
Abstract
Background: Despite the constitutional right of all Russian citizens to free medical care, out-of-pocket payment is a widespread phenomenon for all types of medical treatment. The aims of this paper are twofold: To present new evidence on the use of, and payment for, outpatient and inpatient treatment in Russia; and to compare the motivations behind both official and informal payments for outpatient services provided in public medical institutions. Methods: This study uses data from a quantitative household survey conducted in April 2014. The sample comprised 1602 individuals aged ⩾ 18 years, representing the entire adult population of the Russian Federation. We studied three types of medical care: inpatient treatment, outpatient treatment and medicines. Results: Our study found that 22.2% of patients pay for outpatient services, 37.5% pay for inpatient services and 91.5% pay for outpatient medicinal treatment. The informal payments are almost equally met in both outpatient (13.4%) and inpatient (12.2%) care; while the official payments are more common in inpatient care (25.2%), compared to outpatient care (8.8%). The main reasons for informal payment include: improvements in the quality of care and gratitude for medical staff. The official payments are more frequently motivated by an inability to receive a certain treatment free of charge.
Keywords
Background
Over the last 2 decades, the Russian health care system has seen significant changes, including the decentralization of government management, restructuring in the network of health facilities, the introduction of mandatory health insurance and changes in the drug reimbursement program [1]. One thing remains constant: According to the constitution of the Russian Federation, all Russian citizens still have the right to access healthcare services free of charge, in public institutions providing healthcare services. Keeping broad state guarantees against the backdrop of a substantial budget deficit in the 1990s was accompanied by a decrease in health care funding. The introduction of mandatory health care insurance, while it had a positive effect on the sustainability of financing for the health care system, was not able to insulate the health care sector from severe underfunding [2–4]. During the late 1990s through the beginning of the 2000s, the Russian health care sector was estimated to be financed at a level of only about 40–50% of actual needs [4]. Voluntary medical insurance is not yet widespread, covering about 5–6% of the population [5].
After the adoption in 1996 of Government Resolution number 27 on the ‘Provision of Paid Medical Services’ [6], public health facilities were permitted to provide certain health services on a chargeable basis, for patients who agreed to pay. During the Russian transformational period of the 1990s, charging for healthcare services in public medical institutions served as a means to reduce the gap between the state guarantees of free health care and declining government expenditures on health care. Moreover, the gap in health care system funding was largely being filled by informal payments.
The ‘Health for All Database’ reports that from 1995 to 2012, the share of Russian households’ out-of-pocket expenses on health (official and informal) rose from 16.9% to 34.3%. Nationally representative survey-based estimates report that informal payments covered about 15–17% of patients receiving outpatient care from 2006–2008 [7,8]. Other studies suggest different prevalence rates that range from 1.4% to 20.0%, depending on the type of healthcare service and method of estimation [2,9]. Widespread in the USSR as a form of gratitude to medical specialists, informal payments still remain a norm in post-communist Russia [6]. Even after the increase in health care funding that began in the year 2000 and the implementation of the ‘Health’ National Priority Project in 2006, followed by the increase in official salaries of healthcare practitioners, the out-of-pocket payments still made up for a significant part of healthcare expenditures [8].
In addition to the out-of-pocket payments for inpatient and outpatient care, Russians officially pay for outpatient drug treatment. Unlike the drug reimbursement systems with universal coverage that prevail in Europe, Russian patients get free medicine only when receiving inpatient care in public hospitals. A small percent of Russians are eligible for reimbursement of outpatient drug treatments, under the framework of two state programs:
The first, called ‘7 Nosologies’, is targeted at patients suffering from specific diseases that require particularly expensive treatment. The most recent available estimates suggest that this program has approximately 100,000 participants [10].
The second, the essential drug reimbursement program, targets certain groups of the population (mainly the disabled, individuals with chronic conditions and veterans).
After the introduction of broad social benefit reform in 2005 aimed at the monetization of social benefits, those eligible for the drug reimbursement program obtained the right to choose between receiving the medicine free of charge or receiving monthly cash benefits. As a result, the majority of eligible individuals (especially those with low incomes) choose cash benefits, viewing them as supplementary income for satisfying their basic needs [11], while only 3.8 million individuals choose the option of receiving the free medicine [12]. In sum, under the two existing drug reimbursement programs, < 5% of the Russian population has access to free outpatient drug treatment [13].
