
Abstract
Aims: The aims of this study were to examine, on a population level, where people die in Sweden, and to investigate associations between place of death and underlying cause of death, socioeconomic and environmental characteristics, with a particular interest in people dying from life-limiting conditions typically in need of palliative care. Methods: This population-level study is based on death certificate data for all deceased individuals in Sweden in 2012, with a registered place of death (n=83,712). Multivariable logistic regression was performed to investigate associations between place of death and individual, socioeconomic and environmental characteristics. Results: The results show that, in 2012, 42.1% of all deaths occurred in hospitals, 17.8% occurred at home and 38.1% in nursing home facilities. Individuals dying of conditions indicative of potential palliative care needs were less likely to die in hospital than those dying of other conditions (OR = 0.73; 95% CI = 0.70–0.77). Living at home in urban areas was associated with higher likelihood of dying in hospital or in a nursing home (OR = 1.04 and 1.09 respectively). Educational attainment and marital status were found to be somewhat associated with the place of death.
Keywords
Introduction
Place of death has become increasingly important in the discourse of quality of end-of-life care [1,2]. The proportion of people dying in their preferred care place has been acknowledged as a quality of care indicator in several countries [3]. Many people prefer to be cared for and die at home, provided that quality of care can be ensured [4]. Prior studies indicate that dying at home, if preferred, contribute to a higher degree of wellbeing compared to dying in institution [1,2,5].
Most western countries have ageing populations. Modern medicine has increased survival and longevity from severe and chronic conditions [6]. A growing number of people now die after years of illness and declining health and functional capacity [7], which implies opportunities for end-of-life care planning. This, and changed palliative care recommendations claiming the right to high quality of care at the end-of-life for all [8, 9], increasingly confront health care systems with challenges of organising and providing timely and appropriate care. Care at the end-of-life, including place of death, has thus become an important public health concern [10].
The place of death varies between European countries [11,12] and across patient groups [13,14]. Factors related to health service organisations, for example, availability of palliative care services and the role of primary care, and cultural attitudes towards death seem largely responsible for these differences [15]. It has also been shown that demographic, clinical and environmental factors contribute to unequal opportunities for individuals to receive home-based care at the end-of-life [16–18].
Apart from a few regional studies [cf. 19, 20], Sweden lacks substantial population-based studies about place of death and the factors that may influence where people die. In 2008, the Dying Well in Europe project, in which Sweden participated with data from 2002, presented place of death results from six European countries [21]. At that time, however, place of death was not systematically registered in the Swedish death certificate register and data for the deceased was therefore derived from the postcode of the locality of death. Moreover, analysis could only distinguish between deaths occurring in or out of hospital, with many deaths in nursing homes likely registered as hospital deaths, thus suggesting that the previously published Swedish results should be interpreted somewhat carefully.
Safeguarding a good ending for dying people and their families is a primary goal of palliative care and a public health responsibility. Quality of end of life is closely tied not only to the care being provided but also to the place of care, often being the same as place of death. Studying place of death on a population level is thus critical for informing end of life health promotive policy, services and public practices.
Objectives
The objectives of this study were to examine, on a population level, where people die in Sweden, and to investigate the associations between place of death and the underlying cause of death, as well as socioeconomic and environmental characteristics of the deceased.
Design and methods
Study population
This population-level study includes all deceased individuals in Sweden in 2012 with a registered place of death (n= 83,712 of a total population of 91,934). The 8.9% missing individuals were (when performing descriptive analyses) randomly distributed within the population.
Death certificate data (sex, age, underlying cause of death and place of death) were obtained from the Swedish National Board of Health and Welfare. In Sweden, physicians complete the death certificates, including ICD-10 codes for underlying cause of death and co-morbidity, and the National Board of Health and Welfare processes all information from the death certificates into the register. Using the national identification number of the deceased individuals, these death certificate data were linked with data extracted from the total population register, the multigenerational register, the historical population register and the register for data on properties, educational attainment and geographical location. Information about the number of hospital- and nursing home beds per 10,000 inhabitants in each health care region was retrieved from the National Board of Health and Welfare.
