
Abstract
Aims: The main aim of this paper was to investigate whether ethnic heath inequalities exist in self-rated health and risk-taking behaviours (smoking, drunkenness, use of cannabis) between ethnic majority (Estonian, Latvian, Lithuanian) and minority (Russian) population groups of school-aged children in three Baltic countries. Methods: Investigation was carried out in the framework of Health Behaviour in School-aged Children (HBSC) study. Randomly selected students aged 11, 13, and 15 years answered questionnaires in the classroom in 2006. In total, 14,354 questionnaire forms were selected for analysis. Results: Russian boys were more likely (p<0.05) to evaluate their self-rated health positively in schools with Russian teaching language. Odd ratios for current smoking and drunkenness were significantly lower among Russian boys in the schools with Russian language of instruction (p<0.05) in comparison with the reference group. Russian girls did not differ significantly (the exceptions were smoking in Estonia and cannabis use in Latvia) from the majority population girls by self-rated health as well as by the risk of smoking, drunkenness, and use of cannabis.
Keywords
Background
Health inequalities and especially the socioeconomic determinants of mortality and morbidity have been analysed extensively in many countries during the last decades and these research issues continue to be in focus [1–3]. However, significantly less attention is paid by researchers to investigation of such health predictors as migration, ethnicity, or religion. Also, relatively few studies have analysed the ethnic disparities in risk-taking behaviour or self-perceived health in youth [4].
Socioeconomic status (i.e. income, occupation, and education) does not explain the whole range of health and health-behaviour variations in Europe. The findings indicate that ethnicity, migration status, and integration into local community are also important factors in terms of health among adult populations. The above-mentioned determinants could be really important, especially in the countries with a high proportion of migrants or with a substantial ethnical minority population. Very few studies have compared self-perceived health and risk-taking behaviour in children between migrant or minority populations and the native population. In addition, EU countries have a relatively weak database for collecting information and assessing health for migrant and ethnic minority populations [5,6]. To a large extent it could be explained by lack of agreement on the definition and collection of data on the ethnic minorities.
The Health Behaviour in School-aged Children (HBSC) study, which is based on nationality rather than ethnicity, has provided data on behavioural health indicators (smoking, alcohol and drug use, bullying at school, self-perceived health, and life satisfaction). The data on international comparison within the study showed that despite of some regional health-related behaviour differences in school-aged children, these children populations in many variables are similar and very close to the European statistical average [7]. Such a feature of national aggregation of similarities have been observed and widely commented by many researchers also in other European regions and countries [8].
There is a lack of studies comparing health in different types of schools for students of minority and majority populations. However, the parallel educational systems in the teaching languages of the majorities (Estonian, Latvian, Lithuanian) and also in Russian in the Baltic countries still coexist. This has allowed us to include and analyse the teaching language as a school-related factor that is hypothetically associated with health.
The aim of our study was to analyse whether inequalities exist in self-rated health and risk-taking behaviour (smoking, drunkenness, use of cannabis) between ethnic majority (Estonian, Latvian, Lithuanian) and minority (Russian) population groups in school-aged children of three Baltic countries – Estonia, Latvia, and Lithuania. We were also interested to find out whether there are any differences in self-rated health or risk-taking behaviour between students in schools with schooling language of the majority and students in schools with Russian as teaching language.
Materials and methods
Study population and survey procedures
The research was carried out in the framework of the World Health Organization collaborative HBSC study. The questionnaire survey was conducted among the national representative samples of 11-, 13-, and 15-year-old children during March and April 2006 in three Baltic countries – Estonia, Latvia, and Lithuania. A cluster sampling design was applied. School and class were used as the sampling units. The samples were drawn to be representative by age, gender, place of residence (urban and rural), and teaching language at school in each of the countries. The recommended sample size for each of the three age groups was approximately 1500 students.
The quality of data collection (sampling, development of survey instrument, conducting questionnaire survey, data collection and management) was ensured by following the standardised international HBSC research protocol within each country [9]. Survey permissions were approved by the Ministries of Education as well as by national or regional bioethics committees. Pre-trained personnel administered the completion of questionnaires in classrooms. Completed questionnaires were collected in individually sealed envelopes. Participation was voluntary, ensuring confidentiality and anonymity. Each country followed legal and ethical requirements for this type of survey.
After completion of the fieldwork, the data from each country was checked, recorded into files, and submitted to the HBSC International Data Bank at the University of Bergen, Norway. In total, 14,354 questionnaire forms selected by quality criteria of the international HBSC database (4477 in Estonia, 4245 in Latvia, and 5632 in Lithuania) were used for the final analysis. The number of collected questionnaires constituted over 80% of the whole selected sample.
Questionnaire and variables
Two independent variables were used in our analysis: (1) language reported spoken in the family by the respondent; and (2) language of instruction at school. According to the first criterion, all respondents were attributed to the dominating ethnicity in the country (Estonian, Latvian, and Lithuanian) or to the minority population (Russian). We also applied such independent variables as gender and age group in our analysis.
A set of health and health-behaviour indicators was used as dependent variables. Students were asked to rate their health as “excellent”, “good”, “fair”, or “poor”. In further analysis responses were dichotomised into “excellent or good” and “fair or poor”. The last category was used in the final analysis.
