
Abstract
Aim: Increased food consumption and the related problem of obesity have spurred initiatives to motivate consumers to eat healthier. Some strategies have shown positive but only short-term effects, as consumers or other stakeholders do not accept them sufficiently in the long term. The aim of this study was to investigate opportunities for healthier eating in Norway according to both consumers and other stakeholders. Methods: Five focus-group sessions were conducted with individuals working in the food industry, retail, public health, research and various non-governmental organisations related to food consumption. Topics that were discussed in the focus groups were transformed into a consumer survey, which was conducted with 1178 respondents. Results: The focus groups often indicated a specific responsibility for the food industry to get people to eat healthier. Survey respondents indicated that all actors in the food chain had responsibility for healthier eating in the population, but agreed that the food industry, as well as the health authority, have major responsibilities. Food education was regarded as a favourable strategy in the focus groups and by survey respondents to help people to eat healthier, as were less advertising of unhealthy food and developing new healthy food products. Such strategies should be focused on parents, families, schools and children according to both focus group and survey participants. Implementation challenges include consumers wanting freedom to choose what they eat and consumers wanting food information that is easier to understand.
Keywords
Introduction
Overconsumption and accompanying problems such as obesity and diabetes type 2 have been a concern in the past decades in both developed and developing countries. Overweight and obesity have nearly doubled worldwide since 1980 (WHO obesity factsheet 2013), and currently 1.4 billion adults are overweight. In Norway, approximately 50% of adults are overweight, and childhood obesity (i.e. a body mass index [BMI] > 30) is estimated between 15% and 20% for children between 8 and 12 years of age [1]. Obesity is complex, as it is associated with both excess food intake and low levels of physical activity [2].
In Norway, between 40% and 50% of adults are considered ‘physically inactive’ [3], although only physical activity above the current recommendations may be enough to prevent weight gain [4]. Physical activity is also low in children and adolescents, with an estimated 80–90% of Norwegian adolescents being ‘physical inactive’ [3], while Norwegian children aged 10–12 years are among the most active in Europe [5]. On the other side of the energy balance scale, there has been an increase in food consumption per capita by 27% worldwide between the early 1960s and 2009 [6]. A higher consumption of sausages, hamburgers, boiled potatoes and sugar-free soft drinks and a lower consumption of any type of bread (but wholegrain bread in particular), fruits and berries, vegetables, pasta and rice have been implicated as risk factors for obesity in Norway [7].
These unfavourable consumption patterns have spurred governmental and food-industry initiatives to motivate consumers to eat healthier, including information campaigns, nutritional labelling, environmental changes that increase the availability of and access to healthy foods, improving the healthiness of existing food products and producing new food products with specific health benefits. While these strategies may be beneficial, they are often not evaluated for long-term effects or only have short-term effects on healthier eating. Consumers may not respond as expected to food labelling or other health messages on the package, or to new or altered food products. They may expect a less favourable taste, find the products unnatural or, because many healthy foods tend to cost more than unhealthy foods [8], expect new healthy foods to be expensive [9,10]. The effectiveness of health messages may also depend on environmental factors and socio-economic factors, which makes designing effective health strategies or new food products even more complex. If consumers do not want to eat the healthier products, or they stop eating them after the novelty wears off, then the food industry will not want to develop, produce and sell such food products. Health authorities, researchers and politicians are also stakeholders who may also develop strategies that are not acceptable to both consumers and the food industry, and will therefore not be successful. In other words, strategies to help people to eat healthier may only be successful on the long term if consumers and other stakeholders (the food industry, politicians, health authority, researchers, schools, health-care providers, etc.) can accept and implement such strategies successfully.
The aim of this study was to investigate opportunities for healthier eating in Norway according to both consumers and stakeholders working in the food industry, retail, public health and various non-governmental organisations related to food consumption. Similar studies that involved various stakeholders and/or consumer groups have previously been conducted, but not before in Norway. Such studies identified a need for clearer food information and labelling (Australia, New Zealand, nine European Union [EU] countries), restricting availability and marketing of unhealthy foods (Australia, the USA and nine EU countries), reducing the price of fruit and vegetables (Australia) and a specific focus on children, with more food education and more involvement of parents (Australia, New Zealand, the USA and nine EU countries) as necessary next steps to make the population of the respective country eat healthier [11–15]. However, consumer and other stakeholder attitudes differ per country and culture, and Norway has a different economical structure than the countries described above: it is a small country with only a few large food producers and retailers. Therefore, there is a need to study opportunities for healthier eating in Norway by involving Norwegian consumers and stakeholders.
Methods
This study consisted of two steps. In step 1, focus groups were conducted with participants who represented different stakeholders in the issue ‘opportunities for healthier eating in Norway’. These focus groups resulted in a number of key points, which were transformed into survey questions. In step 2, a survey was conducted with Norwegian consumers. In this article, the results from the survey are compared with the results from the focus groups in order to find agreement between consumers and stakeholders on what the opportunities are for healthier eating in Norway.
