
Abstract
Aims: Childhood illnesses such as diarrhoea and pneumonia remain major contributors to child mortality globally and need to be continually targeted in pursuit of universal health coverage. This study analyses time trends in the prevalence of fever/cough and diarrhoea in Nepal and applies an equity lens in order to identify disadvantaged groups. Methods: Data from the Nepal Demographic Health Surveys of 2001, 2006, and 2011, together with data from the most recent Multiple Indicator Cluster Survey of 2014 performed in Nepal, were utilized for analysis. Results: Analyses revealed improvements (lower prevalence) of diarrhoea and fever/cough in children under five in Nepal over the last 15 years, with an equitable distribution of symptoms over socio-economic determinants. There was, however, a marked and maintained inequity in care seeking for these symptoms, with less educated mothers and those from poor households being only approximately half as likely to seek care for their children.
Introduction
Despite recent improvements in global child survival there is still a long way to go before all preventable child deaths are averted [1]. Globally, most of the deaths of children under the age of five are due to a limited number of causes, with pneumonia and diarrhoea as the main killers [2]. This is despite the fact that the timely recognition of danger signs, with appropriate care seeking, and the administration of simple drugs such as oral antibiotics, oral rehydration solutions (ORS), and zinc could prevent most of these deaths [3]. Efforts have been made to implement this knowledge, which has contributed to the rapid improvements in child survival. Even if the gains have favoured the more disadvantaged, with a decreasing inequity in child illness and greater survival as a result [4], there are still reasons to raise concerns about the unequally distributed burden of childhood disease and deaths [5].
In light of the new Sustainable Development Goal (SDG) agenda, it is not only important to continue to promote the implementation of antibiotics, ORS, and zinc for small children, but also to assure universal coverage of these interventions [6]. However, pneumonia – and, even more so, diarrhoea – has societal causes, with improper hygiene, poor sanitation, and malnutrition as root causes [7,8]. Thus, it is not only the lack of knowledge or accessibility to treatment that pose a challenge to equity since the prevalence of these diseases can be assumed to be skewed in disfavour of the disadvantaged [7].
In Nepal, despite being a low-income country and having slow improvement in per capita income during the last two decades, significant improvements have been made in child survival, with a 77% reduction of the country’s under-five mortality rate during the Millennium Development Goal (MDG) reporting period, from 158/1000 live births in 1990 to 36/1000 in 2015 [4]. This achievement in reaching the MDG 4 target has largely been attributed to broad coverage and reduction of the equity gap in vaccination against childhood disease [9]. In the last two decades, investments have also been made in developing and strengthening a community-based network of health volunteers all over the country [10]. Local communities selected female community health volunteers (FCHVs) from their community to promote preventive health services as well as refer for care to health facilities [11]. Volunteers promoted immunization services as well as provided treatment to children with suspected pneumonia and diarrhoea [12]. These FCHVs diagnose acute respiratory infections in children and treat with oral antibiotics; they also identify cases of diarrhoea in the community and provide ORS and zinc [13]. To improve access for services, the community-based program called Community-Based Integrated Management of Childhood Illness (CB-IMCI) entrusted the FCHVs with the treatment of sick children at the household and community level [14]. The CB-IMCI had three major strategic approaches of implementation: (1) training the health workers and FCHVs in the case-based management of diarrhoea and pneumonia; (2) community mobilization of a community-based network to improve care seeking from care givers; and (3) strengthening the supply of commodities such as oral antibiotics, zinc, and ORS [15,16]. The program started in 1998 and was scaled up nationwide in 2009 [17]. The objective of this public health effort was to access the hard-to-reach and it was expected that this intervention would reduce inequity in child health [16].
In Nepal, health care-seeking behaviour for childhood illnesses is known to be associated with social factors such as the caregiver’s level of education, family income [18], and the child’s gender [19]. This is further compounded by the existing traditional beliefs and practices that not only delay care seeking but also push the sick child towards severity.
