
Abstract
Background
The survival time following an initial Alzheimer's disease dementia (ADD) diagnosis is influenced by various demographic, cognitive and clinical factors. Cognitive clusters are more detailed than individual cognitive measures, but they are rarely used as predictors in survival analyses.
Objective
We conducted a long-term retrospective study following patients from the time of their initial ADD diagnosis until their death. Cognitive clusters as well as clinical data were assessed as predictors of survival time.
Methods
We used hierarchical clustering to identify cognitive clusters based on the results of neuropsychological examinations (CERAD-Plus). We fitted a Cox regression model with cognitive clusters and clinical covariates (e.g., age, sex, Mini-Mental State Examination [MMSE] score, annual rate of hospitalizations, and pre-existing diseases) to predict survival time.
Results
Data from 202 patients (mean age = 77.79 ± 5.35 years; mean survival time 74.04 ± 41.03 months) were analyzed. Two cognitive clusters were identified: the amnestic cluster (AC, N = 89) and the mixed cluster (MC, N = 80). The Cox regression models identified the following variables as most predictive of shorter survival times: higher age (HR = 1.04) and lower MMSE score at baseline (HR = 0.92), pre-diagnosed atrial fibrillation (HR = 2.06) and delirium (HR = 3.13), and a higher annual rate of psychiatric (HR = 4.84) and somatic (HR = 1.67) hospitalizations. Patients in the MC had a shorter survival time than those in the AC group (HR = 1.45).
Conclusions
This study provides evidence that a detailed analysis of neuropsychological profiles at the time of ADD diagnosis can predict disease progression. Preventing psychiatric hospitalizations, especially, could positively influence the survival of ADD patients.
Introduction
Alzheimer's disease dementia (ADD) is the most prevalent form of dementia worldwide and, consequently, represents the greatest financial burden. It is expected to affect an increasing number of people, primarily due to the ongoing trend of rising life expectancy.
The majority of patients with Alzheimer's disease (AD) are not diagnosed until the onset of clinical symptoms, meaning they are diagnosed at the dementia stage. During this phase, treatment costs escalate rapidly, particularly in terms of care expenses, and there is a concomitant decline in both quality of life and life expectancy. Although new therapeutic strategies for AD 1 will slightly slow the progression of the disease in a small proportion of patients, controlling modifiable risk and progression factors remains an essential part of dementia therapy.
The diagnosis of ADD is primarily based on clinical symptom presentation and typical patterns of cortical atrophy. The amnestic hippocampal type is the most common clinical phenotype, with impaired learning and recall of new information being key symptoms. 2 Other atypical AD phenotypes include the dysexecutive frontal variant, the logopenic variant, primary progressive aphasia, or the corticobasal variant. 3 However, clinical phenotypes, particularly in atypical variants, can sometimes overlap. 4
The median survival time following an ADD diagnosis ranges from three to seven years. 5 Survival prospects are influenced by various factors, including age, sex, somatic and cognitive deficits, as well as behavioural symptoms. Somatic factors that increase the risk of death in people with ADD include common comorbidities such as cardiovascular disease, cerebrovascular disease, and diabetes.6,7 In addition to these comorbidities, acute medical events such as infections also increase the risk of death in people with ADD. 8 Infections are also among the most common causes of hospital admission in people with dementia, alongside falls, hip fractures, and delirium. 9 People with ADD are usually admitted to psychiatric wards as inpatients due to an acute deterioration in behavioural and psychological symptoms of dementia (BPSD), which makes care at home difficult. Symptoms such as agitation, aggression, mood disorders, and sleep disturbances can be challenging for family members and professional carers to manage. Such conditions frequently often in hospital admission. 10 Frequent readmissions to hospital may indicate inadequate or incorrect treatment of BPSDs or other somatic disorders.9,11 This is particularly relevant for patients with ADD, given that ADD itself increases the risk of in-hospital mortality.12,13
A significant proportion of studies on mortality risk in people with ADD have focused on demographics or pre-existing somatic conditions at the time of diagnosis. However, only a limited number of studies have examined how different medical events influence survival time between diagnosis and death. Furthermore, most studies concentrate on predefined follow-up periods rather than real survival times for patients with ADD, which diminishes their significance, e.g.,.14–16
