
Abstract
Aims: The Swedish National Inpatient Registry is an important source of data for numerous epidemiological studies, amongst them studies on chronic obstructive pulmonary disease (COPD). General validation studies indicate that in general 85–95% of diagnoses reported are correct, but this is not true for all groups of diseases, why specific validation studies are of great importance. Methods: Charts from 374 individuals discharged with a COPD diagnosis between 2000–07 from two central hospitals and two university hospitals in the county of Skåne were validated against the original medical files. Criteria for the degree of certainty of the COPD diagnosis were predefined and the association between predictors of diagnostic probability and the level of certainty was assessed using an ordinal logistic regression model. Results: According to the Global Initiative for Chronic Obstructive Lung Disease criteria, 21.7% of the diagnosis were classified as proven COPD, 35.5% were classified as probable, another 34.0% as possible COPD, 2.1% were classified as having an uncertain diagnosis, and 7.0% as an unlikely COPD diagnosis. Age category (adjusted ORs: 60–79 years, 2.6, 95% CI 1.2–5.4; ≥80 years, 1.6, 95% CI 0.7–3.3) and discharge from a non-surgical department (adjusted OR: 1.7, 95% CI 1.1–2.8) were significantly associated with higher level of diagnostic certainty.
Chronic obstructive pulmonary disease (COPD) has reached epidemic proportions and is a major cause of morbidity and mortality worldwide [1]. The estimated prevalence of physician diagnosed COPD in Sweden is 5–10% [2 –4]. This relatively high prevalence in combination with national health care registers offers unique opportunities to perform epidemiological studies.
The Swedish National Inpatient Registry is an important source of data for epidemiological studies [5]. General validation studies suggest that 85–95% of diagnoses reported are correct but this is not true for all disease groups, why specific validation studies are of great importance [6,7].
The sensitivity of identifying COPD patients has been estimated to be about 50% during a 5-year period [8] but the validity of the COPD diagnosis is less well elucidated. In this mini-validation study, the ICD codes from 400 individuals discharged with a COPD diagnosis noted in the Swedish Inpatient Registry were validated against the original medical files.
The County of Skåne, with around 1 million inhabitants, has nine coordinated hospitals with a common electronic chart system (Melior; Siemens, Upplands Väsby, Sweden) which was gradually introduced between 1999 and 2006. All laboratory data (such as clinical chemistry, X-ray results) are available. Old paper charts are concurrently being scanned and added to the electronic charts. We restricted the analysis to discharge diagnoses between 1 January 2000 and 31 December 2007, due to the availability of the electronic charts.
From an existing cohort of 280,000individuals from Southern Sweden, (4800 cases of pneumococcal disease, 48,000 randomly selected control subjects from the general population and their respective first-degree relatives (Chronic pulmonary diseases and the epidemiology of Invasive Pneumococcal Disease. Inghammar, M (not published), we identified 1997 individuals, discharged from either Helsingborg, Kristianstad (central hospitals), Malmö, or Lund (university hospitals) with a COPD diagnosis (between 2000–07) according to ICD-9 (491–492, 496) and ICD-10 (J41–J44), either as a main or as secondary diagnosis. We randomly selected 100 patients from each of the hospitals, whose complete charts were reviewed by one of two authors (MI and AE). Data were extracted according to a prespecified protocol and were made unidentifiable before analysis. All accessible data were used and the total body of evidence from all different wards and clinics, laboratory data, and X-ray findings were included in the total assessment of “how much evidence is there for the doctor in charge to support a discharge diagnosis of COPD”.
We predefined the following criteria for the degree of certainty of the COPD diagnosis:
Proven COPD: according to the criteria from the Global Initiative for Chronic Obstructive Lung Disease (GOLD) [9], forced expiratory volume in the first second/forced vital capacity (FEV1/FVC) <0.7 post bronchodilation.
Probable COPD: a combination of at least three of the following five criteria: (a) FEV1/FVC <0.7 without bronchodilation; (b) physician or self-reported COPD with or without treatment with either inhalation drugs (anticholinergic drugs, long-term β2-agonists, or inhaled corticosteroids) or treatment with theophyllamine or acetylcysteine per os on admission; (c) signs of lung emphysema using computed tomography (CT), high-resolution computed tomography (HRCT), or conventional chest X-ray; (d) a history of tobacco smoking; (e) chronic or an acute episode of respiratory failure (pO2 <7.3±pCO2 >6.0) and/or long-term oxygen treatment.
