
Abstract
Aims: To investigate factors related to unsafe medication management among 75-year-olds during preventive home visits, and to describe the interventions district nurses used. Methods: An explorative study. During a 9- to 12-month period, 36 DNs used the Safe Medication Assessment (SMA) tool during preventive home visits to 75-year-olds who used at least one drug (n=113). Results: One or more factors related to unsafe medication management were identified in 84% of the 75-year-olds. More than 40% used five or more drugs, and 34.5% reported symptoms potentially indicative of adverse effects of their drugs. Nearly 30% had prescribers from more than two medical units, and 7.1% of the older persons were appraised as having reduced cognitive ability. DNs intervened in more than two-thirds of the cases and used a variety of nursing care interventions to improve the safety of medication management.
Introduction
It is essential to prevent factors related to unsafe medication management among older persons and/or to identify such factors as early as possible. Preventive home visits (PHVs) by district nurses (DNs) might provide an opportunity to identify such factors. The general goal of these visits is to prevent diseases, delay the onset of cognitive impairment and promote health [1]. PHVs are currently performed in various parts of Sweden as well as in other countries [2–4]. In Stockholm County, DNs are obliged to offer PHVs to all 75-year-old persons.
The DN is a specialist nurse with a multidisciplinary primary care background who plays an important role in the Swedish primary health care system. Many DNs are accountable for their own patients and work closely with family doctors and other health care professionals at health centres (HCs). Besides providing direct patient care, the DN has a teaching role and helps enable people to care for themselves and their family members. After specialization, which entails one academic year of full-time studies (50 weeks) after the bachelor’s degree in nursing care, the DN has the right to prescribe aids for patients with incontinence and diabetes, technical aids to facilitate daily living and certain drugs[5].
There is little scientific knowledge about the clinical practice of DNs as it relates to safe medication management among older persons. Further investigation is needed in this area because nearly 90% of persons over 75 years of age are on prescription drugs [1,6], and older persons are more prone to side effects of drugs and to drug-related illness than those who are younger [7,8]. Furthermore, drug-related problems cause suffering [7,9] account for nearly 16% of all hospital admissions among individuals over 75 years of age in Sweden [10–12] and impose high costs on society [13].
Safe medication management often means that a patient has agreed to the prescribed therapy and fully understands how to use the drug correctly and safely [14–16]. Furthermore, safe medication management is associated with factors such as patients’ cognitive functions, socioeconomic variables and levels of adherence [14,17]. Factors that negatively affect adherence include poor communication between patients and health care providers, long-term therapies, decline in functional abilities and polypharmacy [7,18,19]. The aims of this study were therefore to investigate factors related to unsafe medication management among 75-year-olds during PHVs and to describe the interventions DNs used.
Methods
Study design and sample
This exploratory study was carried out by DNs from HCs in Stockholm County, Sweden. During a 9- to 12-month period between 2010 and 2011, DNs used the Safe Medication Assessment tool (SMA) [20] during preventive home visits to 75-year-olds who used one or more drugs.
First, HCs that employed DNs who had participated in a 2-day course on health promotion and methods in preventive home visits to 75-year-olds were identified [1]. Of the 175 HCs in Stockholm County, 55 were identified at which DNs had taken the course and which had not been included in any other study about safe medication management for elderly patients conducted by the Centre for Family Medicine.
An information letter about the study was sent to all unit managers at the 55 HCs, and after two reminders, 16 HCs and 50 DNs working at these centres expressed interest in participating. On a later occasion, 14 of the 50 DNs declined to participate because of lack of time for preventive home visits or organizational changes. The remaining 36 DNs were all women working at 16 HCs. Their mean age was 51 years (range 31–64), and the mean length of their experience as DNs was 12 years (range 1–35).
A total of 119 elderly persons were informed about the study by the DNs during routine preventive home visits. Of these, 113 agreed to participate and provided written informed consent.
The Safe Medication Assessment tool
A number of tools have been developed to facilitate the assessment of medication management [20,21,22]. One of these is the SMA tool. The tool was chosen because the findings of a study showed that included items in the tool could be used to identify factors related to unsafe medication management among elderly patients [20]. The SMA assessment is performed by the DN, who fills in the paper assessment form. The tool consists of a 20-item instrument that assesses a patient’s medication management and identifies potential problems (provides a risk assessment). Response alternatives are typically ‘yes’ or ‘no’, but some responses include the options ‘possibly’, ‘in part’ and ‘sometimes’. The first four items are about medication management, and the patient is asked to disclose which prescription drugs and/or over-the-counter drugs they use, including routes of administration, potency and dosage. In addition, DNs ask whether someone assists the patient in dispensing the drug (for example into a dose dispenser), and if so, who (e.g. health care professionals, pharmacists or relatives) and whether the patient receives someone’s help with taking the drug out of its bottle or other container.
