
Abstract
Aims: Physicians’ high dropout rate is a significant problem in primary care in many countries. One solution to this issue is to recruit internationally mobile physicians. This study explores the role of psychosocial factors in explaining intention to leave among GPs including potential differences between foreign-born and Finnish GPs. Methods: A cross-sectional questionnaire was sent to randomly-selected Finnish physicians (n = 7000) and all foreign-born physicians (n = 1297) living in Finland in the year 2010. The questionnaire was returned by 4333 physicians, of whom 832 were GPs. Of those 176 were foreign-born GPs. Results: Intention to leave was more common among foreign-born GPs (59%) than among Finnish GPs (52%). High job demands were associated with higher intention to leave from primary care both in foreign-born (OR 1.90) and Finnish GPs (OR 2.20). This association remained among foreign-born GPs after adjusted the model for the country of origin or the reason for migration (OR 1.80, 1.82). Lack of job control, patient-related stress, and stresses related to teamwork were associated with higher intention to leave only among Finnish GPs (ORs 0.45, 1.75 and 1.99).
Keywords
Introduction
Physicians’ high dropout rate is a significant problem in primary care in many countries, with potentially negative consequences for both health services and patient care [1]. In some developed countries, such as the United Kingdom, New Zealand, and the US, foreign-born physicians fill part of the gap in the medical workforce in primary care [2]. Recent studies of medical migration have been focused e.g. on ethical recruitment [3] and inflows of foreign-born physicians [4]. Not much research has been carried out into the foreign-born physicians’ length of the stay and the factors affecting their motivation to stay and work as a GP in a target country.
It has often been shown that a negative psychosocial work environment is associated with intention to leave and actual turnover behaviour among native physicians [5,6]. One of the most widely-studied theoretical approach is the “Job Demand-Control” (JDC) model [7], which suggests that employees working under high demands and low job control have a higher risk of health problems and reduced wellbeing than those with no such strain. The JDC model was initially used to explain patterns of exhaustion and job dissatisfaction, but was later expanded to predict a wide variety of motivational outcomes, such as intention to leave jobs [8,9].
Less is known about specific psychosocial work-related factors that may affect a physician’s intention to leave, such as patient-related issues or problems with teamwork. Dealing with uncooperative patients has been recently shown to increase work stress among general practitioners [10]. Poor teamwork has been suggested to decrease the job satisfaction of GPs [11] and increase psychological stress [12]. Even less is known about foreign-born physicians’ stress factors and how they affect their intention to leave. However, some studies have found differences in the stress levels and coping mechanisms of physicians in different countries; for example, job demand increases job stress among Indian physicians but not among their Norwegian peers [13].
The Finnish health care system faces many challenges, including a shortage of GPs, high physician turnover from public primary care to special health care or the private sector, and the rising costs of health care [14]. During 1999–2007, the percentage of unfilled GP positions increased from 5 to 18% [15]. The number of foreign-born physicians has increased rapidly in Finland during the past 10 years. In 2000, foreign-born physicians accounted for less than 4% of the practising physicians of working age, but in 2010 foreign-born physicians made up nearly 8% of the medical workforce [16]. Since 1990, the Russian Federation has been the most important source country for foreign-born physicians in Finland, although since 2006, Estonia has been a growing source country for physicians as well [16]. It has been suggested that foreign-born physicians should be recruited to health care sectors in order to ease the shortage of physicians in Finland [17].
In this study, we first aim to examine whether there are differences in intention to leave between foreign-born and Finnish GPs. Secondly, we investigate the associations of potential psychosocial factors (high job demands, high job control, patient-related stress, and stresses related to teamwork) with intention to leave among GPs. Thirdly, we study whether there are differences in these associations between foreign-born and Finnish GPs.
