
Abstract
Aims: Insomnia is a large health problem. In some prior studies, positive associations between insomnia symptoms and sickness absence have been observed. There is, however, no previous nationwide cohort study of clinically diagnosed insomnia and risk of incident sickness absence. Methods: Prospective nationwide cohort study based on Swedish population-based registers including all 4,956,358 individuals registered as living in Sweden on 31 December 2004/2005, aged 17–64 years, not on disability pension, old-age pension or on-going sickness absence. Those having insomnia inpatient or outpatient care, defined as having at least one admission/specialist visit with a main or secondary diagnosis of disorders of initiating and maintaining sleep [insomnias] (ICD-10: G47.0) during 2000/2001–2005, were compared to those with no such care. All-cause and diagnosis-specific incident sickness absence were followed during 2006–2010. Incidence rate ratios (IRRs) and 95% confidence intervals (CIs) were estimated by Cox proportional hazards regression. Results: In models adjusted for prior sickness absence, socio-demographic factors and inpatient and specialized outpatient care, associations between insomnia and increased risks of all-cause sickness absence (IRR 1.18, 95% CI 1.04–1.35) and sickness absence due to mental diagnoses (IRR 1.75, 95% CI 1.36–2.25) were observed. After further adjustment for insomnia medications these associations disappeared. No associations between insomnia and risk of sickness absence due to cancer, circulatory or musculoskeletal diagnoses, or injuries, were observed.
Introduction
Sleep problems and sleep disorders are major, and increasing, health problems in the Western world [1,2], including Sweden [3], and in Africa and Asia [4]. Difficulties initiating or maintaining sleep are common symptoms in the population, while a diagnosis of insomnia, defined as complaint of such symptoms or non-restorative sleep that impair daily social, occupational or other functioning [5,6], is less common [5], although the most common sleep disorder [2]. The prevalence of insomnia in the general population ranges from 4%–50% depending on the definitions used, while only 6%–15% among adults is diagnosed with insomnia [2,5–7]. Moreover, direct and indirect costs of sleep disorders are substantial for individuals, employers and society at large [1] as persons with such disorders consult health care more often, report a higher intake of both prescribed and over-the counter medications and experience lower work productivity than good sleepers [1,7–9].
The aetiology of sleep disorders is often multifactorial [10] and studies have shown that such disorders are associated with older age, female sex, work-related stress and low socioeconomic status (SES) [1,6,10,11]. Moreover, insomnia may present as a primary syndrome with no other mental or physical conditions present or manifest as a symptom of another disease (i.e., comorbid insomnia) [2,5–7]. Short-term effects of sleep problems and insomnia have been described as adversely influencing quality of life, well-being and performance, resulting in daytime sleepiness and fatigue [2,10]. Long-term consequences include hypertension, inflammation, obesity, cardiovascular disease, cognitive and intellectual impairment, mental disorders and premature mortality [2,5,12,13], i.e., insomnia seems to be a risk factor for cardiovascular disease and diabetes [14] while both preceding and being a consequence of depression [7,14,15]. Furthermore, insomnia is often comorbid with physical and mental disorders, predominantly anxiety and depression [1,10,16]. Thus, as it is difficult to know whether sleep disorders are the result or the cause, or both, of morbidity a bidirectional link between sleep and health has been suggested [2,17,18].
Sleep problems are typically persistent and relapses are frequent [7]. Chronic, and often untreated, sleep problems may negatively impact an individual’s work capacity [1,7,19], while, in addition, the relation between work performance and sleep quality might be bidirectional [19]. Thus, an association between insomnia and onset of sickness absence might be expected [12,19], potentially mediated by other diseases [2] or poor self-rated health [20]. It has been stressed that the impact of insomnia on public health warrants a better understanding of the economical, social and occupational consequences of insomnia and more specifically how sleep problems contribute to sickness absence [1,7,19]. However, despite substantial evidence regarding the adverse economic and health-related effects of insomnia, few studies have focused on the influence of insomnia on social outcomes, including the individual’s work capacity [5,12,19]. A recent review concluded that insomnia symptoms seem to be associated with increased levels of sickness absence [19], although the evidence is limited [21]. Direct comparisons between prior studies are difficult due to different assessments and definitions of exposures (i.e., sleep problems and/or insomnia) and outcomes (i.e., sickness absence), different data sources, different social security settings and different response rates [14]. Even more importantly, the majority of prior studies are cross-sectional, i.e., limiting the understanding of causality, and/or based on smaller, selected, i.e., not population-based, samples, including only all-cause, not diagnosis-specific, sickness absence and self-reported, not objective, exposure measurements, while not adjusting adequately for morbidity [1,2,5,14]. Thus, the aim of the present study was to – for the first time – examine clinically-diagnosed insomnia and risk of all-cause and diagnosis-specific incident reimbursed sickness absence in a nationwide prospective cohort study including data regarding several potential confounders.
