
Abstract
Aim: The comprehensive cardiac rehabilitation (CR) programme after myocardial infarction (MI) improves quality of life and results in reduced cardiac mortality and recurrence of MI. Hospitals worldwide face problems with low participation rates in rehabilitation programmes. Inequality in recruitment and participation among low educated and socially vulnerable patients must be addressed to lower inequality in post-MI health. Our aim was to improve referral, attendance, and adherence rates among socially vulnerable patients by systematic screening and by offering a socially differentiated cardiac rehabilitation programme. Methods: From 1 September 2002 to 31 December 2005, 388 first-incidence MI patients ≤75 years were hospitalised. Register check for newly hospitalised MI patients, screening interview, and systematic referral were conducted by a project nurse. Patients were referred to a standard rehabilitation programme (SRP). If patients were identified as socially vulnerable, they were offered an extended version of the rehabilitation programme (ERP). Excluded patients were offered home visits by a cardiac nurse. Concordance principles were used in the individualised programme elements. Adherence was registered until the 1-year follow up. Results: 86% were referred to the CR. A large share of elderly patients and women were excluded. The attendance and adherence rates were 80% and 71%, respectively among all hospitalised patients. Among referred patients, the attendance rate was 93%. Patients were equally distributed to the SRP and the ERP. No inequality was found in attendance and adherence among referred patients.
Keywords
Background
For Western societies, it has been documented that social class, years of education, and occupational status determine level of risk of myocardial infarction (MI) and cardiac death. Inequality in cardiac health has increased during the last three decades [1]. Blue-collar workers, singles, socially isolated people, and people experiencing life stress and depression are experiencing a higher risk of MI or cardiac death [2–5]. Recurrence of MI is higher and the relative risk for death up to 7 years from infarction for patients with less than a high school education is 1.47 [6]. For decades, first-incidence single MI patients with low social support have been pointed out as vulnerable to poor prognosis or cardiac death [7]. Today, singles have a 2-fold risk of experiencing acute coronary syndrome [8].
Comprehensive cardiac rehabilitation (CR) includes exercise training, behavioural changes, education, and psychological support. The aim of a CR programme after MI is to aid patients to function as normal as possible when they return to their daily lives and interactions with the community. CR is well documented in reducing the risk of recurrent MI and mortality [9,10]. A meta-analysis of psycho-educational programmes for low educated and socially vulnerable patients suggested that the programmes yielded a 35% reduction in cardiac mortality and a 29% reduction in recurrence of MI [11].
It is a challenge to recruit and motivate all eligible patients to participate and adhere to a full CR. Participation rates range from 21% in a study among elderly patients to 86% in other studies. Most studies report participation rates between 25 and 55% [12]. Several studies report that participants are more likely to be younger men with low comorbidity [12–17]. Systematic screening for MI and bedside interview were implemented at the Department of Internal Medicine and Cardiology, Aarhus Sygehus by year 2000. Compared to other CR programmes, a high attendance rate of 71.2% was achieved [18] until 2002. Systematic screening among all MI patients was not in use in Denmark until then.
Non-attenders are more likely to live alone, to have a low socioeconomic status, and to have atypical symptoms at admission [18]. Reducing social inequality in rehabilitation is stressed [19]. The findings clarify the importance of reducing inequality in referral, attendance, and adherence to the CR.
A review of referral and adherence predictors for the CR showed positive predictors to be the physician’s endorsement and attitude towards effectiveness of the CR, an ease of physical access and transportation, a high level of self-efficacy, great social support, and a high education level [20].
If the CR attendance and adherence rate among socially vulnerable patients can be improved, this might affect the prognosis after MI. Thus, screening tools to detect the socially vulnerable patients are important to develop and there is a need to develop the CR programmes that meet the needs of socially vulnerable patients.
Aim
To achieve more equality, the first goal is a higher referral rate to CR by the hospital staff. Second goal is a higher attendance rate for the initial part of the CR programme and a better adherence throughout the programme by the patients. The first aim of this study was to provide screening tools to detect and improve referral of socially vulnerable patients. The second aim was to evaluate actual attendance and adherence by the patients to socially differentiated CR.