Possible COPD: a combination of one or two of the above criteria (except smoking history alone), with or without medical treatment.
Uncertain COPD: smoking history alone or none of the above criteria.
Unlikely COPD: FEV1/FVC >0.7 or a concurrent or subsequent more plausible differential diagnosis as deduced from charts.
Chi-squared tests and Fisher’s exact tests were used to assess the distribution of criteria according to the degree of diagnostic precision. Partial ordinal logistic regression was used to assess predictors of diagnostic probability [10]. We considered gender, age (divided in categories: ≤59, 60–79, and ≥80 years of age), discharge from medical or surgical department, COPD as main or additional diagnosis, and hospital for inclusion in the model.
The study was approved by the Lund University Research Ethics Committee (223/2009 and 590/2004).
Twenty-six of the 400 individuals had no electronic chart from the date of interest, thus analyses were based on the remaining 374 individuals. Clinical criteria are detailed in Table I. In total, 23 individuals (6.1%) had a concurrent or were later diagnosed with an explicit alternative diagnosis (e.g. pulmonary fibrosis, hypoventilation) as stated by a pulmonologist. Eight individuals (2.1%) were misclassified asthma patients, whereas another 19 (5.1%) were considered having both asthma and COPD. Concurrent asthma (J45) and COPD discharge codes (from different occasions) were noted in 9.9% of the charts due to both stated overlap and erroneous coding.
Distribution of clinical criteria used to validate the probability of having COPD
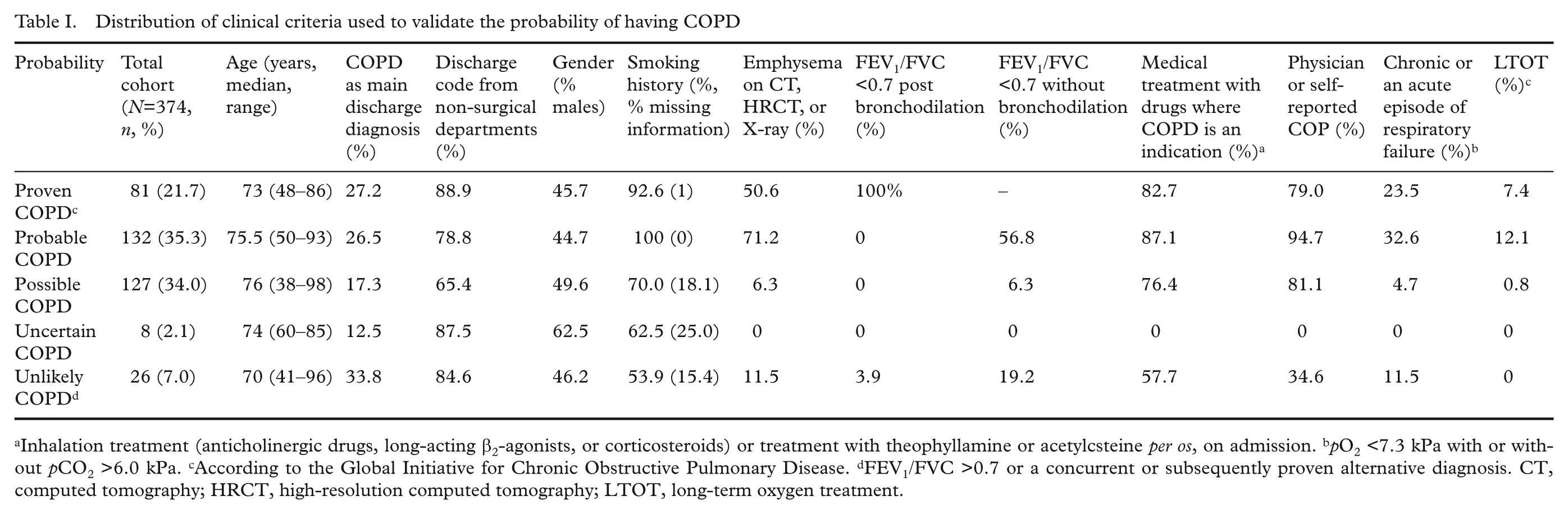
Inhalation treatment (anticholinergic drugs, long-acting β2-agonists, or corticosteroids) or treatment with theophyllamine or acetylcsteine per os, on admission. bpO2 <7.3 kPa with or without pCO2 >6.0 kPa. cAccording to the Global Initiative for Chronic Obstructive Pulmonary Disease. dFEV1/FVC >0.7 or a concurrent or subsequently proven alternative diagnosis. CT, computed tomography; HRCT, high-resolution computed tomography; LTOT, long-term oxygen treatment.