Variables
The outcome variable for all analyses was place of death, categorised into four distinct alternatives: hospital (unspecified within hospital), home, nursing home, other place (e.g. public places, roads, workplace). Nursing home refers to long- or short-term care facilities in which the majority of residents are old and/or have dementia. It should be noted that a negligible number of younger individuals might also die in long-term facilities designated for severely disabled people, but the death certificate does not distinguish between types of nursing homes.
Underlying cause of death of the individuals was grouped into 11 disease categories according to the ICD-10 classifications. An additional ‘Potential palliative care needs’ variable was created (supplementary material) according to Rosenwax et al. [22], in order to take into account the end-of-life trajectory of the deceased.
Individual and socioeconomic characteristics known to affect place of death were included in the analyses: sex, age, marital status (unmarried, married, widowed or divorced) and educational attainment (operationalized according to the Swedish classification system SUN2000 into ‘no formal or elementary education’, ‘lower secondary education’, ‘higher secondary education’ and ‘higher education’). Additionally, two environmental factors were considered. The first was degree of urbanisation of the area of residence (urban/rural). This categorisation was made by Statistics Sweden, defining urban as ‘an area with continuous settlements/houses, with 200 metres or less between the houses and with at least 200 inhabitants.’ The other factor was number of hospital- (all specialities) and nursing home beds per 10,000 inhabitants in each of the six a health care regions (supplementary material).
Statistical analysis
Percentages were calculated for distribution of place of death by underlying cause of death and other variables. To investigate associations between individual, socioeconomic and environmental characteristics of the deceased and their place of death, multivariable logistic regression analyses were performed. Using place of death as a dependent variable, we developed three complementary models controlling for different combinations of covariates (model 1 = sex, age; model 2 = sex, age, cause of death, potential palliative care needs; model 3 = sex, age, cause of death, palliative care needs, marital status, education, urbanisation level) in order to gain more insight on the respective role of these individual characteristics. The analyses were also stratified (and performed separately) according to the living situation of the deceased in order to understand the patterns of place of death, depending on whether people were living at home or in a nursing home (living at home and dying in hospital vs. dying at home or in nursing home, and living in nursing home and dying in hospital vs. dying in nursing home). For calculations of the model with only individuals residing in nursing homes, we only included the last four age categories (60–95
Finally, in an additional set of multivariable regression analyses, we used the final model (with the same dependent variables and stratifications) as described above, to determine associations between place of death and health care regions, and between place of death and the ratio of available hospital- and nursing home beds, by creating a fourth model, also including the variables health care region, and number of hospital- and nursing home beds/10,000 inhabitants respectively.
Covariates were considered to have a significant association with the outcome if p<0.05. The goodness-of-fit was systematically assessed using the area under the ROC curve (C statistic) as a proxy.
All statistical computations were made using SPSS 22.0 for Mac (SPSS, IBM Corp.). For the mapping of place of death by health care regions we used the Magic Maps software, version 1.4.8 for Mac.
The Regional Ethical Review Board in Stockholm, Sweden approved the study (no. 2013/1745-31/5).
Results
Distribution of place of death
Of all deaths in Sweden in 2012, 42.1% occurred in hospitals, 38.1% in nursing homes, 17.8% at home and 2.0% elsewhere. Of the 454 children (0–17 years) who died, the majority (74.5%) did so in hospitals. Of the 19,812 deceased persons aged 90 and older, 61.9% died in a nursing home facility. Individuals aged 18–29 years were the only age category that more often died at home (44.4%) than in hospital (25.6%).
Overall, 45.0% (n=37,699) of all deaths were caused by conditions indicative of potential palliative care needs. Of these individuals, 40.0% died in hospital, 43.0% in nursing homes 16.0% at home, and 0.9% elsewhere (Table I).
Distribution of place of death in Sweden, 2012.