The 16 risk-assessment items include domains relevant to safe medication management:
the patient can report or show all drug he or she has been prescribed, including the reason for the drug,
the patient can state the medical condition for which each drug is used,
the patient can report/show the dose and dosage form of each drug,
the patient has prescribers from more than two medical care units,
the patient uses five or more drugs,
in your opinion, the patient has difficulty swallowing his or her drug,
in your opinion, the patient’s has a complex drug regimen,
the patient has methods for remembering to take his or her drug,
in your opinion, the patient has reduced cognitive ability,
the patient stores his or her drug adequately,
in your opinion, there is a suspected risk for interactions between the patient’s drugs,
the patient has symptoms that are more than temporary and could possibly be a side effect/the side effects of drugs,
the patient deliberately takes a dose other than the one prescribed without consulting with the prescribing doctor or DN,
in your opinion, the patient has difficulty understanding Swedish,
in your opinion, the patient has alcohol-related problems, and
the patient thinks he or she has too many drugs.
The information gathered via the SMA tool should be used to help DNs make decisions regarding medication management for decision support. In the SMA assessment, each item represents a potential risk factor and is assigned an allotted number of points, and the total score is an indicator of overall medication safety. The maximum possible score is 28 points; the higher the score, the safer the medication management. However, the SMA manual instructs DNs to consider the impact of every factor (item) that may cause harm to the patient regardless of the total score. This means that each factor in the SMA is important to achieving safe medication management.
Education and support for district nurses
The DNs were informed about the study both verbally and in writing, and attended a two-hour course at their HC that was divided into two sessions of one hour each. The course included dialogue, feedback, formative assessments and case discussions. Learning outcomes included knowing how to use the SMA tool and being able to do the following: identify factors related to unsafe medication management, recognize nursing care interventions that can help ensure safe medication management, describe issues that can pose risks, and document nursing care interventions used to help ensure safe medication management in accordance with the VIPS (Well-being-Integrity-Prevention-Safety) model. In Sweden, the VIPS model has become the most common tool for structuring nursing documentation [23]. After approximately one month, the DNs received an hour-long follow-up session at their HC. Additional support was available by phone or at the workplace, although none of the DNs opted to use either of these sources of support. Codes protected the identities of DNs and older persons. The Stockholm County Council Research Ethics Committee at Karolinska Institutet approved the study (Registration number 2010/5:6).
The 36 DNs received a sample copy of the SMA tool, a manual that explains the purpose of each item in detail, and a sheet with examples of nursing care interventions that can be used to help ensure safe medication management. Furthermore, they were asked to:
ensure that the older persons who used one or more drugs were properly informed about the study and signed a consent form, should they agree to participate,
record older persons’ marital status, living arrangements (whether they lived alone or with at least one other person), educational level and country of birth,
use the SMA tool to assess medication management,
document the results of the assessment and document the nursing care interventions used, and
perform a follow-up evaluation after two to three months, but only if the DN thought the older person’s medication was managed unsafely.
Data analysis
Data were analysed using STATA statistical software version 9.2. Frequencies were described with numbers and proportions with percentages. Prescribed drugs were classified using Anatomical Therapeutic Chemical (ATC) classification codes [24]. Twenty-five was chosen as the cut-off point between two groups of SMA scores for the purpose of statistical analyses, for two reasons. Firstly, the median total risk assessment score was 25 and closest to the 50th percentile of the distribution of SMA score. Secondly, it was important to consider every factor covered by the SMA clinical practise, so no known clinically motivated cut-off point was present. Fisher’s exact test was used to compare differences in factors related to items in the risk assessment between persons with an SMA score of <25 and those with a score of ≥25. The significance level was set at p<0.05.
Results
Characteristics of the older persons
Of the 113 older persons who participated in this study, 53.1% were women, 59.3% were married and 62.8% lived with at least one other person. Furthermore, 47.8% had at least an elementary school diploma and 77.9% were born in Sweden (Table I).
Characteristics of 75-year-olds (n=113) and distribution of Safe Medication Assessment (SMA) score.
Results presented as median with 95% confidence interval.