Stakeholder focus groups
Five focus group sessions were conducted. The total number of participants was 19, plus three researchers who were present during the focus groups to facilitate and transcribe the discussion. Forty participants were originally approached, of whom 23 accepted the invitation. Four participants did not join any of the groups in the end due to illness or other unforeseen commitments. Participants all had background knowledge that was relevant to the aim of identifying opportunities for healthier eating, were respected individuals within their institutions, covered different angles with regards to healthier eating and represented different parts of the food value chain. Participants included five individuals working in the food industry (retailers and producers), five individuals working in non-governmental organisations who work with food and consumers, one individual working as a market researcher, six individuals working as food, public health or consumer behaviour researchers in universities, and two individuals working as consumer researchers in other research institutes. Fourteen individuals were female and five were male, and the average age was around 40 years. All participants had at least a master’s degree, and eight participants had a PhD.
All focus groups were conducted in two phases. The first phase consisted of presentations that aimed to provide all participants with the same information and a framework for discussion. The information was focused on the overall aim of the research project, which was to find ‘sustainable next generation approaches to food and healthier eating’. Participants received information on the problem with overconsumption and obesity, followed by some examples of food and consumption innovations, as well as animal model research used to understand human consumption and the effects of food on health. The second phase consisted of the group discussions. The discussion was guided by five questions that were set up to structure the focus groups (structure questions). These structure questions asked participants to discuss: (1) what comes to mind when hearing ‘next generation approaches to food’; (2) what incentives are needed to make changes towards healthier eating in Norway; (3) whose responsibility it is to make changes and implement next generation approaches that help people to eat healthier; (4) which strategies that help people to eat healthier could be successful in Norway; and (5) at what level implementation should take place/who the target group is. The discussion section lasted approximately 75 minutes. All participants volunteered to participate without payment and only received food and drinks during the session as a reward.
The discussions of the focus groups were transcribed on site by one researcher. The analysis focused on distilling the key points raised by the focus groups in response to the questions, and the number of focus groups in which these points were mentioned. The key points were either linked to clear opinions of all participants (‘it is important to have food information on all packaging’) or to issues debated by several groups but with different opinions (the role of the government in stimulating healthy eating and limiting access to unhealthy food).
Consumer survey
The key points raised by the stakeholders in the different focus groups were used to create questions for the consumer survey. Selection of topics mentioned in the focus groups for inclusion in the survey was generally done based on the following criteria, in order of priority: (1) all topics mentioned in three or more focus groups were included; (2) questions that the stakeholders had a very strong negative or positive opinion about were added, even if the topic came up in fewer than three focus groups; and (3) questions were added that could help with interpretation of the other questions asked, or to complete the possible answer alternatives.
For structure questions 1 and 2, all topics mentioned in three or more focus groups were added. These included consumer-specific topics, structure of the Norwegian food-industry topics, government involvement topics and topics related to providing information to consumers. Since several stakeholders were members of the food industry, and may thus have had very branch-specific ideas, an exception was made for Norwegian food-industry topics: all topics mentioned in two or more focus groups were added. Topics that were included because of strong feelings from the stakeholders included liking Norwegian versus imported food, current level of food innovation, limiting access to unhealthy foods at schools, employee sports programs, unhealthy eating due to time limitations and the role of appetite during shopping. In addition, for clarity of interpretation of the other questions, questions were added on the use of social media and willingness to pay for preferred but unhealthy food.
For structure questions 3, 4 and 5, the focus was more on providing survey participants with a complete list of possible responsible parties, strategies and target groups. For structure questions 3 and 4, all topics mentioned in two or more focus groups were added. Retailers were added as a possible responsible actor in the food chain, since one focus group that discussed this felt strongly about it. Limiting unhealthy food at school was added as a possible strategy due to strong opinions in one focus group. For structure question 5, since exclusion of possible target groups or using the response alternative ‘other’ would make the interpretation of the results complicated, all target groups mentioned in the focus groups were used in the survey. The elderly, women and overweight individuals were added for completeness.
The consumer survey consisted of 71 questions in total, of which eight were general questions related to consumer characteristics. All the questions were answered on a seven-point Likert scale, with the exception of the questions related to who is responsible for making changes and implementing next generation approaches and at what level implementation should take place: those questions were answered with a four-point scale, ranging from ‘not responsible/not important’ to ‘very responsible/very important’. All questions also had an option to answer ‘I don’t know’. The general questions were used to investigate variation in the following attributes: sex, age, civil status, highest completed education, working status, income and whether the person is the primary buyer in the household. The survey was pilot tested by eight individuals, and small amendments were made afterwards. The survey was done through a market analysis company and was completed online. Participants were recruited by email from a pool of participants to which the company had access, and invitations to complete the survey were sent based on age and sex distribution to balance the sample. At the start of the survey, participants received an explanation of the study, including its voluntary nature, and the click to start the survey was the consent to the study. The survey received 1178 responses within a four-day period. The attributes of the respondents are shown in Table I.
Characteristics of survey respondents (n = 1178).