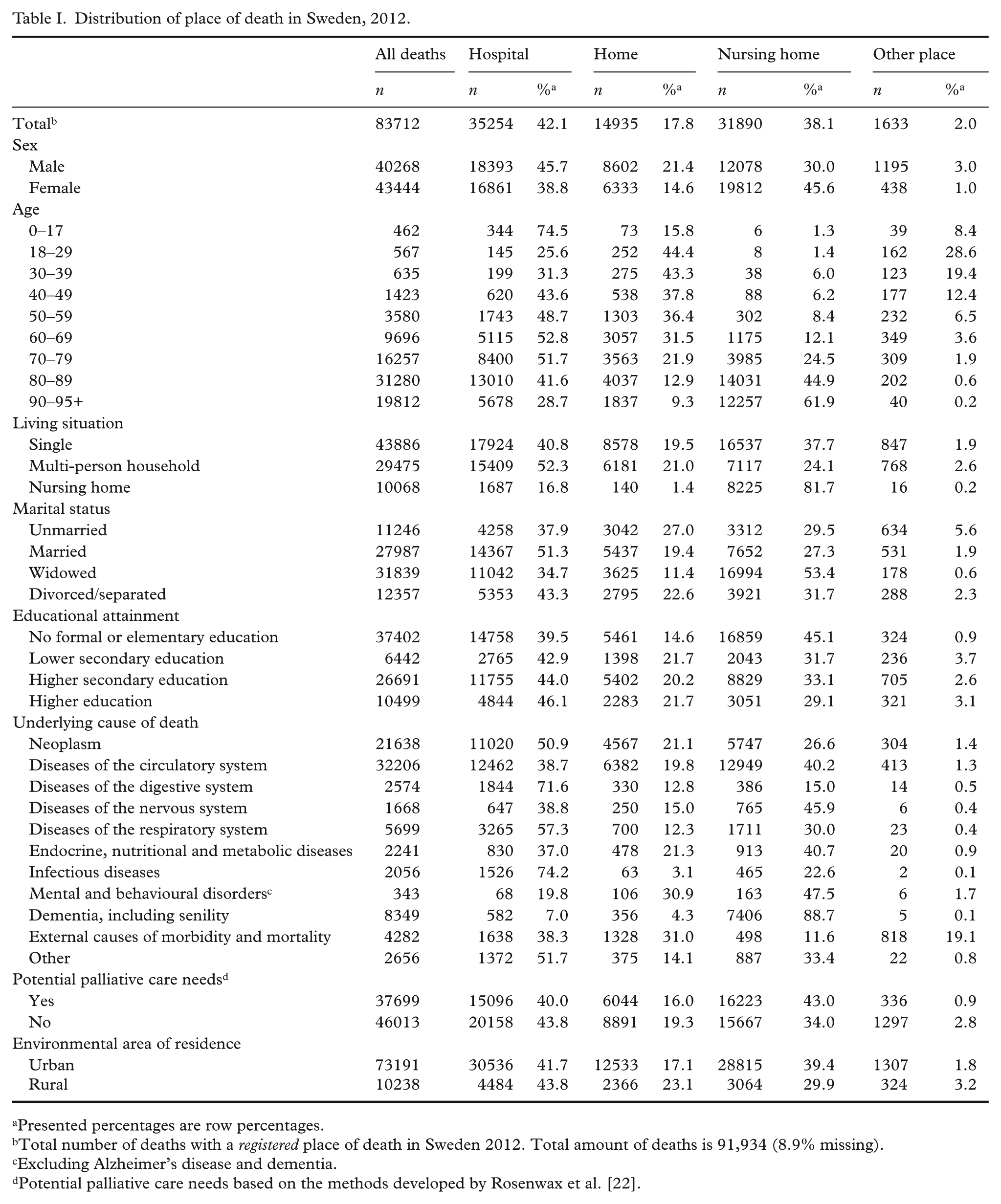
Presented percentages are row percentages.
