
Abstract
Aims: Lack of brief questionnaire instruments for quantifying affective reactions to and behavioral disruptions attributed to sounds and electromagnetic fields (EMFs) motivated the present development and metric evaluation of such instruments, called the 11-item Noise Sensitivity Scale (NSS-11) and the 11-item Electromagnetic Field Sensitivity Scale (EMFSS-11). Another objective was to establish normative data for these instruments. Method: Data from 3406 individuals who took part in the Västerbotten Environmental Health Study was used. The participants constitute a random sample of inhabitants in the county of Västerbotten in Sweden, aged 18 to 79 years, stratified for age and gender. The participants responded to the NSS-11 and EMFSS-11 and to additional questions for evaluation of concurrent validity. Results: The results show satisfying reliability (Cronbach α = 0.71–0.85, varying with age group and gender), concurrent validity, and unidimensionality of the NSS-11 and EMFSS-11, and that the scales generate scores with approximately normal distributions, irrespective of age group and gender. Mean scores, standard deviations, and confidence intervals constitute normative data.
Keywords
Introduction
The impact of environmental exposures is a considerable public health problem. However, reactions to such exposures vary considerably between individuals. Whereas some show no adverse reactions, others show reactions that range from annoyance to intolerable health symptoms, despite similar exposure. The sensitive person may relate the annoyance or symptoms to one or several environmental factors, such as chemicals and biological materials (e.g., mold) that generate odor and sensory irritation (pungency), mechanical phenomena that generate sounds, and switched-on electrical devices that generate electromagnetic fields (EMFs). Health effects of exposure to strong EMF fields are well documented, and such exposure is controlled by regulations and guidelines. However, there is no existing evidence for health effects from low-level EMF exposure. Instead there is evidence for a classical-conditioning based nocebo effect in triggering acute health effects [1]. Nevertheless, public health problems evoked in the presence of electrical equipment is a concern. Although it may not be the EMFs from electrical devices that evoke annoyance or symptoms, we will here for simplicity use the terms annoyance/intolerance to EMFs.
The concept of environmental annoyance is complex, and can be considered a perception, an emotion, an attitude or a mixture of these. Importantly, annoyance is likely to precede symptom development [2], and should, thus, be taken seriously for prevention of long-term health effects. Consequently, annoyance is considered by the World Health Organization as a community problem even when only a small proportion of the population (5%) is bothered during short periods of time (2%). Results from population-based studies show rather high prevalence for annoyance attributed to environmental odorous/pungent chemicals (17–33%), traffic noise (25–29%) and EMFs (13%) [3 –6]. Eek and associates [7] conducted a large-scale longitudinal, population-based questionnaire study in which annoyance was rated from each of the five items fluorescent tube lighting, visual display units, other electrical equipment, breathing air that smells of chemicals, and other smells. The authors found that those respondents who at baseline reported relatively strong subjective health complaints, high levels of stress, strain, and lack of recovery, more dissatisfaction with their work situation, and lower personal social support rated relatively high environmental annoyance at 5-year follow-up. This suggests that negative affect may contribute to environmental annoyance.
Intolerance to conditions in the environment can be considered as more severe than annoyance, with symptoms being attributed to the exposure. As would be expected, the prevalence rates are somewhat lower than for annoyance, regarding odorous/pungent chemicals (9–19%) [8,9], certain buildings (nonspecific building-related symptoms; 4%) [10], sounds (8–15%) [11,12], and EMFs (1.5–5%) [13,14]. Apart from general symptoms (e.g. fatigue) being very common in these intolerances, certain symptoms may be slightly more common for a certain type of intolerance, compared to other intolerances. For example, airway symptoms appear to dominate in intolerance to odorous/pungent chemicals, mucosae and skin symptoms among nonspecific building-related symptoms, attentional and emotional symptoms in intolerance to sounds, and skin symptoms in intolerance attributed to EMFs. However, the symptom picture varies considerably within intolerances, with large overlap between intolerances [13]. The negative impact on quality of life can be considerable in environmental intolerance [15]. As for intolerance to EMFs [1], classical conditioning [16], but also neural sensitization [17] and neurogenic inflammation [18] have been suggested as underlying mechanisms in intolerance to odorous/pungent chemicals. Cognitive and emotional processes, such as stress, depression and anxiety, are likely to play critical roles in these mechanisms [19]. Sound intolerance has also been found to be associated with stress, depression and anxiety [20]. However, understanding for the pathology of environmental intolerance is still limited. Nevertheless, these studies, together with the study by Eek and associates [7], highlight the important role of negative affect in environmental annoyance and intolerance, but the distinction between annoyance and intolerance is not clear.
Concomitant hypersensitivities with symptom attribution to odorous/pungent chemicals, sounds and EMFs appear to be rather common [4,13]. This emphasizes the role of person variables for understanding mechanisms underlying these conditions. However, in most cases, single questions have been used to assess these intolerances, with no or limited documentation of reliability or validity. The rather crucial question of concomitance does indeed call for reliable and valid tools for quantifying extent of intolerance attributed to these different environmental factors, and preferably relatively quick tools with normative data. For the study of concomitance it is also a great advantage if the instruments used for the different environmental aspects are analogous, enabling direct comparison.