The project was a feasibility study and the programme elements were adjusted simultaneously.
Methods
A socially differentiated CR was offered to all eligible first-incidence MI patients aged ≤75 year admitted at Aarhus Sygehus University Hospital from September 2002 to December 2005.
The first part of the intervention was to establish a systematic screening procedure to guide the referral procedures at the organisational level. The hospital register was checked for new hospitalised MI patients on a daily basis using the MI criteria from 2000 [21]. Referral to CR through a screening interview was carried out preferably on the third day of hospitalisation. Register check, screening interview, and referral were managed by a project nurse. Thus, staff was facilitated in referral and motivated to inform the project nurse on request. She was responsible for systematically gathering information on diagnosis, patient condition, and inclusion and exclusion criteria for each patient before carrying out the screening interview.
Systematic tracing of patients whom it had not been possible to contact during hospitalisation and screening for socially vulnerability was added during the present study (April 2002).
The project nurse was responsible for contacting patients not present at the department, i.e. patients initially hospitalised outside the catchment area or patients referred to surgical treatment at other hospitals.
Exclusion criteria were severe comorbidities (e.g. terminal cancer), severe apoplexy, dementia, severe psychiatric disease, mental retardation, and alcohol or drug addiction (Figure 1). Patients suffering from anxiety or moderate to mild depression were not excluded from the study. Excluded patients and patients rejecting participation in the CR were followed up by phone, and if relevant offered home visits by a nurse experienced in cardiology. There were no control groups in the study. Neither vulnerable nor non-vulnerable persons were left out of the screening intervention.
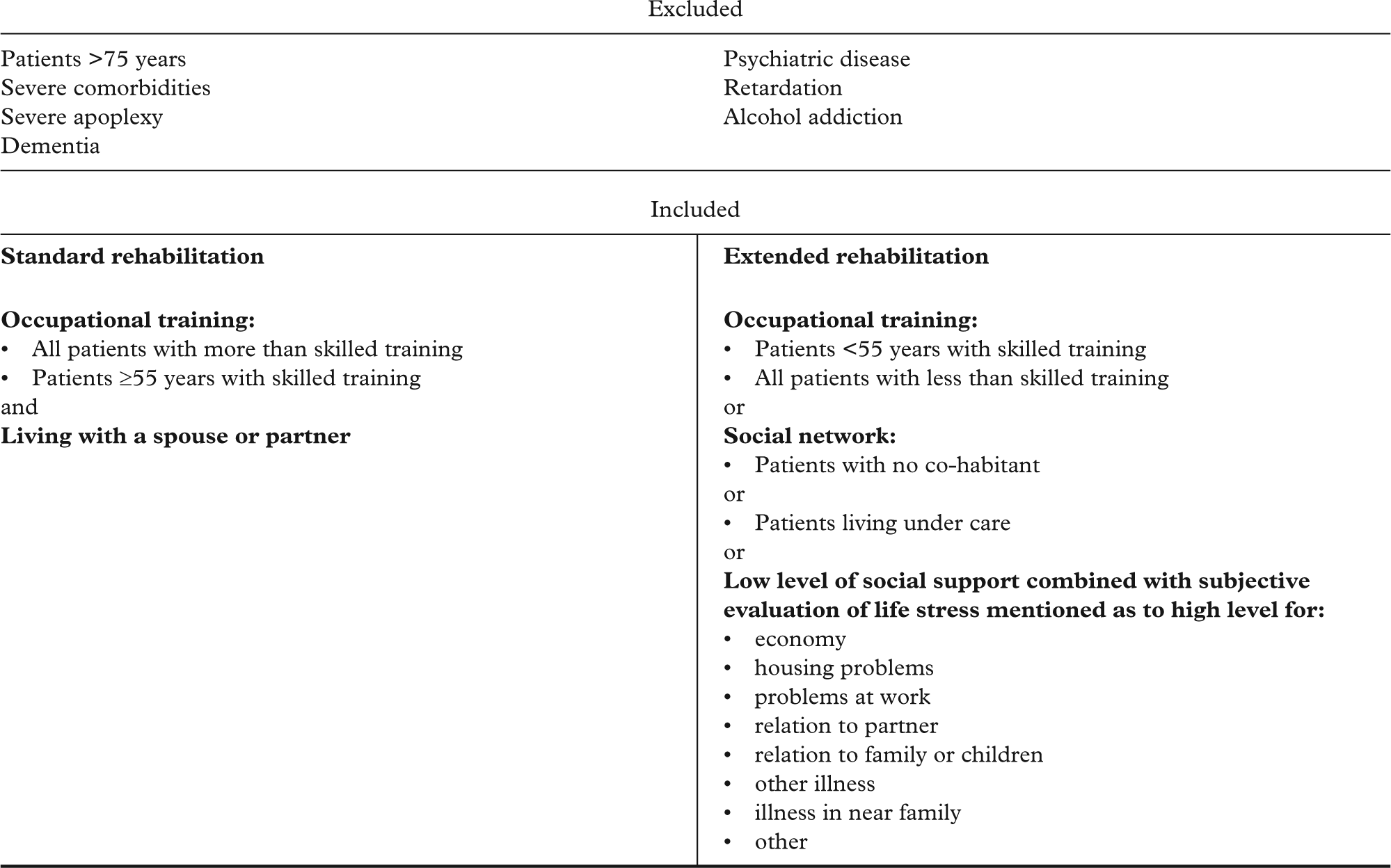
Inclusion criteria in socially differentiated rehabilitation programme at Aarhus Sygehus University Hospital, Denmark.
Second part of the intervention was randomised recruitment to either the standard rehabilitation programme (SRP) or the extended rehabilitation programme (ERP). The project nurse referred to the 6 or 8 weeks of socially differentiated CR. All well-educated patients, according to the Danish Educational Nomenclature (DUN) classification 5–8 Statistics Denmark, and their partner were invited to the SRP. The ERP was offered to the socially vulnerable patients and their partner or other relative. The socially vulnerable patients were identified by a low education level according to DUN classification 1–4, single living, or experiencing high level of life stress combined with the lack of a social network [22]. Married patients aged ≥55 were recruited to the SRP if they had skilled training according to DUN classification level 4.