Total number of deaths with a registered place of death in Sweden 2012. Total amount of deaths is 91,934 (8.9% missing).
Excluding Alzheimer’s disease and dementia.
Potential palliative care needs based on the methods developed by Rosenwax et al. [22].
Factors associated with likelihood of dying in hospital
While controlling only for age and sex in the first model, compared to people aged ⩾90 years, people within all age categories, regardless of living situation, were more likely to die in hospital than to die at home (or in a nursing home, if ⩾ 60 years), apart from those aged 18–29 years (OR = 0.80), who were more likely to die at home. In the second model, when adding the variables ‘cause of death’ and ‘potential palliative care needs’, people within the age category 30–39 years were more likely to die at home. This was also true of the third model, adding the variables ‘marital status’, ‘educational attainment’ and ‘urbanisation level’. Model 1 and 2 are provided as supplementary material.
Compared to male home dwellers, female home-dwellers were associated with a lower likelihood of dying in hospital and higher likelihood of dying in a nursing home than dying at home, in all three models. The higher likelihood of dying in hospital among females dwelling in nursing homes (as compared to men, OR = 1.35) was no longer significant when marital status, educational attainment and urbanisation level were included.
The results from the final model 3 (Table II) showed that among individuals residing at home, and controlling for all other covariates, those dying from digestive (OR= 2.12), respiratory (OR= 1.34) or infectious diseases (OR= 2.54) were more likely to die in hospital than die at home, compared to those dying from neoplastic diseases. Individuals with neoplasm residing at home were less likely to die in a nursing home than at home, than all other causes of death, except those with external causes.
Factors associated with the likelihood of dying in hospital versus dying at home or in nursing home, final model.
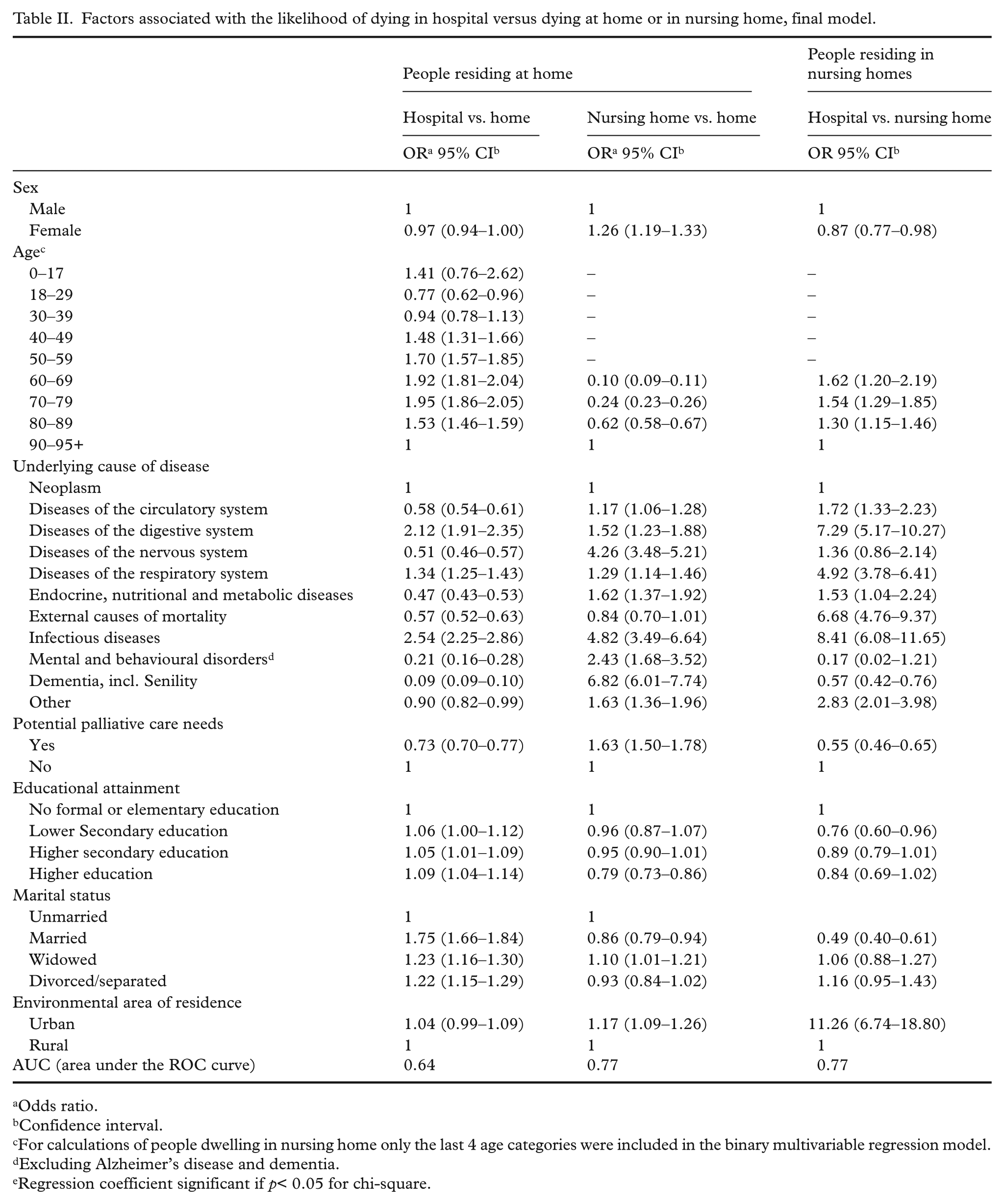
Odds ratio.
Confidence interval.