The Noise Sensitivity Scale (NSS) was developed by Weinstein [21] to quantify affective reactions to and behavioral disruptions by environmental sounds. The NSS consists of 21 statements for the individual to respond to on a Likert scale. The 21-item Chemical Sensitivity Scale (CSS) [22] was subsequently developed to be analogous to the NSS. This was achieved by having the statement about environmental odorous/pungent chemicals for each CSS item correspond as closely as possible to a statement in the NSS about the sound environment. For example, the CSS item “At movies, other persons’ perfume and aftershave disturb me” corresponds to the NSS item “At movies, whispering and crinkling candy wrappers disturb me.” Furthermore, the response alternatives in the two scales are identical for each corresponding statement. Both the NSS and CSS have good test-retest reliability, internal consistency and validity, and generate approximately normal distributions [21 –23].
From the 21-item CSS, a short version was formed by selecting the 11 items with highest sensitivity and specificity for differentiating individuals who are intolerant to odorous/pungent chemicals from those who are tolerant. Since the intolerant subjects were patients with sensory hyperreactivity (SHR; a form of intolerance to odorous/pungent chemicals) [24], the 11-item scale was referred to as the Chemical Sensitivity Scale for Sensory Hyperreactivity (CSS-SHR). As for the CSS, the CSS-SHR has good test-retest reliability, internal consistency, validity [25], and normative data [26]. Apart from use of the CSS-SHR for clinical investigation of patients with suspected SHR, this short scale has proven useful for assessing general forms of chemical annoyance/intolerance [27] as well as pregnancy-induced odorant annoyance/intolerance [28].
A short questionnaire-based tool for quantifying affective reactions to and behavioral disruptions attributed to EMFs, analogous to the CSS-SHR, would be particularly valuable for direct comparison of annoyance/intolerance to odorous/pungent chemicals and EMFs. Prior research has used those 11 NSS items about sound annoyance/intolerance that are analogous to the 11 CSS-SHR items, together with the CSS-SHR items, for direct comparison between annoyance/intolerance to odorous/pungent chemicals and sounds [21]. However, metric properties and normative data for this short version of the NSS have not been documented. This noise instrument would, in combination with the CSS-SHR and an analogous EMF instrument enable direct comparison with quick assessment between degree of environmental annoyance/intolerance to chemicals and biological materials, mechanical phenomena, and electrical equipment.
An advantage of assessing affective reactions and behavioral disruptions for quantifying environmental sensitivity is that these responses are valid for a wide sensitivity range, including annoyance and intolerance. A somewhat higher than normal score on an environmental sensitivity scale of this kind, but yet not a high score (e.g. below 1 or 2 standard deviations above the mean for normative data) can represent environmental annoyance, whereas a high score (e.g. 1 or 2 standard deviations or more above the mean for normative data) can represent environmental intolerance. Rather than being used for clinical urposes, cutoffs based on standard deviations may have very useful epidemiological applications.
A first objective of the present work was to develop an easily administrated, inexpensive and quick (11-item) annoyance/intolerance instrument, analogous to the CSS-SHR, for quantifying self-reported affective reactions to and behavioral disruptions attributed to EMFs. This instrument is referred to as the 11-item Electromagnetic Field Sensitivity Scale (EMFSS-11). A second objective was to metrically evaluate the EMFSS-11 and the 11-item version of the NSS (analogous to the CSS-SHR and EMFSS-11). This short version of the NSS is referred to as the 11-item Noise Sensitivity Scale (NSS-11). The metric evaluation of the NSS-11 and EMFSS-11 was conducted with respect to the scales’ frequency distribution of scores, reliability (internal consistency), concurrent validity, and dimensionality. A third objective was to establish normative data for the NSS-11 and EMFSS-11. In addition to normative data for a general population, the objective was to provide reference data for combinations of specific age groups (young, middle-aged and elderly adults) and gender. This was conducted with data from a population-based study, the Västerbotten Environmental Health Study.
