
Abstract
Aims: Adolescence is considered a critical phase for smoking initiation, while smoking initiation in adulthood has received less attention. In the present study, we investigated smoking initiation in early adulthood, with an additional focus on how socioeconomic status (SES) relates to late-onset smoking. Methods: The Norwegian Longitudinal Health Behaviour Study followed a representative sample of adolescents (n=530) from age 13 (7th grade) to age 30 (years 1990–2007) through 9 waves of data collection. Information was collected on the adolescents’ gender, smoking, alcohol use, cannabis use, physical activity, and SES. Those reporting to be smokers at age 30, but not at age 18, were defined as “late-onset smokers”. Results: At age 30, 21% were daily smokers, of which 45% met our definition of late-onset smoking. Participants with a low SES had a higher odds ratio for late-onset smoking (OR=3.42) and a lower odds ratio for quitting smoking (OR=0.40) after adjusting for confounders.
Background
Over the last decades, smoking prevalence has declined in many developed countries [1,2], although this trend now seems to have slowed. One commonly suggested explanation for the latter is that the tobacco industry has increased its focus on adult smokers, combined with a delay in the development of preventive efforts directed towards this group [3,4].
A common assumption has been that smoking initiation, in essence, occurs during adolescence [1,3], and a crude description of anti-tobacco interventions is measures to prevent smoking initiation among adolescents and promoting cessation among adults [1]. Smoking initiation in adulthood is described much less frequently and considered a neglected research issue [5], both concerning the understanding of the phenomenon and the development and testing of programmes to counter it [3].
Some studies suggest that a proportion of those who smoke as adults actually established the habit as adults [1,3]. Important factors for adolescent smoking initiation, like peer smoking [6], siblings’ smoking [7], parents’ smoking [7], as well as predictors for quitting [8], have been transferred to subjects of interest in studies regarding adult smoking onset [9]. Beyond this, the role of mental illness in association with adult smoking initiation has been investigated both by using clinical samples [5] and cohort studies [10]. There have also been efforts to study whether adult smoking initiation co-occurs with a broader change in health behaviours, such as the use of alcohol and cannabis as well as reduced physical activity [11–13]. In another study, those who started smoking as adults were backtracked using longitudinal data; in their adolescence, such individuals were less likely to have had friends or parents who smoked, compared to their smoking adolescent counterparts [14]. In sum, there seems to be other important predictors for smoking initiation in adulthood [15], and it seems reasonable to assume that also adolescent non-smokers, and not only adolescent experimenters, are at risk for smoking initiation as adults [16].
In adult populations, the association between current smoking and socioeconomic status (SES) is well documented [17,18]. Smokers with a high SES are more likely to quit smoking [19] and more frequently report future health concerns as a reason for quitting [20] than do their lower-SES counterparts. One study found that the choice of school type, with bearing for later socioeconomic status, was strongly associated with smoking among 16–20 year olds [21]. A recent review concluded that adolescent smoking is more likely if parents have a low SES, although the findings are mixed [22]. It is possible that the stronger SES-smoking association in adults may in part be caused by a social gradient in late-onset smoking.
Aims
The main aim of this study was to investigate late-onset smoking and to what degree early adulthood could be considered as an additional critical phase for smoking initiation and development. A secondary aim was to investigate the role of SES in late-onset smoking and smoking cessation in young adulthood.
Methods
We used data from the 9-waves study entitled the Norwegian Longitudinal Health Behaviour Study (NLHB), which followed a representative sample of a cohort of adolescents from age 13 (7th grade) to age 30 (years 1990–2007). Initially, 924 pupils (55% boys) and parents gave written informed consent, and the study was approved by the Norwegian Data Inspectorate. Detailed information on data collection has been published elsewhere [23]. We defined wave 5, at age 18, as the demarcation between adolescence and adulthood and waves 6–9 (age 19–30) as adulthood. The attrition analysis (data not shown) showed that adolescent smokers and males had higher dropout rates than non-smokers and females. Only participants who answered the smoking question in 2007 were included in this study (n=530).
Variables
Smoking was measured by the following item in all 9 waves, “How often do you smoke?” (every day, every week, less than once a week, not at all), a wording similar to other studies [12]. This ordered categorical variable on smoking frequency was used to construct a dichotomous variable on smoking: those smoking every day vs. all others. The dichotomous variable “Adolescent smoker” was defined as smoking daily at age 18, based solely on wave 5. “Adult smoker” was defined as being a daily smoker solely at wave 9, at age 30. “Late-onset smoker” was defined as being an adult smoker, but not an adolescent smoker. “Quitter” was defined as being an adolescent smoker, but not an adult smoker. “Adolescent trier” was based on participants with valid answers on three or more of the first 5 waves (ages 13–18) and defined as those who tried smoking at least once.