There is a notable lack of research investigating the use of neuropsychological profiles as predictors of survival in ADD. While some studies have examined neuropsychological variables in order to predict the rate of future cognitive decline, 17 none have examined survival rates. Neuropsychological profiles provide a more comprehensive description of patients with ADD than individual neuropsychological variables (e.g., verbal memory). They also help capture the neuropsychological heterogeneity found in patients with ADD. Several studies have identified various cognitive profiles in patients with ADD, showing impairment in different neuropsychological domains.18,19 However, few studies have examined neuropsychological profiles in clusters of ADD patients and their potential as a prognostic indicator of survival time.20,21 To address this issue, the current retrospective, long-term follow-up study evaluated the predictive value of detailed neuropsychological and clinical measures for survival time from initial ADD diagnosis at a mild-to-moderate stage until death. We hypothesize that clinical and neuropsychological factors positively or negatively influence the survival of patients with mild to moderate ADD. Our analysis focused on modifiable factors and distinct cognitive clusters as predictors of shorter survival time after the initial diagnosis. Furthermore, we evaluated the impact of pre-existing diseases and annual hospitalizations following the initial ADD diagnosis as potential risk markers for survival time with ADD. We believe that our data has the potential to improve care planning for patients, their families, and healthcare providers.
Methods
This long-term, naturalistic follow-up study examined the factors that influence post-diagnostic survival in patients with mild-to-moderate ADD. Data on 202 patients who were initially diagnosed with ADD at the Memory Clinic (Department of Psychiatry, Psychotherapy, Psychosomatics and Medical Psychology) at the Medical University of Innsbruck between 2006 and 2019 were collected retrospectively from their medical records. The initial dementia assessment included a clinical interview, a detailed neuropsychological examination, blood sampling, as well as a cerebral computed tomography (CT) or magnetic resonance imaging (MRI) scan. Data from patients who had died by the time of data analysis (May 1, 2025) were included in the study. The Austrian death registry was consulted to ascertain the dates of death of the patients. Inclusion criteria comprised a diagnosis of mild to moderate probable ADD according to the NINCDS-ADRDA's criteria 22 including: i) significant impairment in cognitive function, corrected for age and education, in at least one memory domain (verbal or figural) and at least one other cognitive domain; ii) subjective memory complaints over the previous six months; iii) deficits in activities of daily living; iv) a Clinical Dementia Rating (CDR) scale score 23 of >0.5; and v) age >60 years. ADD patients with severe dementia (MMSE score ≤15) or other major neurological, mental, or somatic disorders that could influence disease progression were excluded. The primary endpoint of the study was the survival time (in months) between diagnosis and death.
This retrospective study was approved by the Ethics Committee of the Medical University of Innsbruck, Austria (approval number 1102/2024). As the study was retrospective, patients were exempt from signing an informed consent form.
This study adhered to STROBE guidelines for observational studies 24 wherever possible.
Neuropsychological and clinical measures
During the initial assessment, all patients underwent a comprehensive neuropsychological examination comprising the Mini-Mental State Examination (MMSE) 25 and subtests from the Consortium to Establish a Registry for Alzheimer's Disease (CERAD-Plus) battery. 26 This battery included subtests for verbal memory (word list learning, word list recognition, and word list delayed recall), constructional praxis (figure drawing), figural memory (delayed recall), object naming (Boston Naming Test [BNT]), verbal fluency (animals/min, s-words/min), psychomotor speed (Trail Making Test-A [TMT-A]), and cognitive flexibility (Trail Making Test-B [TMT-B]). Age- and education-corrected z-scores were calculated for all cognitive measures. Depression was assessed using the 30-item Geriatric Depression Scale (GDS). 27
Baseline clinical data were retrospectively collected from the local hospital information system and the Austrian electronic health record (Elektronische Gesundheitsakte [ELGA]). This included information on the presence of comorbidities, pre-existing diseases, and medication at the time of ADD diagnosis. During the study period, all documented hospitalizations were categorized as either psychiatric or somatic. The total number of hospitalizations was quantified by the number of admissions per year of survival, reflecting the average number of admissions per year. This measure reflects the overall burden of hospitalizations between the baseline and the time of death, accounting for differences in follow-up time. The exact time of death was retrieved from the Austrian death register.