Substance use such as tobacco smoking, alcohol (for all age groups), and cannabis use (only for 15-year-olds) was also covered by the questionnaire. Current smoking was assessed by the question “How often do you smoke tobacco at present?” Possible four response categories were “everyday”, “at least once a week, but not every day”, “less than once a week”, and “I do not smoke”. The first three response categories were grouped into one category and used as criterion of current smoking. Self-reports on drunkenness were obtained by asking “Have you ever had so much alcohol that you were really drunk?” The response categories “no, never”, “yes, once”, “yes, 2–3 times”, and “yes, 4 or more times” were offered to choose for the respondents. We applied in our analysis only responses “yes, 2–3 times” and “yes, 4 or more times” as the indicator of drunkenness and excessive alcohol consumption. For measuring the cannabis use, the question “Have you ever taken cannabis in your life?” was presented. The response categories were “never”, “1–2 times”, “3–5 times”, “6–9 times”, 10–19 times:, 20–39 times”, and “40 or more times”). The responses of students who reported the experience of cannabis use at least once in their life were included into analysis of lifetime cannabis use.
In our statistical analysis, the respondents were divided into four groups, which were defined by ethnicity and instructional language at school.
Statistical analysis
For individual variation analysis, we used Statistical Package for the Social Sciences version 15.0 (SPSS, Chicago, IL, USA) [10]. Z and χ2 tests were applied for evaluation of statistical hypotheses on difference in distribution of variables between groups of respondents. Odds ratios (OR) were standardised by age. For that purpose, the Mantel–Haenszel test for estimating odds ratio estimates was used. Only results with a significance level of at least p<0.05 (two-tailed) were reported.
Results
Table I presents the distribution of respondents into four groups, selected by the language used in the family and in the school setting. Russian students formed quite a significant proportion of the sample populations in Estonia and Latvia and a lower proportion in Lithuania. Group 4 did not occur numerously and was, therefore, excluded from the final analysis. The students from group 1 were used in the following statistics as a reference group.
Distribution of 11-, 13-, and 15-year-old respondents by the language spoken in family and the language of instruction at school in the Baltic countries.
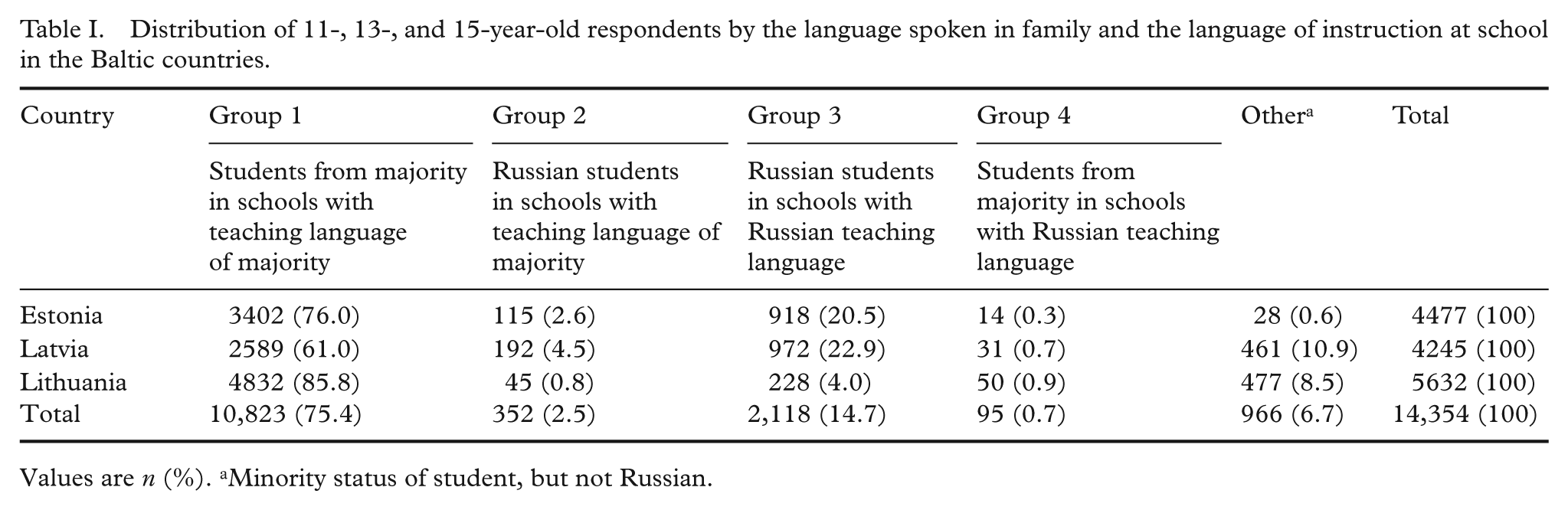
Values are n (%). aMinority status of student, but not Russian.
Self-rated health
The prevalence and OR of “fair or poor” self-rated health in language and gender groups are presented in Table II. Russian boy students in schools with Russian language of instruction (group 3) had lower OR of self-rated “fair or poor” health in comparison with reference group 1 in Estonia (OR 0.58, 95% CI 0.40–0.84, p<0.05) and Latvia (OR 0.63, 95% CI 0.45–0.88, p<0.01). However, the opposite results were observed for Russian girls in schools with Russian as teaching language in Lithuania: the OR of “fair or poor” health was higher (OR 1.74, 95% CI 1.13–2.71, p<0.05) compared to Lithuanian girls in the Lithuanian language schools (group 1).
