
Abstract
Background: During past decades the formerly active lifestyle in Greenland has become sedentary, and the intake of traditional food has gradually been replaced with imported food. These lifestyle and dietary habits may affect pregnant women. Aim: To describe age and regional differences in reproductive factors, lifestyle and diet among Greenlandic pregnant women in their first trimester. Methods: A cross-sectional study during 2013–2015 including 373 pregnant women was conducted in five Greenlandic regions (West, Disko Bay, South, North and East). Interview-based questionnaires on reproductive factors, lifestyle and dietary habits were compared in relation to two age groups (median age ≤28 years and >28 years). Results: In total, 72.4% were Inuit, 46.6% had BMI >25.0 kg/m2, 29.0% were smoking during pregnancy and 54.6% had used hashish. BMI, educational level, personal income, previous pregnancies and planned breastfeeding period were significantly higher in the age group >28 years of age compared to the age group ≤28 years of age. In region Disko Bay, 90.9% were Inuit, in region South more had a university degree (37.9%) and region East had the highest number of previous pregnancies, the highest number of smokers during pregnancy and the most frequent intake of sauce with hot meals and fast-food.
Keywords
Background
Greenland has experienced major changes since the beginning of the 20th century. The former traditionally physically active life has been replaced by a more sedentary lifestyle [1].The traditional marine food, rich in beneficial polyunsaturated fatty acids and vitamins, has gradually been supplemented by imported foods often high in saturated fat, sugar and salt [2, 3]. The changes in lifestyle and dietary pattern are believed to be associated with an increased prevalence of lifestyle-related diseases such as obesity, cardiovascular diseases, diabetes and certain cancers [3–5]. In addition, several studies have documented a high content of harmful substances such as persistent organic pollutants (POPs) and heavy metals in the traditional Greenlandic food [6, 7] with adverse health effects found in the areas of reproduction, pediatrics, cardiology and oncology [7–9].
Pregnant women are particularly vulnerable to lifestyle and dietary changes. When investigating reproductive factors, lifestyle and dietary habits, it is thus important to study regional and age differences to provide adequate advice for this group.
During the last decade, only a few studies have investigated the reproductive factors, lifestyle and dietary habits in Greenland and most of these studies were not representative for all regions [6, 10, 11]. Our recent study, a sub-study of the ACCEPT (Adaption to Climate Change, Environmental Pollution, and Dietary Transition) study – a geographical and prospective Greenlandic Birth Cohort and biobank (2010–2015) – studied age and regional differences in lifestyle, reproductive factors and food intake among pregnant women during 2010–2011, based on data from questionnaires filled in during the 2nd and 3rd trimester of pregnancy [12]. The present study is a continuation of the ACCEPT sub-study 2010–2011, including more Greenlandic towns where enrolment of pregnant women between 2013 and 2015 predominantly took place in the 1st trimester of pregnancy.
Methods
Study population
Seven towns in Greenland were selected for enrolment of participants; selection was based on geographical and logistic possibilities (Figure 1). Upon contact all women meeting the inclusion criteria of being pregnant, ≥18 years of age and living in one of the selected towns at the time of inclusion, were invited to participate. The Greenlandic population often relocates nationally and internationally; thus, the selected towns for enrolment only represented the place where the women lived at the time of inclusion. To assess which reproductive factors, lifestyle, and dietary habits were most pronounced throughout life, the region where the women had lived for the longest time was used for the statistical analyses. When sparse or no information was available, data from the enrolment town was used. Women were recruited between June 2013 and November 2015. Midwives or staff of the Centre of Arctic Health at Aarhus University were responsible for the recruitment and distribution of the questionnaires. In total, 405 pregnant women were invited to participate; 31 women left the study due to abortions, or because they regretted participation or moved abroad. A total of 374 participants remained in the study; one woman participated twice as she had more than one pregnancy during the data collection period. One participant was <18 years of age and thus excluded from the study. The final number of study subjects was 373, resulting in a participation rate of 92%, equivalent to 23% of the total number of registered births at the seven selected enrolment towns and 15% of the total number of registered births in Greenland during 2013–2015 [13] (Supplementary I).