Methods
Study design
This prospective cohort study consists of all 5,620,619 individuals who were registered as living in Sweden on 31 December 2004 and 31 December 2005, respectively, and were 17–64 years old on 31 December 2005. Data from the following nationwide population-based registers were linked by using the Personal Identity Number (a unique 10-digit number assigned to all Swedish residents): 1) Longitudinal Integration Database for Health Insurance and Labor Market Studies (LISA), held by Statistics Swede, including data for cohort definition, potential confounders (i.e., socio-demographic factors), old-age pension and follow-up regarding migration, 2) Micro Data for Analysis of the Social Insurance database (MiDAS), held by the Swedish Social Insurance Agency, including outcome data (i.e., all-cause and diagnosis-specific sickness absence) and data regarding disability and old-age pension, 3) the National Patient Register (PAR), 4) the Swedish Prescribed Drug Register and 5) the Causes of Death Register, all held by the National Board of Health and Welfare, including exposure data (i.e., insomnia), potential confounders (i.e., inpatient/specialized outpatient care and medications) and mortality data, respectively. The study was approved by the Regional Ethical Review Board in Stockholm, Sweden.
Insomnia
Exposure data was based on inpatient and specialized outpatient care (PAR data) where in-/outpatient diagnoses are classified according to The International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10). Insomnia was defined as having at least one admission/hospitalization or at least one specialist visit with a diagnosis of disorders of initiating and maintaining sleep [insomnias]) (ICD-10, chapter VI: G47.0). Inpatient care was based on admissions during 2000–2005 and specialized outpatient care on visits during 2001–2005 (i.e., nationwide specialized outpatient care data, not including primary care, available since 2001). We constructed five different exposure variables regarding insomnia in- and outpatient care with main and/or secondary diagnoses, studied separately and combined, dichotomized a priori into i) no insomnia (G47.0) in-/outpatient care during 2000–2005/2001–2005 (unexposed/reference group) and ii) at least one admission/specialist visit with insomnia (G47.0) during 2000–2005/2001–2005.
The Swedish social insurance system
All adults in Sweden with income from work or unemployment benefits may receive sickness benefits covering up to 80% of lost income if the individual’s work capacity is reduced due to disease or injury. A sickness certificate from a physician is required from the eighth day of a sick-leave spell. Sick pay is provided from the employer for the first 14 days of a sick-leave spell and thereafter the Social Insurance Agency pays sickness benefits. Disability pension may be granted when a disease or injury has lead to permanent work incapacity. Old-age pension is mostly granted at 65 years, but may be granted earlier.
Incident sickness absence
To identify all incident/new sick-leave spells we used the MiDAS, which includes sickness benefits (not sick pay) data for all Swedish residents. Sickness absence outcomes were defined as incident/new sick-leave spells starting during follow-up in 2006–2010. Nationwide diagnosis-specific sick-leave data is available since 2005. Sick-leave diagnoses are classified according to ICD-10. We analyzed all-cause sickness absence and diagnosis-specific sickness absence due to the most common diagnostic groups regarding sickness absence and/or common chronic diseases. Thus, the following main sick-leave diagnoses were studied: i) malignant and benign tumours (ICD-10, chapter II: C00-C97, D00-D48), ii) mental and behavioural disorders (ICD-10, chapter V; F00-F99), iii) diseases of the circulatory system (ICD-10, chapter IX; I00-I99), iv) diseases of the musculoskeletal system and connective tissue (ICD-10, chapter XIII: M00-M99) and v) injury, poisoning and certain other consequences of external causes (ICD-10, chapter XIX: S00-T98).
Exclusions of cohort members
The cohort included 5,620,619 individuals. After excluding 30 individuals who were erroneously registered as alive in 2005, 28,131 individuals with early old-age pension starting before or at 1 January 2005, 563,536 individuals with on-going or newly-granted disability pension in 2005 and 72,564 individuals with on-going sick-leave spells 2005/2006 not ending in 2006, respectively, 4,956,358 individuals were included in the statistical analyses.
