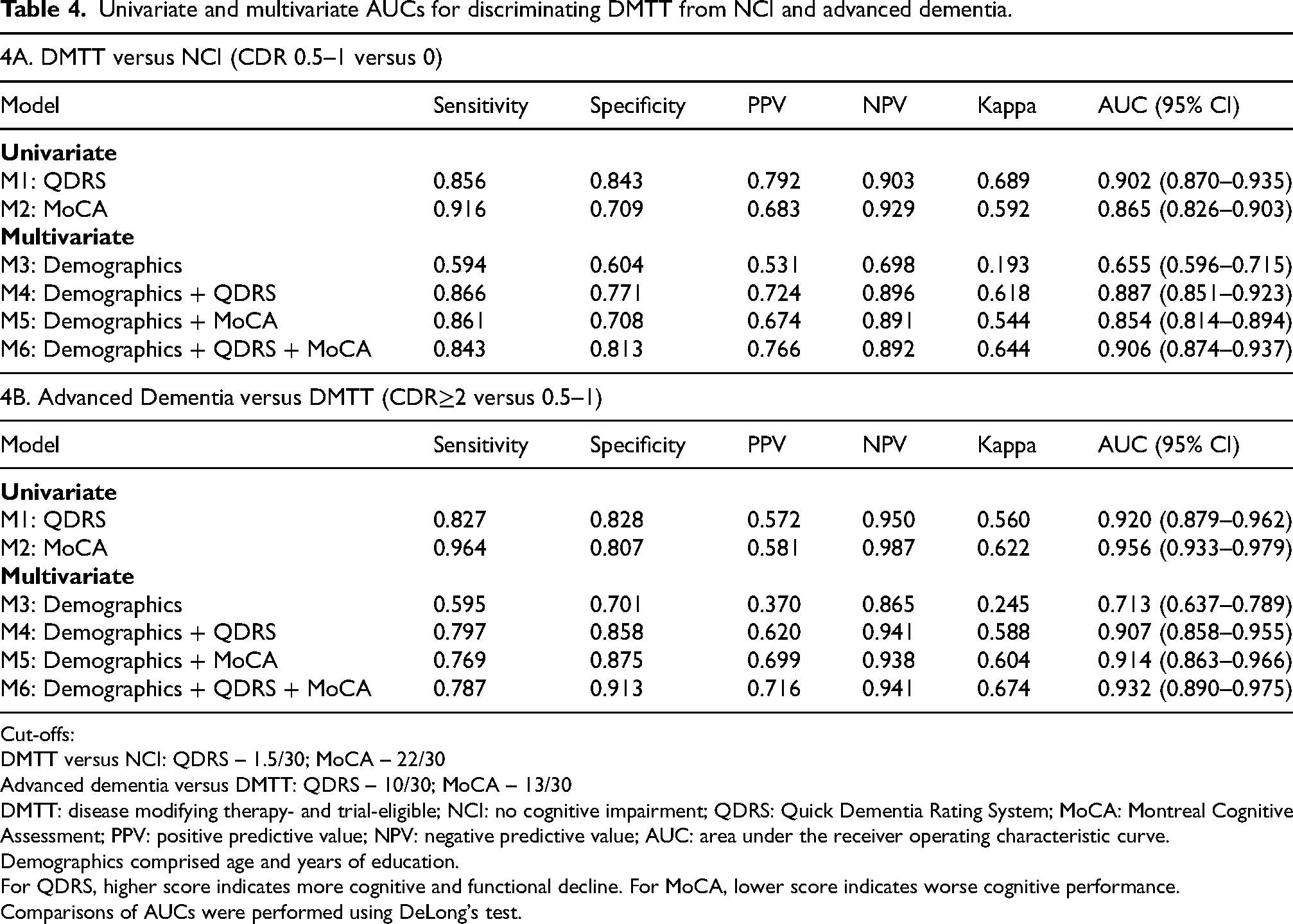
Cut-offs:
DMTT versus NCI: QDRS – 1.5/30; MoCA – 22/30
Advanced dementia versus DMTT: QDRS – 10/30; MoCA – 13/30
DMTT: disease modifying therapy- and trial-eligible; NCI: no cognitive impairment; QDRS: Quick Dementia Rating System; MoCA: Montreal Cognitive Assessment; PPV: positive predictive value; NPV: negative predictive value; AUC: area under the receiver operating characteristic curve.
Demographics comprised age and years of education.