Method
Data
This study is a part of the Finnish Health Care Professionals Study [18]. The data of the present study consisted of two parts: 1) a random sample of 7000 Finnish physicians (33% of the whole physician population). The response rate was 56% (N = 3780); and 2) of foreign-born physicians including all (N = 1292) foreign-born physicians living in Finland. Of the foreign-born physicians, 553 responded, and thus the response rate was 43%. The term “foreign-born physician” refers to a physician who was born and educated outside Finland, regardless of whether he/she is a foreign national or a person born abroad who now holds Finnish citizenship. The combined data included 4333 physicians of whom 832 (19%) were GPs. Of those, 176 (21%) were foreign-born GPs.
Data collection
First, an URL to the web-based questionnaire was sent to physicians by email during the autumn of 2010 with up to three reminders. Physicians were able to select the English, Swedish, Russian or Estonian version of the questionnaire. Email addresses were drawn from the Finnish Medical Association. Due to the relatively poor response rate of foreign-born physicians, after the first round, printed questionnaires were mailed to foreign-born non-responders in Finnish language only and one more postal reminder was mailed to those who had not answered. Out of 204 internet responses, 10 foreign-born physicians answered in English, 111 in Swedish, 16 in Russian and 20 in Estonian.
Measures
Intention to leave was established by the following question: “Would you like to switch from your present physician’s job to another physician’s job?” The response format was: “1 = No, 2 = Perhaps, and 3 = Yes”. In the analyses, the alternatives “perhaps” and “yes” were merged into one.
Psychosocial factors
High job demands were measured by a 5-item scale derived from Harris’ (1989) stress index, using the question “How often have you been distracted, worried or stressed about . . . ?” The response format was a 5-point rating scale ranging from (1) never to (5) very often. Sample items included “Constant rush and pressure due to in completed work”, “Not enough time to perform work properly” and “Insufficient number of physicians” [19]. The mean response of the scale was scored (as with each of the psychosocial stressors). The Cronbach’s alpha for this sample was 0.87.
High job control was measured by decision authority with 3 items (α = 0.68) derived from Karasek’s Job Content Questionnaire (JCQ) [20]. Decision authority measures the freedom to make independent decisions and possibilities to choose how to perform work. The items were rated with 5-point rating scales, ranging from (1) strongly disagree to (5) strongly agree. The scores were coded so that the higher scores indicated higher levels of control.
Patient-related stress was measured with a 3-item scale (α = 0.79) derived from the health care stress questionnaire [21], using the question “How often have you been distracted, worried or stressed about . . . ?” Sample items include “Patients’ expectations frequently differ from those of health care personnel” and “Patients are unwilling to co-operate and are passive” and the response format was a 5-point rating scale, ranging from (1) never to (5) very often.
Stresses related to teamwork was measured with a 4-item scale (α = 0.80) derived from the Nurse Stress Index [19], using the question “How often have you been distracted, worried or stressed about . . . ?” Sample items include “Human relationship problems in workplace”, “Lack of trust and openness in workplace” and “pressure to work together with other colleagues”. The response format was a 5-point rating scale, ranging from (1) never to (5) very often.
Potential confounders
Potential confounders were demographic factors (age and gender) and specialization status, existence of on-call duty, and labour contract (permanent or fixed-term) and intention to move from the country. The latter was established by the following question: “Have you had plans for moving to work in another country during the next 12 months?” The response format was: “1 = No, 2 = Perhaps, and 3 = Yes”. In the analyses, the alternatives “perhaps” and “yes” were merged into one.
Among foreign-born GPs, potential confounders were also the country of birth (1. Russia; 2. Estonia; 3. Other country), reason for migration and the length of stay. Reasons for migration were defined as ethnic returnees, family-related factors (“the spouse or child of a native of Finland” or “the spouse or child of a migrant resides permanently in Finland”) and an employment-based migrant. The length of stay was categorized as follows: Physicians arrived to Finland 1) before 1989; 2) in the 1990s; 3) 2000–2005; and 4) 2006–2010.