Statistical analysis
Determining neuropsychological clusters
We performed a hierarchical clustering analysis on neuropsychological variables obtained from the CERAD-Plus battery. Since standard hierarchical clustering requires complete data, we excluded patients with missing values in any of the considered neuropsychological variables (N = 33). This restricted the clustering process to 169 ADD patients with complete data. To assess potential selection bias, we compared excluded and included patients regarding our primary outcome, survival time. To address multicolinearity, one representative variable per cognitive domain was considered for cluster analysis, 28 hence circumventing the need to build sum scores or extracting factors across measures. The following neuropsychological variables were included: word list delayed recall, figural memory (delayed recall), constructional praxis, TMT-A, BNT, and verbal fluency (s-words). All variables were on the same scale provided by the CERAD-Plus battery (z-transformed norms of healthy individuals, adjusted for age, sex, and education). The clustering procedure was performed with the squared Euclidean distance in combination with Ward's linkage method. Ward's method was chosen to avoid small sized clusters as it has the tendency to create balanced cluster-solutions and is recommended to be used in combination with the squared Euclidean distance. 28 The optimal number of clusters was chosen by visual inspection of the scree plot (see Supplemental Figure 1) and the dendrogram (see Figure 1). The t-test was used to compare clusters with normally distributed continuous variables, the Wilcoxon test was used to compare clusters with non-normally distributed continuous variables, and the chi-square test was used to compare clusters with categorical variables.

Dendrogram of the hierarchical cluster analysis performed with squared Euclidean distance method and Ward's linkage method on neuropsychological variables in 169 patients with Alzheimer's disease dementia. Patients were iteratively clustered together using Ward's linkage method, revealing two distinct neuropsychological clusters: cluster ‘Mixed phenotype’ (left side, n = 80) and cluster ‘Amnestic phenotype’ (right side, n = 89). The red horizontal line indicates the distance at which the dendrogram was cut to obtain the two-cluster solution.
A logistic regression with leave-one-out cross validation was conducted to check the internal validity and the relative contribution of neuropsychological variables to the cluster solutions.
The following considerations led to the selection of neuropsychological variables from the CERAD-Plus battery: delayed recall is the measure of episodic memory most consistently reported to have the highest sensitivity for ADD and was hence chosen over other measures of episodic memory (e.g., immediate recall, word list recognition). 29 The TMT-B is commonly used to evaluate executive functioning in patients with ADD, but it could only be administered to a small subset of patients (n = 58), as the majority of the sample were unable to comprehend the instructions or made invalid attempts. Therefore, we selected a verbal fluency task to measure executive functioning in the cluster analysis. While both semantic and phonetic verbal fluency tasks assess executive functioning, we included phonetic fluency (s-words) in the cluster analysis as it relies less on language proficiency. 30 The cluster analysis revealed preserved phonetic fluency performance in patients of the amnestic phenotype (mean z-score = 0.21) and relatively impaired performance in patients of a mixed phenotype (mean z-score = −0.76) with a significant difference of almost 1 standard deviation. Further analysis showed that patients with the mixed phenotype were more likely to have missing data on the TMT-B (Odds Ratio = 2.8; χ2(1) = 9.41, p = 0.002), which further indicates that the clustering process was sensitive to deficits in executive functioning.