Self-rated health as fair or poor for 11–15-year-old students by gender, country, and group of respondents defined by the language spoken in family and the language of instruction at school.
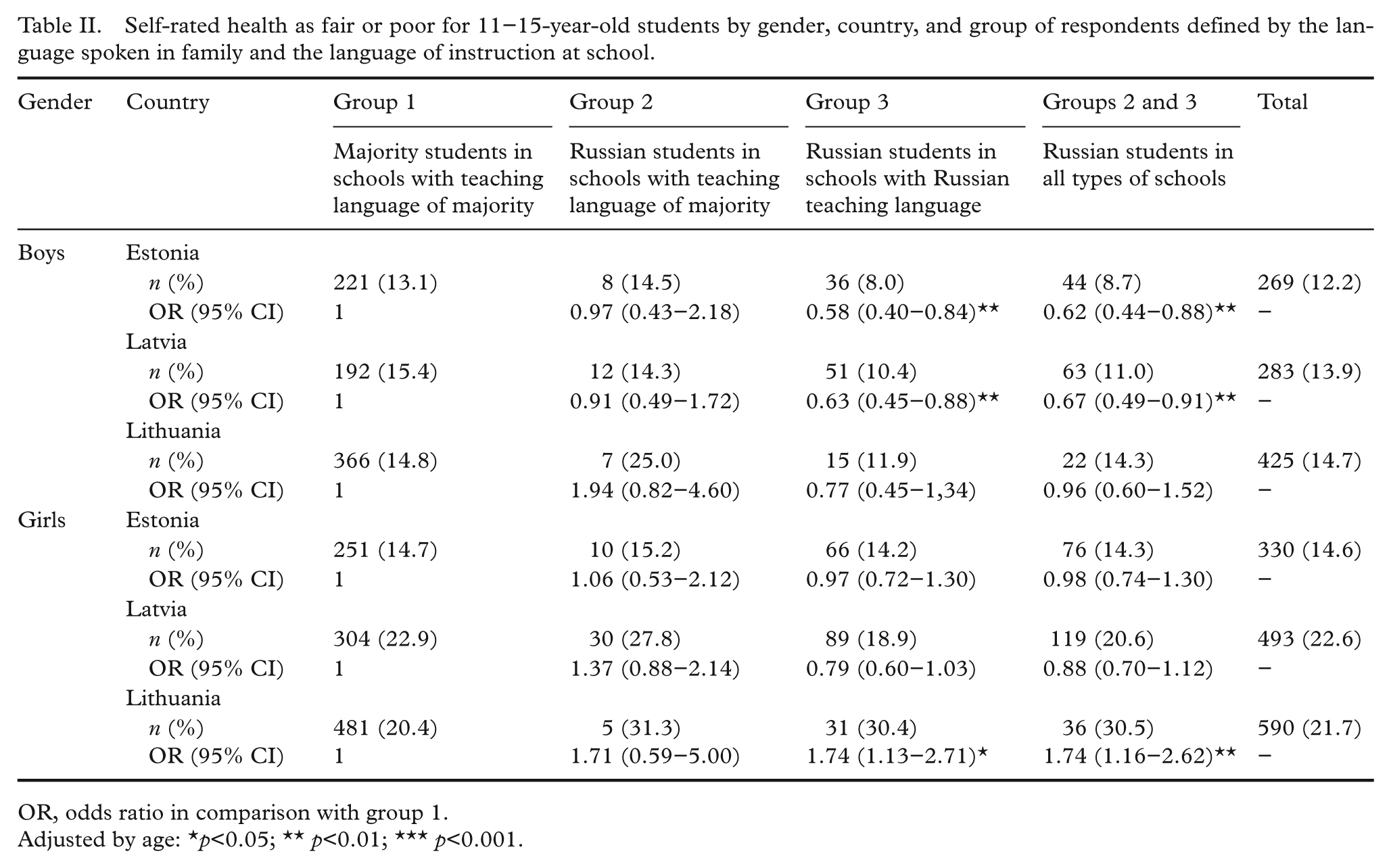
OR, odds ratio in comparison with group 1.
Adjusted by age: *p<0.05; ** p<0.01; *** p<0.001.
We have also compared OR of “fair and poor” self-rated health in merged groups 2 and 3 with the reference group 1. Data analysis showed similar results as for the comparative analysis of group 3 vs. group 1.
Risk-taking behaviours
The estimated OR of current smoking (Table III) was significantly lower in Russian boys who were enrolled in schools with Russian as language of instruction in Estonia (OR 0.72, 95% CI 0.54–0.98) and Lithuania (OR 0.44, 95% CI 0.23–0.81). The opposite was found (OR 1.84, 1.37–2.47, p<0.001) among Russian girls from group 3 in Estonia.
Self-reported current smoking for 11–15-year-old students by gender, country, and group of respondents defined by the language spoken in family and the language of instruction at school.
