
Abstract
Background:An introduction to a forensic medical homicide database established at the Department of Forensic Medicine in Copenhagen. Content: The database contains substantial clinical and demographic data obtained in conjunction with medico-legal autopsies of victims and forensic clinical examinations of perpetrators in homicide cases in eastern Denmark. Validity and coverage: The database contains information on all homicide cases investigated at the Department of Forensic Medicine in Copenhagen since 1971. Coverage for the catchment area of the department is assumed to be very good because of a medico-legal homicide autopsy rate close to 100%. Regional differences might exist however, due to the fact that the catchment area of the department is dominated by the city of Copenhagen.
Introduction
The Department of Forensic Medicine in Copenhagen is the largest of three, national forensic departments in Denmark. It is an academic institution operating under the Faculty of Health and Medical Sciences at the University of Copenhagen. In addition to traditional academic functions such as research and teaching of students, the department provides services in forensic anthropology, chemistry, genetics, pathology and clinical forensic medicine. These services include medico-legal autopsies and forensic examinations which are performed at the request of the police in accordance with Danish legislation [1]. The catchment area for the department is eastern Denmark and thus services are provided to all police precincts on Zealand, including Copenhagen, the islands south of Zealand and the island of Bornholm, comprising a population of approximately 2.5 million. The medico-legal autopsy frequency in Denmark has been relatively constant at around 2.5% of all deaths during the past decades. This rate is lower than in the rest of the Nordic countries, possibly due to differences in legislation and economic priorities [1]. In Danish homicide cases, however, the medico-legal autopsy frequency is close to 100% and often the police investigation will also include a request for a clinical forensic examination of the (suspected) perpetrator.
At the initiative of one of the authors (PT), data obtained in conjunction with homicide investigations at our department has been registered in a database covering the period from 1971 to present. These data consist of clinical data obtained during autopsies and examinations such as type and distribution of lesions, as well as data pertaining to the circumstances of the homicide, which have been obtained from police reports, crime scene investigations and forensic psychiatric evaluations. On some occasions, Danish newspapers have presented previously unknown information in the homicide cases. This information, when relevant, has been an additional source of data provided police verification of its authenticity.
All individuals in the database are identified by their unique personal identification number (social security number) which enables the linkage of the database with other Danish health registers and social registers on an individual level. Furthermore, victims and perpetrators are linked to each other, which allows for the investigation of features in victims and perpetrators based on common denominators such as manner of death or type of weapon used.
The database belongs to the Department of Forensic Medicine and is not publicly available. However, researchers interested in forensic as well as epidemiological aspects of homicide can access the database in collaboration with researchers at the Department of Forensic Medicine in Copenhagen. In accordance with the Data Protection Act, researchers are required to guarantee confidentiality and anonymity and results must be published at an aggregate level.
Content
According to Danish criminal law homicide covers intended and unintended manslaughter, violence resulting in death, child murder, feticide, euthanasia, and assisted suicide. In a medical context however, deaths are categorized according to manner of death (natural, accident, suicide, or homicide) and cause of death (the disease or condition directly leading to the death) [2]. The material in the database is defined by the medical criteria for homicide and thus includes all cases in which the manner of death is listed as homicide on the death certificate. Traffic crash homicide victims are excluded since manner of death is usually listed as “accident” on the death certificate possibly due to lack of intent of the perpetrator.
All homicide victims and perpetrators who have been autopsied and examined at the Department of Forensic Medicine in Copenhagen since 1971 have been registered in the database. The database contains a total of 1214 homicide cases including a detailed description of 1360 victims and 1572 perpetrators for the period 1971–2010 (both years included). Among the variables registered are manner and cause of death, number and distribution of lesions, toxicology results, information on somatic and psychiatric disease, and background information on upbringing, education, employment, and social network. A complete list of the registered variables is shown in Table I. Whereas personal data, data on homicide circumstances, and health-related data are typically obtained from police reports and autopsies and examinations performed at the forensic department, data on upbringing, education, economy, social network, and criminal record are typically obtained from forensic psychiatric evaluations. In the event that a forensic psychiatric evaluation has not been performed, this type of information will invariably be scarce and fewer variables are registered.
Variables included in the database.