Statistical analyses
The cohort members were followed from 1 January 2006 or (if on-going sick-leave spell 2005/2006) end date of on-going sick-leave spell 1 January–31 December 2006, through 31 December 2010, 31 December the year the participant turned 65, date of incident disability pension, date of emigration, date of death or date of incident sickness absence, whichever came first. Incidence rate ratios (IRRs) and 95% confidence intervals (CIs) were estimated by Cox proportional hazards models, using time since entry into the cohort as underlying time scale and the PHREG procedure in SAS, release 9.2 (SAS Institute Inc. Cary, NC). Data were analyzed in crude and multivariable models. The following potential confounders, i.e., known risk factors for insomnia and all-cause sickness absence, respectively, were successively adjusted for: Prior sickness absence, i.e., sickness benefits (in three predefined categories; i) no sickness benefits, ii) 1–179 sick-leave days, and iii) 180+ sick-leave days), age (in 10-year intervals, reference group “17–24 years”), sex (reference group “men”), education (in three categories, reference group “high educational level, i.e., more than 12 years”), region of residence (in three categories, reference group “larger cities”), summarized number of hospitalization days, i.e., inpatient data, and summarized number of specialist visits, i.e., outpatient data (i.e., two variables in three categories: i) 0 hospitalization days/visits [reference group],ii) ≤ median hospitalization days/visits, and iv) > median hospitalization days/visits) and finally medical treatment for diseases of the nervous system, i.e., psycholeptics/insomnia medications, i.e., prescribed and dispensed drugs classified according to the following Anatomical Therapeutic Chemical (ATC) codes; antipsychotics (N05A), anxiolytics (N05B) and hypnotics and sedatives (N05C) (dichotomized as: i) no purchased antipsychotics, anxiolytics or hypnotics and sedatives and ii) at least one purchase of antipsychotics, anxiolytics or hypnotics and sedatives). Prior sickness absence was based on sickness benefits 2003–2005, socio-demographic factors on registration 31 December 2005, inpatient care on admissions during 2000–2005, specialized outpatient care on visits during 2001–2005 and insomnia medications on purchases during July–December 2005 (i.e., nationwide data available since July 2005). Summarized number of hospitalization days/visits was based on main ICD-10 diagnoses only and normal delivery, singleton (080), chapter XVI (perinatal conditions) and chapter XXI (factors of significance for health and for contacts with health care, except for e-codes) were not included. The median for inpatient care was 4 days during 2000–2005 and the median for specialized outpatient care was 3 visits during 2001–2005. Stratified analyses by sex (as female sex is a risk factor for both insomnia and sickness absence) and insomnia medications were also performed. Observations with missing data on any of the covariates included in the models were excluded from the analyses. The number of missing data was, however, few (Tables I–II).
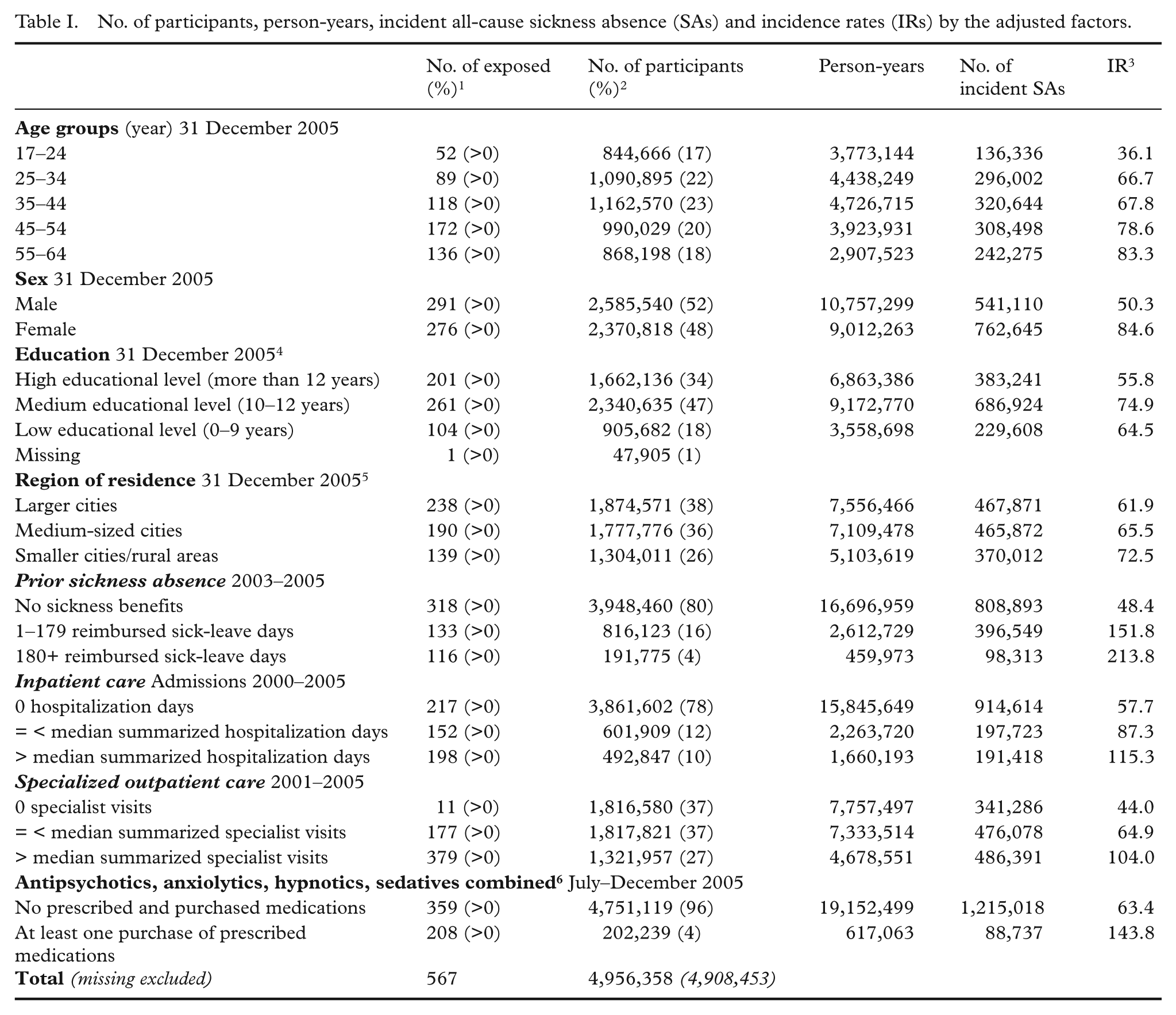
No. of participants, person-years, incident all-cause sickness absence (SAs) and incidence rates (IRs) by the adjusted factors.
Results
Characteristics of study participants
The 4,956,358 study participants together contributed with almost 20 million person-years at risk of incident sickness absence during follow-up 2006–2010 (Table II). Insomnia inpatient/specialized outpatient care, i.e., the exposure, was rare, including in total only 567 exposed individuals (0.01%). The distributions across the adjusted factors for insomnia inpatient/outpatient care combined, including both secondary + main diagnoses [ICD-10 G47.0], are shown in Table I. The all-cause sickness absence incident rate (IR) was very high within all categories of the factors adjusted for and highest in the age category 55–64 years (IR 83.3), among women (IR 84.6), among persons with medium educational level (IR 74.9), among those living in smaller cities/rural areas (IR 72.5), among those with prior sickness absence (IRs 151.8 and 213.8, respectively), among those with hospitalization days (IR 115.3) and specialist visits (IR 104.0) above the median, respectively, and among those having at least one purchase of insomnia medications (IR 143.8) (Table I). Among those having insomnia inpatient/outpatient care, 208 persons (37%, IR 171.7) had at least one purchase of insomnia medications, while 359 persons (63%, IR 100.7) had no such purchase. The most common incident sick-leave diagnoses during follow-up were musculoskeletal and mental diagnoses (data not shown).