Predictors of survival time: clinical measures, demographics, and neuropsychological clusters
To test for differences in survival time between neuropsychological clusters, Kaplan-Meier survival curves were computed, stratified by cluster-membership, and survival probabilities were compared using a log-rank-test. Then, a Cox regression model was used to determine the effect of clusters on survival time. Similarly, to determine the influence of clinical variables on survival time, additional Cox regression models were fitted. One model included baseline comorbidities and pre-existing diseases as predictors (see Table 1), and another included baseline medication (see Supplemental Table 2). Due to the high number of variables, predictors were selected in a stepwise manner (forward and backward) using the Akaike Information Criterion (AIC) in both models. Finally, an additional Cox regression model included annual rates of hospitalizations (somatic and psychiatric) as predictors of survival time. All Cox regression models were fitted with baseline MMSE score, age, education, and sex as covariates. E-values were calculated to determine how robust the observed association was to unmeasured confounding factors, i.e., factors that were not measured but could be associated with both the predictor of interest and survival. More specifically, e-values indicate how strongly an unmeasured factor would need to be associated with both the predictor and survival to fully explain the observed association. 31
Demographic and clinic characteristics of 202 patients diagnosed with Alzheimer's disease dementia at baseline.
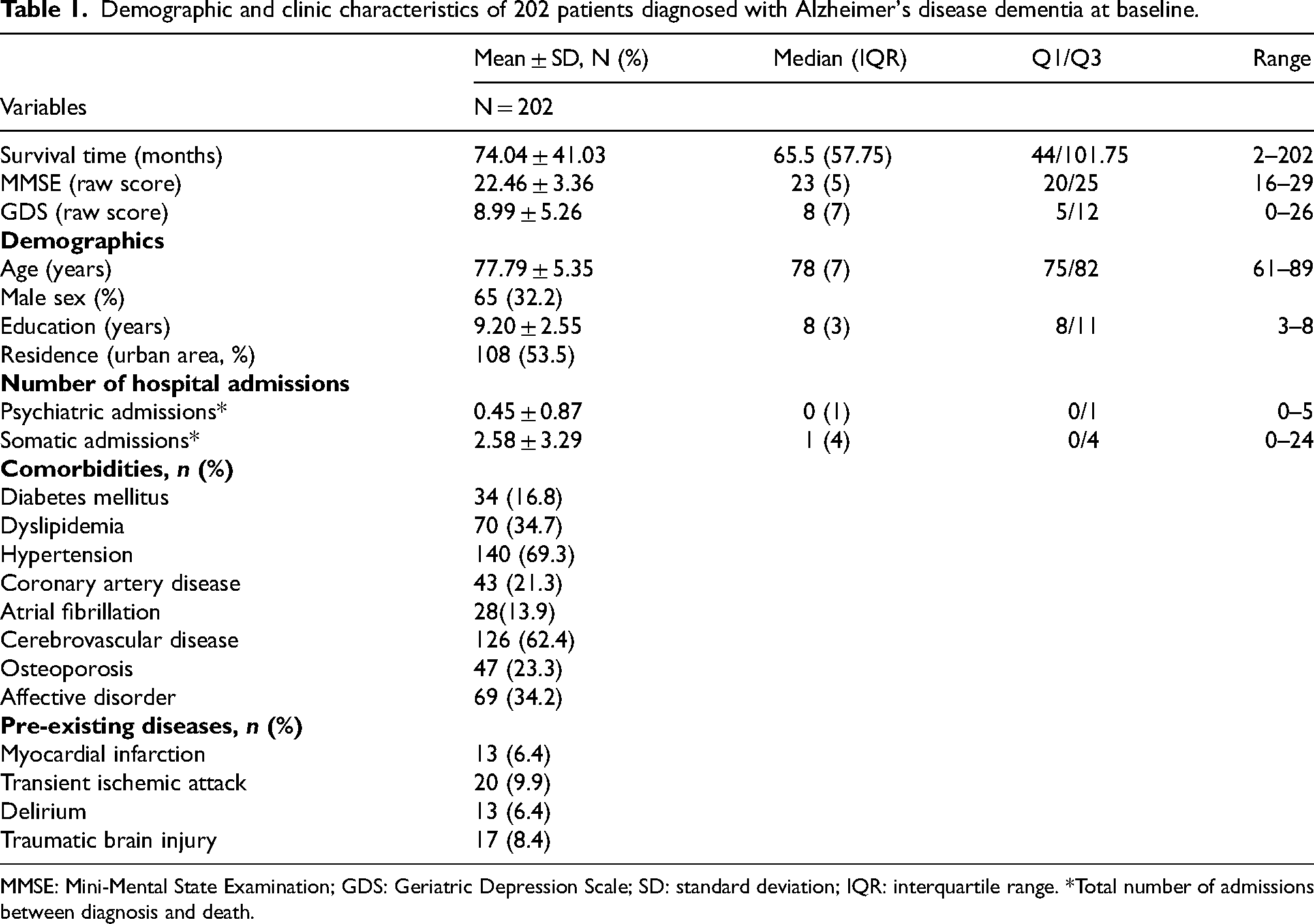
MMSE: Mini-Mental State Examination; GDS: Geriatric Depression Scale; SD: standard deviation; IQR: interquartile range. *Total number of admissions between diagnosis and death.