Investigating changes in health equity over time adds another dimension to the efforts to reduce child mortality. The importance of not only achieving improvements in overall survival but making survival less unjust has been highlighted in recent years. Furthermore, there is growing evidence of more people opting towards the private sector, raising concerns about the quality of some of these services provided by public institutions. It is evident that Nepal has made huge strides in the struggle to improve the health of children. The aims of this study are, therefore, to assess changes in equity for the prevalence of fever/cough and diarrhoea and care seeking in connection to those symptoms of illness over the past 15 years.
Method
Sample and variables of interest
Data from the Nepal Demographic Health Surveys (DHS) of 2001, 2006, and 2011, together with data from the most recent Nepalese Multiple Indicator Cluster Survey (MICS5) of 2014, were utilized for analysis. Sampling procedures have been described elsewhere and can be considered representative for Nepal at large [20–23]. The main outcome variables were whether parents reported that their child had diarrhoea or fever/cough within the two weeks prior to the survey. In addition, seeking care for the symptoms reported was included as an outcome variable of interest. In order to analyse equity gaps in relation to these main outcome variables, all available structural determinants were included as independent variables. The theoretical framework set up by the Commission of Structural Determinants of Health (CSDH) guided the analysis [24]. The CSDH framework emphasizes social position, as decided by a number of structural determinants, as the main driver of inequities in health. We thus included wealth status, education level of mother, ethnicity of household head (not available in MICS5), religious belonging (not available in MICS5), and gender of child in the analysis. We deviated, however, from the CSDH framework by including place of residence as a structural determinant. In the CSDH framework, living area is considered a proximal determinant; but given the inaccessible geography of Nepal’s mountainous regions, as well as recent research focus on the urban–rural divide, we also incorporated these variables as potential drivers of inequity.
Wealth, or economic status, was defined through a pre-set wealth index based on assets and calculated by Principal Components Analysis as defined in the respective survey methodologies [25]. Mother’s education level was defined as either the mother being illiterate or literate, or whether the mother has completed primary education or not. There are multiple ethnic groups in Nepal and the caste system is interlinked with ethnicity. A dichotomization between advantaged and disadvantaged groups was made, with Dalits, lower-caste Janajatis, non-dalit Terai caste, and religious minorities classified as disadvantaged, and upper-caste and better-off Janajatis being classified as advantaged groups. In addition, a dichotomization of Hindu and non-Hindu was made.
Data analysis
The prevalence of diarrhoea and fever/cough in children as defined by the respective survey was calculated and divided by the structural determinants described above. The Chi-square test was used to detect group differences and a p-value of <0.05 was considered significant.
A multivariable logistic regression analysis was then applied. Even if inequity in health outcomes can be driven by all structural determinants, we chose to keep a focus on wealth status and the mother’s education level, since these variables are mostly used to measure inequity in health outcomes. Thus, belonging to the lowest wealth quintile and the mother being illiterate were variables included in all regression models, together with the variables showing a significant difference in the previous analysis using Chi-square tests. Adjusted odds ratios (AdjORs) and 95% confidence intervals (CIs) were calculated.
A subset analysis of children who reportedly had had diarrhoea or fever/cough in the last two weeks was performed using multivariable logistic regression with care seeking as the dependent variable, classified into whether care was sought for the child or not. In this multivariable analysis, all structural determinants available in the respective surveys were included.