All-cause sickness absence
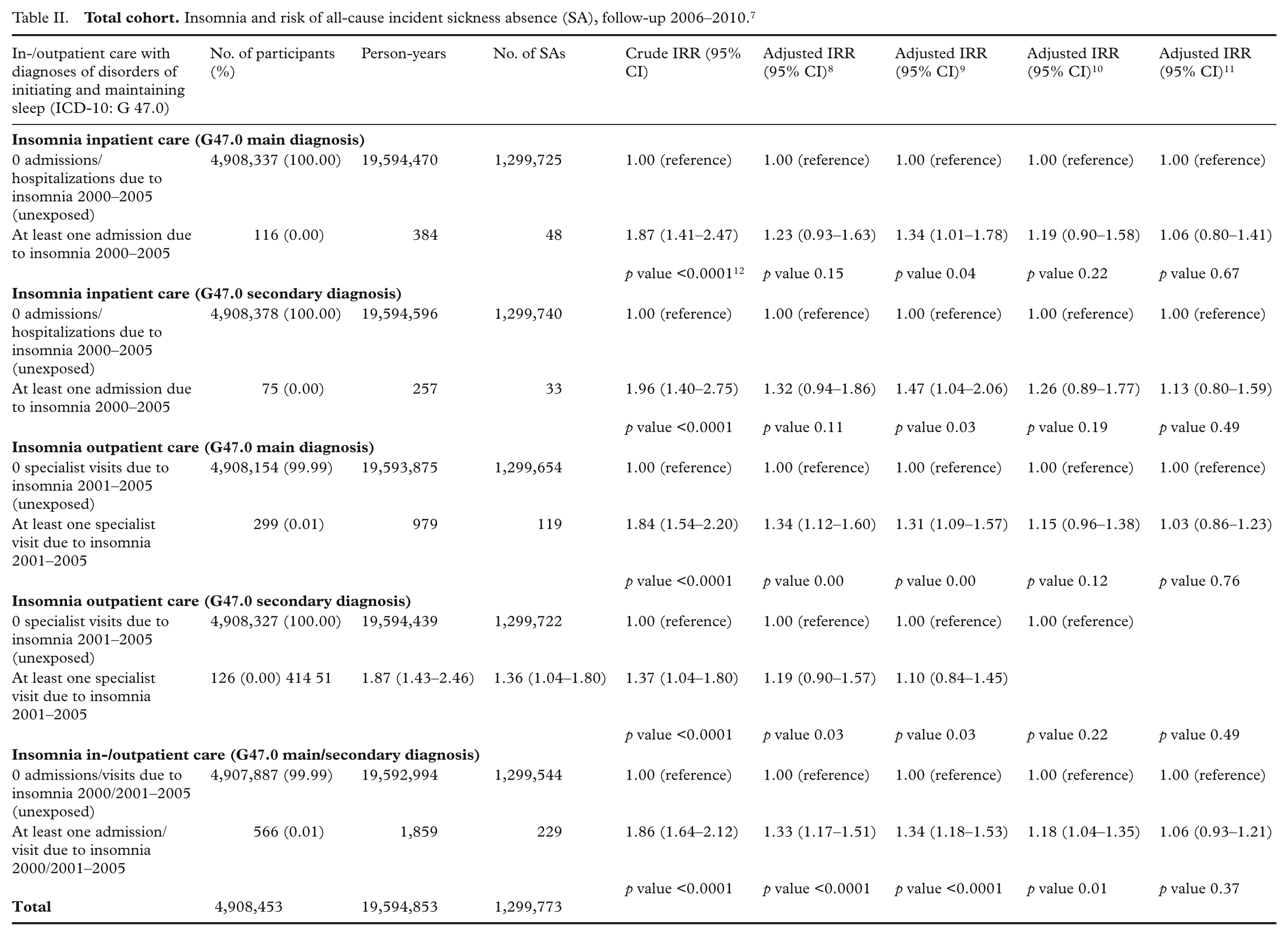
In total, we observed 1,303,755 incident sick-leave spells during follow-up in 2006–2010, more among women (762,645, 58%) compared to men (541,110, 42%) (Table I). Almost twofold increased risks of all-cause sickness absence were observed among persons having insomnia inpatient- or specialized outpatient care regarding all five exposure variables (IRR 1.86, 95% CI 1.64–2.12 [insomnia in-/outpatient care combined, main/secondary G47.0 diagnosis], crude model) (Table II). There were no major differences regarding having insomnia as a main or secondary diagnosis, although the strongest association (crude and adjusted for prior sickness absence and socio-demographic factors) was observed regarding insomnia inpatient care as a secondary diagnosis. After adjustment for prior sickness absence, socio-demographic factors and summarized inpatient/specialized outpatient care, respectively, the positive association regarding combined insomnia in-/outpatient care remained, although attenuated (IRR 1.18, 95% CI 1.04–1.35), while the positive associations regarding the other four exposure variables disappeared. After further adjustment for antipsychotics, anxiolytics, hypnotics and sedatives, the association regarding combined insomnia in-/outpatient care also disappeared (Table II). In addition, we adjusted for hypnotics and sedatives separately (i.e., ATC code N05C; hypnotics and sedatives combined), but the influence on the associations was similar as when adjusting for antipsychotics, anxiolytics, hypnotics and sedatives combined (data not shown).