For QDRS, higher score indicates more cognitive and functional decline. For MoCA, lower score indicates worse cognitive performance.
Comparisons of AUCs were performed using DeLong's test.
Discriminating MCI from NCI
For distinguishing MCI from NCI (CDR 0.5 from 0; Table 2), the combined QDRS + MoCA + demographics model achieved the highest performance (M6 AUC 0.868). DeLong's test revealed significantly higher discrimination for the combined model compared to MoCA + demographics (M6 versus M5; AUC 0.868 versus 0.786; 95% CI = 0.037–0.125; p < 0.001), but not compared to QDRS + demographics (M6 versus M4; AUC 0.868 versus 0.839; 95% CI = −0.007–0.064; p = 0.111).
Discriminating dementia from MCI and non-dementia
Models including either QDRS or MoCA with demographics showed excellent discrimination in identifying CDR-staged dementia from MCI and non-dementia (AUC 0.92–0.97; M4 and M5 in Table 3(a) and 3(b)). For distinguishing dementia from MCI (CDR≥1 from 0.5; Table 3(a)), DeLong's test revealed significantly higher discrimination for the combined model compared to QDRS + demographics (M6 versus M4; AUC 0.960 versus 0.933; 95% CI = 0.009–0.045; p = 0.003) and MoCA + demographics (M6 versus M5; AUC 0.960 versus 0.921; 95% CI = 0.016–0.061; p < 0.001). A similar pattern was observed when distinguishing dementia from non-dementia (CDR≥1 from ≤0.5; Table 3(b)), where the combined model showed significantly greater discrimination compared to QDRS + demographics (M6 versus M4; AUC 0.981 versus 0.966; 95% CI = 0.005–0.025; p = 0.003) and MoCA + demographics (M6 versus M5; AUC 0.981 versus 0.963; 95% CI = 0.007–0.029; p = 0.001).
Discriminating DMTT from NCI and advanced dementia
For discriminating individuals eligible for DMTs and clinical trials, models including either QDRS or MoCA with demographics achieved good discrimination against NCI (AUC 0.85–0.89; M4 and M5 in Table 4(a)) and excellent discrimination against advanced dementia (AUC 0.91; M4 and M5 in Table 4(b)). When distinguishing DMTT from NCI (CDR 0.5–1 from 0; Table 4(a)), DeLong's test showed significantly higher discrimination for the combined model compared to QDRS + demographics (M6 versus M4; AUC 0.906 versus 0.887; 95% CI = 0.005–0.033; p = 0.009) and MoCA + demographics (M6 versus M5; AUC 0.906 versus 0.854; 95% CI = 0.015–0.089; p = 0.006). However, when distinguishing advanced dementia from DMTT (CDR≥2 from 0.5–1; Table 4(b)), the combined model did not show statistically significant improvement over QDRS + demographics (M6 versus M4; AUC 0.932 versus 0.907; 95% CI = −0.028–0.079; p = 0.353) and MoCA + demographics (M6 versus M5; AUC 0.932 versus 0.914; 95% CI = −0.002–0.037; p = 0.073).
Classification agreement of the QDRS and MoCA with the CDR
Classification agreement of the QDRS and MoCA for detecting MCI versus NCI and dementia versus MCI relative to the CDR is reported in Table 5(a) and 5(b), respectively. No significant differences were observed between the QDRS and MoCA in classifying NCI (112 [85.5%] versus 122 [93.1%]; p > 0.05) and dementia (87 [71.9%] versus 97 [80.2%]; p > 0.05). The QDRS identified a significantly greater proportion of MCI cases than the MoCA (69 [55.6%] versus 24 [19.4%]; p < 0.001). In terms of overall classification accuracy, the QDRS outperformed the MoCA across both comparisons (MCI versus NCI: 71.0% versus 57.3%; dementia versus MCI: 63.7% versus 49.4%; both p < 0.05). Classification agreement with the CDR for the DMTT subgroup is reported in Supplemental Table 2. Among the 192 patients classified as DMTT (CDR 0.5–1), the QDRS correctly identified more cases than the MoCA (113 [58.9%] versus 80 [41.7%]; p < 0.001).
Classification agreement of QDRS and MoCA with the CDR for detecting NCI, MCI, and dementia.