Results
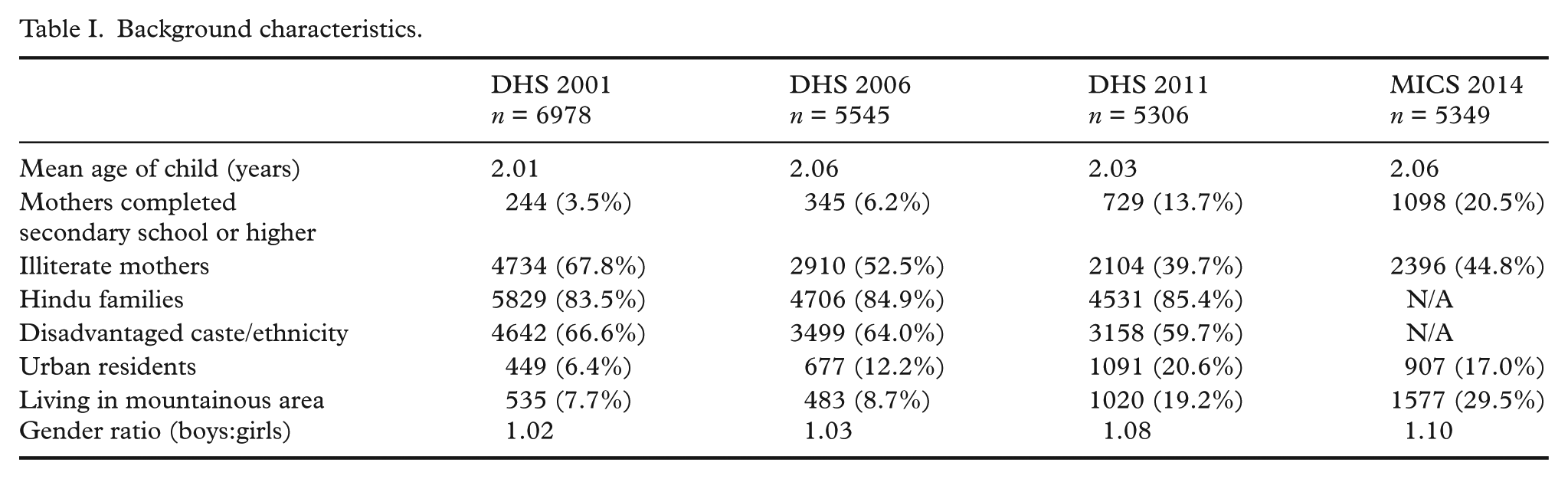
More than 5000 children were included in each of the surveys (Table I), with the largest sample size in DHS 2001 (n = 6978). Overall, there was a trend towards higher education for mothers over the study period, with an increasing literacy rate from 32.2% in 2001 to 55.2% in 2014, and a greater share of mothers having completed at least secondary education from 3.5% in 2001 to 20.5% in 2014. There is also a clear urbanization trend with a threefold increase in the proportion of families living in urban areas over the study period. Contrary to this trend, it should also be noted that there is a considerably larger proportion of families living in mountainous areas in the MICS5 sample compared to the DHS samples, which might be due to different sample procedures in the survey methodologies. Over time, we can also see an increasing sex ratio between boys and girls in the data material.
Background characteristics.
Prevalence rates – total and classified by structural determinants – of diarrhoea and fever/cough during the two weeks prior to data acquisition are displayed in Table II. It is notable how the prevalence of both diarrhoea and fever/cough in children dropped by more than 40% between DHS 2001 and DHS 2006 (p < 0.01) and how the prevalence since then has remained steady – around 20% for fever/cough and a little more than 10% for diarrhoea. When classifying prevalence by structural determinants, many group comparisons result in significant differences. There is a general trend to a more equitable distribution over the structural determinants for fever/cough prevalence; whereas, for diarrhoea, there is a pattern of maintained inequity with all structural determinants except gender, showing significant discrepancies between the most disadvantaged and the advantaged.
Prevalence of childhood illnesses (fever/cough and diarrhoea) two weeks prior to survey, divided by structural determinants over time among children in Nepal.