Patients were encouraged to participate by the medical staff, who communicated the CR as a part of the treatment for MI, and the staff initiated medical, social, and behavioural advice at the coronary care unit. The date for the first appointment at the rehabilitation unit was set within 2 weeks after discharge. The medical check up with the cardiologist was linked tightly to other parts of the CR.
SRP consisted of individually based visits during 6 weeks, leaving patients out of the SRP before the end of their sick leave 8 weeks from hospitalisation:
medical examination three times: workload test, medical treatment, BP measure, and if necessary X-ray of heart and lungs
nurse consultation four times: hospitalisation, physiology in MI, guidance in medicine, body signals, physical condition, psychological condition, and lifestyle
dietician consultation twice: diet anamnesis and follow up
physical training two times a week during 4 weeks: physical training was offered in groups
1-year follow up: medical examination by cardiologist, BP measure, cholesterol and fasting glucose measures, and nurse consultation.
All patients were screened for depression and anxiety symptoms during the project period. If the screening indicated depression, patients were advised to consult their GP for diagnosis and eventually treatment.
The ERP consisted in addition to the SRP of:
extra individual nurse-led consultation: the patient defined a plan for his/her third rehabilitation phase
the patient plan being sent to the GP in order for him/her to take over third rehabilitation period: half an hour was advised for a prevention consultation with the GP after ended ERP
2 months from end of the ERP (4 months from discharge) the nurse conducted a follow up on patient plans by phone
action-oriented and skills-training elements in diet, exercise, relaxation, and smoking cessation for up to 1.5 years after hospital admission, at the Counselling Centre of the Danish Heart Foundation
for retired patients, non-cardiac-specific activities at the community local centres.
Patient-oriented communication methods consistent with motivational interviewing were used by the nurses [23]. Patients were encouraged to define goals and motivate action routes from concordance principles rather than compliance principles. Interpretation was offered to patients who did not speak Danish.