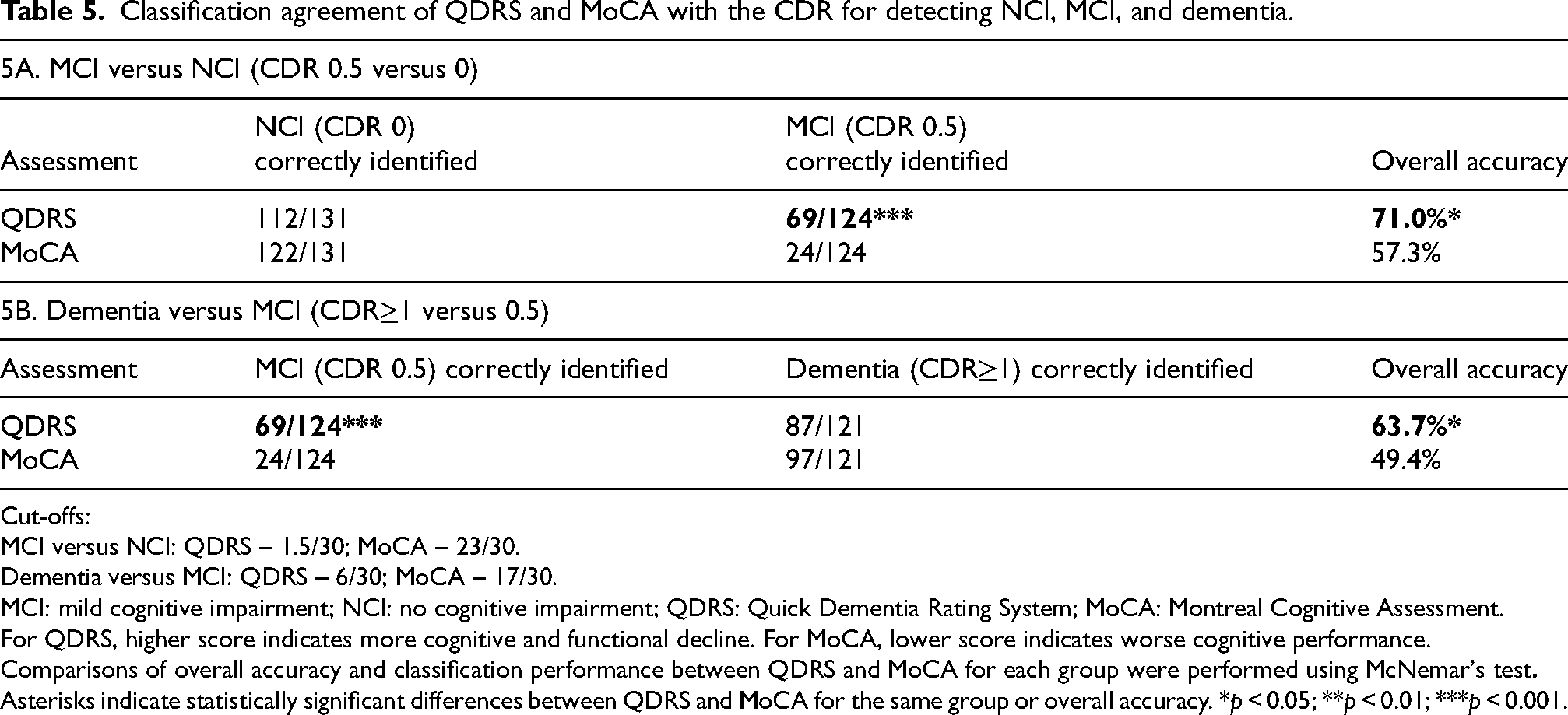
Cut-offs:
MCI versus NCI: QDRS – 1.5/30; MoCA – 23/30.
Dementia versus MCI: QDRS – 6/30; MoCA – 17/30.
MCI: mild cognitive impairment; NCI: no cognitive impairment; QDRS: Quick Dementia Rating System; MoCA: Montreal Cognitive Assessment.
For QDRS, higher score indicates more cognitive and functional decline. For MoCA, lower score indicates worse cognitive performance.
Comparisons of overall accuracy and classification performance between QDRS and MoCA for each group were performed using McNemar's test
Asterisks indicate statistically significant differences between QDRS and MoCA for the same group or overall accuracy. *p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
This study compared the discriminatory performance of the QDRS and MoCA in detecting MCI, dementia, and DMTT in a memory clinic sample, as staged on the CDR-GS. We hypothesized that the QDRS would be superior in detecting MCI and DMTT, whereas the MoCA would be superior in detecting dementia. The QDRS and MoCA demonstrated good discrimination (all AUC≥0.79) across all CDR-GS-staged cognitive and functional impairment groups. However, neither tool outperformed the other in univariate and multivariate analysis (all p > 0.05), demonstrating comparable performance in stage-dependent discrimination.