Methods
Study population and sampling
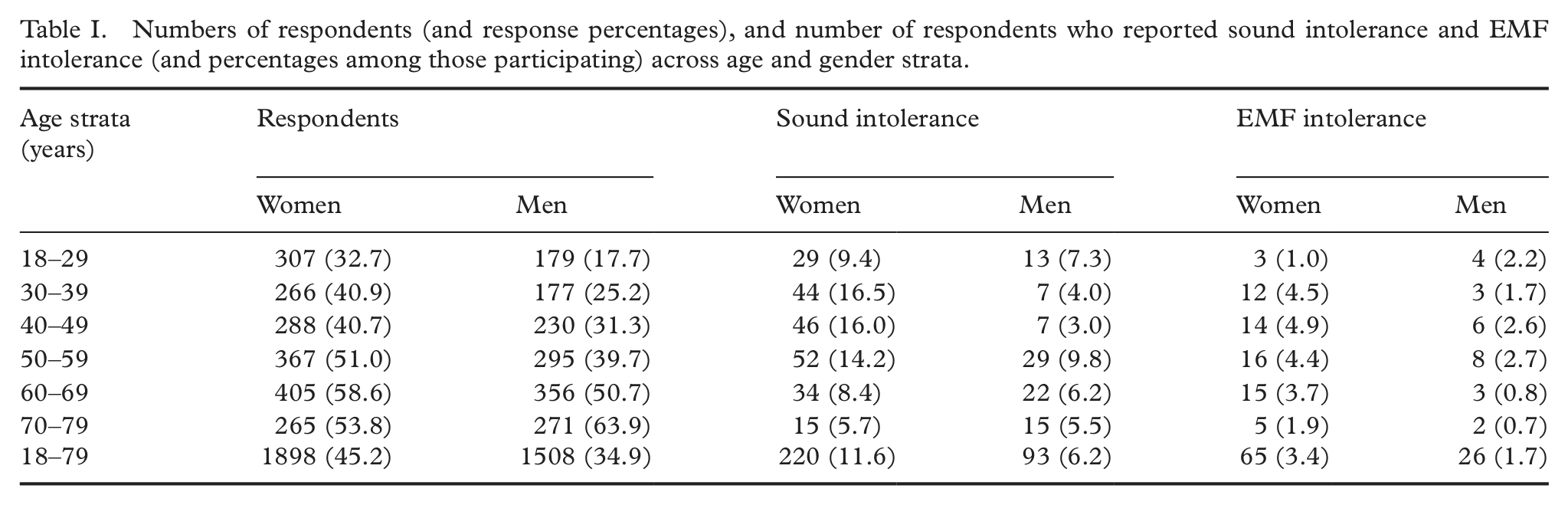
The Västerbotten Environmental Health Study is an embracing name for different investigations on the same general population regarding various forms of environmental intolerance in Sweden. The study population, inhabitants in the county of Västerbotten in Northern Sweden, has an age and gender distribution that is very similar to that of Sweden in general [29]. A random sample, drawn from the municipal register, of 8520 individuals aged 18 to 79 years was invited to participate. The sample was stratified for age and gender according to the following age strata: 18–29, 30–39, 40–49, 50–59, 60–69 and 70–79 years. Of the 8600 individuals, 8520 could be reached, among whom 3406 (40.0%) agreed to participate. Age and gender distributions for the respondents are given in Table I. The highest non-response rate is found among men aged 18–29 years. The respondents are further described in Table II with respect to demographic and health issues of relevance to sound and EMF intolerance.
Numbers of respondents (and response percentages), and number of respondents who reported sound intolerance and EMF intolerance (and percentages among those participating) across age and gender strata.
Description of the respondents (n = 3406).
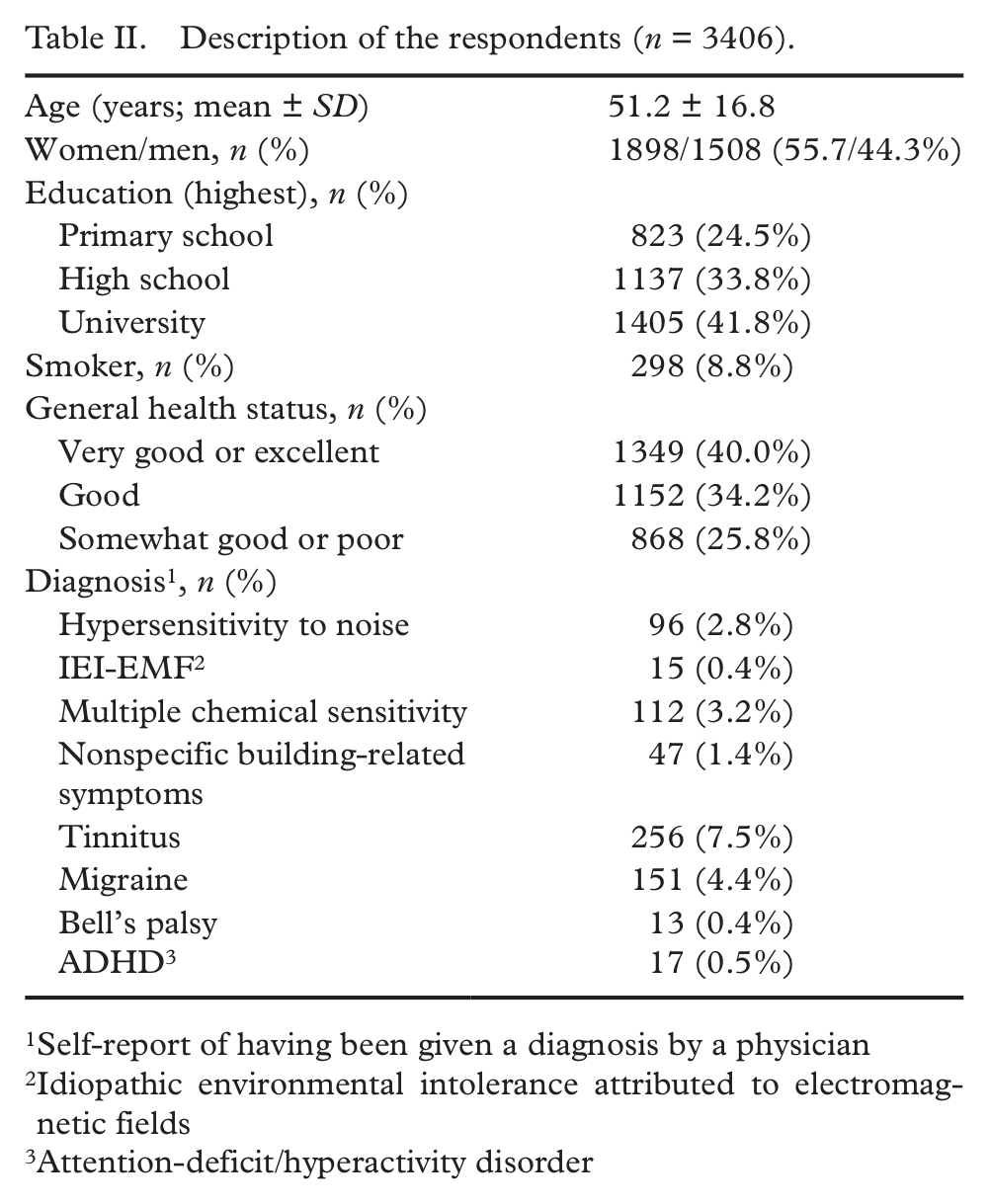
Self-report of having been given a diagnosis by a physician
Idiopathic environmental intolerance attributed to electromagnetic fields
Attention-deficit/hyperactivity disorder
Questions and questionnaire instruments
A questionnaire was used that included questions on background information pertaining to the demographic and health issues (Table II). The questionnaire also included the instruments NSS-11 and EMFSS-11 that are given in Table III together with the CSS-SHR for comparison. The NSS-11 includes the 11 items from the 21-item NSS that correspond to the items in the CSS-SHR. For the EMFSS-11, we generated 11 statements about common situations of exposure to EMFs (e.g. “At music concerts or similar events, it is disturbing to know that there is a lot of electrical equipment around me”) based on statements in the CSS-SHR (e.g. “At movies, other persons’ perfume and aftershave disturb me”) and NSS-11 (“At movies, whispering and crinkling candy