Attendance and adherence was registered by a nurse-administered questionnaire throughout the CR.
Patients recruited for the study signed informed consent. Ethical considerations were submitted to the Ethical Committee, Aarhus County, Denmark.
Statistical analysis
Data were entered twice in SPSS Data-entry. Analyses were conducted in SPSS11 and STATA10. The statistical analysis included Pearson’s chi-squared test or Fisher’s Exact test for the 2×2 tables. We applied p<0.05 as the general level of significance.
Results
Of 388 first-incidence MI patients, 333 (86%) were referred to the CR and 55 (14%) were excluded due to comorbidity. A total of 16 (4%) patients did not give informed consent. These patients were offered the SRP and no 1-year follow up.
There were 155 (40%) patients attending the SRP and 154 (40%) patients attending the ERP. Only six (1.5%) patients declined participation in rehabilitation and 12 (3%) accepted, but did not attend, hereof three in the group that was offered the ERP. The risk of non-attendance was identified among patients with severe comorbidity like stroke and severe three-vessels coronary heart disease. Six patients were rehabilitated at other hospitals. Attendance rate for the CR was 80% of all patients and among eligible patients the attendance rate was 93%. No patients were lost in the follow-up process.
Adherence was evaluated from physician- and nurse-conducted consultations defined as four or more meetings out of four to six. Not all patients participated in dietician consultations and physical training through the CR (Figure 2). A total of 276 adhered to the CR at 1-year follow up. Of patients giving informed consent adherence was 91% to a full CR due to adherence criteria, but 97% participated in the 1-year follow up and medical examination.
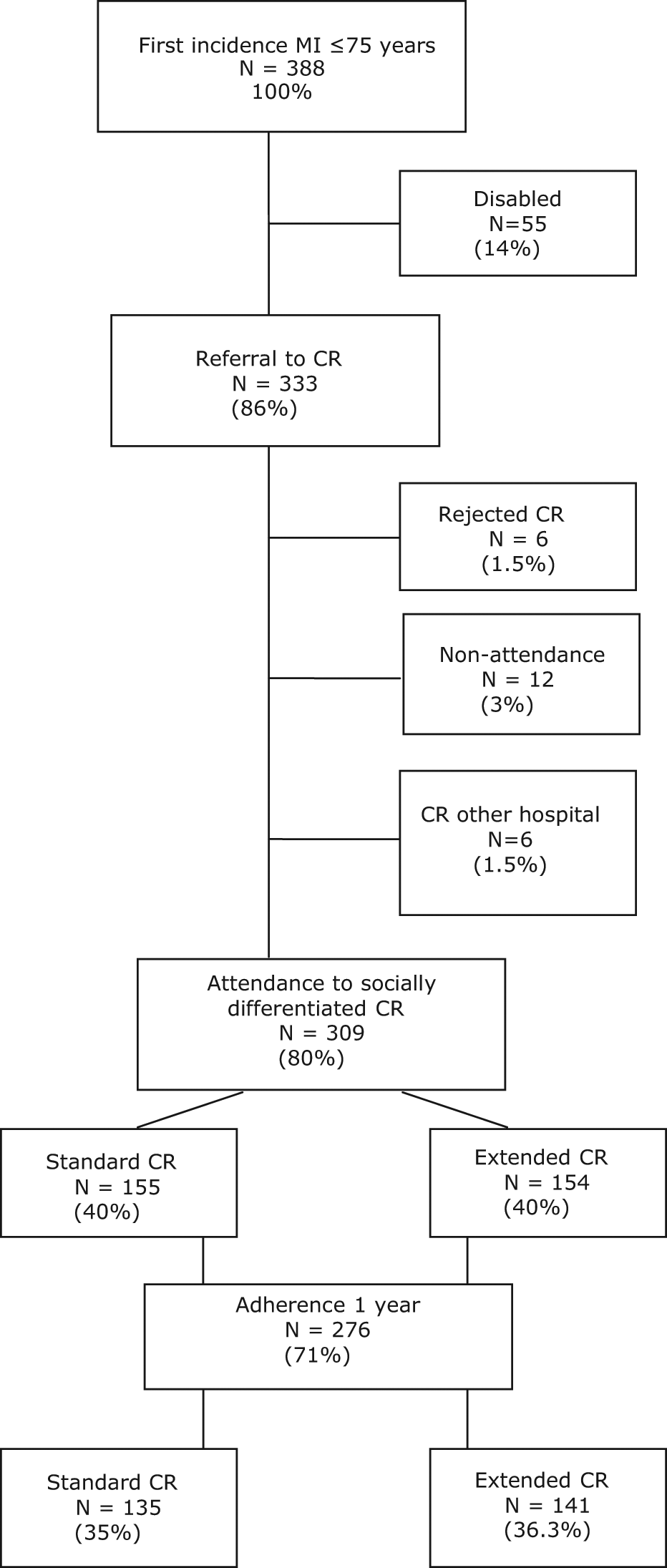
Referral and attendance for socially differentiated cardiac rehabilitation programme at Aarhus University Hospital, among first-incidence MI patients ≤75 years.