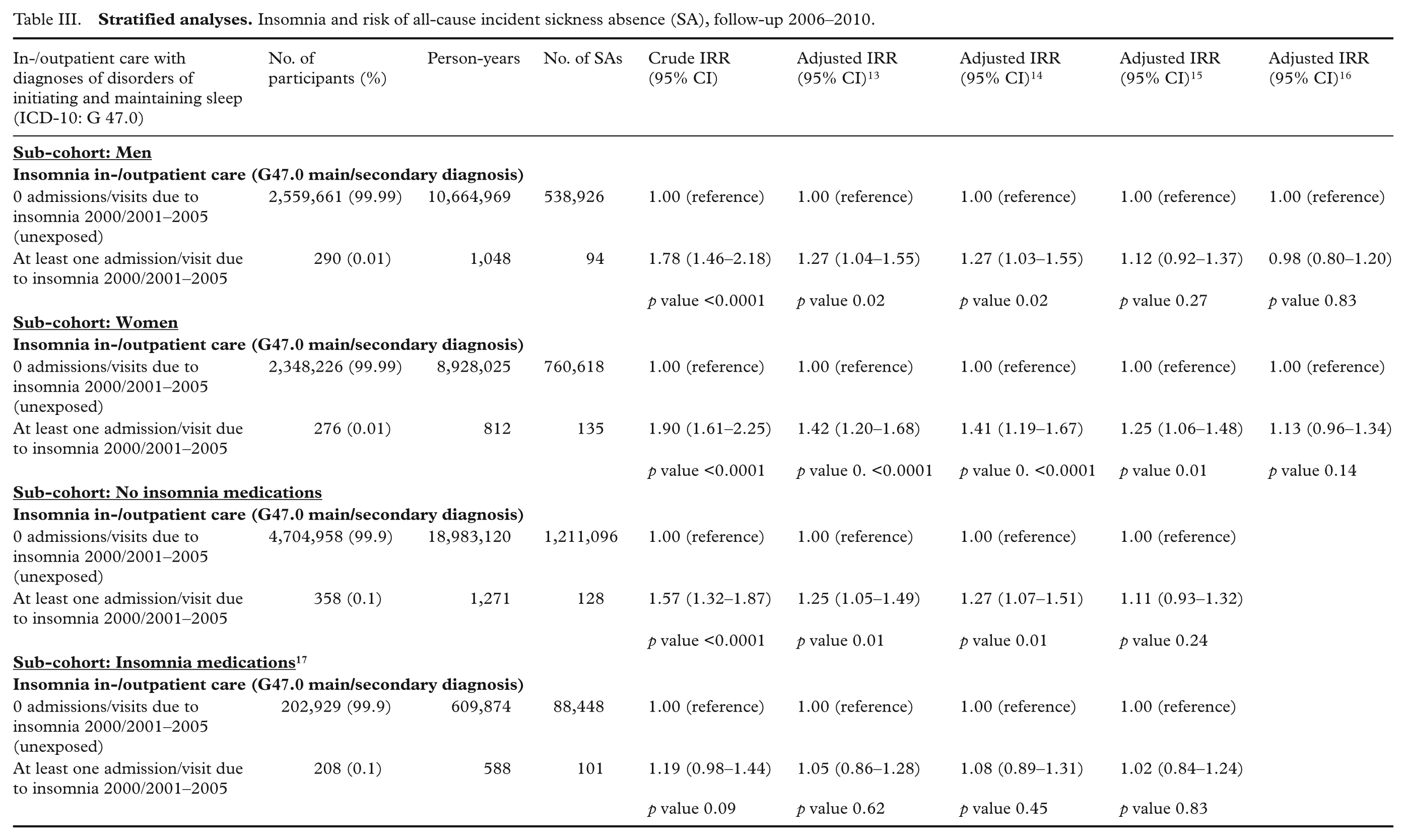
In the stratified analyses, a similarly increased risk of all-cause sickness absence was observed among men having insomnia inpatient/specialized outpatient care (IRR 1.78, 95% CI 1.46–2.18, crude model), but this association disappeared after additional adjustment for inpatient/outpatient care and insomnia medications. Among women, a positive association between insomnia and risk of all-cause sickness absence was observed (IRR 1.90, 95% CI 1.61–2.25, crude model) that disappeared after adjustment for insomnia medications. Among the majority with no purchased insomnia medications in 2005, there was a positive association between insomnia and risk of all-cause sickness absence that disappeared after adjustment for inpatient/outpatient care, while among the 205,239 individuals having at least one purchase of insomnia medications no association between insomnia and risk of all-cause sickness absence was observed (Table III).