wrappers disturb me”). Thus, we strived to make the statements in the EMFSS-11 as analogous as possible to those in the CSS-SHR and NSS-11. The unweighted sum of the 11 items (after reversed coding of seven items; Table III) makes up the individual’s total NSS-11 and EMFSS-11 score. The score on each scale can range from 0 to 54 (high score representing high annoyance/intolerance).
Items and rating scales of the 11-item Chemical Sensitivity Scale for Sensory Hyperreactivity (CSS-SHR), the 11-item Noise Sensitivity Scale (NSS-11) and the 11-item Electromagnetic Field Sensitivity Scale (EMFSS-11).
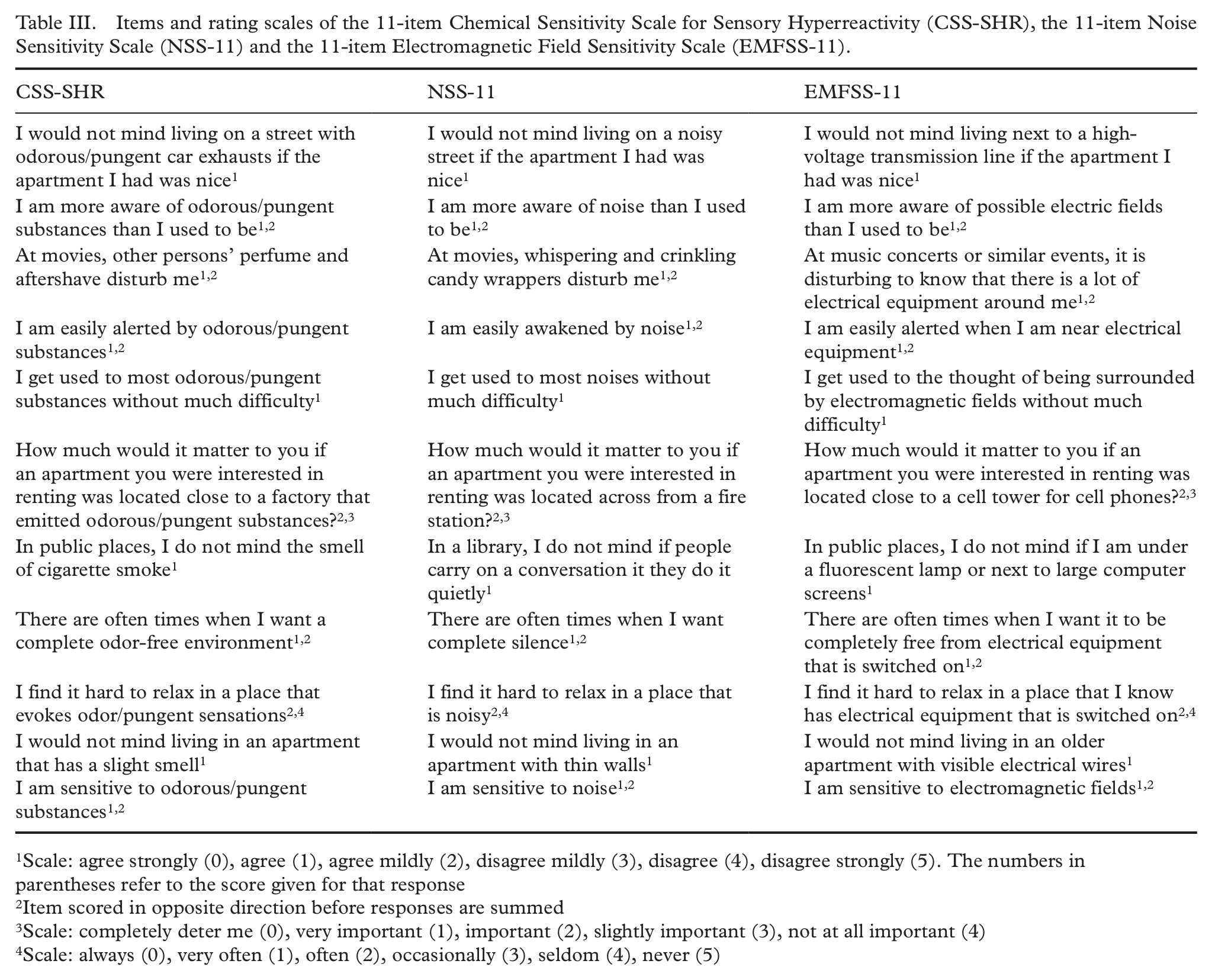
Scale: agree strongly (0), agree (1), agree mildly (2), disagree mildly (3), disagree (4), disagree strongly (5). The numbers in parentheses refer to the score given for that response
Item scored in opposite direction before responses are summed
Scale: completely deter me (0), very important (1), important (2), slightly important (3), not at all important (4)
Scale: always (0), very often (1), often (2), occasionally (3), seldom (4), never (5)
The following two general questions about noise and EMF annoyance/intolerance were used for concurrent validation of the NSS-11 and EMFSS-11, respectively: “Do you have a hard time tolerating everyday sounds that you believe most other people are not bothered by?” and “Are you bothered by certain switched-on electrical devices that you believe most other people are not bothered by?”
Concurrent validation of the NSS-11 and EMFSS-11 was further conducted with sound and EMF symptom-trigger indices, respectively. These indices were based on ratings of 10 specific sound and 10 specific EMF environments/sources. The 10 sound environments/sources were mechanical, monotone sounds/buzzing machines; chinking from chinaware/clanking/clattering sounds; background sounds from radio/stereo/TV; speech sounds; surging ventilation/dull fan sounds; sound from hammer strokes; sounds from cell phones (ring signals/conversations); paper rustling; traffic noise; and alarm signals and similar unexpected sounds. The 10 EMF environments/sources were other persons’ cell phones; wireless phones; cell towers for cell phones; computers/computer screens; train trips; own use of cell phones; fluorescent lamps/low energy lamps; home