Recent papers on the use of medical care are mostly focused on informal payments [2,5,14–17]; however, empirical evidence has suggested that both official and informal out-of-pocket payments were responsible for an increase in unequal access to public healthcare services and an underuse of medical services and medicine [2].
This paper addresses the gap in the literature. It aims to present new evidence on the use of, and payment for, outpatient and inpatient treatment in Russia; and to compare the motivations behind both the official and informal payments for outpatient services that are provided in public medical institutions.
Methods
This paper uses data from a ‘Monthly Omnibus Study’ that was undertaken by the Levada-Center (an independent Russian polling and sociological research organization) in April 2014. The study was carried out in accordance with the ‘Russian State Directive On Personal Data’ (approved by the Federal Government from 27 July 2006 (N 152) and reapproved from 21 July 2014). The data were collected through a face-to-face interview in the homes of the respondents. Each interview lasted for about 1 hour. Participation in the survey was voluntary. All respondents were assured of confidentiality and verbally consented to be interviewed. The response rate was 30%, a rate that is rather low but typical for this type of survey in Russia. The sample may, to some extent, be biased and mainly reflect the opinions of the respondents who are more interested in health care issues and/or take greater advantage of the health care system than the general population; however, the final sample (which comprised 1602 individuals ⩾ 18 years of age) accurately represents the entire adult population of the Russian Federation by their federal district, settlement size, residence type (urban or rural), age and gender, thereby mitigating the potential bias of a low response rate.
The survey included questions about health status, outpatient care, hospital stay, use of medicine and out-of-pocket payments for health care, as well as a set of questions designed to determine the social and economic status of the respondents. This made it possible to study separately the use of outpatient and inpatient services, and outpatient drug treatment, as well as to compare the proportions of individuals paying for different types of care.
Statistical calculations were performed using STATA for Windows version 12. Statistical significance was calculated using the Pearson chi-square test. The mean values were compared using the Mann-Whitney U test.
Results
Russian patients today have greater choice of medical facilities and providers compared to Soviet (USSR) patients [1]. They may receive care in public and quasi-public health care institutions 1 as well as private hospitals and outpatient clinics. Thus, a patient today may receive a medical service free of charge, pay officially, buy health insurance or pay the medical staff informally. Different combinations of these options are also possible; however, the majority of Russians still opt for getting medical treatment in public medical institutions. The survey results show that 90.1% of all patients’ most recent visits to the doctor took place in a public institution and 5.1% in a quasi-public institution, where treatment was expected to be free of charge. Only 4.8% received outpatient treatment in private institutions.
The survey data show that out-of-pocket payments were common in all types of care. Table I demonstrated that many respondents received various types of medical care and paid for them out-of-pocket. Table I shows that respondents of different genders, age groups and health status differed in their probability of receiving medical treatment and paying for it. In particular, it reported that 521 female patients received outpatient care, representing 59.3% of all female subjects in the sample; however, only 98 female patients (18.4% of all females who received outpatient care) paid for it. Male patients were less likely to receive outpatient care (42.5%), but reported paying for outpatient care much more often than female patients. The female respondents were not only using more medical services, but were also more likely to take medicine compared to the male respondents (57.4% versus 35.2%, respectively); however, the probability of paying for medicine was equivalent for both genders. Our survey also showed that older adults receive treatment more frequently than younger respondents; however, there was no evidence that they are more likely to pay for their treatment, apart from paying for their medicine. Similarly, the survey respondents with chronic conditions reported using medical treatment more often than the rest of the sample, yet there was no statistically significant difference in paying for treatment, between those who suffer from chronic conditions and those who do not. Surprisingly, those in average financial situations reported receiving less outpatient and inpatient care than those in either good or bad financial situations. It appears that those in good financial standing have a greater probability of paying for care, but due to a small number of our respondents reporting a good financial status, there is no statistically significant difference between the groups with varying financial statuses.
Social and economic characteristics of respondents (n = 1602) reporting use of medical treatment.