For calculations of people dwelling in nursing home only the last 4 age categories were included in the binary multivariable regression model.
Excluding Alzheimer’s disease and dementia.
Regression coefficient significant if p< 0.05 for chi-square.
Among individuals residing in nursing homes, only those with dementia (OR= 0.17) and mental or behavioural disorders (OR = 0.57) were less likely to die in hospital.
Individuals with potential palliative care needs were less likely than those without such needs to die in hospital than at home but also more likely to die in a nursing home than die at home (OR = 1.63).
Associations between education level and place of death were found among individuals residing at home: those with lower secondary education or more were (slightly) more likely to die in hospital compared to individuals with no or only elementary education. No associations between place of death and educational attainment were found among individuals residing in nursing homes.
Unmarried individuals and those living at home were more likely to die in hospital and more likely to die in nursing homes than those who were widowed. Being widowed or/divorced when residing in a nursing home was also associated with a higher likelihood of dying in hospital instead of in the nursing home.
Finally, in urban areas, those living at home were more likely to die in a nursing home than at home, and those living in a nursing home were more likely to die in a hospital (OR= 11.26).
Associations between hospital deaths, health care region and number of beds
Controlling for cause of death, individual and socioeconomic covariates, and adding the variables ‘health care region’ and ‘number of hospital- and nursing home beds per 10,000 inhabitants’, multivariable logistic regression showed that individuals in the Stockholm region living at home were more likely to die in hospital than die at home, than individuals in the north region living at home (OR= 1.13). People residing in nursing homes in the north region were less likely to die in hospital than remain in the nursing home than in all other regions except the southwest (Figure 1).