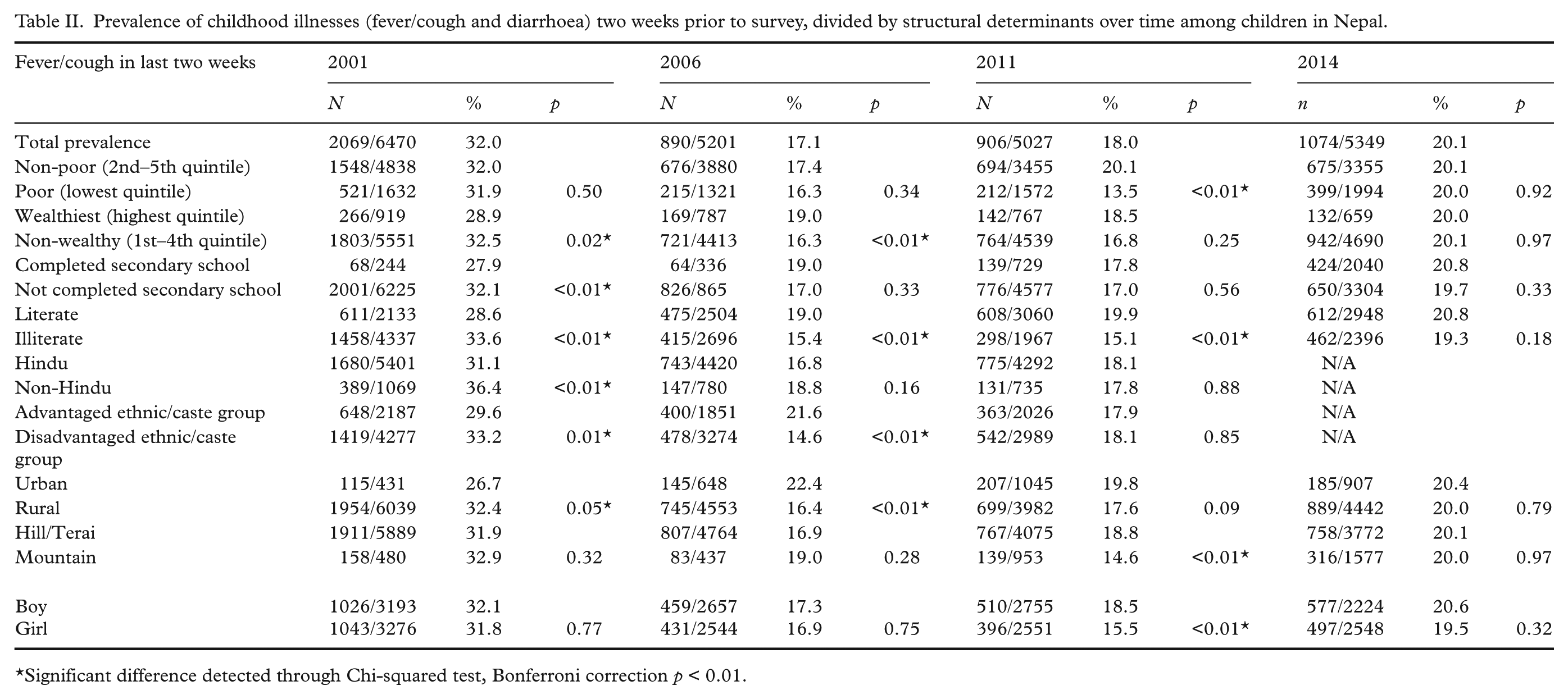
Significant difference detected through Chi-squared test, Bonferroni correction p < 0.01.
The multivariable regression analysis indicates a rather equitable distribution of the risk for diarrhoea and fever/cough over wealth and literacy status, with only minor discrepancies between the different surveys. The only result that stands out is the risk for diarrhoea, which in MICS5 data from 2014 displays an increased risk for the poorest segment (AdjOR 1.28, CI 95% 1.07–1.54) as well as for children of illiterate mothers (AdjOR 1.23, CI 95% 1.04–1.46). For reported fever/cough there are no significant differences between groups, neither within nor between surveys (Table III).
Multiple logistic regressions for childhood illnesses among children in Nepal. Adjusted Odds Ratios displayed.