Statistical analyses
First, we calculated the percentages of the intention to leave between foreign-born and Finnish GPs. Second, we analyzed the associations of high job demands, lack of job control, patient-related stress, and stresses related to teamwork (in separate analyses) with intention to leave among all GPs. These analyses were conducted in two steps. In the first step, analyses were adjusted for demographic factors (age and gender). In the second step, analyses were additionally adjusted for work-related factors (specialization status, on-call duty, and employment contract) and intention to move from the country. Third, we tested whether the associations between psychosocial factors and intention to leave differed between Finnish and foreign-born GPs with interaction terms adjusted for age and gender. Finally, the significant interactions were examined by testing the associations separately among Finnish and foreign-born GPs. These analyses were conducted in two steps as mentioned above regarding the second analyses. As sensitivity analyses, we additionally adjusted the analyses testing the associations of high job demand with intention to leave for the country of birth (Russia, Estonia and Other countries), reason for migration and the length of the stay in separate analyses.
All the analyses were conducted with logistic regression models using the SPSS software, version 19.0.
Results
Table I shows the characteristics of the study sample. Among foreign-born GPs, two-thirds of the respondents were female and the mean age was 42.8 years (range 24–69 years, SD = 10.6). More than half of the Finnish GPs were female and the mean age was 43.8 years (range 25–67 years, SD = 12.1). Foreign-born GPs were less likely to be specialized and more likely to work on fixed-term contracts compared to Finnish GPs. There were no significant differences between foreign-born and Finnish GPs in terms of age, intention to move from the country, job demand, high job control, patient-related stress