Proportional hazard (PH) assumption was tested for all four Cox regression models. We confirmed the proportional hazard assumption using Schoenfeld residuals (for details see Supplemental Figures 2-5).
Results
Patient characteristics
We analyzed data from 202 patients from the time of their initial mild-to-moderate ADD diagnosis at a specialized memory clinic until their death (baseline age 61 to 89 years). The study population included significantly more women than men (χ2 = 25.66, p < 0.001). At the time of ADD diagnosis, the most common comorbidities were hypertension and cerebrovascular disease (prevalence > 60%), followed by dyslipidemia and affective disorders (prevalence >30%). These comorbidities were equally distributed between the sexes. Consistent with this, the most common drug therapies were medications for treating cardiovascular and cerebrovascular diseases and antidepressants. Following the initial dementia assessment, 93% of patients were initiated on antidementive treatment (Supplemental Figure 1). The mean survival time after ADD diagnosis was 74.04 ± 41.03 months, ranging from two to 202 months. Detailed information on the demographic and clinical characteristics of ADD patients at the time of diagnosis is presented in Table 1.
Neuropsychological clusters
Complete data from all neuropsychological subtests could be collected from 169 of the 202 patients included in the study, and this data was used for cluster analysis. The results of the hierarchical cluster analysis by inspecting the dendrogram (Figure 1) indicated that a two-cluster solution (mixed phenotype and amnestic phenotype) was optimal. A comparison of the two clusters’ neuropsychological measures (Table 2) showed that patients in both clusters performed similarly poorly (z-score ≤1.5) on verbal and figural memory tests. Patients with deficits solely in the memory domain were assigned to the amnestic phenotype cluster. Those assigned to the mixed phenotype cluster also showed mild to moderate deficits (z-score ≤1) in non-memory domains, including visuo-construction, attention/processing speed, and object naming. Demographic variables (age, sex, and education) were comparable between clusters. Patients in the mixed phenotype cluster had significant lower baseline MMSE scores and survival times than those in the amnestic phenotype cluster. Logistic regression with leave-one-out cross-validation showed 90.53% accuracy in discriminating between clusters using the six neuropsychological variables. Based on their regression coefficients, constructional praxis (B = −2.75, SE = 0.567, p > 0.001) and TMT-A (B = −2.67, SE = 0.561, p > 0.001) had the greatest influence on differentiating between clusters, followed by phonemic fluency (B = −0.95, SE = 0.313, p = 0.002) and BNT scores (B = −0.76, SE = 0.277, p = 0.006). Word list delayed recall and constructional recall did not contribute significantly (p > 0.05). Comparing the mean survival of patients excluded (N = 33, mean survival = 65.06 months, SD = 39.39) and included (N = 169, mean survival = 75.90 months, SD = 41.81) in the clustering process showed no significant difference, t(47.20) = −1.43, p = 0.159.
Comparison of demographic and neuropsychological variables of the two cognitive phenotypes of patients with Alzheimer's disease dementia (n = 169).