electronics (e.g. TV/radio/stereo); office machines (e.g. copy machines); and high-voltage transmission lines. Each environment/source was rated on the Environmental Annoyance Scale (EAS), with respect to extent to which it causes annoyance/intolerance. The EAS is a category scale with seven semantic descriptors: Not at all (0), a little (1), partly (2), pretty much (3), rather much (4), to a large extent (5), and extremely much (6). It has ratio scale properties, and good reliability and validity [30]. The unweighted sum of the 10 sound and 10 EMF environments/sources made up the individual’s symptom-trigger index for sound and EMF, respectively, and could range from 0 to 60 (high score representing high annoyance/intolerance).
Procedure
The respondents were mailed a questionnaire, to be returned by mail with prepaid postage. Non-responders received up to two reminders. All participants responded to the questionnaire during the period March–April 2010, before the onset of the pollen season in Västerbotten. The study was conducted in accordance with the Helsinki Declaration and approved by the Umeå Regional Ethics Board. The study conforms to the principles embodied in the Declaration of Helsinki as well as to the International Ethical Guidelines for Biomedical Research Involving Human Subjects and the International Guidelines for Ethical Review for Epidemiological Studies. All participants gave their informed consent to participate.
Statistical analysis
Descriptive statistics and Cronbach α coefficients were computed for the NSS-11 and EMFSS-11. One-way analyses of variance (ANOVAs) were conducted for comparing NSS-11 and EMFSS-11 scores between participants responding positively vs. negatively on the general questions about sound and EMF annoyance/intolerance. Spearman correlation coefficients were computed between scores on the symptom-trigger index for sounds and the NSS-11, and between the symptom-trigger index for EMFs and the EMFSS-11. Finally, factor analyses with Varimax rotation and Kaiser normalization were carried out for the NSS-11 and EMFSS-11 data to study dimensionality. A scree test plot was made to identify the number of factors to be extracted. IBM SPSS Statistics 19 (IBM Corporation, New York) was used for statistical analysis. The α-level was set at 0.05.