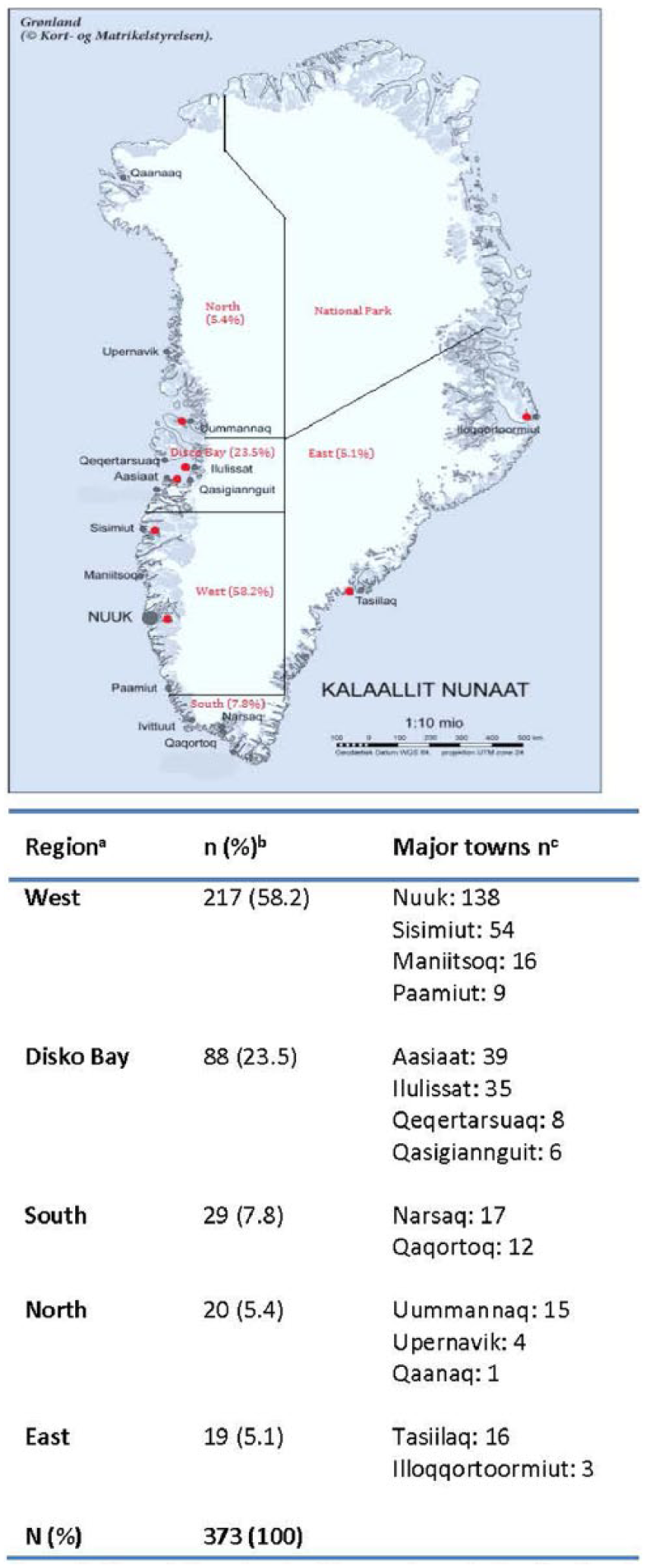
Map of Greenland with recruitment sites (red) and regions from [33], the Agency for Data Supply and Efficiency, under a CC-BY license.
Prior to data collection, all participants received a detailed description of the project’s purpose and the questionnaires to be filled in. Moreover, the women were informed that participation was voluntary and they could withdraw from the study at any time. Written informed consent was obtained from each participant. The study was conducted in accordance with the Helsinki Declaration II and approved by the Ethical Commission for Scientific Investigations in Greenland.
Lifestyle Questionnaire and Food Frequency Questionnaire
Upon enrolment the participants completed an interview-based lifestyle questionnaire (LQ) and a food frequency questionnaire (FFQ) available in both Greenlandic and Danish.