The age for hospitalised patients in the study group was (mean±SD) 60.4±10.1 years and 71% were male. Mean age for patients referred to the CR was 59.3 years. Excluded patients were more likely to have comorbidities, be female, and of older age compared with referred patients (Table I).
Socio-demographic variables among incident MI patients ≤75 years.
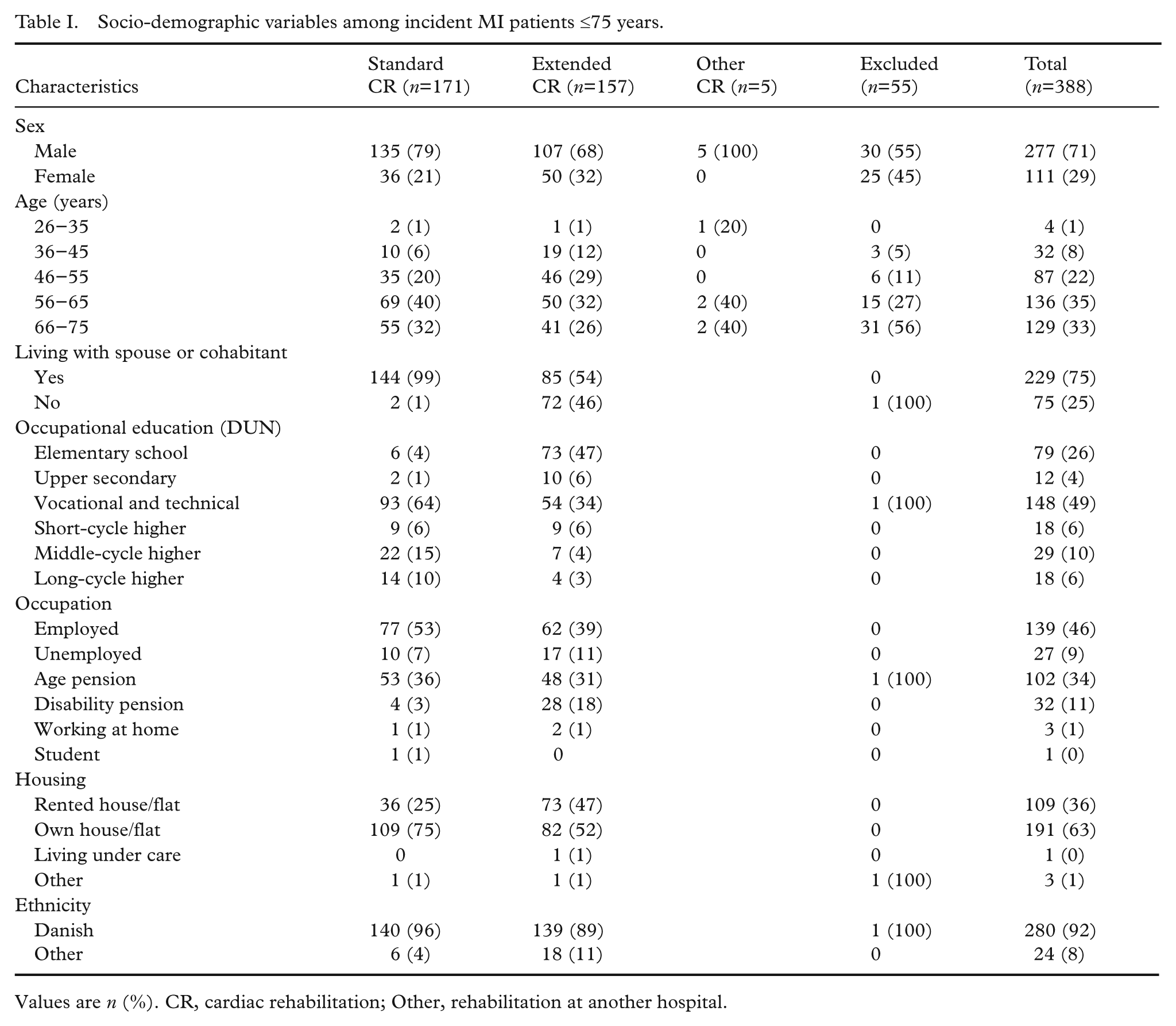
Values are n (%). CR, cardiac rehabilitation; Other, rehabilitation at another hospital.