Results
Frequency distributions and normative data
Descriptive statistics for the NSS-11 and EMFSS-11 are presented in Table IV, for combinations of specific age groups (young [18–34 years], middle-aged [35–54 years], and elderly [55–79 years]) and gender, for the three age groups separately, for gender separately and for the total sample. For each subgroup the skewness and kurtosis was less than three times the standard error of the corresponding skewness and kurtosis measure, respectively, suggesting approximately symmetrical and mesokurtic distributions. The means, standard deviations and confidence intervals constitute normative data.
Descriptive statistics for scores on the 11-item Noise Sensitivity Scale (NSS-11) and the 11-item Electromagnetic Field Sensitivity Scale (EMFSS-11), constituting normative data, and the scales’ reliability (Cronbach α) for various subgroups and for the total sample.
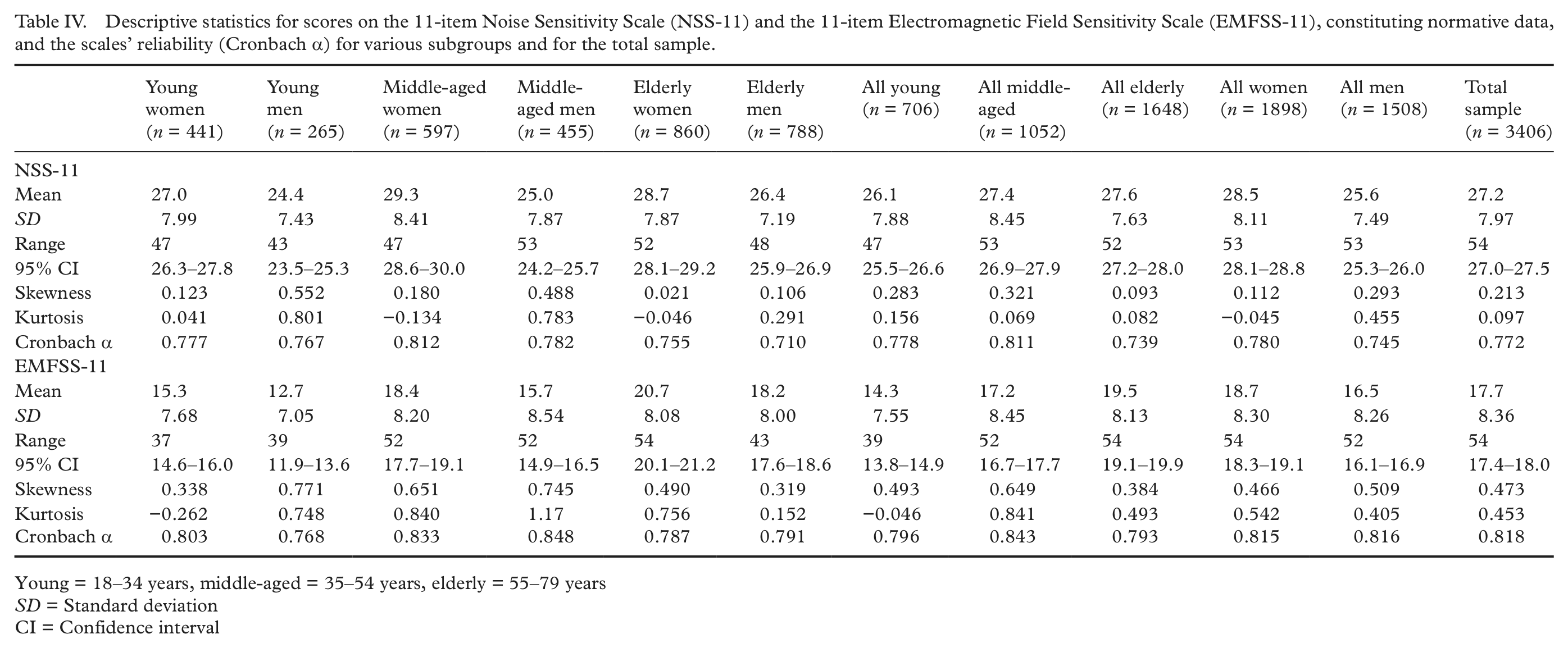
Young = 18–34 years, middle-aged = 35–54 years, elderly = 55–79 years
SD = Standard deviation
CI = Confidence interval
Reliability
Cronbach α coefficients of internal consistency are given in Table IV for the NSS-11 and EMFSS-11, for combinations of specific age groups and gender, for the three age groups separately, for gender separately, and for the total sample. These coefficients range from 0.71 to 0.85, suggesting satisfying reliability of the NSS-11 and EMFSS-11.
Concurrent validity
Three-hundred and thirteen participants responded positively to the general question about sound intolerance, and 3018 participants responded negatively to this question. Among women who responded positivity, 54 were aged 18–34 years, 95 were aged 35–54 years and 71 were aged 55–79 years. Corresponding numbers for men were 17, 29 and 47, respectively. Regarding the general question about EMF intolerance, 91 participants responded positively and 3248 participants responded negatively to this question. Among women who responded positivity, 8 were aged 18–34 years, 29 were aged 35–54 years and 28 were aged 55–79 years. Corresponding numbers for men were 7, 13 and 6, respectively.