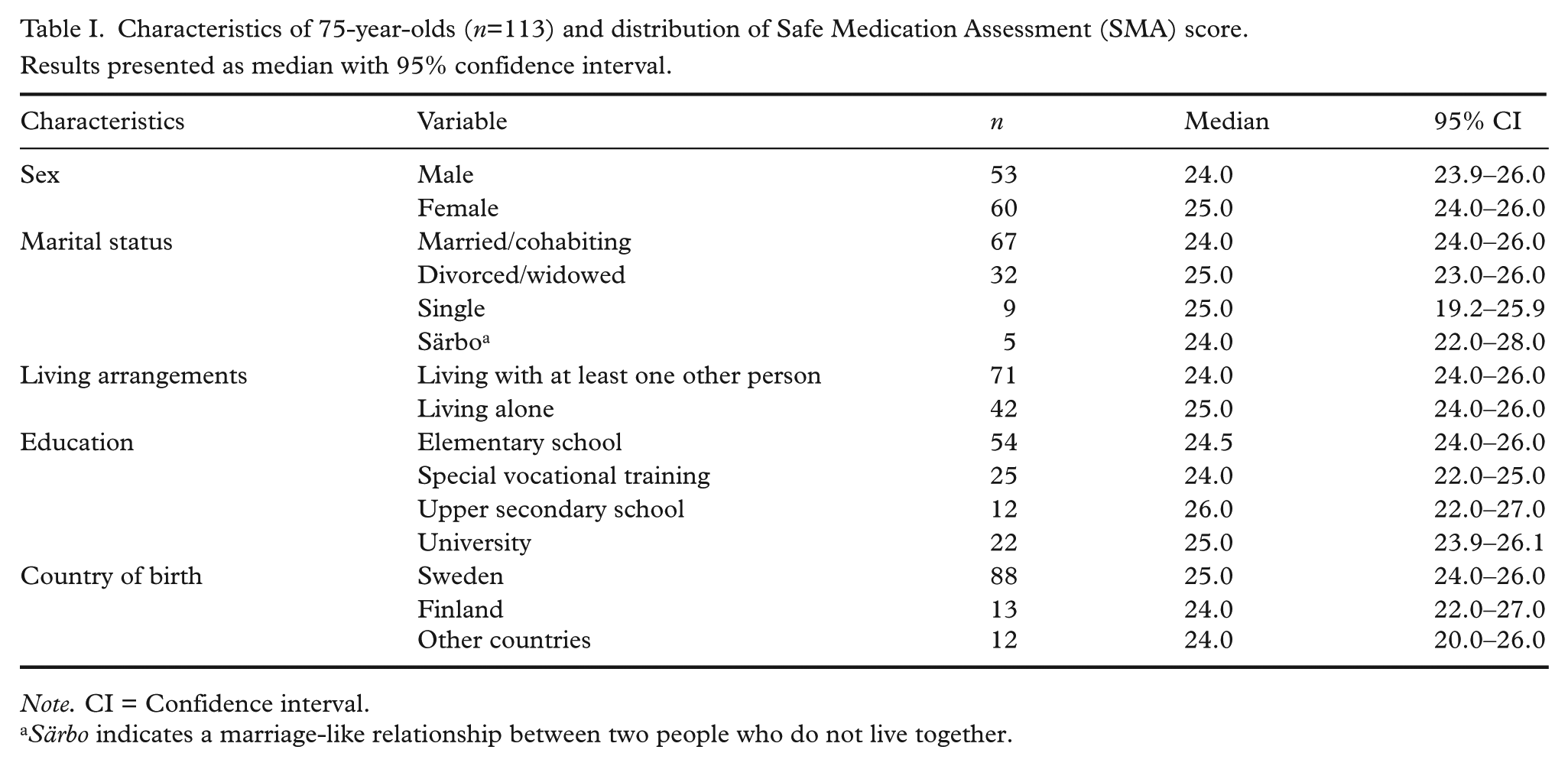
Note. CI = Confidence interval.
Särbo indicates a marriage-like relationship between two people who do not live together.
Medication management
The older persons used a median of five drugs (interquartile range 3–7), no matter whether over-the-counter medications were included in the calculations or not. Of the 113 persons, the percentages who used each kind of drug, classified on the basis of the Anatomical Therapeutic Chemical Classification System, were as follows: 71.8%, drugs acting on the cardiovascular system; 56.7%, drugs acting on the alimentary tract and metabolism; 53.1%, drugs acting on the blood and blood forming organs; 40.7%, drugs acting on the nervous system; 23.9%, drugs acting on the musculo-skeletal system; 19.5%, drugs acting on the genito-urinary system and sex hormones; 15.1%, systemic hormonal preparations, excluding sex hormones and insulin; 14.2%, drugs acting on the respiratory system; 12.4%, dermatologicals; 8.8%, drugs acting on the sensory organs; and 6.2%, anti-infectives for systemic use. A total of 6% used over-the-counter medications.
A total of 6.2% of the older persons had the assistance of health care professionals or pharmacists in dispensing drugs (for example into a dose dispenser), and 2.6% had the assistance of relatives. Furthermore, 2.6% had assistance in taking their drugs from a bottle or dose dispenser.