The LQ was based on data from the pregnant women’s medical record supplemented with questions also used in the ACCEPT sub-study 2010-2011 (12). Those questions concerned biological, cultural and sociodemographic characteristics, reproductive factors such as reproductive history and breastfeeding plans, Body Mass Index (BMI, calculated as weight in kilograms/height in metres2) [14], smoking status, alcohol consumption and use of hashish.
The FFQ was based on questionnaires previously used in Greenland and optimized for the ACCEPT sub-study 2010–2011 [12]. It contained questions about 40 traditional and 23 imported foods, divided into seven main traditional food groups: ‘Marine mammals’, ‘Seabirds’, ‘Fish’, ‘Dried fish’, ‘Shellfish’, ‘Terrestrial animals’ and ‘Berries’ and seven main imported food groups: ‘Meat products’, ‘Carbohydrate foods’, ‘Sauce’, ‘Fruit’, ‘Vegetables’, ‘Fast food’ and ‘Sweets and Snacks’ (Supplementary II). Eight response categories from ‘never’ to ‘several times a day’ were listed in the FFQ to measure the consumption of the different food items. As the questionnaire did not include portion size, the exact amount of each dietary item consumed was unknown. A frequency score was therefore applied transforming all categories from ‘never’ to ‘several times a day’ into number of times consumed per month (Supplementary III). This method has been used previously [12, 15, 16]. See Supplementary IV or more details on calculation of frequency score.
Statistical analysis
All LQ and FFQ data were manually double-entered into the validated program, Epidata, and statistically analyzed using IBM SPSS version 22 software. The statistical significance level was set to p ≤0.05. P-values ≤0.1 were considered borderline significant. To improve the normality and homogeneity of variance, data was transformed using natural logarithmic transformation [ln(x)]. Independent samples t-test and one-way analysis of variance (ANOVA) were used for comparison of mean scores of food intake between age groups and regions, respectively. Post-hoc tests were conducted if a statistically significant difference was found in the overall ANOVA analysis. Levene’s test for homogeneity of variance was conducted to test whether the variance of scores was the same in age groups and across the five regions. When the assumption of homogeneity of variance was violated, a second p-value or the result from the Welch test was interpreted in the independent t-test and ANOVA, respectively. Pearson’s chi-squared test was conducted for comparison of categorical data between age groups and between regions. When the assumption of minimum expected cell frequency of ≥5 was violated, an additional Fischer’s exact test was conducted.
Results
Characteristics, reproductive factors and lifestyle of the study participants are presented in Table I. Median age of participants at inclusion was 28 years. Median BMI was 24.2 kg/m2 with 28.0% and 18.6% of the participants being overweight (BMI ≥25.00–29.99 kg/m2) and obese (BMI ≥30.00 kg/m2), respectively. In total, 72.4% were Inuit and 18.5% were partly Inuit. A total of 27% had passed primary school, 46.6% had passed high school and 26.5% had a university degree. Annual personal income was equally distributed between the following annual income groups <DKK 100,000, DKK 100,000–250,000, >DKK 250,000 and ‘don’t know’. A total of 57% and 9.3% of the participants had 1–2 and 3 previous pregnancies, respectively; 55.0% and 25.1% had 1–2 and 3 abortions, respectively; 99.2% planned to breastfeed their infant; 46.0% planned to breastfeed for 6–12 months and 40.4% were in doubt regarding the duration of planned breastfeeding. A total of 52% smoked pre-pregnancy and 29.0% smoked during pregnancy. Before pregnancy, 48.1% consumed alcohol <1 time a month and 10.3% consumed alcohol >1 time a week. During pregnancy, 44.2% consumed alcohol ≤1 time a month and 55.8% did not answer the question. A total of 55% had used hashish at some point in their life and 8.4% had used hashish during the last year before pregnancy.
Study participant characteristics, reproductive factors and lifestyle (N=373).