Sickness absence due to mental diagnoses
In total, 223,940 incident sick-leave spells due to mental diagnoses were identified during follow-up, although only 61 among the exposed. An almost threefold increased risk of sickness absence due to mental diagnoses among exposed persons was observed in the crude model (IRR 2.82, 95% CI 2.19–3.62 [insomnia in-/outpatient care combined, main/secondary G47.0 diagnosis]). This association remained strong after adjustment for prior sickness absence, socio-demographic factors and inpatient/outpatient care, but disappeared after further adjustment for insomnia medications (IRR 1.18, 95% CI 0.92–1.52) (data not shown in Tables).
Sickness absence due to musculoskeletal diagnoses
In total, 278,109 incident sick-leave spells due to musculoskeletal diagnoses were observed, although only 42 among the exposed. In the crude model, a positive association between insomnia and risk of sickness absence due to musculoskeletal diagnoses was observed (IRR 1.57, 95% CI 1.16–2.12 [insomnia in-/outpatient care combined, main/secondary G47.0 diagnosis]), but after adjustment no association was observed (data not shown).
Sickness absence due to cancer diagnoses, circulatory diagnoses and injury, poisoning and other external causes
In total, 54,093 incident sick-leave spells due to cancer diagnoses, 54,446 incident sick-leave spells due to circulatory diagnoses and 170,736 incident sick-leave spells due to injury, poisoning and other external causes were identified during follow-up. No associations between insomnia and risk of sickness absence due to these diagnoses were observed (data not shown).
Discussion
In this nationwide prospective cohort study, positive associations between clinically diagnosed insomnia and increased risks of all-cause sickness absence and sickness absence due to mental diagnoses were observed even after adjustment for prior sickness absence, socio-demographic factors and summarized inpatient/specialized outpatient care in the total cohort and among women analyzed separately. The most strongly increased risk was observed regarding sickness absence due to mental diagnoses. After adjustment for insomnia medications, these associations disappeared. No associations between insomnia and risk of sickness absence due to cancer diagnoses, circulatory diagnoses, musculoskeletal diagnoses or injuries, poisonings and other external causes were observed.
The population-based nationwide prospective cohort design, including the whole Swedish population aged 17–64 years, entailing high statistical power and excluding selection bias, is a major strength of this study. Moreover, the availability of objectively measured register data regarding clinically diagnosed insomnia, incident sickness absence and covariates with no or very few missing and the possibility to adjust for several potential confounders, including prior sickness absence, in-/outpatient care and insomnia medications, are other strengths as the importance of adjusting for physical and mental disorders when studying consequences of poor sleep has been stressed [22]. The follow-up and detection of incident sickness absence are complete due to the high quality and nationwide coverage of the Swedish population-based registers used [23,24]. Limitations include that for employed individuals only sick-leave spells longer than 15 days were included. Moreover, there is only one study of the validity of sick-leave diagnoses, but this study showed a high validity of register-based sick-leave diagnoses compared to sick-leave diagnoses in medical records [25]. Potential underestimation of the exposure is another limitation, as insomnia inpatient and specialized outpatient care is rare in Sweden since insomnia symptoms often are untreated or treated in primary care and no nationwide primary care data is hitherto available in Sweden. Studies have shown that only 1 in 20 patients with insomnia seek treatment, i.e., mild and even severe insomniacs do not always seek help for treatment [1,6]. This may have resulted in limited statistical power to ascertain weak associations or attenuated the associations observed. Moreover, many individuals with self-reported insomnia symptoms were probably included in our reference, i.e., “unexposed”, group, although our exposure definition may have identified patients with the most severe insomnia. Other potential limitations include that insomnia medications were assessed for 6 months only, and that data regarding adverse life style factors and work-related stress was not included in the nationwide registers, although some of these factors are associated with low SES and should partly be adjusted for by our adjustment for SES based on education.