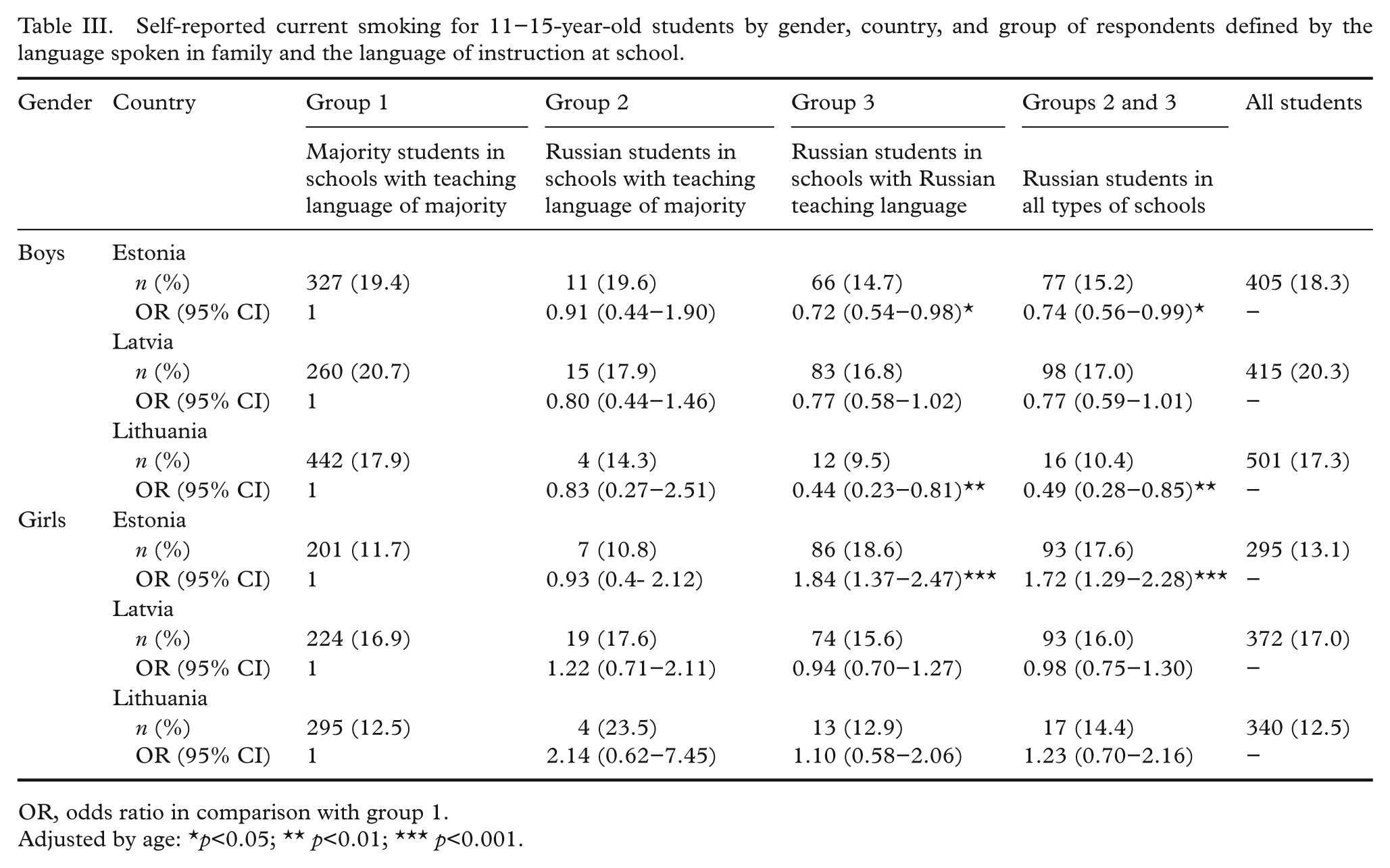
OR, odds ratio in comparison with group 1.
Adjusted by age: *p<0.05; ** p<0.01; *** p<0.001.
In all the countries, the OR of drunkenness was lower in the Russian boys who were enrolled in schools with Russian language of instruction (Table IV). Drunkenness (self-reported as “have been drunk at least twice in my life”) was less prevalent (OR 0.69, 95% CI 0.53–0.90, OR 0.74, 95% CI 0.57–0.97, and OR 0.56, 95% CI 0.34–0.91, in Estonia, Latvia, and Lithuania, respectively, p<0.05) among the Russian boys who were enrolled in schools with Russian language of instruction. Girls of minority and majority populations did not demonstrate disparities in drunkenness behaviour.
Drunkeness at least twice in lifetime for 11–15-year-old students by gender, country, and group of respondents defined by the language spoken in family and the language of instruction at school.