MMSE: Mini-Mental State Examination. *z-scores adjusted for education, sex, and age provided by the Consortium to Establish a Registry for Alzheimer's Disease (CERAD-Plus) test battery are depicted.
Predictors of survival time: results of regression analysis
Influence of neuropsychological phenotype and demographics on survival time
According to a log-rank test (χ2(1) = 7.80, p < 0.01), survival times significantly differed between the two clusters (mixed versus amnestic phenotype), with notably lower survival probabilities for the mixed phenotype cluster, especially between 50 and 90 months after the initial ADD diagnosis. A Cox proportional hazards model (Table 3), which included baseline age, sex, education, and MMSE scores as covariates, identified the mixed phenotype cluster as a predictor of shorter survival time (HR = 1.45, 95% CI 1.055–1.998, p = 0.022). The E-value for this observed effect was 1.91 (lower CI E-value = 1.25). Additionally, the model showed that higher age at baseline predicted shorter survival time (HR = 1.04, 95% CI 1.01–1.07, p = 0.016), while a higher baseline MMSE score predicted longer survival time (HR = 0.92, 95% CI 0.87–0.97, p = 0.002). Survival curves stratified by cluster membership are presented in Figure 2.

Survival curves stratified by cluster membership in 169 patients with Alzheimer's disease dementia.
Multivariable Cox regression analysis using neuropsychological clusters and demographic data to predict survival time in 169 patients with Alzheimer's disease dementia.

MMSE: Mini-Mental State Examination.
Influence of neuropsychological phenotype, demographics, and clinical measures on survival time
The Cox regression model with stepwise selection of baseline comorbidities and pre-existing diseases identified comorbid atrial fibrillation and delirium prior to the initial diagnosis of dementia as significant predictors of shorter survival time. Corresponding E-values were 2.67 (lower CI E-value = 1.79) for atrial fibrillation and 3.78 (lower CI E-value = 2.25) for delirium. A history of myocardial infarction was also included in the model but it did not significantly contribute to the prognosis. Higher age at time of ADD diagnosis and lower MMSE scores were also significant predictors of shorter survival time. In this model, being male was associated with shorter survival (see Table 4).
Multivariable cox regression for the prediction of survival time in 202 patients with Alzheimer's disease dementia patients with baseline comorbidities and pre-existing diseases serving as predictors.

MMSE: Mini-Mental State Examination; SE: standard error; HR: hazard ratio; CI: confidence interval. The minimal model included age, education, sex, and MMSE. Selection criteria for model were the Akaike Information Criteria (AIC); forward and backward selection were applied.
A Cox regression model incorporating stepwise selection of baseline medications, demographics, and baseline MMSE scores revealed a modest influence of antiepileptic medication on prolonged survival time with a corresponding E-value of 2.7 (upper CI E-value = 1.26) Initiating antidementive treatment at the time of dementia diagnosis did not contribute to the model and was not selected for regression analysis.
Influence of annual hospitalizations and demographics on survival time
A multivariable Cox regression model fitted using data on annual hospitalizations revealed that patients with a higher rate of somatic and psychiatric annual hospitalizations had shorter survival times. The calculated E-value for the annual rate of somatic hospitalizations was 2.20 (lower CI E-value = 1.91) and 5.23 (lower CI E-value = 3.73) for psychiatric hospitalizations. Higher age and a lower MMSE score at the time of diagnosis also predicted shorter survival time (see Table 5).
Multivariable Cox regression to predict survival in 202 patients with Alzheimer's disease dementia based on the type of annual hospitalizations (psychiatric and somatic).

MMSE: Mini-Mental State Examination; SE: standard error; HR: hazard ratio; CI: confidence interval. *The number of annual hospitalizations was calculated by dividing the number of hospitalizations by survival time (years).