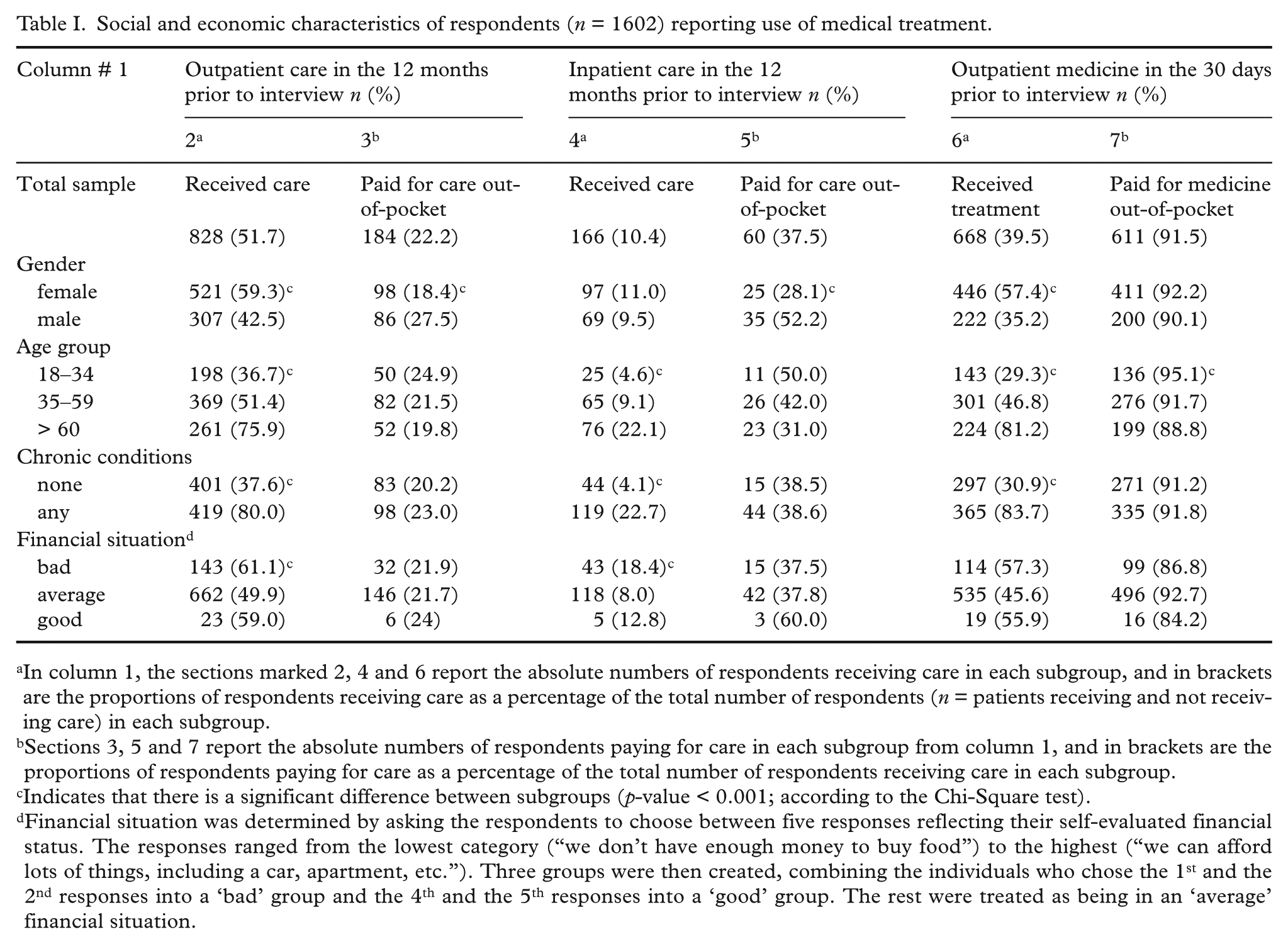
In column 1, the sections marked 2, 4 and 6 report the absolute numbers of respondents receiving care in each subgroup, and in brackets are the proportions of respondents receiving care as a percentage of the total number of respondents (n = patients receiving and not receiving care) in each subgroup.
Sections 3, 5 and 7 report the absolute numbers of respondents paying for care in each subgroup from column 1, and in brackets are the proportions of respondents paying for care as a percentage of the total number of respondents receiving care in each subgroup.
Indicates that there is a significant difference between subgroups (p-value < 0.001; according to the Chi-Square test).