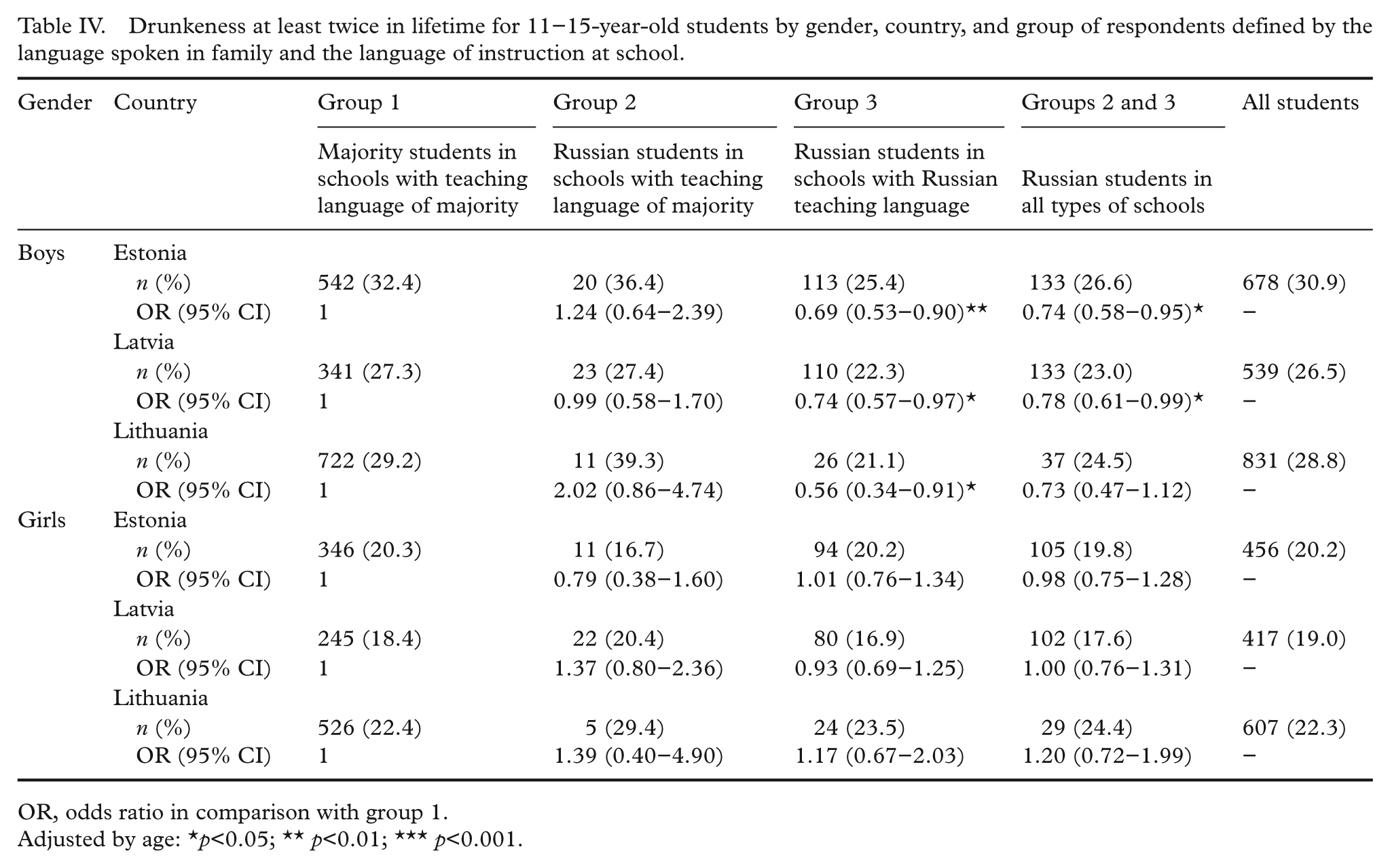
OR, odds ratio in comparison with group 1.
Adjusted by age: *p<0.05; ** p<0.01; *** p<0.001.
Russian girls who were enrolled in schools with Russian language of instruction in Latvia (OR 1.95, 95% CI 1.20–3.17, p<0.01) had higher OR of cannabis use (Table V).
Ever use of cannabis in lifetime for 15-year-old students by gender, country, and group of respondents defined by the language spoken in family and the language of instruction at school.
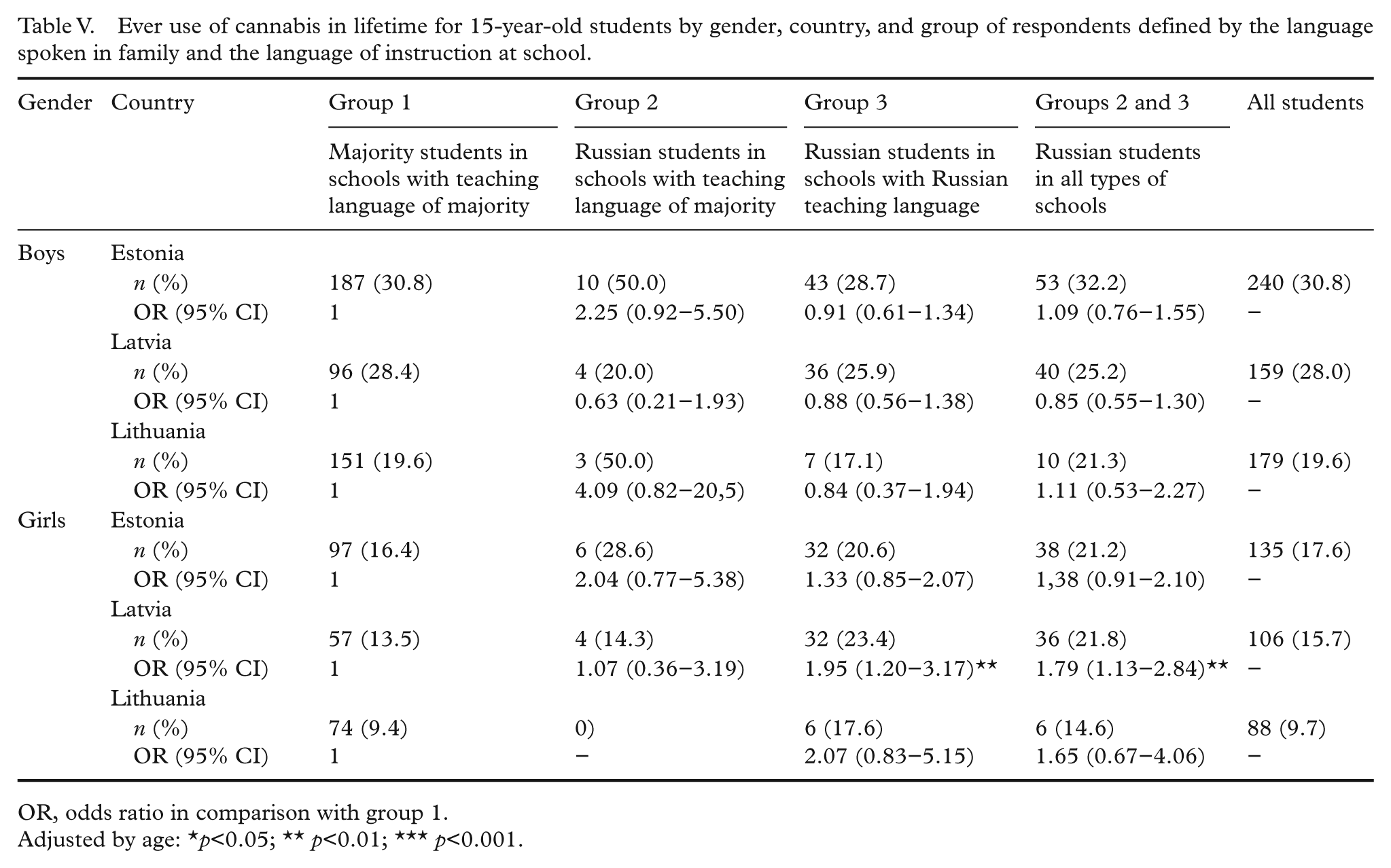
OR, odds ratio in comparison with group 1.
Adjusted by age: *p<0.05; ** p<0.01; *** p<0.001.
Comparative analysis of odds for the above-mentioned risk-taking behaviour was carried out between merged groups 2 and 3 and the reference group 1. Similar results were found as in the comparative analysis of group 3 vs. group 1 for current smoking and cannabis use. Only a minor deviation was established in groups 2 and 3 for Russian boys in Lithuania, who showed no statistical difference with Lithuanian students (group 1) in the analysis of drunkenness. Comparison of all variables from group 2 with the reference group 1 data showed only non-significant differences.
Discussion
The study demonstrated the existence of some differences in self-rated health and in risk-taking behaviour between Russian minority school-aged children and ethnic majority populations. Russian boys were more likely (p<0.05) to evaluate their self-rated health positively in schools with Russian language of instruction. ORs of current smoking and drunkenness were significantly lower among Russian boys in the schools with Russian teaching language (p<0.05) compared to the reference group (boys of majority in schools with the teaching language of majority). In some exceptional cases, the opposite results were obtained in Russian minority girls: significantly poorer self-related health in Lithuania, higher odds for smoking in minority girls in Estonia, and also higher odds for cannabis use in Latvia.