Gender was reported at the first wave. In the last wave, at age 30, the participants were asked about their highest achieved level of education, which we used as a measurement of SES. “Elementary and secondary school (9 years)”, “1–2 years of upper secondary education”, and “3 years of upper secondary education” were coded “low”. “Less than 4 years of college/university” and “Other” were coded “mid”, while “4 years or more at college/university” was coded “high”.
The use of cannabis was measured by one item at age 18, “Have you ever used hashish?” (yes coded 1, no coded 0), and one item at age 30, “How often do you use hashish (cannabis) or other illegal drugs?” (every day, every week, and more seldom than once a week coded 1, never coded 0). Those confirming at age 30 but not at age 18 were defined as “Late-onset cannabis users”. Those confirming at age 18 but not at age 30 were defined as “Cannabis quitters”. Alcohol use was measured using the same two items at age 18 and 30. The first, measured drunkenness: “How many times have you felt drunk over the past 6 months?” Those reporting “never” were coded 0, while all others were coded 1. The second measured alcohol consumption, “How many drinks do you enjoy when drinking alcohol?” Those reporting consumption over the gender-specific 80th percentile were coded as “high consumption”. “Late-onset drinking” was defined as not having been drunk in adolescence but only as an adult. “Alcohol quitter” was defined as having been drunk during adolescence but not in adulthood.
Physical activity was measured with the same items at age 18 and 30, “Leisure time physical activity: how often do you get sweaty/out of breath?”. “Every day” and “4–6 times per week” were coded as “high”, “2–3 times per week” and “once a week” were coded as “mid”, and “1–3 times per month”, “less than 1 time per month”, and “never” (only used at age 30) were coded “low”. The wording were similar to other studies on physical activity and smoking [12], and the scale has been used in previous studies on this dataset [24]. “Increase in physical activity” was defined as an increase on the physical activity scale from age 18 to 30, while “decrease in physical activity” was defined as a decrease on the same scale from age 18 to 30.
Statistical analysis
Analyses were done using Stata/IC 11.1 for Windows. First, we examined the distribution of key variables in groups defined by adult smoking, late-onset smoking, and quitting smoking. We tested for differences using χ2 tests. Second, we examined associations between SES and late-onset smoking using logistic regression analysis. We then adjusted for gender, late-onset cannabis use, late-onset drinking, and decrease in physical activity. Third, we examined associations between SES and quitting smoking using logistic regression analysis and also adjusted for gender, quitting drinking, cannabis use, and increased physical activity. Fourth, among the late-onset smokers at age 30, we investigated the numbers of smoking initiators per year between age 18 and 30 by comparing the observed smoking initiation with a linear model to see if late-onset smoking was most likely soon after age 18. Finally, to see if attrition was associated with the key variables, we examined if participating in 2007 was associated with the participants’ own smoking, parents’ education, parents’ job status, and gender, as reported in previous waves.
Results
Of the 530 included in this study, over 20% (n=110, 21%) (Table I) were daily smokers at age 30. There were no significant association between being an adolescent smoker and attrition in adulthood (data not shown) and no significant gender differences in smoking at age 30 (χ2=1.60, p=0.21). There was a strong association between smoking and SES; 35% of the low-SES group were daily smokers, compared to 18% of the mid-SES group and 10% of the high-SES group (χ2=33.91, p<0.05) (Table I). Smoking was not associated with having been drunk (χ2=1.38, p=0.24) or alcohol consumption (χ2=1.82, p=0.18). There was a positive association between smoking and use of cannabis and other illegal drugs (χ2=24.95, p<0.05) and a negative association between physical activity and smoking: 30% of the low-activity group was smokers, compared with 17% of the mid-activity group and 8% of the high-activity group (χ2=18.23, p<0.05).
The distribution on key variables of smoking, at adulthood (2007).

Differences were tested by Chi-squared tests.
p<0.05.