Data analysis
The focus-group data analysis is described above. Data from the focus groups are presented in the graphs with the consumer survey results. The number of focus groups in which the key point was mentioned is used in the graphs instead of the number of people who mentioned it, as individual statements within a focus group discussion are not necessarily made independently of each other. All survey statements/questions were transformed to positive wording for the sake of analysis and presentations. Cronbach’s alpha for three ‘importance of cheap food’ related questions [16] that were included to test reliability was 0.99.
All statistical analyses were performed using Statistica 11 (StatSoft). Survey statements that were formulated in the same way and thus comparable (structure questions 3–5, themes ‘who is responsible for implementing strategies to help people eat healthier’, ‘what strategies can help people to eat healthier’ and ‘who should be the target group of strategies to get people to eat healthier’) were analysed within structure questions using Kruskal–Wallis analysis of variance (ANOVA) with post-hoc multiple comparisons with Bonferroni correction. The responsible actors, strategies and potential target groups were used as grouping variables, and any comparisons were made between these different actors, between strategies and between potential target groups in order to investigate prioritisation by the participants. p-Values are given as unadjusted p-values when significant after Bonferroni correction.
Effects of gender, work status, education levels, civil status, income and whether the person is responsible for buying the food for the household on the answers were analysed with multiple regressions for all grouping factors within structure questions 3–5, and for the rest questions from structure questions 1 and 2 that the participants agreed on most and least.
Means in the text are shown with standard deviations.
Results
The results are presented per structure question. Responses to questions related to structure questions 3–5 could be compared within structure questions, and these are therefore presented first.
Who is responsible for implementing strategies to help people eat healthier?
Most respondents agreed that all actors in the food chain share responsibility for strategies for healthier eating in the population (mean 3.89 ± 0.38 out of 4; p < .01 for overall ANOVA). In particular, the food industry and the health authority were the major actors that are responsible, while schools were also deemed responsible (means 3.08 ± 0.90, 3.08 ± 0.90 and 2.88 ± 0.90 respectively; Figure 1). Grocery stores, the media and press, and politicians have some responsibility, but they are not the most responsible actors according to the survey respondents (means 2.60 ± 0.91, 2.57 ± 0.95 and 2.29 ± 0.92 respectively; Figure 1). Interestingly, politicians and the media and press were mentioned in three out of the five focus groups as being responsible actors.
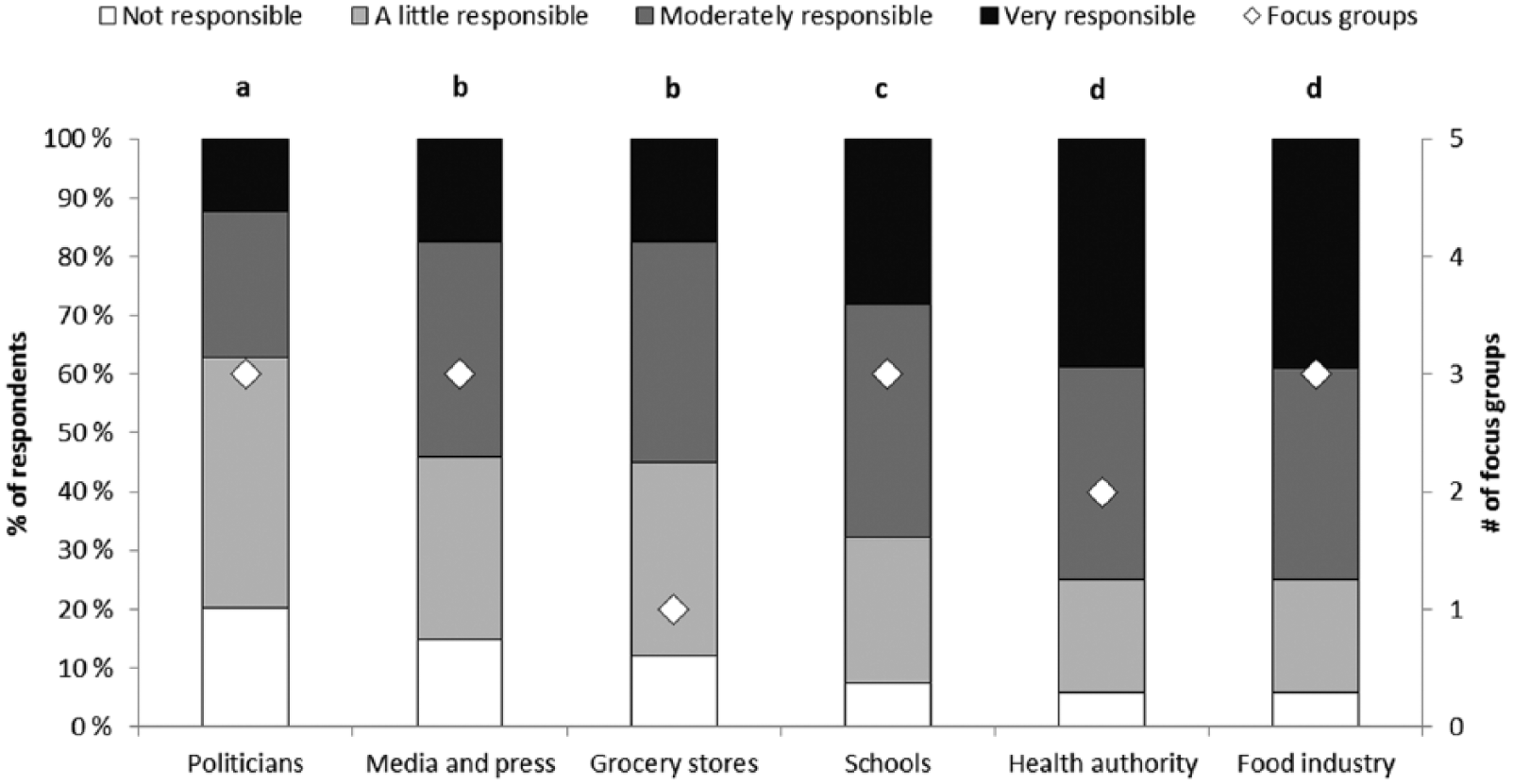
Response to the question ‘Who is responsible for implementing strategies to help people to eat healthier?’ The left y-axis shows the percentage of respondents for each of the answer options. The right y-axis shows the number of focus groups in which each actor was mentioned as being responsible. The letters above the graphs depict statistically significant differences in how survey participants responded to the questions, comparing the different responsible parties, based on the means. Means with different letters are significantly different.