The findings based on results of variations in gender and cases of the individual countries in the Baltic countries show that Russian students as a minority group might be either privileged or disadvantaged (by self-rated health and health behaviour). Some self-rated ethnic health inequalities and their variations within the Baltic countries could be related to the differences in Russian communities in Estonia, Latvia, and Lithuania.
These findings correspond to quite a scattered picture of self-rated health inequalities in other HBSC countries: fair or poor health tends to be more commonly reported by girls than by boys in many countries. In addition, there is a tendency for higher reporting of poor health among older (15-year-old) children [7]. Variation in prevalence of risk-taking behaviour (smoking, alcohol use, cannabis use) was also presented in HBSC reports and showed that rates of weekly smoking were similar among boys and girls of age 13 and 15. We did not find any larger research based on HBSC data on risk-taking behaviour in relation with ethnicity or migration status.
Very few investigations have been conducted in the European countries including Central and Eastern Europe on health inequalities in ethnical minority and migrant groups. Research analysis on health inequalities was carried out among ethnic minority groups aged 15–19 (Croatian, Serbian, Romanian, German, and Hungarian) in Hungary. The authors of this study have concluded that self-reported health evaluation is determined by age, education, chronic disease status, and ethnicity [11]. This study revealed that self-rated health of the ethnic minorities in Hungary was significantly better compared to the Hungarian majority. Our results from the Baltic countries showed that self-rated health of Russian minority boys was also better than that of majority population. However, such results were not observed for girls. Our research suggests that, to some extent, it could be related to higher health satisfaction and healthier life-style – Russian boys in Russian schools have reported lower rates of smoking and drunkenness. The other studies confirm that healthy lifestyle and happiness are related to good self-rated health [12,13].