Discriminating MCI
For distinguishing MCI from NCI (CDR 0.5 from 0), administration of both QDRS and MoCA improved discrimination relative to MoCA alone (p < 0.001) but not QDRS (p = 0.111). Although no significant differences in AUC were observed between the QDRS and MoCA in detecting MCI, the QDRS identified a significantly greater proportion of MCI cases against NCI and dementia (55.6% versus 19.4%; p < 0.001). This appears to be driven by its higher sensitivity (0.758 versus 0.557), indicating better detection of true MCI cases; as well as higher NPV (0.793 versus 0.681), suggesting fewer missed cases among those classified as non-MCI.
This pattern may reflect differences in how each tool captures early cognitive and functional changes. Both the QDRS and CDR evaluate functional decline, whereas the MoCA is primarily a performance-based cognitive tool with limited assessment of everyday function. Individuals classified as CDR 0.5 often exhibit subtle functional impairments that may not be captured by brief cognitive tests 38 ; the MoCA may misclassify such cases, whereas the QDRS remains more sensitive to such changes. Taken together, these findings suggest that the QDRS may be advantageous in settings where sensitivity is a priority, such as in early screening of impairment.
Moreover, the MoCA's poor utility in discriminating between MCI and NCI may be partly attributable to the influence of education in the current cohort. A previous Singaporean memory clinic study demonstrated that education had a stronger effect on MoCA scores than MCI diagnoses (partial η2 estimates: 0.115 versus 0.010); and that the MoCA displayed chance performance (AUC 0.50) in discriminating between MCI and NCI individuals with >6 years of education. 39 Given the relatively high educational attainment of MCI participants in the present study (median education: 10 years), educational attainment may have reduced differences in MoCA scores, and thus the MoCA's ability to discriminate between the MCI and NCI groups.
Although the influence of education on QDRS scores has not been directly examined, the QDRS's utility in discriminating between MCI and NCI in the cohort may be attributable to its informant-based nature, which captures multi-domain cognitive and functional changes, and is less susceptible to educational and cultural influences that may affect performance-based cognitive screening tools such as the MoCA.16,18 Our findings support that the QDRS offers additional discriminatory signal beyond objective cognitive testing, particularly in Asian populations with moderate levels of educational attainment.
Discriminating dementia
For discriminating dementia (CDR≥1) from MCI (CDR 0.5) and non-dementia (CDR≤0.5), combining both tools improved model performance compared to either alone (all p < 0.01). However, incremental gains were modest, as univariate models already demonstrated excellent discrimination (AUC 0.93–0.97). No significant differences were observed between the QDRS and MoCA in identifying CDR-staged dementia (87 [71.9%] versus 97 [80.2%]; p > 0.05; Table 5). Results suggest that either test alone may be sufficient in screening for dementia, with limited added clinical value from combining both measures – particularly in settings where brevity or feasibility is prioritized.
Discriminating individuals eligible for DMTs and clinical trials
In detecting DMTT (CDR 0.5 and 1), the combined QDRS and MoCA model displayed excellent discriminatory performance (AUC 0.91–0.93) in discriminating between DMTT to NCI; and to advanced dementia (CDR 0 and ≥2, respectively). Notably, the QDRS detected a significantly greater proportion of CDR-staged DMTT than the MoCA (113 [58.9%] versus 80 [41.7%]; p < 0.001; Supplemental Table 2). As previously discussed, this may be attributable to the QDRS's ability to detect functional impairment over the MoCA and its potentially lower susceptibility to education effects. This interpretation is consistent with previous research that evidenced lower discriminatory performance of the MoCA in the earliest stages of cognitive impairment (AUC for dementia versus non-dementia [0.91]; and MCI versus NCI [0.80]). 40 As the CDR 0.5–1 subgroup is often the target population for DMTs and clinical trials, the QDRS may be preferred over the MoCA in this context. Previous simulations in a clinical trial setting support this, demonstrating that administration of the QDRS prior to the CDR reduced the time needed to identify MCI subjects by 75.3%. 20
Utility of QDRS and MoCA as brief screening tools
More efficient screening tools are critical to improve triage of individuals for comprehensive evaluations. Results from the current study support a context-dependent approach to employing brief screening tools: the QDRS may be advantageous to screen for individuals with MCI and early stage disease who may be eligible for DMTs and clinical trials, particularly where sensitivity is prioritized and cognitive test performance may be influenced by educational biases. In contrast, both the QDRS and MoCA demonstrated comparable performance for identifying dementia. This approach may optimize accuracy and feasibility in clinical practice, with brief screening to guide triage, followed by subsequent biomarker assessments conducted to confirm underlying pathology.