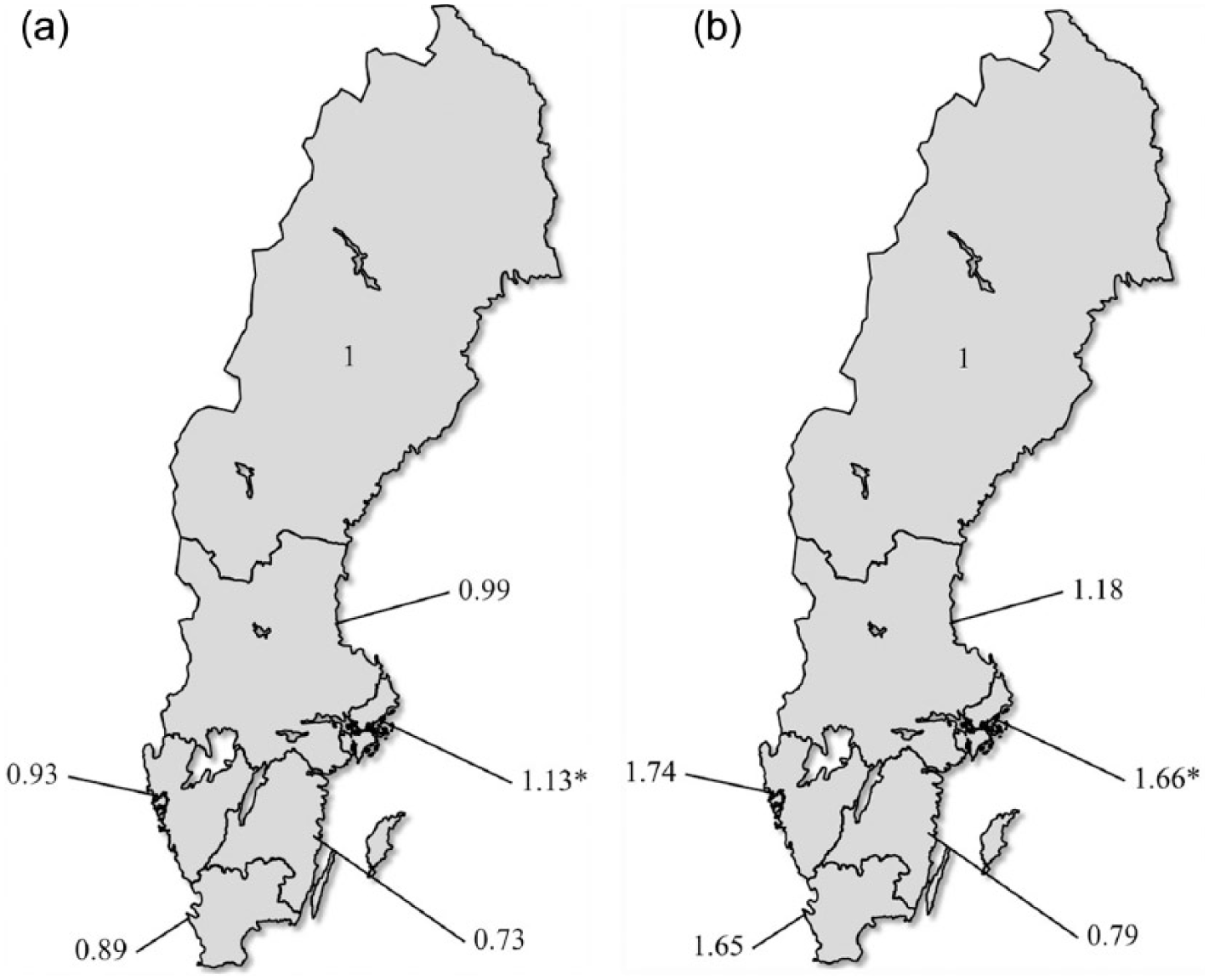
Odds ratios for associations between hospital death and the Swedish health care regions.
Both for those living at home and for those living in a nursing home, a higher number of hospital beds were associated with lower chance of dying in the hospital and a higher number of nursing home beds were associated with lower chance of dying in the nursing home (Table III).
Associations between place of death and the ratio of hospital and nursing home beds in the Swedish health care regions.