Figure 1 portrays the cumulative rates for first-time daily smoking towards age 30, which shows that about one-third of smokers at age 30 started after age 18. Of all daily smokers at age 30, nearly half were not daily smokers at age 18 (n=50, 45%) and met our definition of late-onset smoking (Table I). Of those reporting not being daily smokers at 18, 10% did, however, report at least having tried smoking at some stage prior to age 18; 68% of late-onset smokers and 55% of participants not defined as late-onset smokers had tried smoking in adolescence (χ2=2.94, p=0.086). There was no significant difference between the observed smoking initiation between age 18 and 30 and the postulated linear development (r=0.95, p< 0.05), indicating a similar risk for smoking initiation across all measurements between age 18 and 30. Late-onset smoking was more common among men (χ2=11.53, p<0.05) and there was a significant association between late-onset smoking and SES (χ2=18.36, p<0.05); 24% of the low-SES group, 9% of the mid, and 7% of the high-SES group were late-onset smokers (Table I). Those reporting having been drunk (χ2=1.62, p=0.20) and high alcohol consumption (χ2=1.11, p=0.29) were not associated with late-onset smoking, whereas the use of cannabis or other illegal drugs was (χ2=14.94, p<0.05). A post-hoc analysis showed a significant association between late-onset cannabis and late-onset smoking (χ2=7.28, p<0.05). There was a significant association between physical activity at age 30 and late-onset smoking; 18% of the low-activity group was late-onset smokers, compared to 10% of the mid-activity group and 5% of the high-activity group (χ2=7.30, p<0.05).
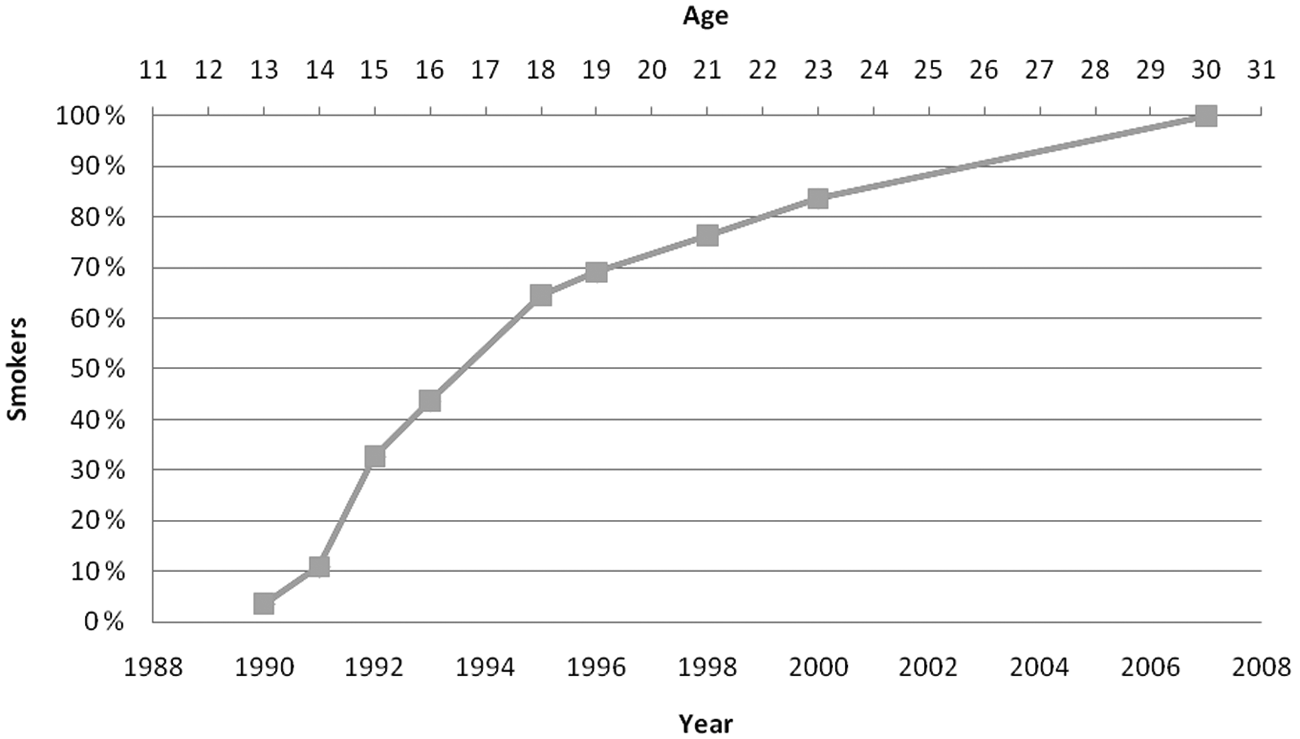
Accumulation of daily smoking at each wave for daily smokers at age 30.