Risk assessment
The median number of SMA assessments each DN made in this study was 3 (range 1–9). One or more factors related to unsafe medication management were identified in 84% of the 75-year-olds. The two most common findings in the risk assessment for unsafe medication management were that the older persons used five or more drugs and had symptoms potentially indicative of adverse effects (Table II).
Responses to individual items on the Safe Medication Assessment (SMA) tool shown for all 75-year-old respondents (n=113), those with SMA scores of <25 and those with SMA scores of ≥25. Results are presented as numbers (n), percentages (%) and p values; Fisher’s exact test.
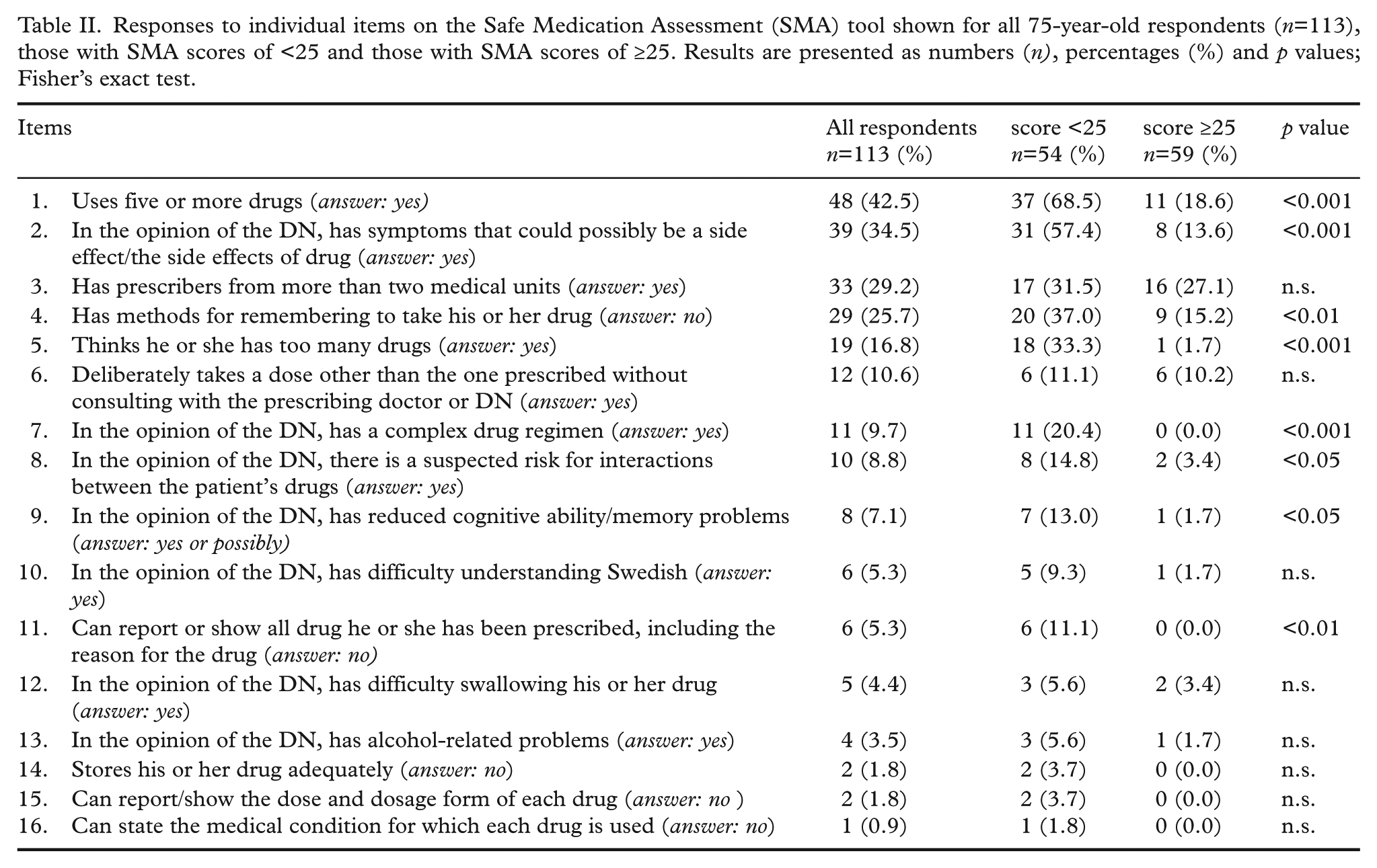
The median total risk assessment score was 25 (range 9–28). A total of 42.5% had an SMA score of <25. The most common factors related to unsafe medication management among those who scored <25 was the use of five or more drugs. Among those who scored ≥25, it was having prescribers from more than two medical units. When responses to individual items on the SMA instrument were analysed (Table II), for eight items, a larger percentage of those with SMA scores of <25 than those with SMA scores of ≥25 had responses potentially indicative of unsafe medication management, such as ‘uses five or more drugs (answer: yes)’.