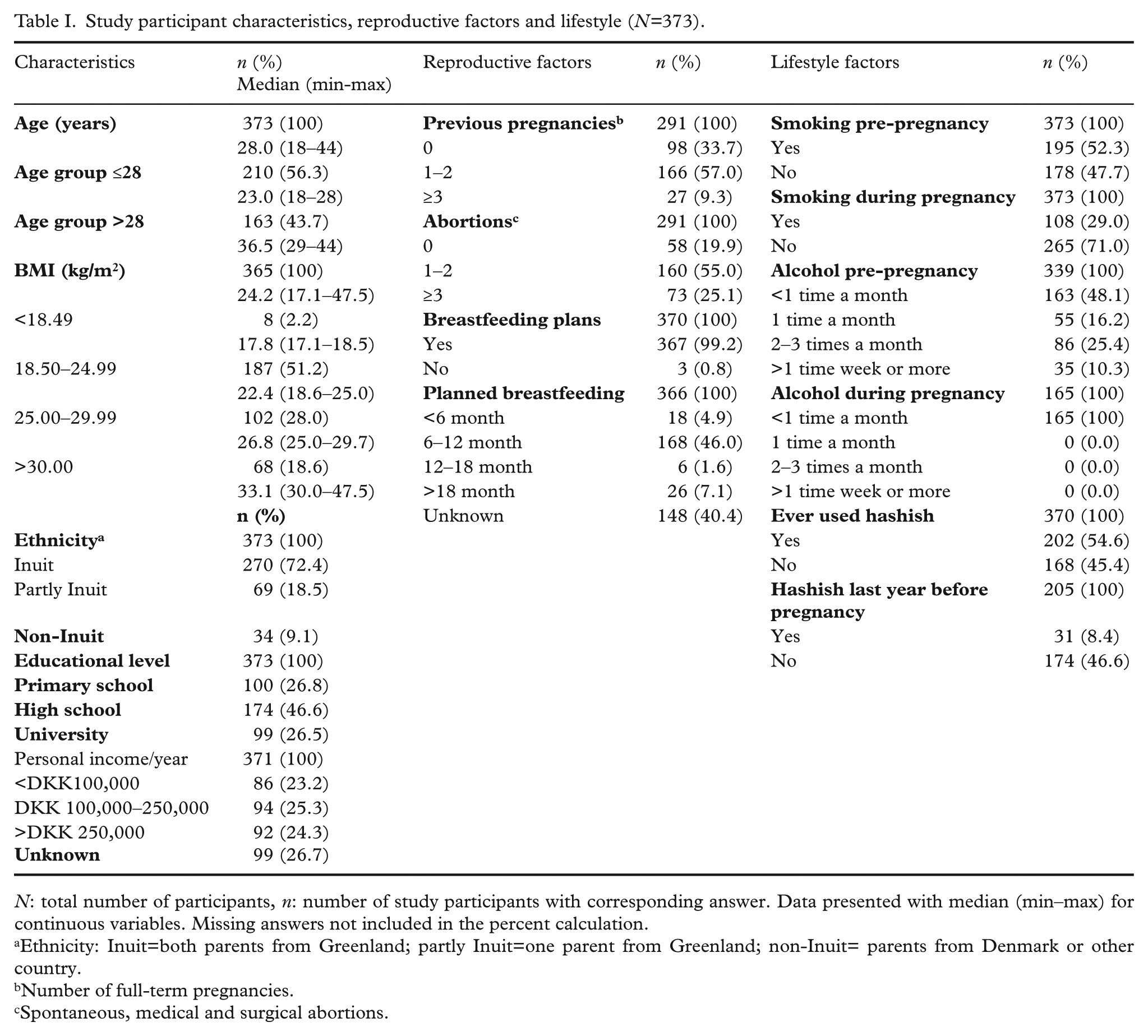
N: total number of participants, n: number of study participants with corresponding answer. Data presented with median (min–max) for continuous variables. Missing answers not included in the percent calculation.
Ethnicity: Inuit=both parents from Greenland; partly Inuit=one parent from Greenland; non-Inuit= parents from Denmark or other country.
Number of full-term pregnancies.
Spontaneous, medical and surgical abortions.
The overall intake of traditional and imported food for all participants was 12% and 88%, respectively (Table II). Marine mammals and fish were the most frequently consumed traditional food items with a median intake of 5.5 and 5.0 times a month, respectively. Carbohydrate food, fruit, and sweets and snacks were the most frequently consumed imported food items with a median intake of 39.0, 30.7 and 26.7 times a month, respectively (Table II).