Pensioners and unemployed participants in particular thought that the food industry has a large responsibility for getting people to eat healthier (p = .04). Participants with higher completed education also found the food industry and politicians more responsible than respondents with lower completed education (p = .01; p = .03)
What strategies can help people to eat healthier?
Food education was considered the strategy that had the most potential to get people to eat healthier (mean 5.72 ± 1.21 out of 7; p < .001 for overall ANOVA; Figure 2). Reducing the advertisement of unhealthy food and producing new healthy food products also have the potential to encourage people to eat healthier according to survey respondents (means 5.05 ± 1.34 and 4.96 ± 1.55 respectively). Food education, reduced advertisement of unhealthy food and new healthy foods were also often mentioned by the stakeholders in the focus groups. Eating less processed food, personalised nutrition and functional foods received a more neutral response from both survey respondents and stakeholders (means 4.81 ± 1.57, 4.74 ± 1.31 and 4.72 ± 1.50 respectively). Having fixed portion sizes for food was deemed as undesirable by almost 50% of survey respondents (mean 3.48 ± 1.69).
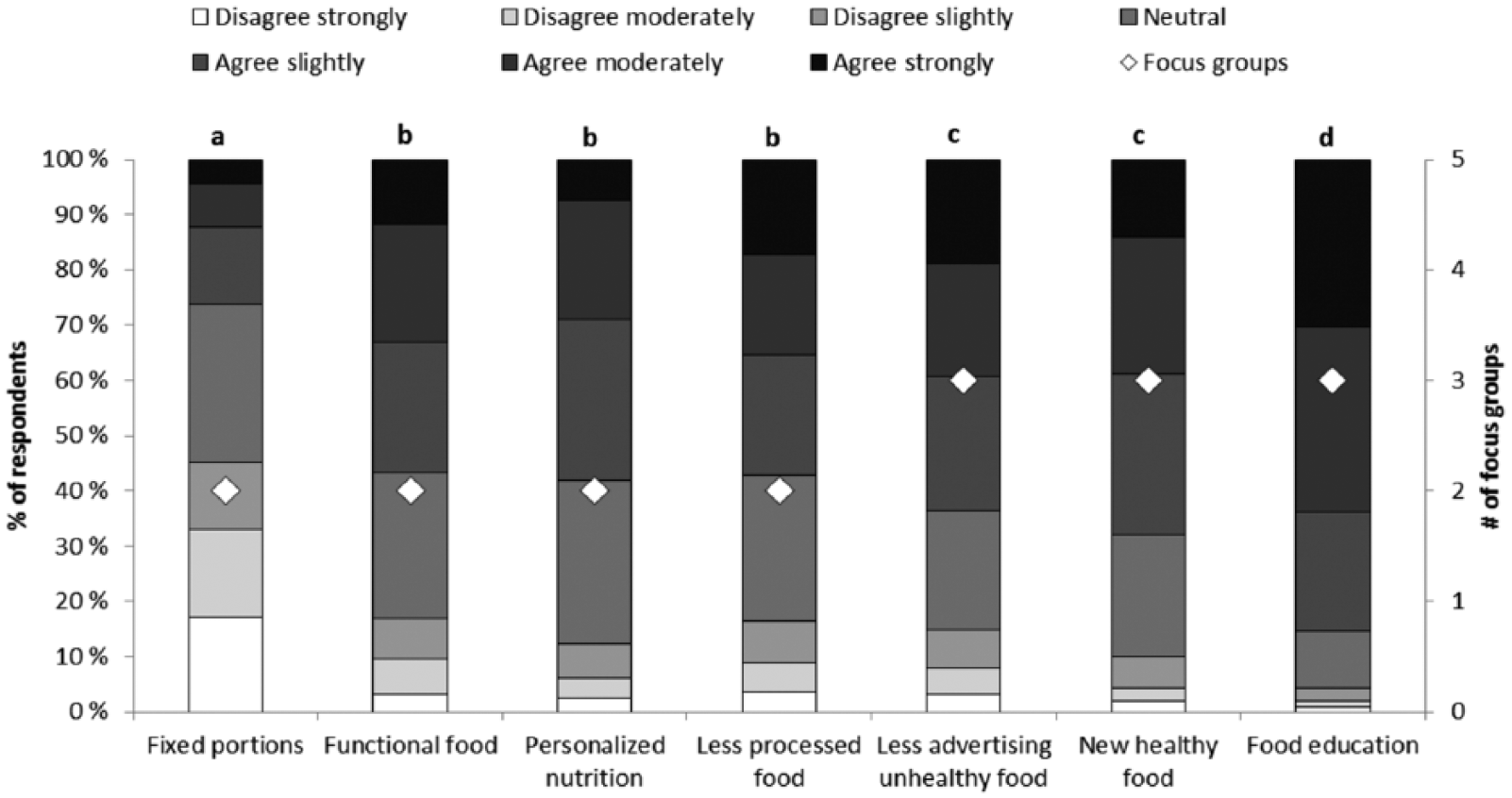
Response to the question ‘What strategies can help people to eat healthier?’ The left y-axis shows the percentage of respondents for each of the answer options. The right y-axis shows the number of focus groups in which each strategy was mentioned as having potential to get people to eat healthier. The letters above the graphs depict statistically significant differences in how survey participants responded to the questions, comparing the different strategies, based on the means. Means with different letters are significantly different.
Women found fixing portion size and eating less processed foods more acceptable strategies than men (p < .01). Respondents with lower education were also more in favour of fixed portion sizes than higher education respondents were (p = .006). Respondents who were the main person responsible for buying food for the household deemed personalised nutrition as more important than those that had no or shared responsibility (p = .02).
Who should be the target group of strategies to get people to eat healthier?
Survey respondents deemed parents the most important target group for strategies that get people to eat healthier (mean 3.57 ± 0.63 out of 4; p < .001 for overall ANOVA; Figure 3). Families and overweight people were also deemed important target groups by consumers (means 3.41 ± 0.70 and 3.36 ± 0.81 respectively) and by most focus groups. In addition, almost 50% of respondents indicated that schools and children were important target groups to focus on (means 3.23 ± 0.83 and 3.17 ± 0.93 respectively), and these target groups were also mentioned in three of the focus groups. Elderly, men, women, low-income groups and customers of grocery shops could be targeted as well, but they were considered less important by the survey respondents (means 2.91 ± 0.93, 2.95 ± 0.85, 2.98 ± 0.82, 2.99 ± 0.93 and 3.02 ± 0.81 respectively). Four out of five focus groups did, however, mention that customers of grocery stores are a good target group.