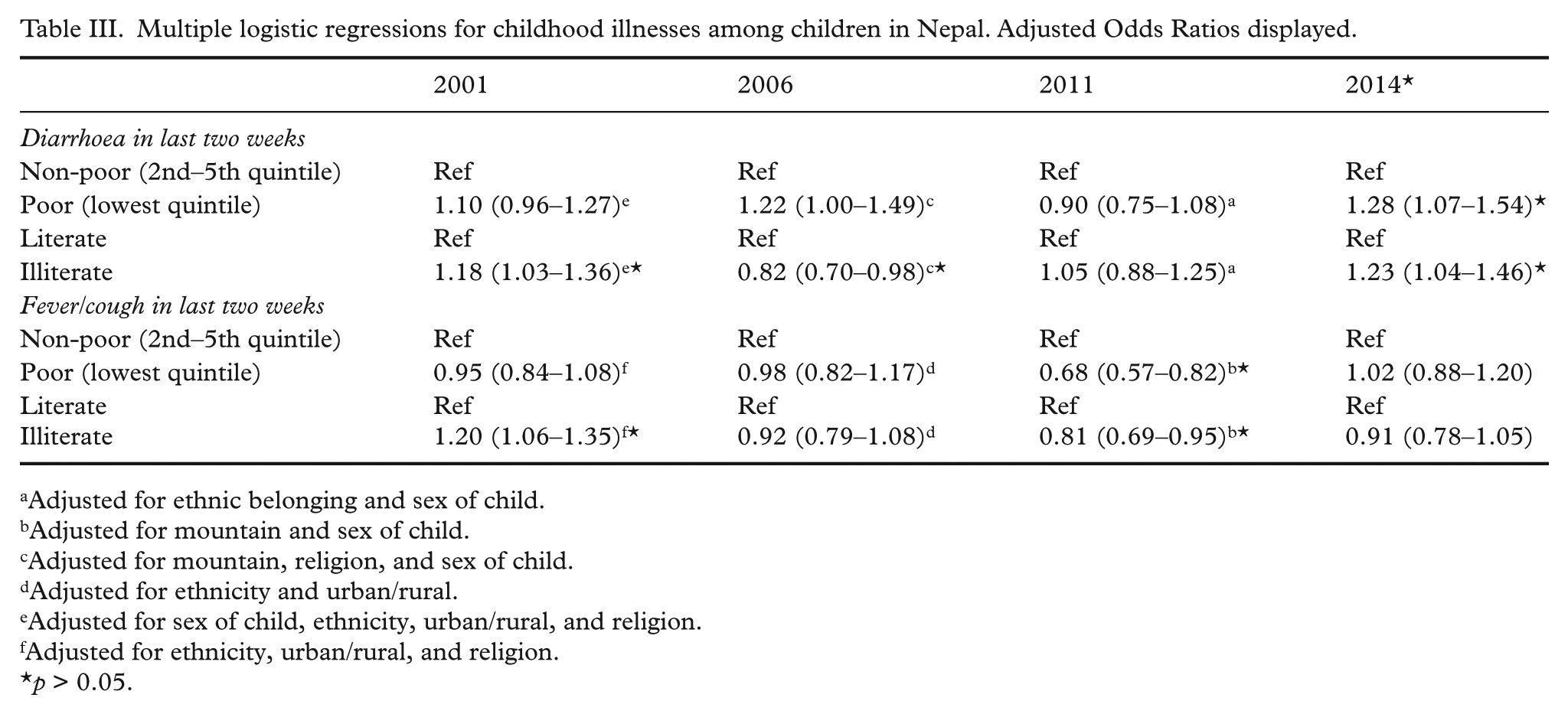
Adjusted for ethnic belonging and sex of child.
Adjusted for mountain and sex of child.
Adjusted for mountain, religion, and sex of child.
Adjusted for ethnicity and urban/rural.
Adjusted for sex of child, ethnicity, urban/rural, and religion.
Adjusted for ethnicity, urban/rural, and religion.
p > 0.05.
Even if there are no great inequities in prevalence of symptoms, a further analysis of care-seeking behaviour for the children with reported symptoms reveals large and persistent inequities, primarily based on wealth status (Figure 1). In 2014, families belonging to the poorest quintile were only half as likely to seek care for children showing symptoms of diarrhoea (AdjOR 0.53, CI 95% 0.37–0.77) or fever/cough (AdjOR 0.56, CI 95% 0.44–0.72) compared to the better-off families. These differences were also observed in the previous surveys, all with significant results and with overlapping confidence intervals between surveys (Figure 2).