and stresses related to teamwork (Table I). Most of the foreign-born GPs (44%) came from the Russian Federation, and 26% came from Estonia. The group “other GPs” comprised 35 different nationalities. The length of stay varied with the country of origin. Of the Russian GPs, 46% had arrived to Finland in the 1990s, and 35% between the years 2000–2005. Most (77%) of the Estonian GPs had moved to Finland after the year 2000, and 44% arrived after the free movement of labour decision (following the Estonian EU membership) between Estonia and Finland (in 2006). Nearly half of the other foreign-born GPs had moved to Finland after the year 2000. Nearly half (49%) of the Russian GPs migrated to Finland due to family-related factors and 34% were ethnic returners. Of the Estonian GPs, 80% were employment-based migrants, and among the other GPs, family related factors were the most important reasons (65%) to move to Finland.
Descriptive statistics of the study population (N range: foreign GPs: 172–176; Finnish GPs: 635–656).
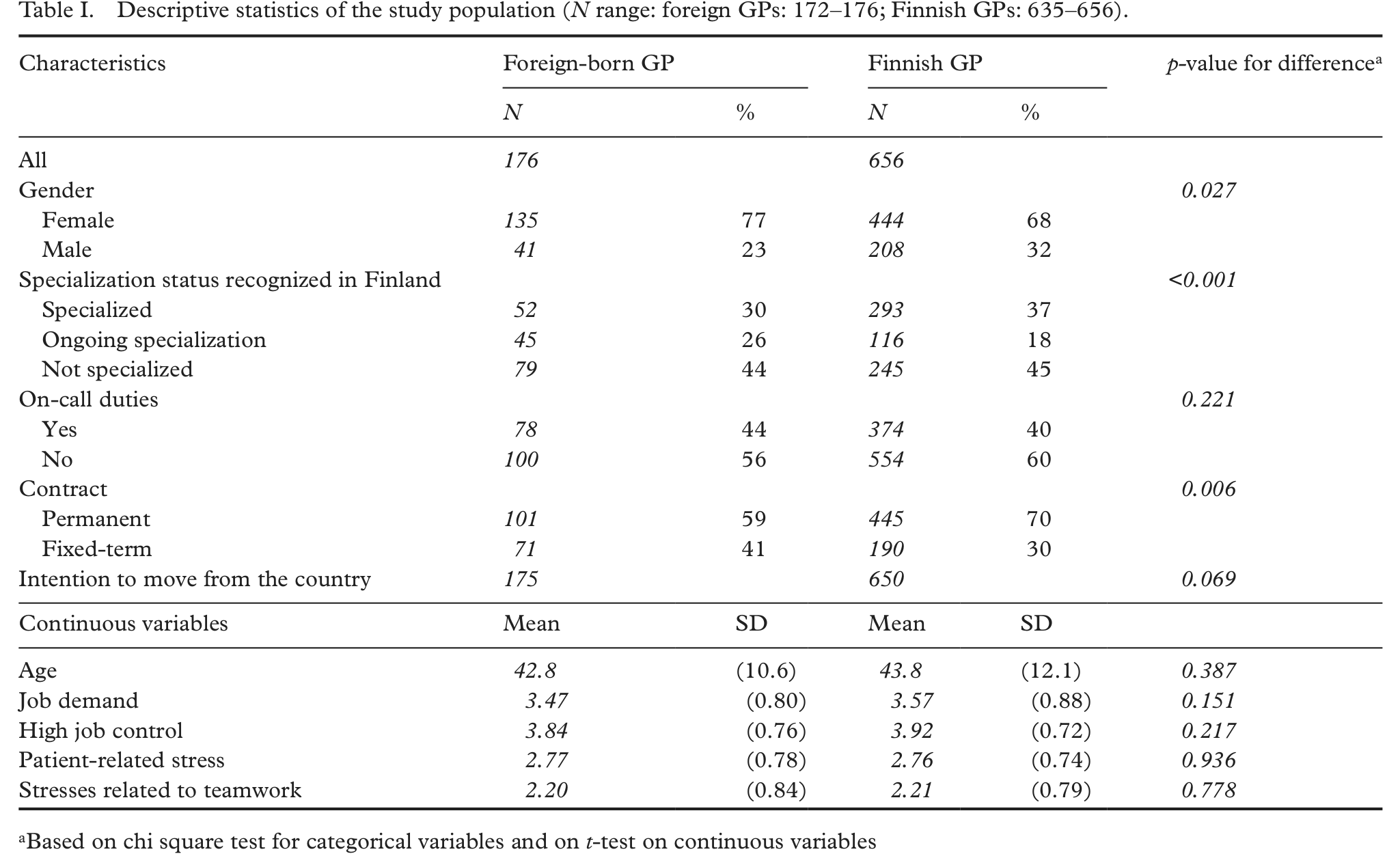
Based on chi square test for categorical variables and on t-test on continuous variables
Of the foreign-born public sector GPs, 59% intended to leave their job. This proportion was smaller among Finnish public GPs (52%). Based on a Chi Square test, the difference was significant (p = 0.050). The associations of psychosocial stress factors (high job demands, high job control, patient-related stress and stresses related to teamwork) with intention to leave were all significant among all GPs (Table II). Those physicians who experienced more psychosocial stress at work more frequently intended to leave, whereas higher control was associated with lower levels of intention to leave. These significant associations persisted after additional adjustments.
The associations between psychosocial work-related factors and intention to leave (0 = no, 1 = yes). Logistic regression analyses with odds ratios (OR) and their 95% confidence intervals (95% CI).