Mean scores on the NSS-11 and EMFSS-11 for the intolerance and non-intolerance groups are presented in Figure 1. The higher NSS-11 and EMFSS-11 scores for those participants responding positively, compared to negatively, to the general questions about intolerance were verified by one-way ANOVAs for the NSS-11 (F = 610.0, p < 0.001) and the EMFSS-11 (F = 232.4, p < 0.001), suggesting good concurrent validity in the NSS-11 and EMFSS-11.
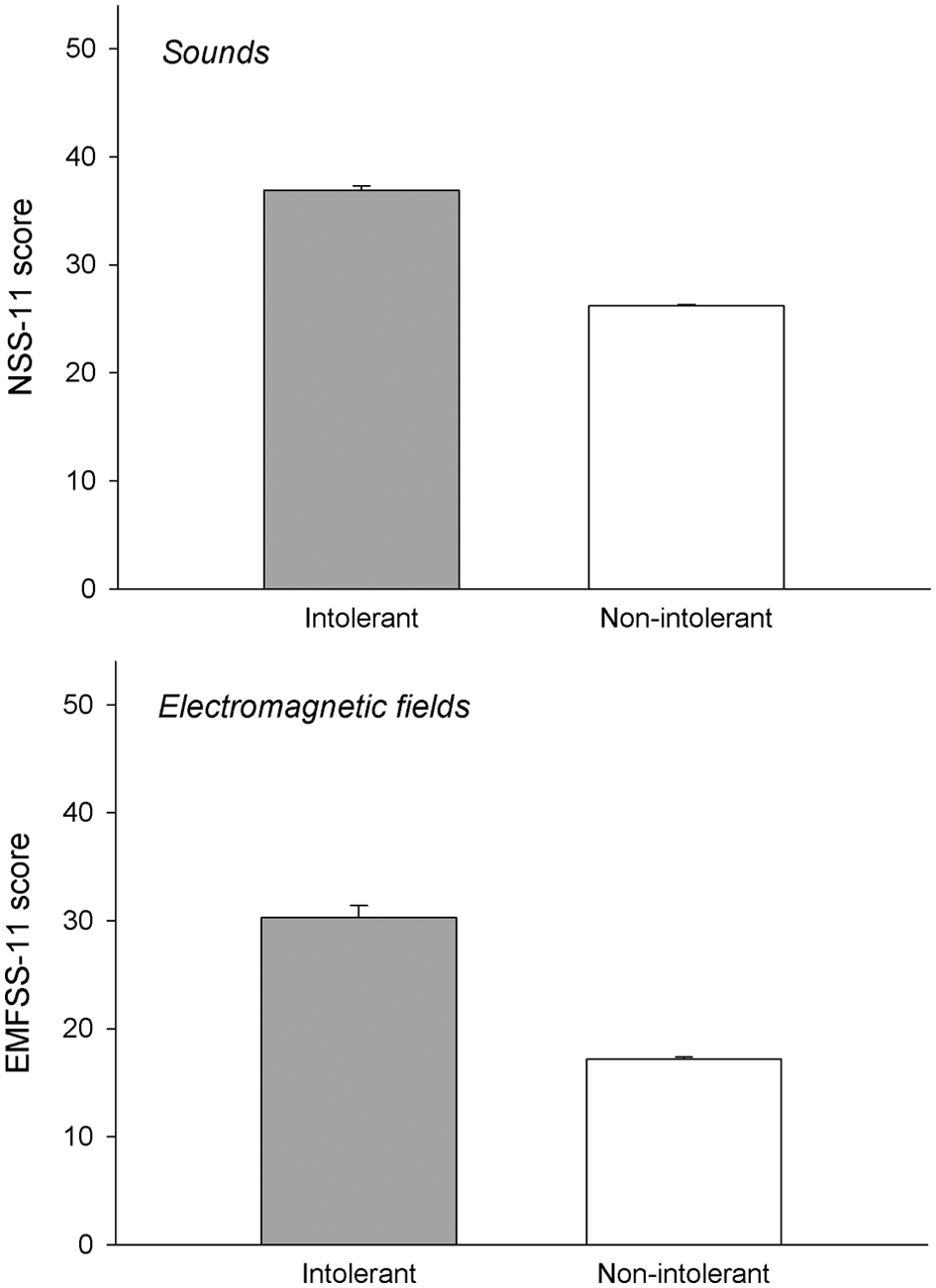
Mean (+SE) score on the NSS-11 for participants responding positively (intolerant) and negatively (non-intolerant) to a question about sound intolerance (upper diagram), and on the EMFSS-11 for participants responding positively (intolerant) and negatively (non-intolerant) to a question about EMF intolerance (lower diagram).
The Cronbach α coefficient was 0.89 for the symptom-trigger index for sounds, and 0.94 for the symptom-trigger index for EMFs. The Spearman correlation coefficient for the relation between score on the symptom-trigger index for sounds (positively skewed distribution) and NSS-11 score was 0.53 (p < 0.001). Corresponding coefficient between the symptom-trigger index for EMFs (positively skewed distribution) and EMFSS-11 score was 0.55 (p < 0.001). These correlations provide further support for concurrent validity of the NSS-11 and EMFSS-11.