Discussion
This long-term, naturalistic follow-up study examined the factors that influence post-diagnostic survival in 202 patients who were initially diagnosed with mild-to-moderate ADD. Survival times ranged from a few months to nearly 16 years after the initial dementia diagnosis. Our results showed a significant association between shorter survival time and higher age, lower MMSE score at time of initial diagnosis, and male sex. However, although being male was associated with a shorter survival time, this effect was only significant when other comorbidities were present. The most significant predictor of shorter survival time was the annual rate of annual psychiatric hospitalizations following an initial dementia diagnosis, with a HR of 4.84. Despite the relatively low prevalence of delirium being diagnosed prior to the onset of dementia (6.4%), it was found to have the second highest negative impact on life expectancy among significant predictors, with a HR of 3.13. Because the E-value for delirium is relatively large (5.71), it is unlikely that its negative impact on life expectancy can be explained by unmeasured confounding factors. A detailed analysis of cognitive measures, including neuropsychological phenotypes, revealed that deficits in constructural praxis, psychomotor speed, and language-associated function, in addition to memory impairment, significantly contribute to reduced life expectancy in individuals diagnosed with ADD.
Influence of demographics on survival time
Regression analysis revealed significant associations between higher age, lower MMSE scores, and shorter survival times in all models that were additionally fitted with clinical or neuropsychological measures. Our results align with those of other studies reporting shorter survival times following dementia diagnosis at an older age and in more severe stages of dementia.5,21,32 While advanced age is widely recognized as a key non-modifiable risk factor for dementia, the age at which patients undergo their initial dementia assessment can be influenced. The median MMSE score of 23 (range 16–29) in our real-world sample indicates that the initial dementia assessment occurred several years after the first clinical symptoms appeared for most patients. This finding confirms previous results from our memory clinic showing that only a small percentage of patients are diagnosed with early-stage ADD at their initial assessment. 33 The late diagnosis in everyday clinical practice limits disease-specific survival analyses of such real-life data. This is because it leads to inhomogeneous study populations. It also causes delayed treatment as a bias. However, data on disease-modifying opportunities and progression markers, even in patients with late diagnoses, are scarce and therefore important in clinical practice. Our study found that male sex was associated with reduced survival time, corroborating previous findings.32,34 However, as mentioned above, this effect was only significant when other comorbidities were present. Since other studies found no sex differences in survival time, 35 we assume that the influence of sex on survival and disease progression in ADD is multifactorial. These factors may include sex differences in biological brain aging 36 and differences in the prevalence of comorbidities, such as cardiovascular disorders, between men and women. 37
Influence of the neuropsychological phenotype on survival time
Our findings show that the presence of cognitive impairment in multiple domains, in addition to the presence of memory impairment at the time of ADD diagnosis, predicts reduced survival time. Accordingly, we observed a lower MMSE scores in the mixed phenotype group, which can be used as a screening measure of multiple cognitive domains. Our results are partially consistent with those of Scheltens et al., who found higher mortality rates in ADD patients with a non-amnestic presentation. 20 However, their data were based on neuropsychological clustering of heterogeneous neuropsychological measures from multiple centers and are therefore not entirely comparable to the homogenous assessments used in our study. Our results are partly in contrast to those of Sood et al., who analyzed three cognitive profiles (marked visuo-spatial, verbal, and balanced visuo-spatial and verbal impairment) and found no association between cognitive profiles and survival time. 21 We hypothesize that deficits in multiple cognitive domains indicate more widespread neuropathology and decompensation of cognitive reserve. This assumption is supported by prior longitudinal data showing that cognitive reserve can modulate cognitive decline in AD. 38
Influence of clinical measures and comorbidities on survival time
We found that the most prevalent somatic comorbidities were cerebrovascular disease/hypertension and dyslipidemia, with prevalence rates of over 60% and 30%, respectively. However, atrial fibrillation and pre-existing delirium, with prevalence rates under 15%, were significant predictors of shorter survival times. Pre-existing delirium, though rare (6.4%), had the greatest negative impact on survival time. Consistent with previous findings that delirium is a risk factor and predictor of accelerated cognitive decline in patients with ADD,39,40 our results underscore the importance of preventing and monitoring delirium and cardiovascular disease in dementia care.