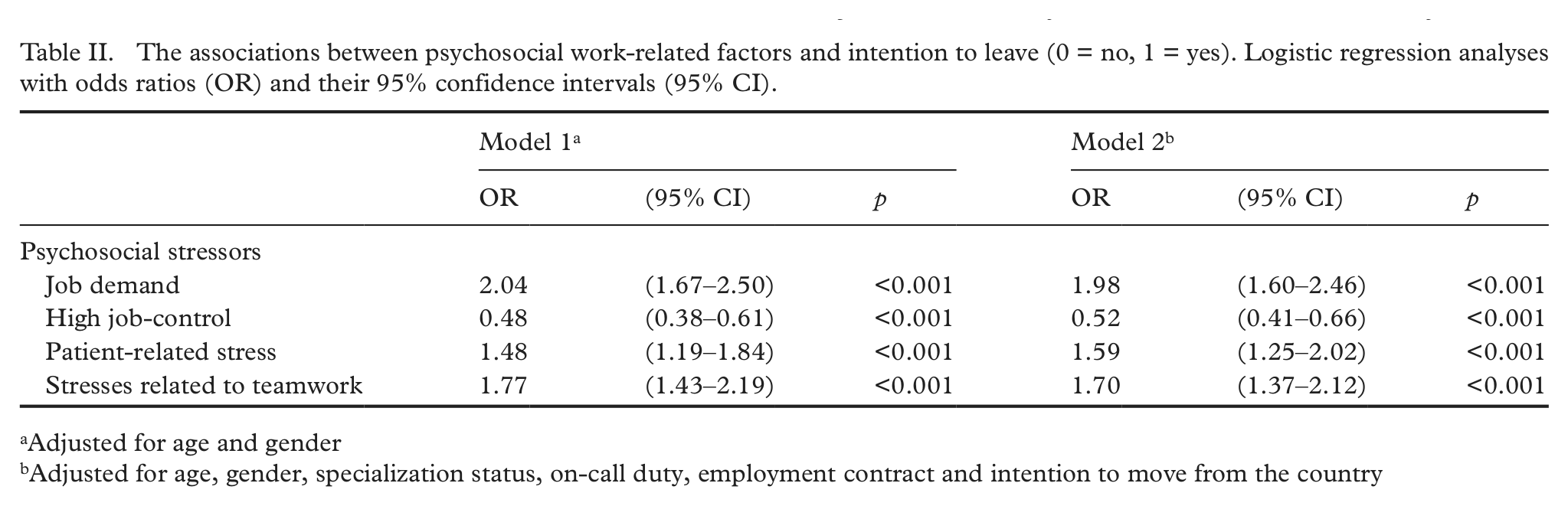
Adjusted for age and gender
Adjusted for age, gender, specialization status, on-call duty, employment contract and intention to move from the country
A significant interaction effect was found between country of origin of GPs and high job control (Wald = 4.85; p = 0.028) and patient-related stress (Wald = 4.91; p = 0.027). Among Finnish GPs, high job control was associated with lower levels of intention to leave, and patient-related stress with higher levels of intention to leave, but this was not the case among foreign-born GPs. Similarly, high stresses related to teamwork were associated with higher intention to leave in Finnish GPs, but not among foreign-born GPs and the interaction was significant (Wald = 4.13; p = 0.042). There were no interaction effects of being a foreign-born or a Finnish GP and job demand (Wald = 0.89; p = 0.345) on intention to leave. Higher job demands were associated with higher intention to leave both in foreign-born GPs and in Finnish GPs (Table III).
The associations between psychosocial work related factors and intention to leave (0 = no, 1 = yes) in foreign-born and Finnish GPs. Logistic regression analyses with odds ratios (OR) and 95% confidence intervals (95% CI).
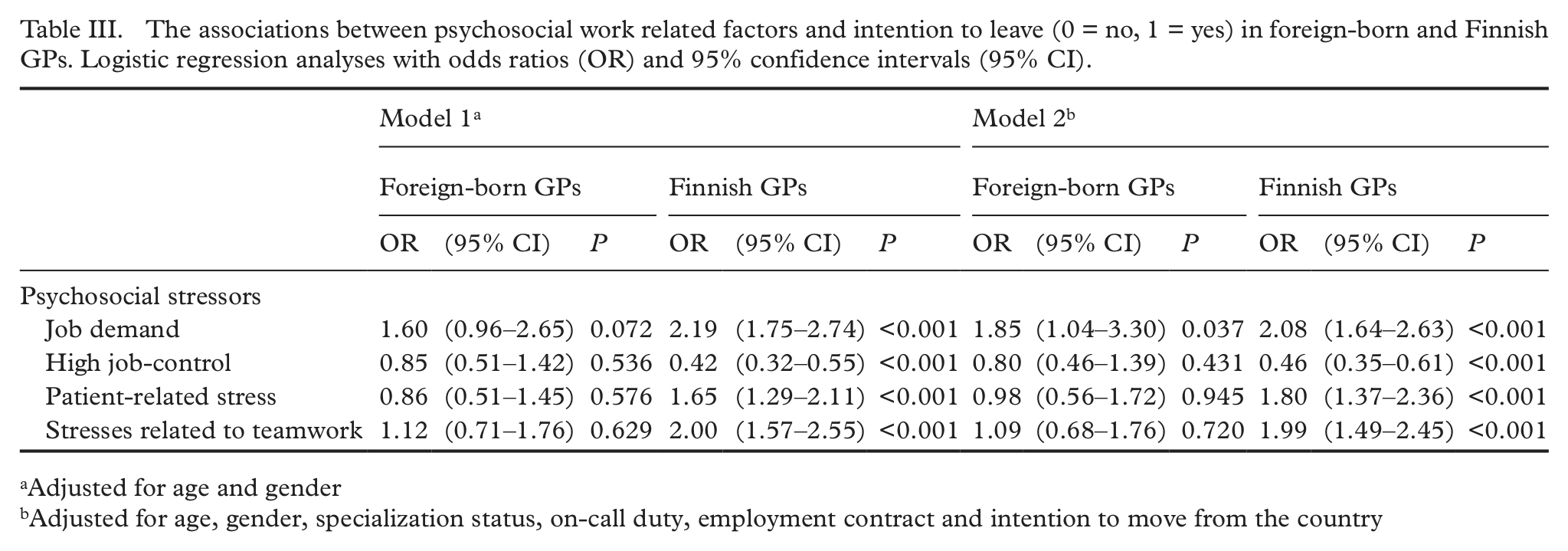
Adjusted for age and gender
Adjusted for age, gender, specialization status, on-call duty, employment contract and intention to move from the country
Job demand was associated with intention to leave after adjusting the model for the country of origin or on the reason for migration (OR = 1.80, p = 0.046; OR = 1.82, p = 0.047). Higher job demands were associated with higher intention to leave in Estonian, Russian and other foreign-born GPs and also among GPs whom arrived to Finland as ethnic returnees, family related migrants or employment-based migrants. After adjusting the models for the length of stay, the association between job demand and intention to leave among foreign-born GPs was no longer significant (p = 0.056).
Discussion