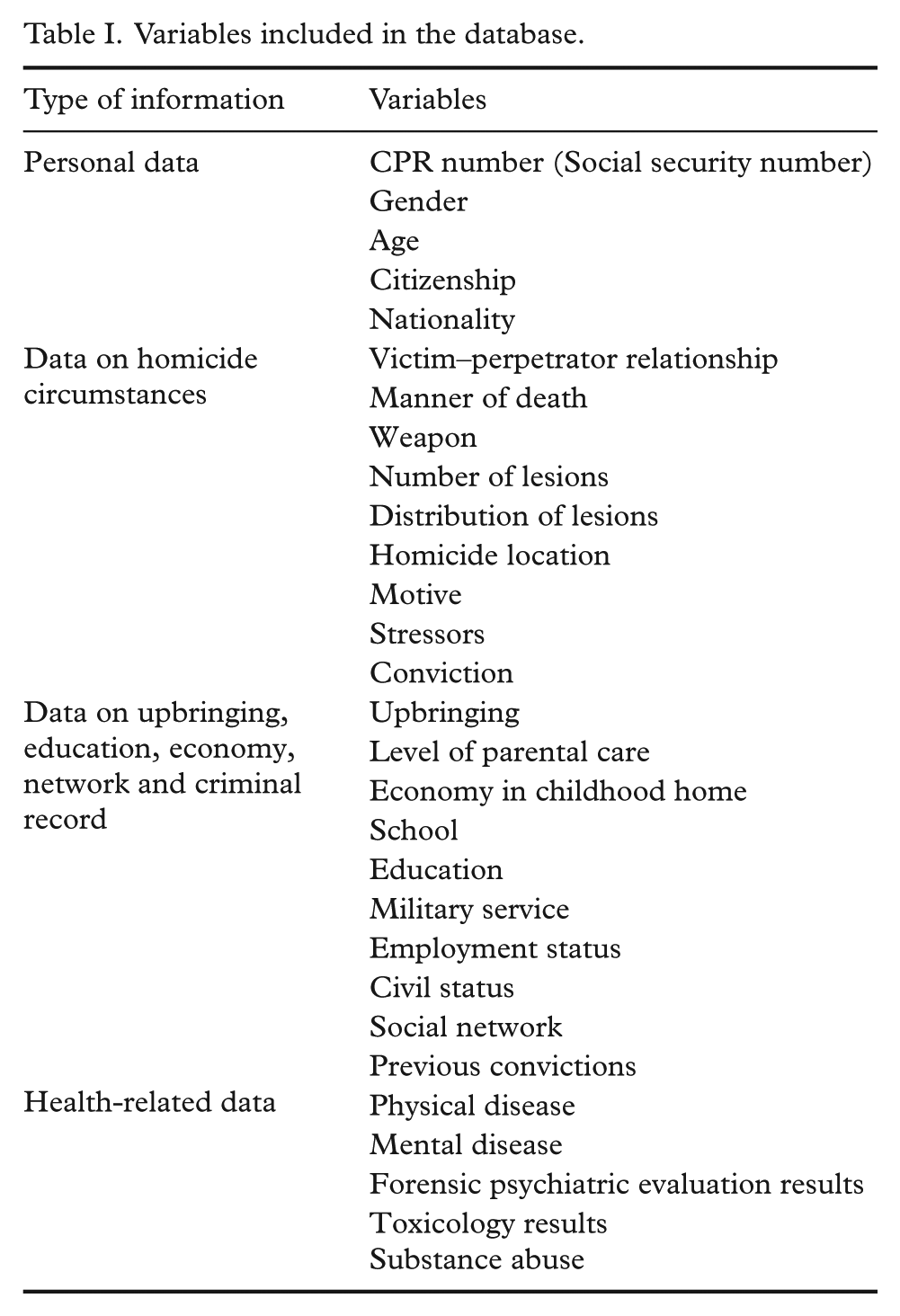
While most of the variables are self-explanatory, some might need further introduction. There is a certain overlap between the two variables Motive and Stressors and in some cases the two variables are identical. However, while Motive refers to the perpetrator’s reason to commit the murder, Stressors refer to one or many life circumstances, which might have added to the perpetrator’s lack of resilience towards committing the murder.