Among all patients referred to the CR, 75% were living with a spouse or cohabitant, 30% had no education or less than skilled occupational training, and 46% were employed.
Patients referred to the ERP compared to those referred to the SRP were more likely to:
be women (32% vs. 21%)
receive disability pension (18% vs. 3%)
be out of the labour market (60% vs. 46%)
live in rented house/flat (47% vs. 25%)
be of other ethnicity than Danish (11% vs. 4%).
Due to referral criteria, patients in the ERP as compared to those in the SRP tended to:
live alone (46% vs. 1%)
be of lower education (53% had less than 12 years of public school and occupational training vs. 5%)
be younger (additional 15% of the patients aged ≤55 years would have been referred to ERP if a no age-limit was set for skilled workers).
In Table II, it is shown that 222 patients did not meet the criteria for the ERP and were either excluded or referred to the SRP. A total of 16 patients did not give informed consent and could thus not fill in the questionnaire and be referred to either of the rehabilitation groups. These patients were all offered the SRP and no 1-year follow up. A total of 166 patients fulfilled one or more of the criteria for the ERP.
Incident myocardial infarction patients fulfilling criteria for extended rehabilitation.
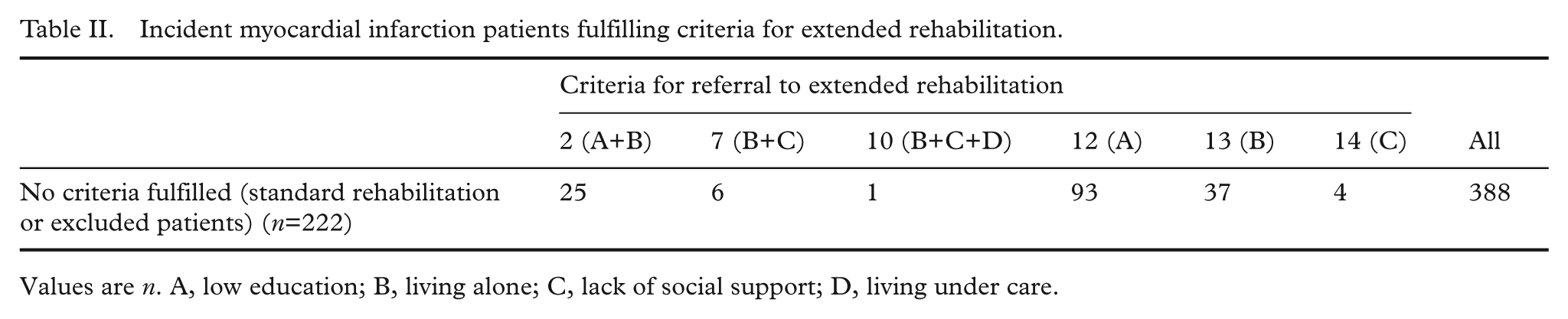
Values are n. A, low education; B, living alone; C, lack of social support; D, living under care.