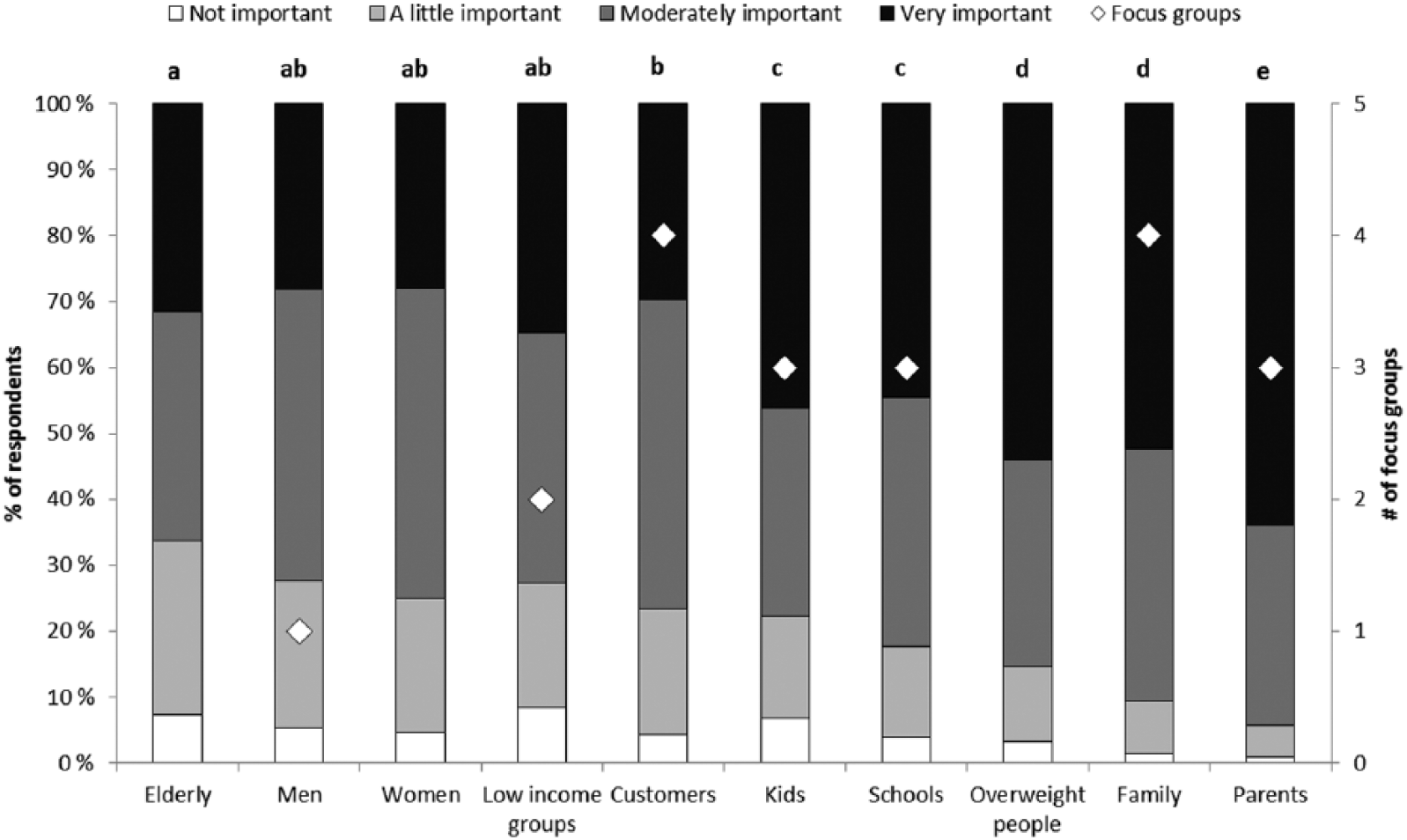
Response to the question ‘Who should be the target group of strategies to get people to eat healthier?’ The left y-axis shows the percentage of respondents for each of the answer options. The right y-axis shows the number of focus groups in which each group was mentioned as being a good target group. The letters above the graphs depict statistically significant differences in how survey participants responded to the questions, comparing the different target groups, based on the means. Means with different letters are significantly different.
Women thought it is more important to focus on the elderly, men, women, customers, families, parents and schools than men did (all p < .05). Respondents with lower completed education thought it is more important to focus strategies on the elderly and overweight people than did people with a higher level of completed education (all p < .05). Low- and medium-income respondents agreed more that families and overweight people are important target groups than did respondents with a high income (p < .05). Stay-at-home parents thought low-income groups were more important targets than respondents with another occupational situation (p = .007).
Other questions
For all questions, the mean response and the number of stakeholder focus groups in which the topic was mentioned by the stakeholders are presented in Figure 4. Many of the responses fell into ‘neutral’, ‘agree slightly’ and ‘agree moderately’ categories, and had a moderate number of focus groups in which the topic was brought up (two to three). Some outliers are found in the top and bottom of the graph. Many people indicated strong agreement with the statements ‘I want freedom to choose what I eat’ (58.9%), ‘Children should not have access to unhealthy food at school’ (47.8%), ‘It is important to have food information on food packaging’ (44.0%) and ‘Expert advice goes in all directions’ (25.9%). Only one stakeholder focus group mentioned that children should not have access to unhealthy food at school, but this was a very well received strategy by consumers. There was a strong consensus on the need for information on food packaging between stakeholders and consumers, while freedom to choose what to eat and confusion regarding expert advice on what to eat were also mentioned several times by the focus groups. Women agreed more than men did on the statement that it is important to have food information on packaging (p < .001), as did low- and medium-income participants compared to high-income participants (p = .02). Stay-at-home parents thought that food information on packaging is less important than the other participants did (p < .05).