Financial situation was determined by asking the respondents to choose between five responses reflecting their self-evaluated financial status. The responses ranged from the lowest category (“we don’t have enough money to buy food”) to the highest (“we can afford lots of things, including a car, apartment, etc.”). Three groups were then created, combining the individuals who chose the 1st and the 2nd responses into a ‘bad’ group and the 4th and the 5th responses into a ‘good’ group. The rest were treated as being in an ‘average’ financial situation.
Outpatient medicinal treatment
According to our survey results, 668 respondents (39.5%) received medicinal outpatient treatment in the 30 days prior to the interview and 611 (91.5%) of them paid for medicine out-of-pocket. The median and the mean monthly expenditures were 700 rubles (14.3 euros) and 1286 rubles (26.2 euros), respectively. The mean monthly payment for medicine was equal to 4.6% of a mean monthly salary of 27,766 rubles (567 euros) in 2014, according to the Russian statistical agency Rosstat). Of those who take medicine prescribed by a doctor on a constant basis, 85.6% pay out-of-pocket. There were 6.7% of the respondents who reported that they had received some medicine for free within the 6 months prior to the interview, but 72% of them stated that they had to buy other medicines out-of-pocket. Those eligible for drug reimbursement programs had to pay for medicine out-of-pocket for various reasons, the main one being that the lists of reimbursed drugs do not include many important conditions.
Inpatient care
Paying for inpatient care is more common than paying for outpatient care. The subsample of respondents who reported receiving inpatient care in the 12 months prior to the interview consisted of 166 respondents (10.4% of all respondents). Of these respondents, 60 (37.5%) paid for various types of medical services during their stay in hospitals, either officially or informally. There were 25.2% of patients who reported making official payments and 12.2% confessed that they had paid informally, in cash or in-kind. Respondents with chronic conditions, adults ⩾ 60 years of age, as well as those in bad financial situations were much more likely to receive inpatient care. There is no statistical difference in the probability of paying for inpatient care among different categories, except between male and female respondents (the male respondents were more likely to pay).
Outpatient care
Of the 1602 individuals, 828 (51.7%) reported having received outpatient care (excluding dental care) in the 12 months prior to the interview: Of them, 184 individuals (22.2%) reported having paid for their last visit officially or informally. There were 8.8% who made official payments and 13.4% who preferred making informal payments. Of those paying informally for outpatient care, the majority (54 individuals) reported giving in-kind presents; while 21 individuals reported giving cash payments and the rest (6 individuals) reported giving both cash and in-kind informal payments. Individuals were asked to estimate the price of the in-kind presents (flowers, alcohol, sweets, etc.) given to doctors during their last visit. This made it possible to compare the expenditures on the official and informal payments. The amount spent on official payments ranged from 200 to 30,000 rubles (4.1–612.2 euros) with the mean payment equal to 3446.5 rubles (70.3 euros) and the median equal to 1000 rubles (20.4 euros) per visit. Informal payments were less generous: They ranged from 150 to 10,000 rubles (3.1–204.1 euros), with mean spending equal to 1083 rubles (22.1 euros) and median equal to 550 rubles (11.2 euros). Therefore, the mean official payments were 3.2 times higher than the informal payments and the median official payments were two times higher than the informal payments (p < 0.000).
Reasons for official and informal payments
Patients in the sample were asked to provide their reasons for having made out-of-pocket payments during their last visit to a doctor. They named various reasons for paying for medical care (Table II). Of those paying officially, 40.1% said that the service they needed was not available for free. The second most widely mentioned reason (28.8%) was the desire to receive better quality of care. The quality-related reason was the first to be mentioned by those who preferred informal payments (50%). In addition, about one-third of the patients stated that they paid informally because they wanted to thank their doctor. Out-of-pocket payments (both official and informal) were also used to gain quicker access to medical care or because a certain specialist would not see the patient without him/her paying for services that were declared as free.
Main reasons for making official and informal payments in outpatient care.