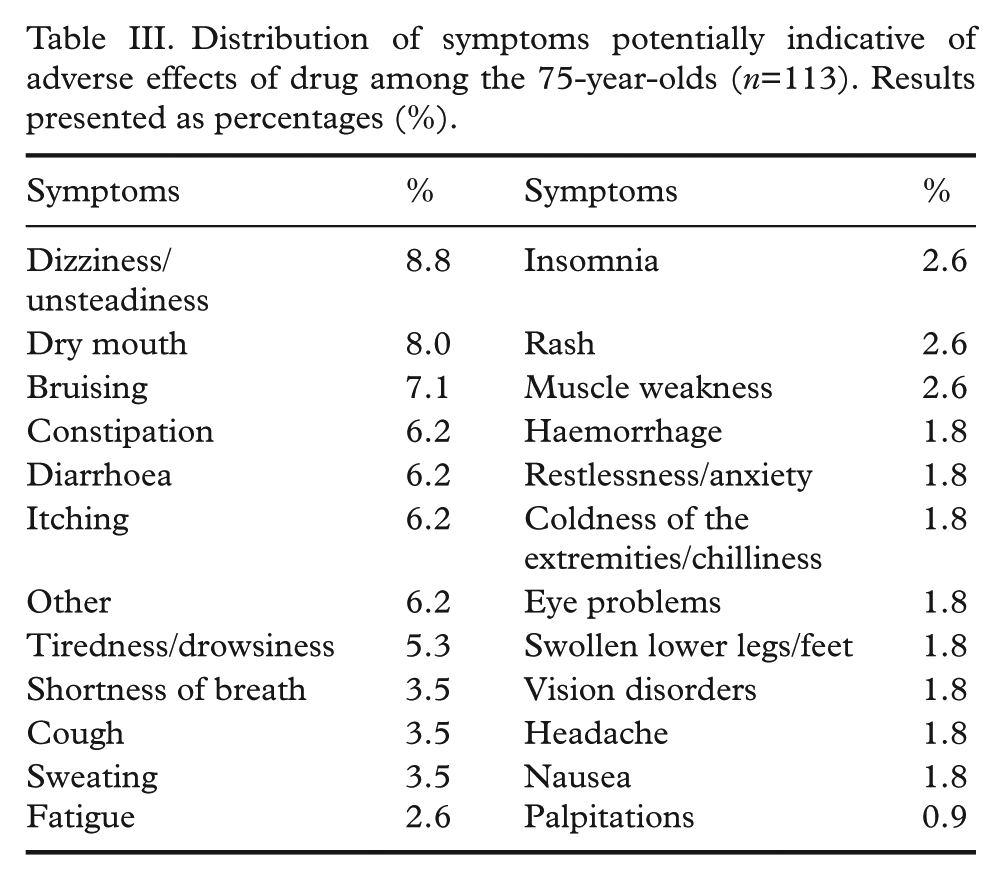
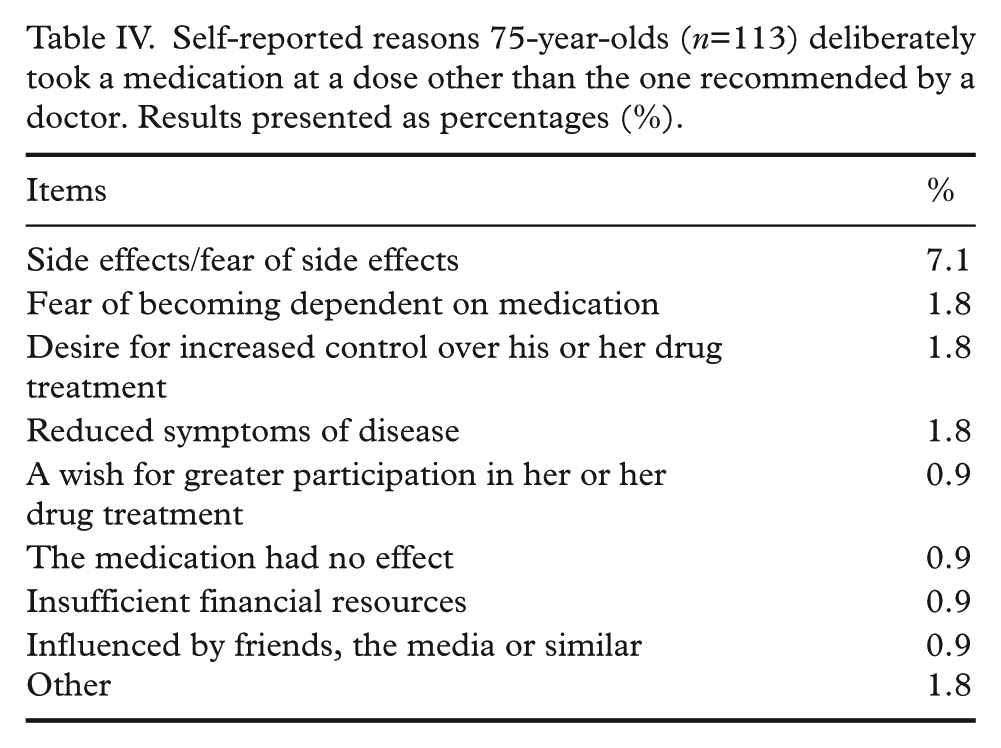
The DNs assessed that, in total 8.8% of the older persons were at risk of interactions and 7.1% had reduced cognitive ability. The most common symptoms of adverse effects of drugs were dizziness (8.8%), dry mouth (8%) and bruising (7.1%) (Table III). The most common cause of deliberately taking a dose other than the one prescribed was fear of side effects (7.1%), (Table IV).