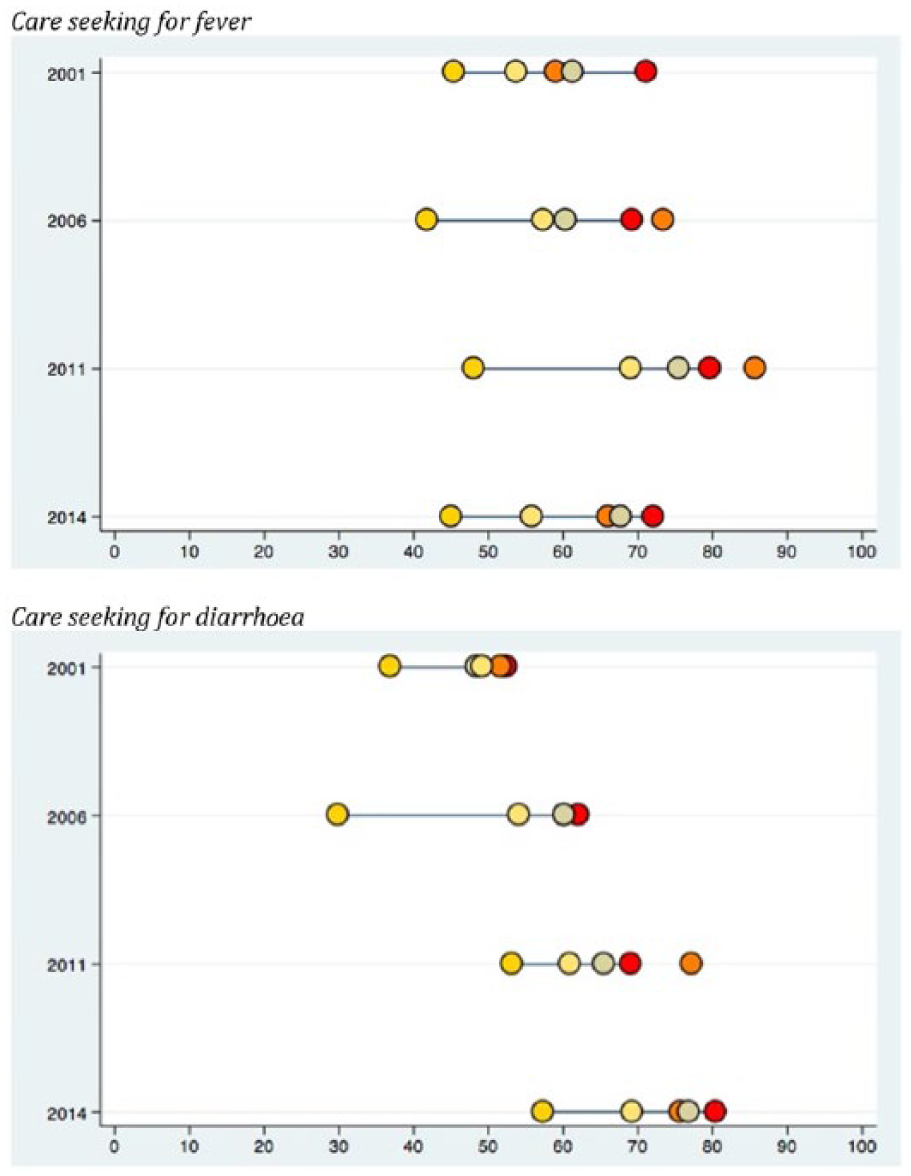
Equiplots displaying percentage of children showing symptoms of fever/cough or diarrhoea in the two weeks preceding survey that care was sought for in Nepal. Wealth quintiles based on DHS 2001, 2006, 2011, and MICS 2014 displayed.