The results of this study showed that more than half of the foreign-born and Finnish GPs intended to leave their job. Previous studies support these results, showing that foreign-born GPs had even more intentions to leave compared to native GPs [22]. As expected, the present study also showed that high job demands were associated with higher intention to leave among GPs, whereas higher control was associated with lower levels of intention to leave. These psychosocial factors correspond to the dimensions underlying the JDC Model, meaning that our results are consistent with previous studies conducted among physicians in different countries [13] and with other occupations [23]. In this study, patient-related stress and stresses related to teamwork were also found to be associated with intention to leave. Similar results have been gained previously showing that patient-related stress was responsible for lower work ability [24] and higher turnover among GPs [25]. Poor teamwork has been shown to increase dissatisfaction [11] and intention to quit among GPs [5].
Job demands seemed to drive both foreign-born and Finnish GPs away from primary care. It has been suggested that in countries where GPs are gatekeepers, their job satisfaction is somewhat lower because they have less latitude to select their case mix [1]. The Finnish health care system is based on gatekeeping and a referral system. In addition, a GP’s area of expertise is especially multifaceted and covers patients of all ages and care provision ranging from preventive health to the management of chronic diseases. Moreover, during the past 15 years, a larger share of the provision of long-term care has been transferred from secondary care to primary care [15]. However, the density of GPs has remained about the same, which has obviously increased workload and job demand among GPs in primary care. These factors may drive GPs, both foreign-born and natives, away from primary care.
The interaction analyses showed that high job control, patient-related stress and stresses related to teamwork were associated with intention to leave differently in foreign-born and Finnish GPs. High job control was associated with lower levels of intention to leave and patient-related stress with higher levels of intention to leave only among Finnish GPs. Similarly, stresses related to teamwork were associated with intentions to leave only among Finnish GPs. It has been widely shown that there are cultural differences in perceptions of job stress [13,26] and that these differences may be affected by national policy, economy, and culture within the country [27].