Altogether, 17 patients were misclassified in the rehabilitation programme. A total of 13 patients meeting the criteria for the ERP due to low education (10 patients), living alone (two patients), or lack of social support (one patient) were not referred to the ERP. They attended the standard rehabilitation programme. Four patients, who did not meet any of the criteria for the ERP, were nevertheless admitted to participate in the extended programme.
Discussion
A high participation rate and adherence to the CR is crucial if we want to reduce cardiac mortality and re-infarction among socially vulnerable patients. The rates for referral (86%) and attendance (80%) to the CR among all hospitalised incident MI-patients seem high when compared to the literature.
Attendants for the CR are cited to be men, younger, and to have low comorbidities. This tendency is also found in this study. Males represent 71% of all hospitalised incident MI-patients ≤75 year. Among excluded patients, women represent 45%. Women are approximately 10 years older when they have their first MI, and high age leads to more comorbidity and other reasons for exclusion. It seems that if women are offered the CR, they participate at the same level as male participants. Women do not seem prone to stay at home, even if they have extra responsibilities towards their family or sick relatives. There were no differences in attendance rate according to gender, age, educational level, or ethnicity among patients referred to the CR. Dismissal rate (1.5%) and non-attendance rate (3%) were very low, although higher among patients offered the SRP. Most were due to comorbidities or death. It seemed possible to eliminate unequal referral, attendance, and adherence due to social circumstances, gender, educational level, and social vulnerability. Systematic screening and referral, a positive attitude towards the CR, and motivation of all patients to participate were practiced as a natural part of the treatment. This indicates that unequal referral and attendance seem to be linked to staff, organisation, and programme principles rather than being only patient determined.
A study was conducted at Aarhus Sygehus University Hospital among the same group of patients 2 years prior to the present study. In this study, patients were likewise recruited to the CR through bedside interviews, though only to the SRP. The attendance rate (calculated among all admitted patients) was 70% for patients <70 years old having an incident MI compared to 85% in this study [18]. Systematic tracing of patients who had not been contactable during hospitalisation and screening for socially vulnerability in addition to systematic checking the hospital register for new hospitalised MI patients increase the referral rate. Aarhus Sygehus University Hospital has a long tradition of offering the CR to patients after MI. For at least 15 years, the SRP has met the criteria as recommended recently by the European Association of Cardiovascular Prevention and Rehabilitation [24]. Thus, referral for the CR is part of the standard treatment. We did not find studies with a similar methodological approach. Since the referral and attendance rates were high when introducing the new elements of screening, there might be a ceiling effect. A higher effect can be achieved in other hospital settings.
Among consenting patients, 22% lived alone. A total of 46% of patients referred to the ERP lived alone. More patients than expected when taking the literature into consideration were in need of the ERP. Socially vulnerable patients can be categorised into three groups. The first and relatively small group consisted of marginalised patients who suffered from addictions or psychiatric diagnoses, who received transfer incomes, or who lived on the street. A second group of socially vulnerable patients were unemployed or at risk of losing their job, had lost their social status or social network, and would potentially run into conflicts. A third large group of patients had strong social ties, were employed, but had a low educational level, lived alone, and perhaps had manageable comorbidities. The screening tool used in this study may include too many patients from the latter group. Up to 70% of the patients would have been included if skilled training (DUN 4) would qualify a patient for ERP. Elderly patients showed a less troublesome management of their illness than younger patients. In this study, single-living, well-educated patients were referred to the ERP, while the SRP was offered to patients with skilled training classified at DUN 4, age ≥55 years, and a marital status of living with spouse or partner. This allocated 50% of the patients to each group. When analysing results from this study, it will be evident whether this is still too wide a group to consider at risk.
Recruitment procedures for the socially differentiated rehabilitation programme enrolled the relevant and targeted patient categories. Educational level and cohabitation as criteria for inclusion into the ERP also caught a higher proportion of women, patients not on the labour market, patients on early retirement, patients of other ethnicities than Danish, and patients living in flats indicating scarce economical resources.