Some prior cross-sectional studies have found associations between sleep problems and sickness absence [17]. To our knowledge, there are only five previous prospective cohort studies, performed in Denmark, Finland, Norway and Sweden, respectively, of insomnia and/or sleep problems and risk of incident sickness absence [12,14,21,26–28]. These studies were, however, based on smaller and/or not population-based samples and included only self-reported, not clinically diagnosed, insomnia. In these studies positive associations of similar magnitudes as in the present study between insomnia symptoms and risk of sickness absence were found after adjustment for socio-demographic factors, except for a recent prospective Danish cohort study including a representative sample of 6,538 employees where no association was observed after adjustment for self-reported depressive symptoms [14]. Insomnia is associated with several physical and mental disorders and the attenuation and disappearance of the associations after adjustment for inpatient/outpatient care and insomnia medications in our study may be due to insomnia being secondary to e.g. depression or other mental or physical disorders. Other potential explanations are limited power, i.e., there were few individuals with a clinical inpatient/outpatient diagnosis of insomnia, and/or that those with self-reported insomnia symptoms were included in the reference group. Although a modest prevalence of clinically diagnosed insomnia was expected the obtained figures are extremely low and may suggest presence of under-diagnosis. However, as our nationwide data included specialized care (i.e., not primary care) due to insomnia, probably only the most severe cases of insomnia were included. Moreover, this is, to our knowledge, the first nationwide cohort study of clinically diagnosed insomnia and risk of incident sickness absence and future studies are needed. Moreover, our adjustment for insomnia medications might partly adjust for those treated for insomnia or a mental disorder in primary care as well as inpatient/specialized outpatient care. Thus, we may potentially have over-adjusted when adjusting for hypnotics and sedatives as hypnotic drugs are among the most widely used treatments in adult medicine, although the indication may not be sleep-related since physicians often use another diagnosis if they believe that insomnia is secondary to other conditions [29]. In a recent study, a cross-sectional association between self-reported sleep disorders and register-based hypnotics (ATC code N05C) was observed [26] and possible over-adjustment due to co-linearity between clinically diagnosed insomnia and insomnia medications may have been introduced in our study by the adjustment for hypnotics, although the majority of those having insomnia inpatient/outpatient care had no purchase of insomnia medications. In addition, the present study is the first to adjust for prior sickness absence.
In contrast, even after adjusting for summarized inpatient and specialized outpatient care (including, e.g., ICD-10, chapter V; mental and behavioural disorders), we observed a strong positive association between insomnia and risk of sickness absence due to mental diagnoses. Potential explanations for this finding are that insomnia induce health problems that are reflected in increased sick-leave rates [17], i.e., mental disorders might be in the causal pathway/mediators between insomnia and sickness absence, or that insomnia is an early symptom of a mental disorder which may be the underlying cause of both insomnia and sickness absence [17,26], although this cannot be determined from our observational data. To our knowledge, only one prior study, including 1-year follow-up of incident sickness absence of more than 9 days and repeated measures of sleep disturbances, has examined diagnosis-specific sickness absence [26]. In that study, consistent with our findings, a positive association between sleep disorders and sickness absence due to mental diagnoses was found, while, in contrast to the present study, sickness absence due to both musculoskeletal diagnoses and injuries was positively associated with sleep disturbances. This might be due to clinically diagnosed insomnia being rare as well as that for those employed, i.e., the majority of the participants in our study, sickness absence shorter than 14 days were not included and according to the Swedish National Board of Health and Welfare’s sickness certification guidelines, long-term sickness absence due to chronic insomnia is only recommended in exceptional cases.
Among women, but not men, we found a positive association between insomnia and risk of all-cause sickness absence after adjustment for prior sickness absence, socio-demographic factors and in-/outpatient care, potentially explained by female sex being a risk factor for both insomnia and sickness absence. That no association between insomnia and risk of sickness absence was found among those with at least one purchase of insomnia medications might be due to limited power as the point estimates were increased or that sickness absence was more common in the reference group.
In conclusion, in this nationwide cohort study, increased risks of all-cause sickness absence and sickness absence due to mental diagnoses were observed among individuals with clinically diagnosed insomnia, although these associations disappeared after adjustment for insomnia medications. Improved sleep has been associated with return to work after sickness absence [30] and there seems to be a consensus that cognitive-behavioural therapy for chronic insomnia might be more successful than hypnotics [29]. Moreover, it has been suggested that occupational health clinicians should pay more attention to sleep problems to prevent reduced work capacity, sickness absence and morbidity [7,30].
Footnotes
Conflict of interest
None declared.
Funding
This study was funded by the Swedish Council for Working Life and Social Research (grant # 2009-1758 [Stockholm Stress Center] and grant # 2007-1762). The funder had no role in the study design, data collection, statistical analyses, interpretation of data, writing of the article, or the decision to submit the article for publication.