Numerous investigations on disparities in adults and children have been conducted in the USA, where race and ethnicity variables are used extensively in the population based research [14,15]. A systematic review of literature (781 articles selected and 111 analysed) on “racial and ethnic disparities in health and health care of children” published between 1950 and 2007 in the USA showed a variety of health and health care disparities [16]. Their report states that “racial/ethnic disparities in children’s health and health care are extensive, pervasive and persistent and occur across the spectrum of health and health care”.
Recently a systematic review of self-rated health among migrants and ethnic minorities (only adults were included) was published in Europe. The authors of the review stated the established poorer perceived health among migrants and ethnic minorities after the analysis of 17 European studies [17]. Similar results were established in the comparative study of Roma children health in schools of Lithuania and Latvia: approximately two-thirds of Roma students have rated their health as poor and very poor in comparison with 4.3% in the reference group of majority students [18]. Children with migration background had higher risk for poor psychosocial health, life satisfaction, and overweight in a German study [19]. The results of our study on self-rated health of school-aged children partially oppose these findings. However, the review mentioned above [17] also presents data of some studies, which have established good self-rated health in some groups of migrants and ethnic minorities in Europe.
The majority of researchers agree that social and environmental factors (smoking of parents, peer pressure, child-problem behaviour, parenting problems) in association with substance use may be more important than ethnical predisposition. Some American authors have found that smoking was less prevalent among black school-aged students [20]. The authors of this research relate this phenomenon with non-ethnical determinants and also indicate the previously mentioned social and environmental factors. These researchers recommend provision of universal anti-smoking interventions rather than ethnically oriented health-promotion measures.
Our current findings indicate that Russian boy students who were enrolled in schools with Russian language of instruction had reported lower percentages of smoking, drunkenness and higher percentage of good self-rated health. Other studies show that “sense of coherence” or “sense of community” could be related to other positive sides of health behaviour. The ethnicity is related to the attitudes and motivation through this protective phenomenon. For example, a lower prevalence of smoking was established among adolescents of Japanese and Chinese origin in the Hawaii Islands, and it was explained by higher sense of coherence in the respondents from these ethnic groups [21]. However, in the case of our research, only Russian boys have demonstrated the predisposition for less involvement in risk-taking behaviour; girls demonstrated behaviour similar to the majority of school-children population in the Baltic countries.
The research on migrants has showed that traditions and patterns of alcohol consumption in parental country of origin could affect alcohol use patterns of the first or second generation of migrant population. This was demonstrated by the study carried out in Netherlands, where students from families of migrants (mainly from Muslim countries) showed lower levels of alcohol use than Dutch students [22]. We observed similar results in our study: drunkenness among Russian boys in the schools with Russian teaching language in the Baltic countries was less prevalent than in boys from the ethnic majority schools. The International HBSC 2006 study report have provided data that the percentage of students who had been drunk two times or more was lower in Russia than in the Baltic states. In addition, the difference was more considerable in boys compared to girls [7]. This is in some controversy with the opinion of researchers about Russia as a country with extremely high consumption of alcohol. Thus, the results of our study are in accordance with the above-mentioned studies. However, the pattern of alcohol health behaviour in the country of origin is not the only factor determining the use of alcohol in migrant or ethnic minority populations.
Literature on the migrant populations often quotes so named “healthy migrant effect” [23]. This phenomenon is related with non-random selectivity and is a kind of paradox that the new migrants are often more healthy than the local population. In the Baltic countries, this phenomenon could be attributed to the Russian minority only to a small extent, because the most of our respondents belong to the second or the third generation of migrants and have already lived in our countries for the several decades. It also implies that the children of the former migrants, who were born in our countries, could not be strictly related to that phenomenon. This is why we take this phenomenon into account for reference purpose only because in our study some health and behaviour indicators (good self-rated health, less prevalence of smoking, and drunkenness) were more favourable for Russian school-aged children compared to Estonian, Latvian, or Lithuanian students – the representatives of the major ethnic communities.
Our research analysis showed that environmental determinants and specifically the school factor (as it relates with the sense of community and community empowerment) could play an important role. Such phenomenon could be explained by the influence of multiple factors: better consolidation of communities of ethnical minorities, higher community empowerment, and larger attention to health and health literacy issues at school and at home [24].
We have already analysed HBSC Lithuanian surveys data of 1994–1998 and have established some minor signs of inequalities related to ethnicity in our previous research [25]. These early studies based their focus on indirect self-reporting of ethnicity – only type of schools was included as an independent variable. More recent investigation was conducted on the Lithuanian HBSC country data of 2006. This newer analysis, which was based on self-reported ethnicity, also showed disparities among Lithuanian, Polish, and Russian school-aged children in Lithuania [26]. In the study mentioned above, self-rated health of Polish boys was similar to Lithuanian ones; however, Polish girls rated their health more negatively.
Current research is a part of the international collaborative HBSC cross-country study. The representativeness of the selected samples and high participation rates are the main strengths of the study. Application of standardised methods, including HBSC questionnaire, which was developed by international experts, is a major advantage of this study for comparative analysis. In addition, the results of this study are also a step forward in filling the gap of mapping and understanding health inequalities in the context of ethnicity and migration in Europe.