Distribution of symptoms potentially indicative of adverse effects of drug among the 75-year-olds (n=113). Results presented as percentages (%).
Self-reported reasons 75-year-olds (n=113) deliberately took a medication at a dose other than the one recommended by a doctor. Results presented as percentages (%).
Nursing care interventions
A total of 81 older persons received nursing care interventions (71.7%). Several different interventions were used to help ensure safe medication management (Table V). The most commonly used intervention was information and education. However, information and education were used more often with persons who had scored <25 on the SMA than with those who had scored ≥25 (Table V).
Comparison of nursing care interventions in 75-year-olds (n=81) with Safe Medication Assessment (SMA) scores of <25 and those with SMA scores of
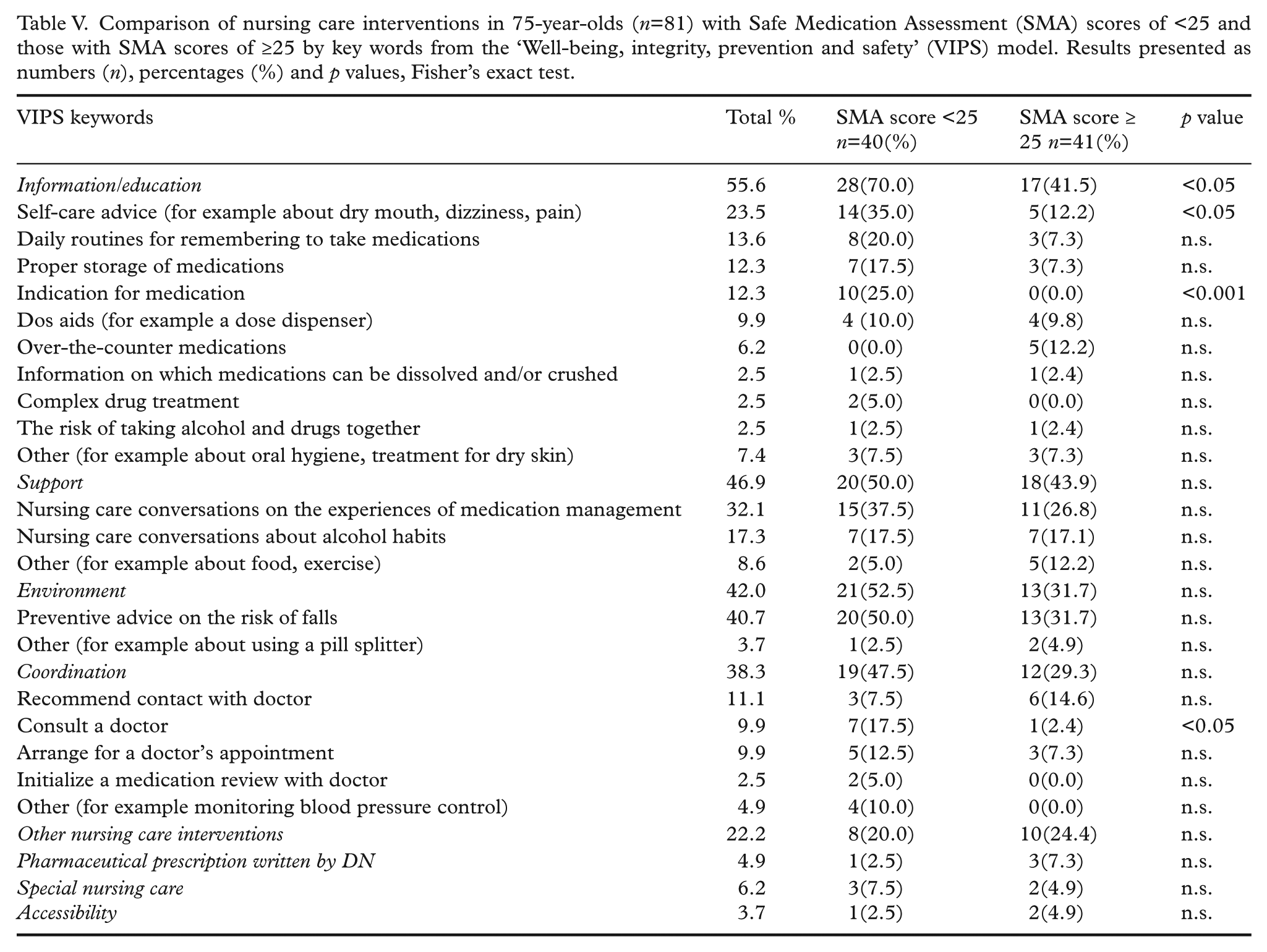
Among the 28.3% of the persons who received no intervention, the most common factors related to unsafe medication management were the use of five or more drugs, lack of methods for remembering to take drugs, and being of the opinion that one was on too many drugs. The median total SMA score among those who received no intervention was 26 (range 15–28). DNs intervened with more than two-thirds of those who had the maximum SMA score of 28 (16%). The most common interventions were nursing care conversations about over-the-counter drugs and alcohol habits and advice on the prevention of falls.
Discussion
In this study, several factors related to unsafe medication management were identified by DNs when they used the SMA tool during preventive home visits to 75-year-olds who used at least one drug. Such factors included polypharmacy, symptoms potentially indicative of adverse effects of drugs, use of drugs prescribed by care providers at more than two medical units, lack of a method for remembering to take drugs, and being of the opinion that one was on too many drugs. Although most of the persons scored high on the SMA, all potential factors identified by the DNs should be taken into consideration to prevent drug-related problems, which might cause unnecessary suffering and hospital admissions. To the best of our knowledge, no other studies of safe medication management to reduce drug-related problems among older persons have looked into the role DNs can play in identifying factors related to unsafe medication management.