In Finland physicians must obtain a license from the National Supervisory Authority for Welfare and Health (Valvira) in order to practise in Finland, and non-EU/EEA physicians must complete additional studies and pass an examination, in Finnish, in order to obtain a license to practise medicine. A previous Finnish study showed that the licensing process may be a very difficult and a long-lasting process among physicians arriving to Finland from countries outside the European Union or the European Economic Area [17]. A similar licensing procedure also exists in the US, and international medical graduates (IMGs) must pass two tests including clinical knowledge and clinical skills before being licensed. A medical licence does not guarantee a job; e.g. in the US, typically more certificates have been granted in a given year than the number of residency positions that have been open to physicians educated outside the United States [4]. Foreign-born GPs may have faced difficulties with employment in a new society, also when changing jobs, due to cultural differences such as language difficulties and smaller social networks in the new society. These factors may lead to high experienced psychosocial job stress and strong coping mechanisms among foreign-born physicians because their actual possibilities to change jobs may be very limited. This is also supported by the result found in this study that the length of the stay seemed to attenuate the association between job demands and intentions to leave. Hence, staying for a long time may be an indicator of organizational commitment or job involvement that may be more important than job demand. It is also possible that potential cultural barriers may not exist so strongly among physicians who have stayed longer in a receiving country.
There were no differences in intention to leave between the country of origin or the reason for migration. This may be partly explained by the mobile profile of foreign-born GPs in our data. All GPs lived permanently in Finland and nearly half of the foreign-born GPs had stayed in Finland more than 10 years. Moreover, the larger share of GPs was ethnic returnees or had arrived to Finland due to family-related factors. Their intention to move from the country may be limited. There is no information available of the amount of temporary workers in Finland, however, the amount may have increased since of the free movement policy for the new EU Member States. For example, between 2006 and 2008, Finland granted 266 licences to physicians from Estonia (Valvira) but we lack information about how many of them actually live and work in Finland.
This study made use of a large sample of Finnish physicians, covering a broad age range. The cross-sectional design prevents us from making any causal interpretations and the use of self-report data may inflate the associations found. To minimize problems with self-reports, we have used well-known validated measures that have shown good reliability. It would have been preferable to use the original demands scale from the Job Content Questionnaire [7]. However, the short, three-item scale from the Harris Stress index that was used in our study overlaps conceptually with the original demand scale. In addition, especially when studying occupational groups, such as physicians that generally produce low response rates, short surveys instruments may be better than the longer versions. The version that was used in our study is also widely used in the studies on health care personnel [5]. Self-reports should have affected the results differently in foreign-born and Finnish GPs in order to explain the differences found. The numbers of foreign-born physicians were relatively small, which may have made it difficult to detect significant associations between psychosocial factors and intentions to leave among foreign-born physicians due to low statistical power. However, the interaction analyses showed that the associations were significantly different between foreign-born and Finnish GPs. The attrition was relatively high although our response rates are comparable to recent studies on physicians conducted in Finland [28]. The attrition analyses of the data we used has been published previously [29], suggesting that the women and older physicians are slightly overrepresented but other bias was not found. We are not, however, able to rule out the possibility that our results are under or over estimates of the true associations.
Conclusions
A very high percentage of GPs expressed their intention to leave, and foreign-born GPs’ intention to leave was even higher than that of Finnish GPs. Thus, foreign-born GPs may not alleviate the shortage of physicians in primary care in the long run. Psychosocial factors of intention to leave partly differed between foreign-born and Finnish GPs, and it seems that stress factors had a greater effect on Finnish GPs’ intentions to leave. However, high job demand such as heavy workload, continuous rush and shortage of GPs, seemed to drive GPs away from primary care. A lighter workload could help to attract more GPs, both foreign-born and Finnish, to primary care.
Footnotes
Funding
This study was supported by the Finnish Work Environment Fund (project number 107154) and the Academy of Finland (project number 128002).
Conflict of interest
None declared.