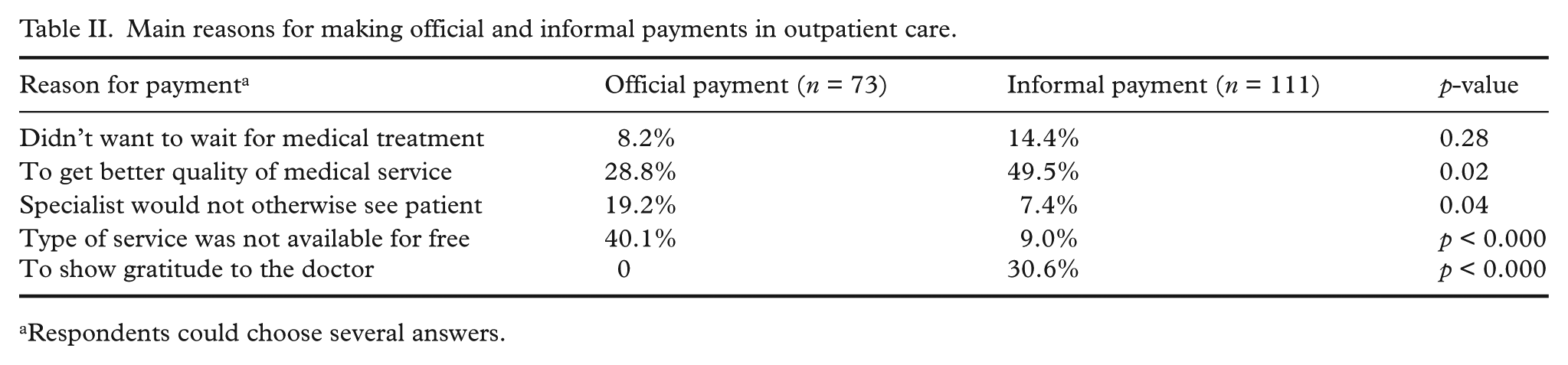
Respondents could choose several answers.
Discussion
The paper presents the results of a recent survey on the use of medical treatment in the Russian Federation. While most previous papers on out-of-pocket payments in Russia focused their attention on informal payments, studying their scope, forms, reasons, etc. [2,5,14–17]; official payments have rarely been devoted much attention, except for in a few papers [8,9,18]. Nevertheless, current governmental policies aimed at rationalizing the provision of health care have resulted in a growing burden of official payments. Still, studying both official and informal payments is important in understanding the availability of medical treatment in Russia.
This paper discusses the scope of official and informal payments for the main types of medical care (namely outpatient medicinal treatment, inpatient and outpatient care in public hospitals). The data showed that > 90% of Russians were not eligible for any outpatient drug reimbursement programs and paid about 4.6% of their monthly salary out-of-pocket for outpatient medicinal treatment. Out-of-pocket payments were more widespread in inpatient care than in outpatient care. Empirical data suggest that 22.2% of patients paid for outpatient services and 37.5% paid for inpatient services. The survey data show that informal payments were made almost equally in outpatient (13.4%) and inpatient (12.2%) care, while official payments were more common in inpatient care (25.2%) than in outpatient care (8.8%). These observations are in general agreement with estimates reported in previous studies [5,8,9]; however, direct comparisons are impossible, due to different data, periods and methods.
The conclusions from previous studies about the association between the social and economic characteristics of individuals and the use of payment for medical care are controversial, especially concerning individuals’ financial situations. The present study revealed the following association: there was a significantly higher number of recipients of medical treatment among women, older adults, individuals suffering from chronic conditions and low-income respondents. Out-of-pocket payments for medical services seemed to be equally widespread in all of the groups under analysis (the exception being male respondents, who were more inclined to pay for both inpatient and outpatient care).
Of those paying for outpatient care, the majority prefers informal payments to official payments, with the difference in the size of payments being more than 2-fold. The study data made it possible to compare the reasons for official and informal payments (while in previous studies, those two were either studied together or only the reasons for informal payments were studied [8,9]). The survey data showed that quality-related issues, along with an intention to show gratitude to medical staff, are the main motivations for informal payments. By contrast, official payments are more common when patients are unable to get medical treatment free of charge. Unfortunately, the small size of this survey made it impossible to compare the reasons for official and informal payments for inpatient care, similarly to outpatient care. Further studies are needed to address these issues and to explore the burden of official and informal payments for various types of medical treatment.
Footnotes
Acknowledgements
I would like to thank two anonymous referees for their valuable comments and remarks.
Conflict of interest
The author declares that there is no conflict of interest.
Funding statement
This work was supported by University College London School of Slavonic and East European Studies (UCL SSEES) (for data collection) and the National Research University Higher School of Economics (NRU HSE) Basic Research Program (for research within the project “Older people opportunities, socio-economic determinants of active ageing, and public policies”).