Polypharmacy was the most common factor (42.5%) related to unsafe medication management found in the present study. This finding is consistent with the findings of a 2012 study of community-dwelling older persons in Sweden, which found that 39.1% had polypharmacy [25]. The 75-year-olds in the current study took a median of five drugs; cardiovascular drugs were the most commonly used. This median number is consistent with that reported in the 2012 study, in which the mean age of the older persons was 76 years [25]. One explanation for the high median number of drugs found in both these studies might be that in recent years, many older persons have been diagnosed with more disorders and symptoms that can be treated with drugs than in the past. Because polypharmacy increases the risk of adverse effects due to drug interactions [11] and negatively impacts adherence [7], it is important for DNs to be vigilant during preventive home visits to 75-year-olds. DNs are in a unique position to identify these factors. To prevent polypharmacy, the DNs in the present study gave self-care advice (such as advice on diet and exercise as a complement to pharmacological treatment) to nearly 25% of the 81 persons who received interventions. However, it is not known if these interventions were sufficient or if further interventions were needed.
The second most common factor was symptoms that can be indicative of adverse effects of drugs (identified in nearly 34.5% of the 75-year-olds). As polypharmacy is common among older persons, the risk of adverse effects due to drug interactions is also common. The frequency of adverse effects of drugs among persons in this study was lower than the 54% previously reported in a Swedish hospital study [26]. An explanation for the higher percentage in the hospital study might be that the participants were older (mean age 78 years), more frail and on more drugs (a mean of eight drugs) than the persons in the current study. However, it is also hard to differentiate between genuine disease symptoms and adverse effects. Yet, in primary health care settings, DNs can use the SMA tool to closely follow up an older person’s drug use to assess the safety of medication management. They can then use the result of the assessment as a basis for discussion with the prescriber.
The DNs assessed that nearly 7.1% of the older persons had reduced cognitive ability. Many drugs can affect cognitive function and can cause deterioration of memory [27]. Persons with dementia are particularly vulnerable to unsafe medication management, and thus special care is needed in the planning of their care. In the present study, the most common interventions DNs used to support persons with suspected reduced cognitive abilities were nursing care conversations about their drug treatment and coordinating patient contact with doctors. This indicates that using the SMA tool could be a way to identify persons with reduced cognitive ability, and if no such reduction was previously diagnosed, to initiate follow-up checks of the older persons’ cognitive functions.