For evident reasons, medico-legal homicide autopsies and forensic examinations are performed in an acute setting which limits the availability of information at the time of the investigation. In a few cases, the perpetrator is never identified and no information is available. In some cases the perpetrator is quickly identified but not apprehended in close proximity to the crime. Depending on the time span between the homicide and the apprehension of the perpetrator, the police might resolve that a forensic examination with the purpose of documenting lesions and sampling DNA evidence is futile. In these cases, the perpetrator is either never examined or examined so late in the course of events that variables such as lesions and toxicology results do not reflect the actual homicide circumstances. In the majority of cases however, a perpetrator has been examined in conjunction with the autopsy.
The four most common manners of death registered in the database in the period 1971–2010 are by blunt force (n=382), gunshot (n=254), strangulation (n=238) and sharp force (n=194) and these cases make up the majority of cases (~88%) in the database. However, because of a medico-legal homicide autopsy frequency close to 100% the database also contains comprehensive data on more uncommon kinds of homicide. These include Danish military personnel killed in the line of duty, honor killings, killings by non-military law enforcement officers, killings of infants and small children, and extended suicides.
Validity and coverage
Approximately 45 homicides are committed each year in Denmark and the majority (~95%) of cases are solved [3]. With a population of 5.6 million inhabitants a crude estimate of the homicide rate is 0.80 per 100,000 inhabitants. At the Department of Forensic Medicine in Copenhagen, approximately 30 homicide victims are autopsied each year although the number varies from year to year. The lowest number of annual homicide victim autopsies in the database is 17 (1975) and the highest is 46 (1985). The database is assumed to have very good coverage for the departments catchment area since the homicide autopsy rate in Denmark is close to 100%. Regional differences may occur though, since eastern Denmark is dominated by the capital city of Copenhagen and therefore extrapolation of results to the rest of the country should be made with caution. It is customary practice in all the forensic departments in Denmark to store data obtained from autopsies and examinations in forensic databases. Thus data on homicides committed in other parts of Denmark is available at the forensic departments in Odense and Århus. However, the database in Copenhagen is the only one that contains a link between the victim and the perpetrator as well as data from forensic psychiatric evaluations.
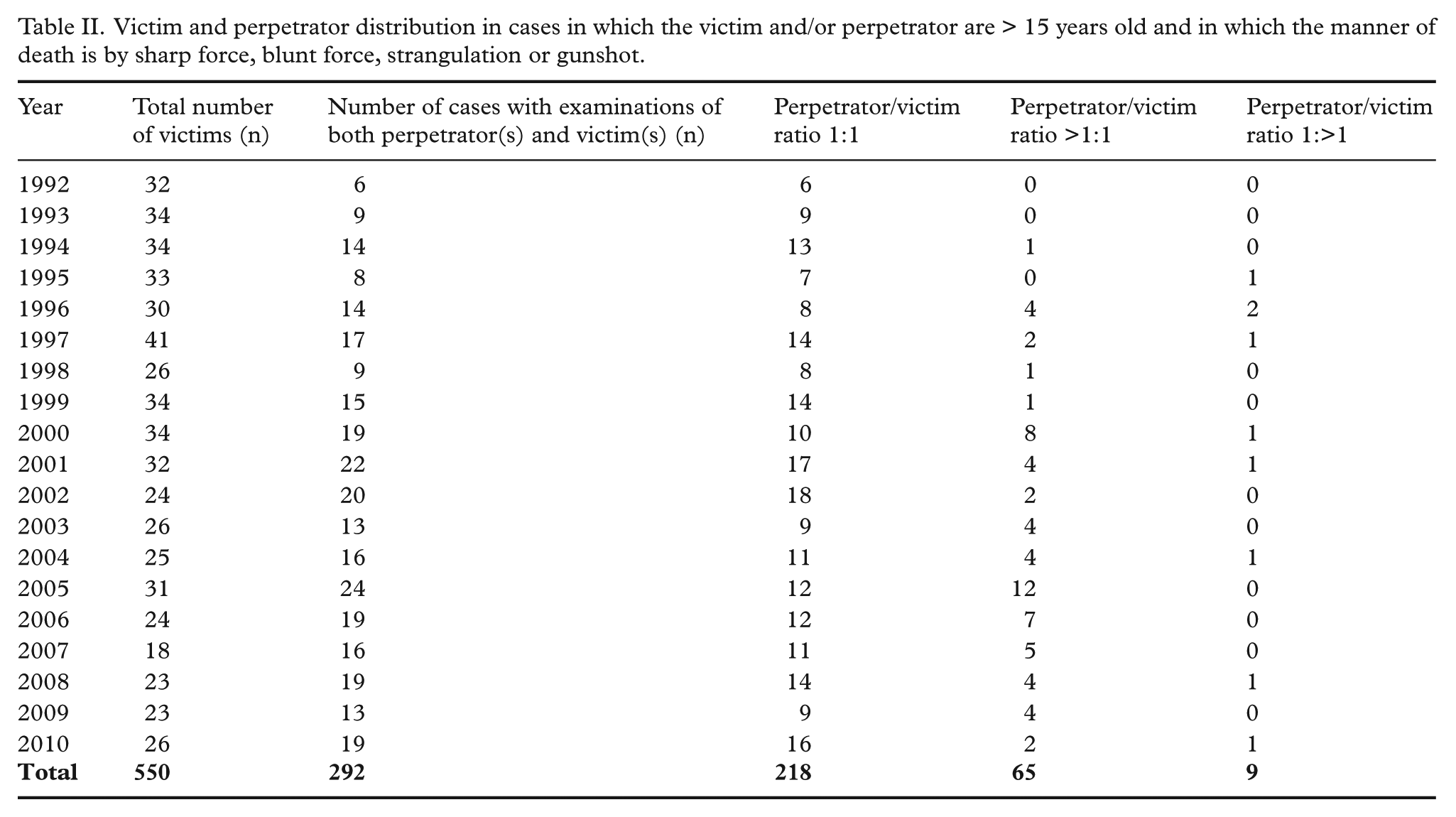