The study has some limitations. One of them is general to all questionnaire surveys – the issue of validity. We agree that application of self-reported data on substance use could lead to biased results. Some studies have demonstrated a trend to under-report when asking questions on such sensitive risk-taking behaviour as substance use [27]. To tackle with this source of potential bias, the efforts to try to guarantee anonymity of responses, as described in the part of “Material and methods”, were applied. Under-reporting could also be a source of collecting data of poor quality due to low participation rate of persons involved in risk-taking behaviour. However, in our survey overall response rate was over 80%, making this an unlikely reason for underreporting bias.
Defining ethnicity was crucial to our research. Usually ethnicity is self-defined and may change over time and circumstances. In our study ethnicity was reported by the respondent and it was based on the language spoken at home in the family. Such selection was more relevant for avoiding the classification problem related with uncertainty of the “Russian speaking person” identity.
We have selected Russians as the most numerous minority population for this region – they constitute 25.6, 29.6, and 6.3% in Estonia, Latvia, and Lithuania, respectively [28]. Therefore, between the two World Wars, the Baltic countries were ethnically quite homogeneous. Although Russian minority population in the Baltic States started to form several centuries ago, the biggest proportion of Russian migrants arrived here more recently, after the Second World War, starting in 1945. These Soviet-era Russian labour migrants settled mainly in larger cities because of the need for industrial workers. In all three countries, the rural settlements were inhabited almost entirely by the main national ethnic groups, except some areas in eastern Estonia and Latvia. It is also important to mention that the Russian minority group was considered quite wealthy and comparable by education and affluence with the majority population, because, as a rule, the Soviet government used to provide these new settlers with good jobs and convenient accommodation.
In this article we used the term “ethnic minority” instead of the term “migrant population” for several reasons: first, the children population analysed is the second or later generation of Russian migrant population; second, this term is more common in national legislation in the Baltic countries. However, we did not restrict making the research hypothesis that health effects of migration could extend beyond the first generation [1].
The samples of school-aged children population we have analysed are 11-, 13-, and 15-year-old children. They do not represent the whole age range of school age population. This does not allow us to make generalisations, which could be applied to the whole school-aged children population in the Baltic countries. Despite of the above-mentioned limitations, such a study is important because it provides basic data that may guide to the development of policy and interventions in tackling with health inequalities among ethnical groups in the European countries [1,5].
This study confirmed the evidence that some perceived health and health-behaviour inequalities found were not large and may be determined by other multicontextual and specific psychosocial environmental factors at these schools. Our investigation has demonstrated that health perceptions and health behaviour of students of Russian minority, who attend schools with Russian as teaching language, is often better (p<0.05 only for boys) in comparison with their peers of native population. In contrast, students of Russian minority, who are enrolled in schools with the language of the majority, have demonstrated the tendency to have less positive health perception and less positive health behaviour in comparison with their peers of majority at the school. Similar results were also found in our previous research, which covered only Polish, Russian, and Lithuanian school-aged children in Lithuania [26]. Studies show that a phenomenon of isolation could be related with the experience of lower sense of belonging and less connectedness of minority school children to school, as well as self-perception of being in the “host” community [29,30].
Estonia, Latvia, and Lithuania have developed bilingual teaching structures for the national minorities established in our countries and that may also benefit for better integration of immigrant students. Despite that we suggest that universal health promotion and disease prevention programmes could be relevant in both types of schools where languages of majority and minority are used, other experts also agree that integrated and structural approaches should be applied [20,24,31]. However, ethnical sensitivity, awareness, and provision of special literature in the national languages for ethnical minorities could be optional complementary measures and it could increase the quality and effectiveness of the health interventions.
Conclusions
The study found some differences in self-rated health and in risk-taking behaviours between Russian minority school-aged children and ethnic majority populations. Gender- and country-related variations of inequalities were observed. Russian boys were more likely to evaluate their self-rated health positively in schools with Russian as teaching language and in general among the Russian minority. Odds ratios for current smoking and drunkenness were significantly lower among Russian boys in the schools with Russian as teaching language in comparison with the reference group. In general, Russian girls did not differ significantly from the majority population girls by self-rated health as well as by risk of smoking, drunkenness, and use of cannabis. The only exceptions were smoking habits in Estonia and cannabis use in Latvia. Each of the Baltic countries had some specific features of perceived health and profile of risk-taking behaviour. Despite that, more similarities than health inequalities between the countries were identified. This investigation implies that, in general, being a member of Russian minority group was not related to poor self-rated health or involvement in risk-taking behaviour among school-aged children in the Baltic countries.
Footnotes
Acknowledgements
This publication reports data from Estonia (Principal Investigator: Katrin Aasvee), Latvia (Principal Investigator: Iveta Pudule) and Lithuania (Principal Investigator: Apolinaras Zaborskis). The international HBSC coordinator is Candace Currie (University of St Andrews, St Andrews, Scotland); the data bank manager is Oddrun Samdal (University of Bergen, Bergen, Norway). We are grateful to all HBSC study team members (a complete list of the participating researchers can be found on the HBSC website ![]() ) and also for all young people who were involved in this survey.
) and also for all young people who were involved in this survey.
Funding
This research was carried out in the framework of the Health Behaviour in School-Aged Children (HBSC), a WHO collaborative cross-national study. The study was financially supported by the ministries of education, science and health of the participating countries.
Conflict of interest
The authors declare that they have no competing interests.