Using the predefined criteria, 81 individuals (21.7%) were classified as Proven COPD according to the GOLD criteria, while 132 (35.3%) fulfilled three or more of the prespecified criteria and were classified as Probable COPD. Another 127 (34.0%) were classified as Possible COPD, eight individuals (0.8%) were classified as uncertain COPD. In total, 26 individuals (7.0%) had a FEV1/FVC of >0.7 or a more plausible alternative diagnosis and were classified as unlikely COPD (Table I). In the group classified as possible COPD, 81.1% had physician- or self-reported COPD, 76.4% were on medical treatment, 70.1% had a history of smoking, 63% had a combination of physician- or self-reported COPD, a smoking history, and medical treatment.
Age category (adjusted ORs, reference category ≤59 years: 60–79 years 2.6, 95% CI 1.2–5.4; ≥80 years, 1.6, 95% CI 0.7–3.3; p=0.002) and discharge from a non-surgical department (adjusted OR: 1.7, 95% CI 1.1–2.8; p=0.02) were significantly associated with higher level of diagnostic certainty, whereas gender, hospital, and COPD as main or additional diagnosis were not, as estimated in partial ordinal logistic regression models. Proportional-odds assumption was not violated in the final model including all of the above parameters except gender.
In this study we show that a COPD diagnosis in the Swedish Inpatient Registry is of relatively high validity based on the data from the original charts. More than half of the patients discharged with a diagnosis of COPD had a proven or clinically probable COPD, another third had possibly COPD, and less than 10% of the individuals had an uncertain diagnosis or were misclassified. All disease states were seen, from mild to severe, especially with COPD as secondary diagnoses, since patients were admitted due to diverse reasons not necessarily linked to COPD.
Electronic charts were not fully introduced until 2006, paper charts are concurrently being scanned but in many cases spirometry results from older paper charts and X-ray results were not retrievable. Full access to all paper charts would probably increase the proportion of proven/possible COPD. 15 individuals of those lacking prior or concurrent spirometry results had a FEV1/FVC of <0.7 noted from later visits.
We extracted data from charts as they were presented, e.g. we did not re-evaluate X-rays. Nor did we question the medical evaluation done by physicians. In case of conflicting judgements in differential diagnoses, statements from pulmonologists were given interpretative prerogative status.
The predefined criteria for the level of diagnostic certainty have not been externally validated and could be discussed since different cut points would change the proportions. On the other hand, these were only used as means for assessing potential restriction criteria for case selection in the Inpatient Registry in the context of epidemiological studies.
COPD patients were identified in a large population-based cohort and performed at two university and two central hospitals, with chart linkage to all but one hospital in the County of Skåne, an area with around 1 million inhabitants. Hence, we feel confident that these results could be generalized to the Inpatient Registry as a whole.
In summary, COPD diagnosis from the Swedish Inpatient Registry is of acceptable validity for epidemiological research.
Footnotes
Acknowledgements
We would like to thank Susanne Sköld, Staben för Verksamhetsutveckling och eHälsa, Skåne University Hospital, for help with retrieving charts.
Funding
The work was supported by the Swedish Heart and Lung Foundation (project no. 20080246), the Swedish Government Funds for Clinical Research (ALF), the foundations of Greta and Johan Kock, Skåne University Hospital, and Alfred Österlund.
Conflict of interest
Gunnar Engström is employed as senior epidemiologist by AstraZeneca R&D. The other authors declare no conflicts of interest.