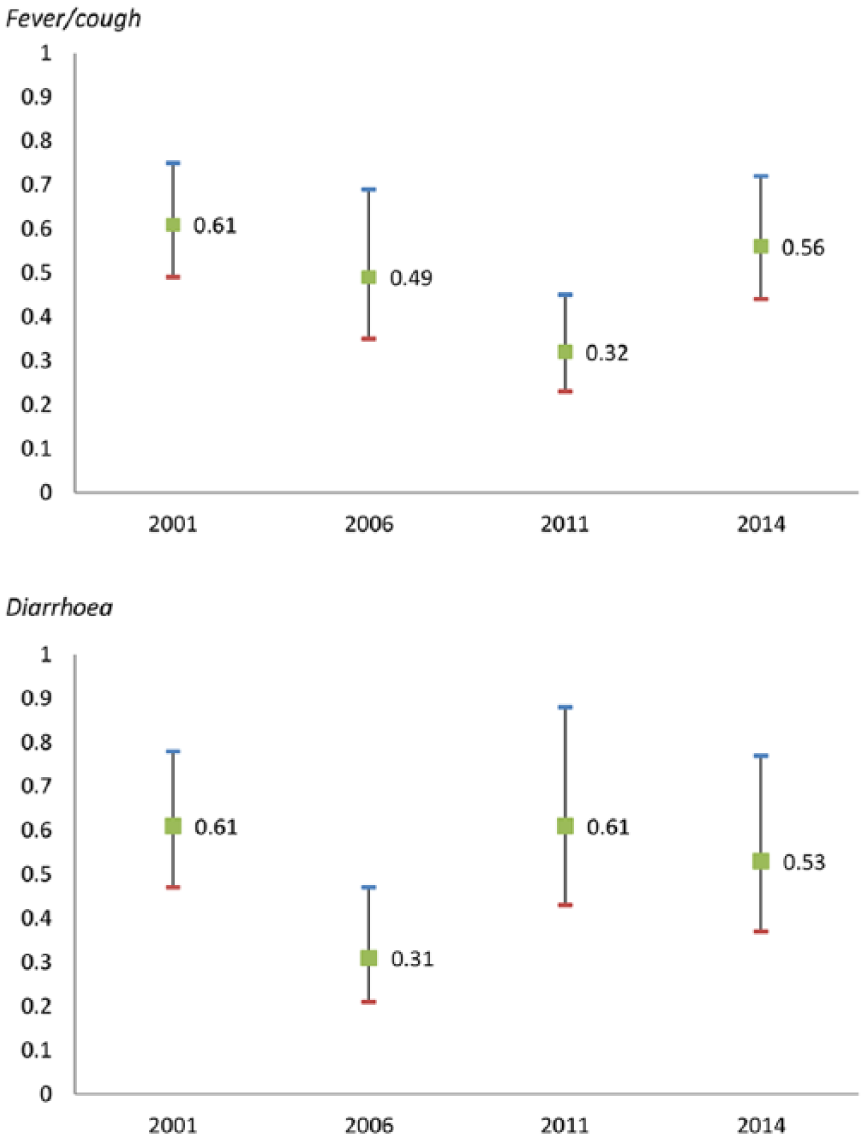
Likelihood of care seeking for child with fever/cough or diarrhoea in the last two weeks for poorest quintile (Ref 2nd–5th quintile. Odds ratios and 95% confidence intervals are presented. Adjusted for mother’s education, living area, sex of child, religious belonging, and ethnicity.
Discussion
To summarize the study, three main results can be highlighted. Firstly, there was a large reduction in disease prevalence between the 2001 DHS and the 2006 DHS, and thereafter the prevalence was steady. The dramatic decrease in the prevalence in diarrhoea and fever/cough from 2001 to 2006 can be attributed to a scaling up of the CB-IMCI program during this period. CB-IMCI programs promoted healthy behaviour for early and exclusive breast feeding, improving hygiene, and sanitation for children.
Secondly, there were no major inequities detected in relation to fever/cough symptoms based on the structural determinants, with a trend towards a more equitable distribution, and only minor inequities in symptoms of diarrhoea in children prevailing over the four surveys.
Thirdly, there were large and persisting inequities in care seeking for the noted symptoms, with family wealth being the most predominant structural determinant. The inequity displayed in care seeking could be explained by a multitude of factors, one being the cost of seeking care, as has been shown in studies from around the world [26–28].
The recognition of childhood illness is a prerequisite for both care seeking and adequate treatment. A systematic review, however, found that there is a scarcity of studies on the recognition of childhood illnesses [29], and that the recognition rate overall was low. The lack of inequity in the prevalence of fever/cough and diarrhoea in the survey material might thus be attributed to a reporting error since symptoms were self-reported by caregivers. From an equity perspective, it thus becomes more important to look at the actual care seeking for a perceived illness.
Footnotes
Data sharing statement
Data was accessed by permission from DHS and MICS. Additional data can be retrieved at: http://dhsprogram.com/data/ and ![]()
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by UNICEF Nepal.