The DNs intervened in the medication management of more than two-thirds of the persons and used several different nursing care interventions to ensure safe medication management. Education was the main nursing care intervention; it was offered to more than half of those who received interventions. This kind of intervention seems to be of great importance; an earlier study showed that nearly 50% of 75-year-olds who received a preventive home visit exhibited both difficulties in understanding and lack of knowledge about their own health and illnesses [1]. Other studies confirm the importance of patient education about drugs, dosage and adverse effects for better medication management and adherence [28,29]. Research also shows that patients prefer to be offered several choices and to be asked their opinion about a specific treatment [30].
The median score of 25 (out of a possible 28) can be seen as a high score; i.e., in general, medication management was rather safe among the 75-year-olds. Although an overall picture of the safety of a person’s medication management (or the safety of medication management among 75-year-olds in a specific geographical area) is important, every individual factor should be considered by the DNs. The DNs are therefore advised to use the SMA tool like a checklist, intervening to address each factor as needed whether or not the person’s total score is high.
The DNs also identified one or more factors related to unsafe medication management in more than 80% of the assessments. This suggests that during these visits, DNs can be instrumental in identifying important factors related to unsafe medication management, which in turn can be critical to avoiding drug-related problems. About a third of the older persons in the study did not receive any nursing care interventions. The median total score in the risk assessment among these persons was 26. In these cases, the DNs may have chosen not to intervene if the older person did not want to talk about his or her drug treatment with the DN. It is also possible that the DN thought the medication management was safe after taking the result of the SMA assessment into consideration or prioritized other issues during the preventive home visit.
The SMA score cut-off point, 25 (see the Methods section), chosen as a way to learn more about risk factors and interventions common in those with relatively high and those with relatively low scores, proved useful. Persons with SMA scores of <25 were found to have a higher proportion of polypharmacy and symptoms indicative of adverse effects of drugs than those with scores of ≥25. The DNs also assessed that a higher proportion of those with an SMA score of <25 had complex drug regimens and a suspected risk for interactions between. In addition, the findings also showed a higher proportion of nursing care interventions for persons with SMA scores of <25. The main interventions were providing information or education (e.g. on proper storage of medication), providing support (e.g. via nursing care conversations about alcohol habits), discussing the person’s environment (e.g. providing preventive advice on the risk of falls), and coordinating with the person’s doctor to help ensure safe medication management (e.g. initializing a medication review with the doctor).
Methodological considerations
The current study sheds new light on factors related to unsafe medication management among 75-year-olds. It also provides information on nursing care interventions to improve medication management that can be undertaken during preventive home visits to 75-year-olds. Strengths of the present study included the number of participants (75-year-olds) and their wide geographical distribution within Stockholm County (in 10 different communities with varying socioeconomic circumstances). An additional strength was that the DNs in this study had a mean of 12 years’ experience as specialist nurses. The main limitations were the lack of a control group and the need to further validate the SMA tool. Furthermore, this was an exploratory study. As such, it marks the beginning of research on nursing care assessment and intervention aimed at improving medication management among older persons that are undertaken during preventive home visits. Moreover, this study will hopefully add to the awareness of identification of factors related to unsafe medication management and hopefully to safer medication management among older persons. However, there is a need for a randomized controlled study on the subject.
Implications for health care and research
The study provided the participating DNs with the opportunity to learn more about drug use among older persons and about how to use an instrument designed to detect and prevent drug-related problems. Despite taking only a two-hour course at their workplace, the DNs were able to use the assessment tool to identify several factors related to unsafe medication management. When used in preventive home visits to 75-year-olds, the SMA tool therefore seems useful in improving the safety of medication management.
Conclusions
During the preventive home visits to 75-year-olds, one or more factors related to unsafe medication management were identified in more than 80% of those visited. DNs intervened in more than two-thirds of the visits and carried out several different kinds of nursing care interventions to ensure safe medication management. Several factors related to unsafe medication management, and thus relevant to the prevention of future drug-related problems, were identified among the 75-year-olds. Preventive home visits seem to provide a unique opportunity to promote safe medication management. Using the SMA tool in preventive home visits therefore seems to be helpful in improving the safety of medication management among older persons.
Footnotes
Acknowledgements
We thank the participating DNs. We also thank statistician Robert Szulkin for statistical advice and statistician Sven-Erik Johansson for valuable contributions regarding the analysis and presentation of the data.
Conflict of interest
There is no conflict of interest.
Funding
This study was financially supported by Folkhälsoanslaget, Stockholm County Council (reference number HSN 0909-0798).