Important features of the two tools should be considered when administered in routine clinical practice. The QDRS offers practical advantages over the MoCA: it can be informant-administered and completed in 3–5 min without trained personnel, delivered remotely (e.g., via digital form or telephone), and is less susceptible to cultural bias and education effects. 16 Its accuracy may also depend on the informant's living arrangement and relationship with the patient.23,41 For instance, spouses and cohabiting informants have been shown to provide more accurate reports of patients’ memory than non-cohabitants. 42 It is worth noting that 101 individuals were excluded from the current study due to the absence of an informant, which highlights minor limitations to applying the QDRS in routine clinical settings. Patients suspected of cognitive impairment require assessment regardless of informant availability, and informant-based measures may not always be feasible. In these contexts, performance-based tools such as the MoCA may be administered to the patient, highlighting complementary roles of the QDRS and MoCA in clinical assessment.
Comparison with existing literature
Our findings align with previous research, which demonstrated that the MoCA was highly sensitive in identifying dementia patients (AUC 0.90–0.91)40,43; and that the QDRS displayed good overall discriminatory ability for both MCI (AUC 0.84–0.88)16,20,44 and dementia (AUC 0.83–0.86).16,18,44 In the present study, both tools demonstrated fair-to-excellent discrimination (AUC 0.79–0.97) across the cognitive and functional continuum. However, past studies primarily compared the MoCA to the MMSE,45,46 and the QDRS only to the Ascertain Dementia 8 (AD8) and MMSE. 20 The current study addresses the gap in existing literature by comparing discriminatory performance of both the MoCA and QDRS relative to the gold-standard – the CDR.
Comparison of optimal cut-offs with previous studies
The optimal QDRS cut-off identified in this study for MCI (≥1.5) is consistent with the original QDRS validation study, 16 whereas the cut-off for dementia (≥5) is consistent with previous South Korean 44 and Chinese 34 studies. A previous study that recruited memory clinic patients in Singapore reported the same cut-off for MCI as the current study, but a higher cut-off of ≥6 for dementia. 20 This discrepancy is likely due to the variance in scores from the two samples.
Differences between the present MoCA cut-offs (≤23 for MCI and ≤19 for dementia) and those established in local 47 and international48,49 validation studies may have arisen due to differences in population-specific factors such as education, which is known to influence MoCA performance. 50 A comparison among validation studies of the MoCA in Asian countries revealed that samples with lower mean years of education reported lower optimal cut-off points for MCI (e.g., Japan: 12.4 ± 2.5 [≤25 cut-off]; Taiwan: 9.8 ± 5.1 [≤23 cut-off]; Korea: 8.3 ± 3.7 [≤22 cut-off]).28,51,52 This trend was consistent in the current study (9.4 ± 5.2 [≤23 cut-off]). In contrast, validation studies of the MoCA in Western countries showed greater variability in regional cut-offs relative to years of education, possibly reflecting wider intra-regional heterogeneity in sociodemographic factors (e.g., United States: 14.0 ± 2.6 [≤23 cut-off]; Colombia: 12.2 ± 5.2 [≤23 cut-off]; Mexico: 10.7 ± 5.2 [≤26 cut-off]; Italy: 8.9 ± 4.3 [≤25 cut-off]).49,53–55 Hence, the authors recommend that future studies employ validated region-specific cut-offs when utilizing the MoCA.
Strength and limitations
A key strength of the current study is the comparison between the QDRS and MoCA against the CDR. Validation of tools against established assessments guides researchers and clinicians in choosing the most appropriate test for specific purposes, such as screening for clinical trial recruitment and DMT eligibility, and identifying dementia patients in a memory clinic setting. Our study is also the first to compare the ability of the QDRS and MoCA in identifying individuals eligible for DMTs and clinical trials based on cognitive and functional impairment, prior to biomarker confirmation. Accurate identification of this population is critical as this subgroup represents the primary target in AD clinical trials and DMT intervention in primary care. 31
One limitation of the current study is that distinct CDR-GS-staged groups were collapsed to form clinically relevant groups. For example, CDR-GS of 1, 2, and 3 were combined to form the dementia group (CDR≥1) whereas CDR 0 and 0.5 were combined to form the non-dementia group (CDR≤0.5), as this better reflects real-world settings where distinguishing dementia from earlier stages (i.e., both MCI and NCI) is critical. Similarly, CDR global scores of 0.5 and 1 were combined to group individuals who may be eligible for DMTs and clinical trials. However, combination of distinct stages may have introduced spectrum effects that could inflate classification accuracy.