In direct comparisons between early and late-onset smokers, there were more males among late-onset smokers (χ2=8.58, p<0.05). SES (χ2=1.46, p=0.48), drunkenness (χ2=0.37, p=0.54), alcohol consumption (χ2=0.04, p=0.85), the use of cannabis or other illegal drugs (χ2=0.00, p=1.00), and physical activity at age 30 (χ2=0.49, p=0.78) was not associated with being an early- or late-onset smoker (Table I).
Of the participants, 16% were quitters (n=73), which implied having reported daily smoking at age 18 but not at age 30. Quitting was not associated with gender (χ2=0.27, p=0.60) (Table I), although quitters had a higher SES (Table I) (χ2=8.34, p<0.05). Neither drunkenness (χ2=0.53, p=0.47) nor alcohol consumption (χ2=0.00, p=0.98) was associated with quitting smoking. There was a significant association between quitting and the use of other illegal drugs (χ2=3.91, p<0.05). A post-hoc analysis showed a strong association between quitting smoking and quitting cannabis (χ2=40.53, p<0.05). There was also a significant association between physical activity at age 30 and quitting smoking; 44% of the low-activity group was quitters, compared to 61% of the mid-activity group and 80% of the high-activity group (χ2=6.22, p<0.05).
Participants with low SES had a higher odds ratio for late-onset smoking (OR=3.42, 95% CI 1.9–6.3) than did the other SES groups (Table II), which remained significant after adjusting for gender, decrease in physical activity, late-onset cannabis use, and late-onset drinking (OR=3.74, 95% CI 1.7–8.1). Participants with low SES had a lower odds ratio for quitting smoking (OR=0.40, 95% CI 0.2–0.8), which remained after adjusting for gender, increase in physical activity, quitting cannabis use, and quitting drinking (OR=0.36, 95% CI 0.2–0.8) (Table II).
Late-onset smoking and quitting by socioeconomic status.
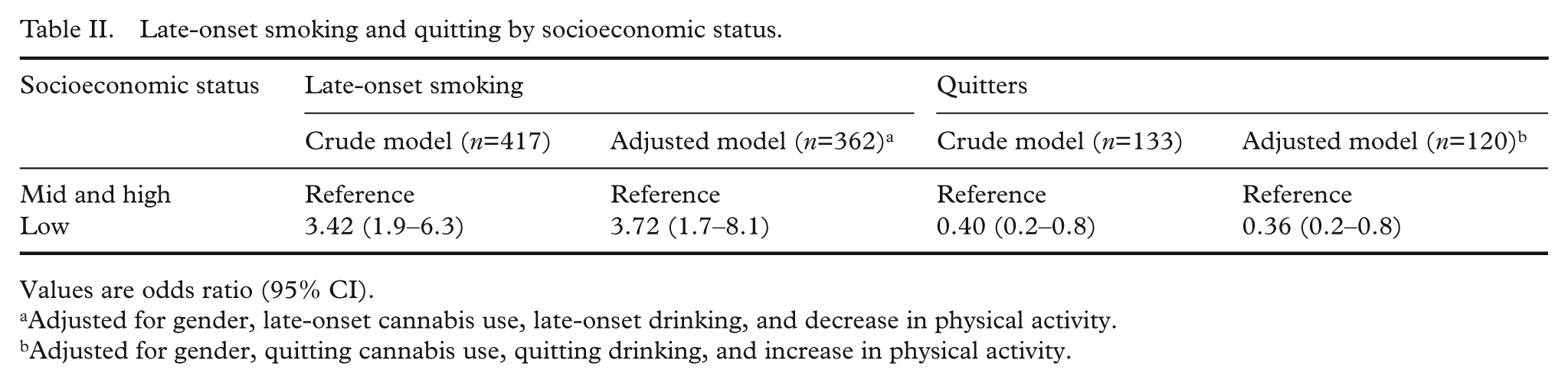
Values are odds ratio (95% CI).
Adjusted for gender, late-onset cannabis use, late-onset drinking, and decrease in physical activity.
Adjusted for gender, quitting cannabis use, quitting drinking, and increase in physical activity.
Discussion
Over 40% of the daily smokers at age 30 could be considered late-onset daily smokers, which indicates that early adulthood is a critical phase for daily smoking initiation. One-third of adult smokers did not report smoking at any stage between 13 and 18 years of age, while adolescent smokers were not more likely to drop out of the study. There was a clear and consistent association between SES and late-onset smoking, which was maintained even after adjusting for confounders. There was also a significant association between quitting smoking and SES, indicating that both late-onset and quitting are relevant factors explaining the clear SES-smoking association in the general adult population.