Influence of somatic and psychiatric annual hospitalizations on survival time
We found a low annual number of somatic and psychiatric hospitalizations in our study population. Although the study was conducted in only one of Austria's nine federal states, we collected patient data from all clinics in the area. Using a multivariate Cox regression model that included the annual rate of hospitalizations, demographics, and baseline MMSE scores, we found over fourfold increased hazard ratios for the annual rate of psychiatric hospitalizations compared to the hazard ratios for MMSE scores or age in predicting shorter survival times. Although the calculation of an annual hospitalization rate does not fully account for time-varying effects, this measure provides reliable information for clinical use. According to Armstrong et al. (2022) and Mendes et al. (2025), severe behavioral disorders associated with dementia increase the risk of mortality and are the main reason for admission to a psychiatric ward. Furthermore, an analysis of longitudinal data from the Prospective Dementia Registry Austria (PRODEM-Austria) study revealed that these disorders are associated with faster progression of dementia. 41 Therefore, preventing psychiatric hospitalizations due to exacerbated behavioral and psychiatric symptoms is an essential component of post-diagnostic support and dementia care.
Taken together, the results of this study suggest that a detailed analysis of neuropsychological profiles at the time of ADD diagnosis can serve as a prognostic marker for the progression of the disease. Additionally, preventing unnecessary hospital admissions, particularly to the psychiatric ward, could positively impact the survival of patients with ADD. However, our results cannot be generalized due to our single-center design and small study population from a high-income Western European region.
Limitations and strength
This study has several limitations. The inclusion criteria comprised the time of ADD diagnosis, but not the onset of the first symptoms, which limited the observation period to the time that patients spent within the healthcare system. Furthermore, patients diagnosed at an advanced stage were excluded because valid neuropsychological assessments are no longer possible at this stage, which limits the generalizability of this study. The baseline prescribed medications were included as predictors in the survival analysis. However, due to the naturalistic study design, ensuring continuous intake was not possible. The low prevalence of certain pre-diagnoses likely reduced the ability to detect the effect of, e.g., myocardial infarction on reduced survival alongside delirium and atrial fibrillation within a single model. This is indicated by an increased hazard ratio despite a p-value greater than 0.05. An external validation of the clustering result by means of an independent study population would have been valuable, despite the clustering methods chosen being well-suited for small sample sizes, but it was not applicable. Since this study was conducted at a single center, its generalizability to other populations may be limited. Furthermore, the exact causes of death were unavailable and could not be included in the analysis. Although our statistical model for analyzing the influence of annual hospitalizations on mortality is not optimal for accounting for time-varying effects, this approach seemed most suitable and clinically useful. At least, the exclusion of 33 patients from the cognitive cluster analysis due to missing data could be a selection bias.
Despite these limitations, the long follow-up times (up to 16 years) enabled us to predict long-term survival in ADD patients, a significant strength of our study. Other strengths include detailed neuropsychological examinations and medical history information (e.g., previous illnesses and number of hospitalizations per year from diagnosis until death) for all ADD patients included in the study.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261468789 - Supplemental material for Multidomain cognitive impairment, along with comorbidities and psychiatric hospitalizations, shorten survival time of patients with Alzheimer's disease dementia: A long term, naturalistic follow-up study
Supplemental material, sj-docx-1-alz-10.1177_13872877261468789 for Multidomain cognitive impairment, along with comorbidities and psychiatric hospitalizations, shorten survival time of patients with Alzheimer's disease dementia: A long term, naturalistic follow-up study by Burak Doganyigit, Timo Schurr, Alex Hofer, Simone Schütz and Michaela Defrancesco in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
This retrospective study was approved by the Ethics Committee of the Medical University of Innsbruck, Austria (approval number 1102/2024).
Consent to participate
As the study was retrospective, patients were exempt from signing an informed consent form.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Austrian Alzheimer's Association and the Dr Johannes und Hertha Tuba-Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data set associated with the paper can be requested as anonymized version form the correspondence author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.