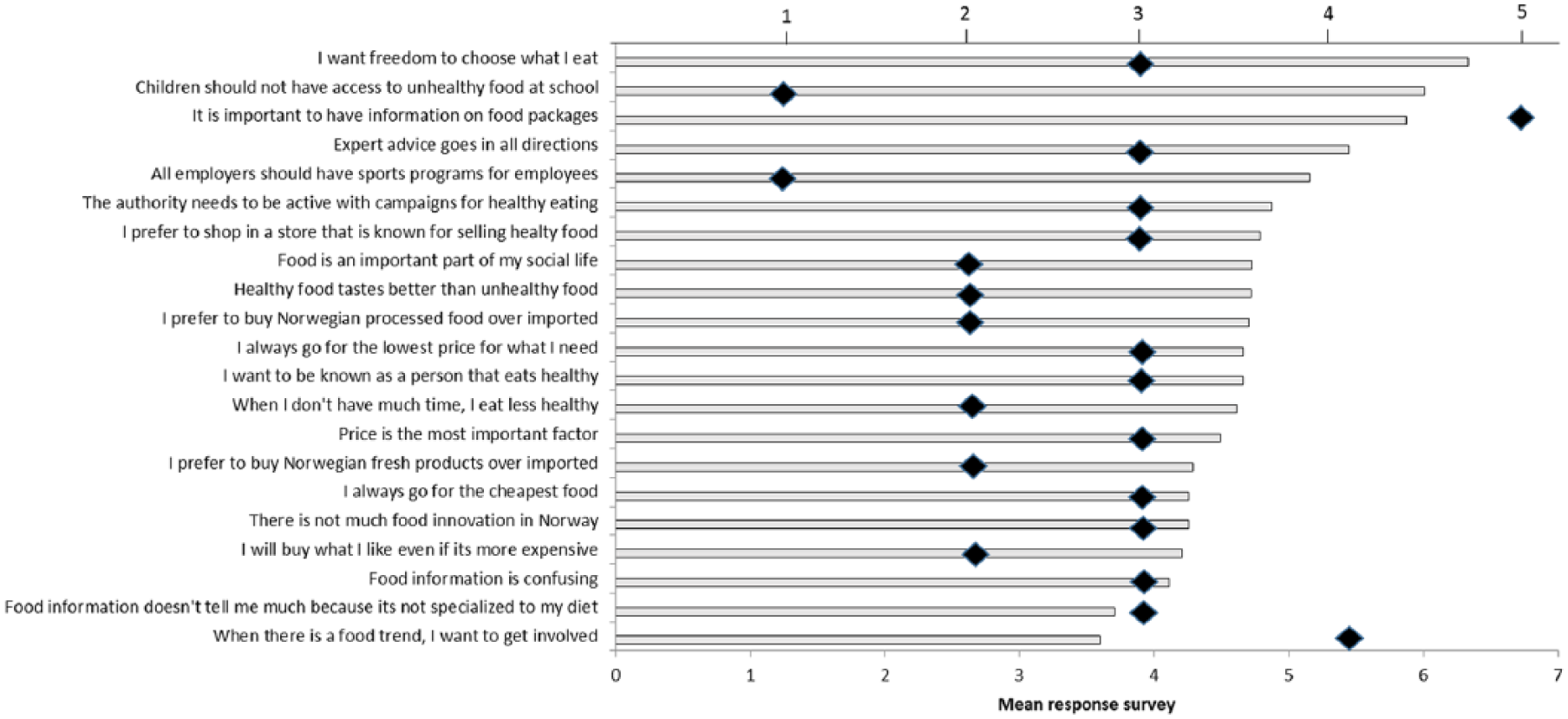
Mean response of survey respondents to consumer-related questions, questions related to the Norwegian food industry, questions related to government involvement and questions related to information for consumers. The bars depict the response of consumers participating in the survey; the diamonds reflect the number of focus groups in which the topic was raised.
At the other end of the scale, 45% of people disagreed strongly, moderately or slightly with the statement ‘When there is a food trend, I want to get involved’. Four out of five focus groups discussed the sensitivity of Norwegian consumers to trends such as the low-carb/high-fat diet and the high willingness to get involved in such trends. Women agreed more than men that they were willing to get involved with food trends, as did participants living together with a partner and with children, and participants primarily responsible for buying food for the household (all p < .05). Pensioners were the least likely to be interested in food trends (p < .001).
The problem that the available food information is not individualised and does not take into account the consumer’s diet, habits and health was another factor that was mentioned several times by the focus groups (three focus groups) but was less agreed on by consumers (36% disagreed, 38% neutral). Men agreed more so than women that food information was not helpful because it is not individualised (p = .001). Pensioners and stay-at-home parents also agreed on this issue more than respondents with a regular job or students, as did participants with low completed education compared to the more educated (p < .05). In addition, participants with lower education tended to agree more with the statement that food information in general is confusing, as did lower-income participants and men, more so than higher-income participants and women (all p < .05).
Discussion
This study aimed to identify opportunities for healthier eating in Norway. It focused on strategies that were deemed viable by consumers, who represent the target group for such strategies, and stakeholders, who develop, implement and evaluate the strategies.
The strategy that was deemed most viable to get people to eat healthier by both consumers and other stakeholders was food education. In addition, consumers and stakeholders agreed that parents, families, children and schools are important target groups in addition to individuals who are already overweight. Consumers in our study did not specify what sort of food education they thought would be effective, but stakeholders mentioned a mixture of school-based education, home economics, learning how to cook healthy