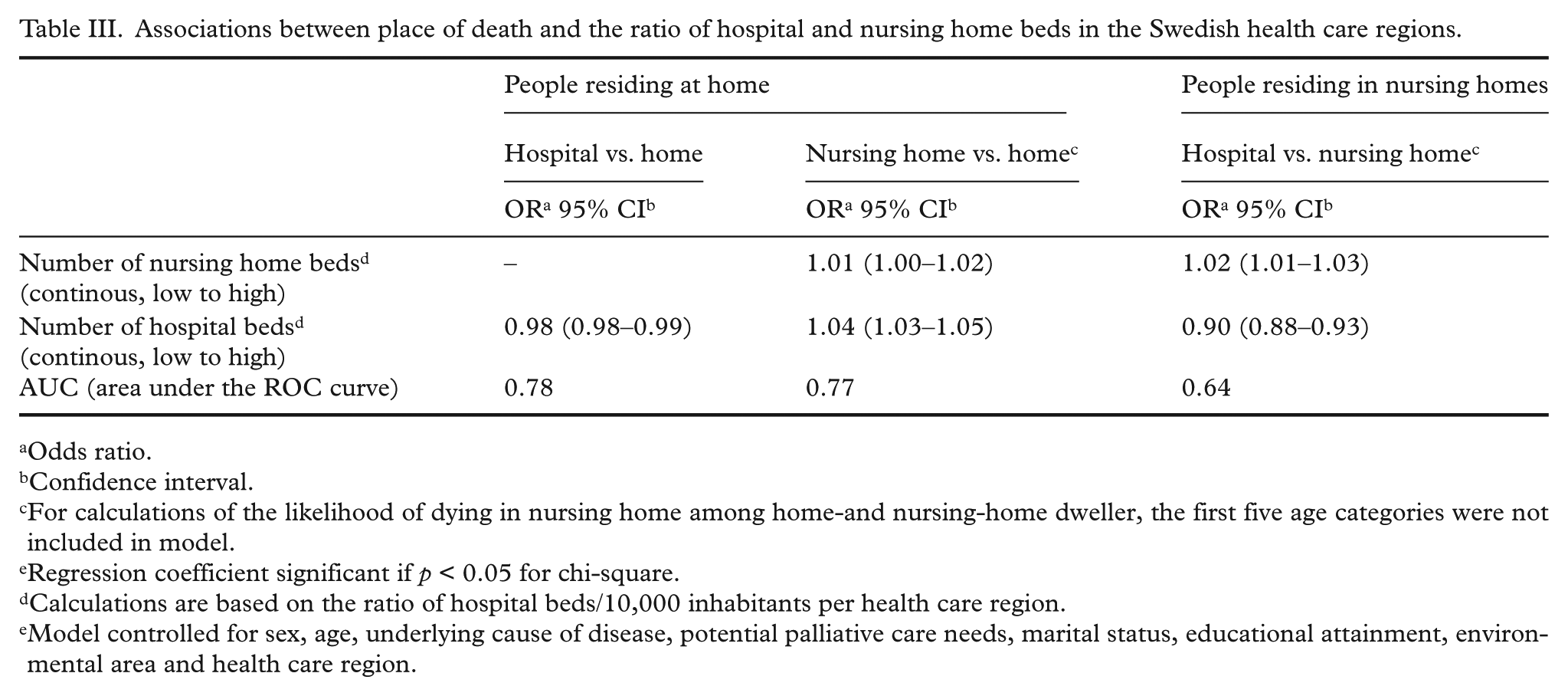
Odds ratio.
Confidence interval.
For calculations of the likelihood of dying in nursing home among home-and nursing-home dweller, the first five age categories were not included in model.
Regression coefficient significant if p < 0.05 for chi-square.
Calculations are based on the ratio of hospital beds/10,000 inhabitants per health care region.
Model controlled for sex, age, underlying cause of disease, potential palliative care needs, marital status, educational attainment, environmental area and health care region.
Discussion
In Sweden 2012, hospital was the most common place of death. The second most common place to die was nursing homes. Less than one fifth of all deaths occurred at home, and only very few individuals died in undefined sites. Individuals dying of conditions indicative of potential palliative care needs were less likely to die in hospital than others.
Population-level studies based on death certificate data have their limitations. There may be inaccuracies in the registering of the underlying causes of disease [11]. Moreover, on Swedish death certificates there is no option for discriminating specialized palliative care, which means that deaths in specialised palliative care services are included in the categories hospital or home.