A socially differentiating approach by offering the SRP and the ERP seem to lead to a high adherence rate (91%). Cardiologist-led follow up seems to be central to adherence. At the 1-year follow up including medical examination, 97% of the referred patients attended, although not all of them had adhered to a full CR.
The CR was individually adapted to meet specific patient needs. This proved to be advantageous. There was no waiting time for gathering enough patients and each programme was completed within 8 weeks from discharge. This is important, especially among patients with jobs, as many patients do not want to follow the CR if they are back to work after a sick-leave period of 8 weeks. Because of the individual and family-oriented approach, patients felt their specific needs met during the CR. The patients were offered group sessions at the Counselling Centre of the Danish Heart Foundation in Aarhus after the hospital-based CR programme. However, few patients chose to participate.
During the screening procedures, DUN classification proved a little difficult to use and most were misclassified due to education; thus 17 patients (5%) were misclassified to either the SRP (13 patients) or the ERP (four patients). It was also a source to misclassification that patients lived with their adult children, but not with a spouse or partner. This potential error should be incorporated in future studies. In this study, the fact that some patients have been misclassified is a source of bias, but a positive one if effects of social differentiation are found, since more patients in the SRP ought to have had the ERP. Age distribution is also a source of bias. Mean age is higher in the SRP.
Implementation of socially differentiated rehabilitation among 200 MI patients a year would cost the salary of a full-time nurse (35 hours a week) once the programme is developed and the staff is trained. The perspective is higher quality of life and a lower rate of recurrent MI and cardiac deaths [9–11].
This study is not randomised and biases have to be taken into consideration. When comparing to a historical control group, there might have been changes in other procedures at the department affecting referral and attendance. Attitudes among staff and patients can have changed over time and days of hospitalisation have been lowered which might have lead to a higher need of consultations after discharge from hospital. We are not able to conclude on causality of motivational staff, motivation of patients, an individual approach, social differentiation, and high attendance in the study, but the attendance rate for CR can and must be improved, especially among socially vulnerable patients.
Low referral, attendance, and adherence rates among vulnerable groups are a challenge to health promotion in both the hospital and community settings. A systematic screening and perhaps proactive approach in combination with a socially differentiated programme can be a key to engage more citizens at risk of preventable diseases in health-promotion activities. Further research in transferability of the method ought to be carried out.
Conclusion
CR has been proven in earlier studies to improve the medical prognosis of MI patients. The current study suggests that social inequality in referral, admittance, and adherence to the CR can be dealt with by systematic referral and a socially differentiated individualised approach.
A systematic screening procedure can help find all eligible patients and support the staff to refer all of them to the relevant programme. It is possible to develop and use a simple screening tool to form patient groups for socially differentiated CR. Out of all patients admitted with incident MI, 86% were referred to the CR and 80% attended the programme. Thus, the fraction of patients adhering to the offered MI aftercare was higher than expected from the literature and from earlier studies in the same setting.
It is possible to equally address low and highly educated patients, males and females, and Danish and patients of another ethnicities to attend the CR in the acute ward.
It is possible to train rehabilitation staff to use concordance-principles, motivational interviewing, and other patient-oriented methods.
It is possible to motivate low-educated and socially vulnerable patients to adhere to an individually and socially differentiated CR.
Footnotes
Acknowledgements
The authors give a special thank you to Aarhus Rehab-group: Birgitte Gustafson, Dorrit G Andersen, Karen Lind (Department of Cardiology, Aarhus Sygehus University Hospital) Mads Melgaard Madsen (Department of Social Medicine and Psychiatry, Municipality of Aarhus), Jørgen Lous and Bo Christensen (Department of General Practice, University of Aarhus), Elisabeth Egeskov (Counselling Centre of the Danish Heart Foundation in Aarhus), and Kirsten Vinther-Jensen (Health Promotion and Prevention, Centre of Public Health, Central Denmark Region).
The study was supported by the Ministry of the Interior and Health, the Ministry of Social Affairs in Denmark (grant number 2003-14004-4), the Danish Heart Foundation (grant number 04-10-B99-A150-22175), and the Aarhus University Hospital Research Initiative.
None.