food, exposure to healthy foods at school, TV shows with food education and learning how to interpret nutrition advice. Similar studies in other countries also often mentioned a need for food education; targeted either at children or at parents. A need for structured food education at school was mentioned as necessary in stakeholder studies in the EU, the USA and New Zealand [11,13–15]. A study with parents and children identified that children have a general concept of what is healthy and what is not, but they do not understand the consequences of preparation methods and eating unhealthy in general [12]. Parents also indicated that they themselves wanted more knowledge on healthy food choices for their children in the same study. Although food knowledge does not always translate into improved behaviour [17], food education can be a useful tool to motivate healthier eating: some studies have found effects of different education interventions at schools on eating behaviour and body weight [18]. However, there are also examples of education interventions with children and adults that failed to show an effect [19], and only a few examples can be found where food education–related interventions still show positive (yet moderate) effects on weight and behaviour years after the end of the intervention [20,21]. Success factors may include having practical elements in the education such as farm or garden visits, computer tailoring of the education program to the individual, follow-up of the intervention and multi-component interventions that combine food education with, for example, physical activity education, price discounts or restricting access to unhealthy foods at school. Such multi-component interventions have previously been tested in Norway with the aim of increasing fruit and vegetable intake, for example the “Fruits and Vegetables Make the Marks” intervention. This intervention, which included a classroom component, a parental component, and encouragement to join a school fruit programme, did not result in a higher intake of fruit and vegetables [22]. On the other hand, the Pro Children intervention, which included similar components, did result in a significant but moderate increase in fruit intake, both immediately and at the one-year follow-up [23]. A high-intensity curriculum with good participation by teachers, parents and students may have been the reason why the Pro Children intervention was more successful than the Fruits and Vegetables Make the Marks intervention. While food education may be useful for stimulating healthier behaviour, it seems unlikely that education interventions can be designed that will have a major impact on food intake and health.