The greatest strength of this study was the follow up over 17 years with repeated measurements of individuals. The study was also based on a representative, non-clinical sample, as opposed to many previous studies of adult smoking. Another strength was the SES measure of achieved education, in contrast to plans for education or parents’ education used in previous studies. The main limitations were that this study was based solely on the participants who answered the smoking question in the last wave. Of the nearly thousand participants, only 530 were included, giving an overall response rate of 50% over 17 years. This may affect the results, as drop out may be associated with late-onset smoking, quitting, or related predictors. However, the attrition analysis showed no increased drop out among adolescent smokers. Men had higher attrition than women, which may have further affected gender differences. Another limitation was the difference in measurement regarding cannabis use between age 18 and 30, where the item at age 30 included other illegal drugs.
There was no gender difference in adult smoking. However, late-onset smoking was more common among males. This pattern was present both in comparisons of late-onset and non-smokers, as well as in late-onset and early-onset smokers. There were no gender differences in quitting smoking. These findings indicate a stronger increase in smoking among males in early adulthood, where males catch up with the higher smoking rates among females in adolescence.
A large study from Finland concluded that smoking in adolescence predicts SES as adults [25]. It is likely that the mechanisms behind educational attainment, like perceived control over outcome [26,27], also explain the link between SES and an elevated risk of late-onset smoking and lower chance of quitting smoking. We found a clear association between late-onset smoking and SES, and also between SES and quitting, which would both contribute to associations between smoking and SES among adults [28]. Previous studies have shown that intentions of smoking cessation are less strongly associated with SES than smoking and smoking cessation [29]. The lack of a social gradient in intention to quit, but a social gradient in smoking cessation indicates that other explanations than the intention to quit is necessary to explain the observed social gradient in smoking cessation. One possible explanation is that low-SES adults started smoking earlier and have more low-SES friends and therefore are more heavily exposed to smoking and social acceptance of smoking. Another possible explanation is that high-SES adults have more knowledge about smoking cessation, higher self-efficacy, and more resources and therefore have a higher success rate in quitting.
As expected, there was a strong and significant association between the use of cannabis and other illegal drug use and all smoking variables. Further, the post-hoc analysis showed an association between late-onset cannabis and late-onset smoking and also between quitting smoking and quitting cannabis. It is therefore reasonable to assume that there was a reciprocal relationship between changes in smoking and cannabis use between age 18 and 30. These associations may be interpreted as both a result of the standard gateway mechanism [30], meaning that smoking leads to cannabis use, or as a result of a reverse gateway mechanism [30] where smoking follows from cannabis use. Studies with higher temporal resolution may yield more information regarding the causality of these associations. Most likely, the association is related to more profound changes in health behaviour that were not accounted for in these analyses.
The findings that 45% of smokers at age 30 are late-onset smokers and the social gradient in both late-onset smoking and cessation suggest that late adolescence and early adulthood are important periods for smoking prevention and not only smoking cessation. Some who initiate smoking in early adulthood may be experimenters who increase their smoking frequency as adults. However, a large proportion of the late-onset smokers did not report smoking at all at any of the data collections prior to age 18. This suggests that the late-onset smoking should not be written off as a delayed behavioural pattern that in reality was established in adolescence. Even if that should be the case, the finding that late-onset smokers constitute a large group, characterised by low SES, highlights the importance of finding an arena for interventions. The social gradient found in late-onset smoking, combined with the reversed social gradient found in quitting smoking, may be key elements in shaping the strong social gradient of adult smoking.
Smoking prevention programmes have largely focused on adolescents, which can easily be reached through schools. Finding a similarly broad arena for interventions focusing on early adulthood could be more difficult, but focusing solely on educational institutions can exclude important groups. Young adults’ workplaces may be challenging, but still more suitable, arenas. Further, the focus may also be enhanced by including the cluster of smoking, drug use, and lack of physical activity. An increased emphasis on late-onset smoking may improve tobacco control, not as a replacement of the traditional strong foci on adolescent initiation and adult cessation [1], but to expand the range of actions.
Footnotes
Acknowledgements
The Norwegian Longitudinal Health Behaviour Study was initiated and conducted by the Department of Health Promotion and Development, Faculty of Psychology, University of Bergen. The founder of the study was Professor Knut-Inge Klepp. The study is currently coordinated by Professor Bente Wold.
Funding
This work was supported by the Research Council of Norway (Grant no. 190443).