It is notable that the first six items of the QDRS correspond to the CDR domains, introducing some conceptual and structural overlap between the two tools. Although this may increase the agreement between the two, it reflects a key feature of the QDRS as a rapid staging instrument designed to approximate CDR ratings for screening. 16 In this study, both assessments were administered to the same informant, which may contribute to higher concordance. Lastly, study participants were predominantly from a single racial group (91.2% Chinese), which limits the generalizability of our findings to different ethnicities in Singapore.
Future directions
Future studies that examine the QDRS and MoCA's ability to predict cognitive decline are necessary to determine their prognostic utility. As the current cohort was predominantly memory clinic-based, validation in a community-based sample where the prevalence of healthy individuals is higher would clarify key discriminatory properties of the QDRS, including its PPV and NPV. Future research should also examine the influence of educational attainment on QDRS scores to determine whether the QDRS is less susceptible to educational bias, especially compared to performance-based assessments like the MoCA.
Clinically meaningful changes in assessment scores have been established for the MMSE, MoCA, and CDR.56,57 Determining the minimum clinically important difference in QDRS scores would enable clinicians to identify meaningful cognitive decline through a rapid screening tool (3–5 min) that can be administered remotely. Literature also supports the added value of integrating cognitive tools and biomarkers in detecting dementia, with a previous study showing that the combination of plasma p-tau, brief cognitive tests, and APOE genotype predicted AD more accurately than plasma p-tau alone (AUC 0.91 versus 0.83, p < 0.001). 58 As no studies have yet to investigate the combined utility of the QDRS and MoCA with blood-based biomarkers, future work could examine whether integrating plasma biomarkers such as p-tau217 with these tools enhances diagnostic and prognostic utility in dementia assessment.
Conclusion
In a memory clinic-based sample in Singapore, the QDRS and MoCA demonstrated comparable overall discriminatory performance in detecting MCI, dementia and individuals eligible for DMTs and clinical trials, as staged on the CDR-GS. Differences in discriminant indices and practical utility suggest that each tool has distinct context-specific advantages. The QDRS offers an efficient and accessible screening tool for MCI, DMT eligibility, and clinical trial recruitment, whereas both tools are effective screening tests for dementia. Further validation of effective and efficient screening tools is essential to ensure timely and accurate diagnoses, and can enable earlier interventions to slow and potentially prevent progression. Further research is recommended to explore the broader utility of the QDRS, with the goal of integrating it into routine practice and clinical trials.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261467344 - Supplemental material for A comparison of the Quick Dementia Rating System and Montreal Cognitive Assessment for detecting mild cognitive impairment and dementia assessed by the Clinical Dementia Rating Scale
Supplemental material, sj-docx-1-alz-10.1177_13872877261467344 for A comparison of the Quick Dementia Rating System and Montreal Cognitive Assessment for detecting mild cognitive impairment and dementia assessed by the Clinical Dementia Rating Scale by Christian Anton Ng, Mark J.H. Lim, Eddie Jun Yi Chong, Giorgio Colombo, Victor R. Schinazi, Narayanaswamy Venketasubramanian and Christopher Li-Hsian Chen in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors thank all participants for their involvement and the research team (clinical research coordinators, psychometric raters, data management team) from the Memory Ageing and Cognition Centre (MACC) in National University of Singapore for patient recruitment, data collection, and data management.
Ethical considerations
Ethics approval was obtained from the National Healthcare Group Domain-Specific Review Board. The study was conducted in accordance with the Declaration of Helsinki.
Consent to participate
Written informed consent was obtained in the preferred language of all participants by study coordinators prior to study recruitment.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the Singapore National Medical Research Council (grants number NMRC/CG/NUHS/2010 and MOH-000707) and the National Research Foundation Singapore (NRF) under its Campus for Research Excellence and Technological Enterprise (CREATE) programme.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material for this article is available online.