Compared to other countries, the proportion of deaths in institutions, and in particular in nursing homes is relatively high [23]. Two specific patterns are worth noting. Firstly, less than a quarter of all people living in a private household eventually die there. Instead, they end up in hospital or in a nursing home at life’s end. During the past decade, health service resources have increasingly been allocated from hospitals to home care in Sweden.
Secondly, compared to other countries [23], relatively few individuals living in a nursing home are transferred to hospital to die there. In Sweden, care for older people is a legally regulated social right. The country has a long-standing tradition of providing special care for those who are old [24]. This has contributed to a strong nursing home establishment, with the numbers of nursing home beds being among the highest in the world [25], and (after The Netherlands), the highest total health and social service expenditures for older people in Europe [25]. Additionally, many nursing homes are specially designated to, or have special units for people with (advanced) dementia, which is likely why so few people with this diagnosis die in hospitals.
We also found regional differences. Other countries demonstrate a synchronised pattern between the ratio of hospital and nursing home beds and the ratio of hospital and nursing home deaths [26]. In contrast, we found that individuals living in regions with higher numbers of hospital- and nursing home beds were less likely to die in hospitals or nursing homes compared to individuals living in regions with lower numbers of beds. These results indicate that the relationship between bed ratios and place of death may not be as straightforward as is often assumed, and this has previously also been shown by Cohen et al. [15], who found logical associations in some countries, but not in others. In one region (southeast), higher numbers of home deaths were observed. This may potentially be explained by long-standing strategic palliative home care development [27].
Since the beginning of the 1990s, older people care is characterised by local self-government of the 290 local municipalities, with county councils being responsible for health services. Accordingly, the ‘outcomes’ of the legislation around care for older people is dependent on financial and political conditions prevailing at municipal level [24], and is thus in reality seemingly indistinct, with a risk for regional inequalities – something we potentially see in our results. An additional explanation for the higher numbers of nursing home deaths in, for example, the north region may be that with the distance to hospitals often being long, fewer transitions likely occur from homes or nursing homes to hospitals.
A relevant question to ask is whether or not the Swedish place of death demography presented in this study is problematic. In the discourse of quality of care at the end-of-life, hospitals and nursing homes have been presented with challenges related to quality of care [28, 29]. We have found no robust Swedish studies investigating and comparing the quality of palliative care between theses places of care and death, and it is thus unclear whether they provide appropriate conditions to die in. Moreover, place of death preferences in the Swedish population are unknown, even though it is reasonable to assume that Swedish people, like people in many other countries [4], would prefer to die at home.
A recent review of Swedish policy documents shows that governmental initiatives to influence palliative care policy are vague [30]. Swedish national guidelines for palliative care provide no recommendations for place of care/death, but stress the expansion of palliative care to include other groups than people with cancer, and to integrate palliative care into chronic illness care contexts [9].
Conclusion and implications
Compared to other countries, nursing homes in particular seem to be frequently used as settings for end-of-life care. As a result, the percentage of older people dying in hospital is lower than in several other countries. The within-country differences by age, sex, underlying cause of death, marital status, educational attainment and geographical area of residence suggest potential inequalities in Sweden regarding the availability and/or utilization of health services at the end of life.
Articulation of policy related to end-of-life, including place of death is needed. This may need to involve a nationwide monitoring and safeguarding of the quality of end-of-life care in nursing homes and hospitals. Additionally, a better understanding of the reasons for, and mechanisms behind the proportions of people dying at home is needed, as this could potentially indicate that the desire of many to die at home is not endorsed, and moreover that the ideal of dying at home may not be appropriate for all individuals. Assuring access to appropriate palliative care (both specialist and generalist) and adequate support in end-of-life situations at any time during people’s illness trajectories (as soon as palliative care needs occur and regardless of care place) will be an important priority for end-of-life care policy to address and hence, for health services to realize.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors thank the Erling Persson Family Foundation for funding the study.