Dimensionality
Separate factor analyses with Varimax rotation and Kaiser normalization for the NSS-11 and EMFSS-11 data identified, in both cases, three factors with an eigenvalue above 1. For the NSS-11, the eigenvalues were 3.59 (32.6% explained variance), 1.17 (10.4%) and 1.03 (9.4%), and for the EMFSS-11, the eigenvalues were 4.28 (38.9%), 1.34 (12.2%) and 1.11 (10.1%). However, scree test plots suggest only one factor to be extracted for the NSS-11 and EMFSS-11. The following factor loadings were obtained for the NSS-11: item 1: 0.34; item 2: 0.58; item 3: 0.41; item 4: 0.44; item 5: 0.54; item 6: 0.44; item 7: 0.11; item 8: 0.52; item 9: 0.74; item 10: 0.25; item 11: 0.77. For the EMFSS-11, the factor loadings were: item 1: 0.33; item 2: 0.66; item 3: 0.72; item 4: 0.77; item 5: 0.46; item 6: 0.58; item 7: 0.40; item 8: 0.63; item 9: 0.68; item 10: 0.28; item 11: 0.67.
Discussion
An objective of the present study was to develop and metrically evaluate short questionnaire-based instruments for quantifying affective reactions to and behavioral disruptions attributed to sounds and EMFs. These instruments are analogous to the CSS-SHR in order to enable direct comparison of annoyance/intolerance to odorous/pungent chemicals, sounds and EMFs. The data from this population-based, large-scale study (n = 3406) suggest that the NSS-11 and EMFSS-11 have satisfying reliability and concurrent validity, and that they are unidimensional. The results further show that the NSS-11 and EMFSS-11 generate scores with approximately normal distributions from young, middle-aged and elderly adults, from women and men, from various combinations of age groups and gender, and from the general population.
Another objective was to establish normative data for the NSS-11 and EMFSS-11. This data makes it possible to quantify individuals or groups with respect to annoyance/intolerance to sounds and EMFs. The quantification can be expressed in terms of, for example, percentile, z and T score, and stanines.
The validation of the NSS-11 and EMFSS-11 was conducted by comparison with a general question about annoyance/intolerance; one question concerning sounds and another concerning EMFs, as well as with a symptom-trigger index for sounds and EMFs. Whereas this two-fold assessment of concurrent validity is an advantage, and the questions can be considered to have good face validity, certain caution should be taken when interpreting the results. Thus, the general questions about annoyance/intolerance are single items, and the symptom-trigger indices have not been validated. Although meta-analyses of single-item questions suggest that the reliability of such questions often correspond well to that of indexes, this may be a limitation.
The present study population has an age and gender distribution that is very similar to that of Sweden in general [29]. This enhances generalization of the findings for use of the NSS-11 and EMFSS-11 on the general Swedish population and other similar populations. However, among the randomly selected individuals, only 40% volunteered. This is a somewhat low percentage, with consequences for the representativeness. Research ethical regulations for conducting research in Sweden do not allow asking the selected individuals why they chose not to participate or about certain characteristics they may possess. However, information on age and gender was available for those who declined participation in this study, and the largest proportion of non-responders was found among young men. Assuming that young men to a relatively low degree are bothered by environmental exposures, the normative data may for the groups “all young”, “all men” and “total sample” have somewhat higher mean scores than otherwise would have been the case.
It is possible that individuals who are high on annoyance/intolerance to sounds and EMFs, compared to those who are low, are more likely to agree to participate, since they may be more inclined to find this type of study to be important. Support for this is provided in Table I, showing that more women than men chose to participate, and that intolerance to sound and EMF was more common among women. This may also have contributed to slightly higher mean scores on the NSS-11 and EMFSS-11. When using the normative data from this study one should therefore bear in mind that the comparison of the obtained NSS-11 and EMFSS-11 scores with the normative data may be a slight underrepresentation of the individual’s annoyance/intolerance. Thus, the normative data may be somewhat conservative.
A mean CSS-SHR score of 29.7 has been reported for the same entire sample as that investigated in the present work [26]. Whereas that score is rather similar to corresponding NSS-11 score of 27.2, it is higher than corresponding EMFSS-11 score of 17.7 (Table IV). Since the items and rating scales in the three sensitivity scales are analogous, this suggests that the general population is more annoyed/intolerant to odorous/pungent chemicals and sounds than to electromagnetic fields. This emphasizes the need to relate obtained scores from the different sensitivity scales to their respective normative data before comparing sensitivities across environmental exposures.
Conclusion
The NSS-11 and EMFSS-11 can be recommended for reliable and valid quantification of affective reactions to and behavioral disruptions by sounds and EMFs. The fact that the two instruments consist of only 11 items enables fast assessment (about 5 min for each instrument), and are thus of particular value for epidemiological purposes.
Footnotes
Acknowledgements
We gratefully acknowledge Annika Glader for supervising the TEMA project of which this work was part.
Conflict of interest
None declared.
Funding
This study was supported by grants from the European territorial cooperation program Botnia-Atlantica (grant number 162621), Region Västerbotten, Sweden (grant number REGAC-2011-148), the Regional Council of Ostrobothnia, Finland (grant number 201126), and the Swedish Asthma and Allergy Association’s Research Fund.