There was less agreement between consumers and other stakeholders in this study on who is responsible for implementing strategies that stimulate healthier eating. All participants agreed that all actors in the food chain shared some responsibility. However, the media and press and politicians were deemed to have limited responsibility by consumers, but were mentioned often in the focus groups as responsible actors. Less advertisement of healthy food was deemed a viable strategy for getting people to eat healthier. However, it seems that consumers want the responsibility for implementation of this strategy, as well as for implementing food education and new healthy food products, to lie mostly with the health authority and the food industry.
Some challenges for healthier eating were identified in this study as well. Consumers deemed strategies that focus on children, either through food education or through restricting access to unhealthy food at schools, desirable, yet they want to maintain freedom to choose what to eat. Nudging is an example of a strategy that can motivate consumers to make healthier choices without explicitly telling the consumer what to choose and without restricting foods. Nudging can result in healthier food choices, without removing the consumer’s freedom of choice, through small manipulations to the environment [e.g. 24], and may be a strategy to be followed up in Norway. Stakeholders furthermore overestimated the willingness of consumers to follow trends consciously. While consumers may be enticed to try out new products through effective marketing, these trends usually only last for a short time, and do not fit the label of ‘sustainable next generation approaches’. Success will also depend on important properties such as convenience, sensory quality and price.
Another challenge that was identified in this study is providing clear food information to consumers. The majority of consumers indicated that they want information on food packaging. Previous research indicated that consumers are willing to pay more for a product with nutritional information [25,26], although not all types of information have a positive effect on consumer expectations (e.g. health claims [9]). Consumers in the current study also agreed that expert advice is often confusing and contradictory. There is thus a need for consensus amongst experts on what food is healthy in order to be able to communicate a clear message to consumers through different channels. Although our understanding of the effects of dietary components and whole diets on health is increasing, there is still a lot of uncertainty, and due to the long lifespan of humans, it is necessary to explore alternative research methods such as the use of animal models (e.g. [27]) to understand fully the effects of diet on health throughout life.
Providing clear food information to consumers may be even more challenging when aimed at groups with low socio-economic status. Previous studies have shown an inverse correlation between socio-economic status and unhealthy behaviours, including bad dietary habits and lack of physical activity for both adults and adolescents, on both the individual level and the neighbourhood level [28,29]. This study showed that consumers with lower completed education and low incomes wanted food information on packaging just like consumers with higher completed education and income did. However, consumers with lower completed education and, to some extent, consumers with lower incomes found food information to be more confusing and less helpful because it is too general and not individualised (e.g. adapted to what they normally eat and want to eat), more so than consumers with higher completed education did. Development of food information strategies should, particularly for consumers with a lower socio-economic status, focus on information and guidelines that are easy to understand and easy to follow. Front-of-pack labels, such as the Nordic Keyhole label, can help consumers make healthier choices within a segment [30]. Future information strategies could instead also focus on entire meals or diets, and include an element of personalisation.
In conclusion, Norwegian consumers and other stakeholders see the greatest opportunities for getting people to eat healthier in providing better food education, and this education should be aimed at parents, families, schools and children. In addition, producing new healthy foods and reducing advertising of unhealthy foods may help people, including overweight and obese people, to eat healthier. All actors in the food chain share responsibility, but the food industry and the health authority may have a special responsibility to provide consumers with clear, easy-to-understand nutritional information on food products, without limiting consumers’ freedom to choose what they want to eat. It may be useful to collaborate with consumers and other stakeholders in future research efforts in order to shape and implement these proposed strategies. Taking the interests of all parties into account may increase the chance of success and sustainability of strategies that motivate healthier eating.
Footnotes
Acknowledgements
The authors thank Ellen van Kleef for her constructive comments on the survey design, and Qing Wang for comments on the manuscript. The authors also thank an anonymous reviewer for constructive comments on the manuscript.
Conflict of interests
The authors declare that there is no conflict of interest.
Funding
This research was supported by the Norwegian University of Life Sciences to MO. This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.