Table II shows the total number of victims and the distribution between victim and perpetrator examinations for the period 1992–2010. Cases shown are those in which both the victim and the perpetrator are at least 15 years old and in which the manner of death is by blunt force, gunshot, strangulation, or sharp force. The total number of victims is relatively constant throughout the period with a slight decline in the last couple of years. According to data from the World Health Organization, Danish homicide death rates showed a decline during the last two decades (1.27/100,000 world standard population in 1992 and 0.70/100,000 in 2006) [4]. Conversely, there is a slight increase in the number of cases in which the perpetrator has been subjected to a forensic examination. This increase possibly reflects a change in the priorities of the police with a more consistent referral of perpetrators to forensic examinations. Although most cases consist of one examined victim and one perpetrator, the database also contains cases with examinations of more than one perpetrator. This raises the question whether one can be sure that the suspected perpetrator examined is also the actual perpetrator of the crime? In most cases, the reason for examining multiple perpetrators is not uncertainty as to who committed the murder, but rather that some of the perpetrators are suspected of accessory to murder. Examples of accessory to murder could be aiding the actual perpetrator with immobilizing the victim or beating the victim in the course of the murder but without delivering the lethal lesion. Additionally, the conviction, or lack hereof, of the perpetrator is registered in the database and serves as a “golden standard” for guilt.
Victim and perpetrator distribution in cases in which the victim and/or perpetrator are > 15 years old and in which the manner of death is by sharp force, blunt force, strangulation or gunshot.
The database was established for surveillance and research purposes. To date, the content of the database has not been subjected to any validation studies. Variables obtained from police reports, autopsies and examinations can be cross-checked with the actual reports which are available in the department archive. Variables obtained from the forensic psychiatric evaluations cannot be cross checked with the actual reports, since those reports have been accessed with special permission by The Danish Medico-Legal Council and are not the property of the Department of Forensic Medicine.
Conclusion
This unique database contains detailed descriptions of homicide victims and perpetrators from the region of eastern Denmark dating back to 1971. The database is thus a valuable tool for researchers interested in forensic and epidemiological aspects of homicide. Individuals registered in the database are identified by their social security number allowing for linkage with other CPR number-based Danish health and social registers. The number of registered variables varies according to availability of information, most notably with fewer variables registered in the event of an unknown perpetrator or a lack of a forensic psychiatric evaluation of the perpetrator. The database has not been subject to any validation studies, but police reports, crime scene investigation reports, medico-legal autopsy reports and forensic examination reports are available for cross reference.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.