Traditional and imported food: median intake times a month.
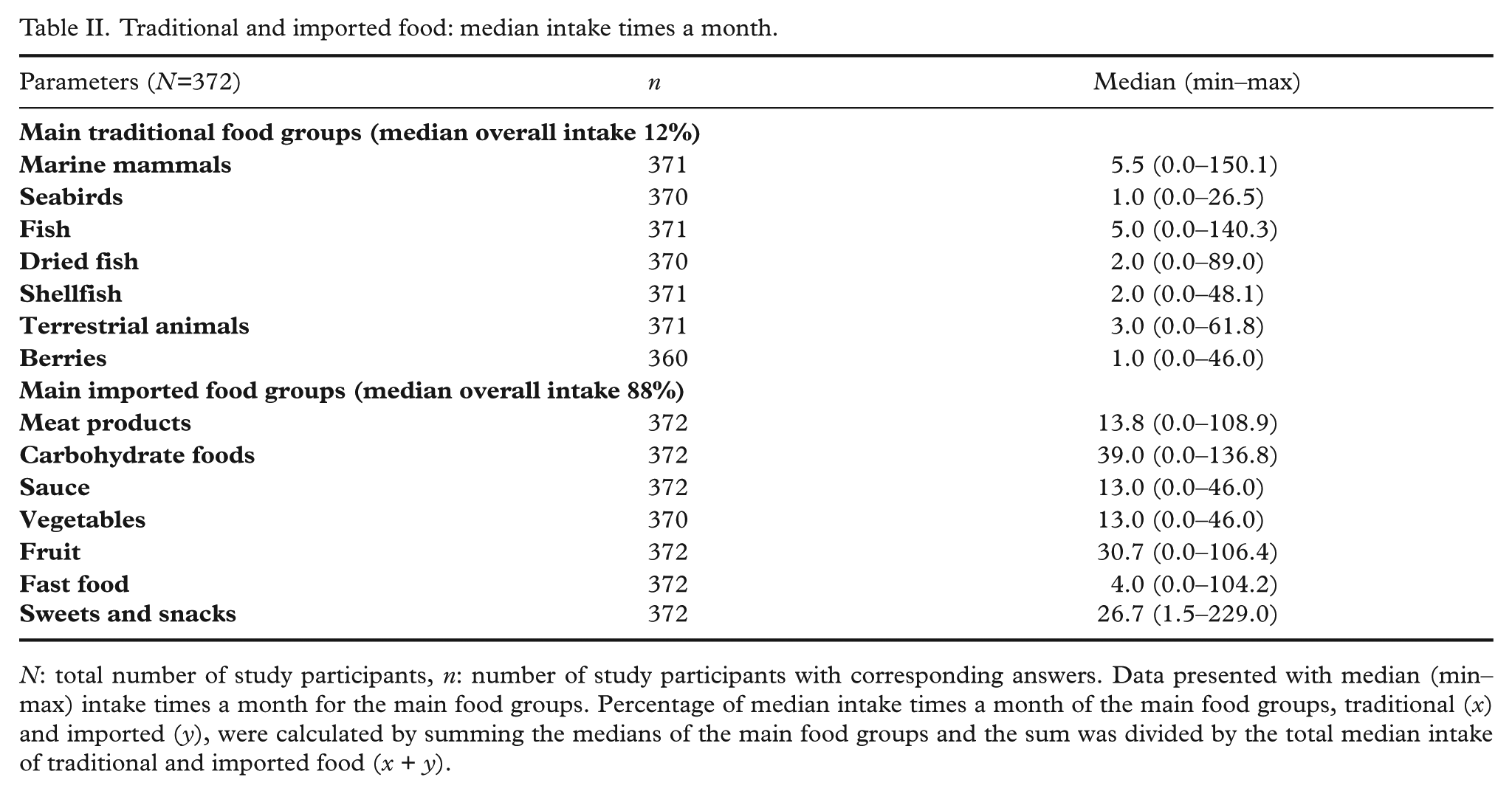
N: total number of study participants, n: number of study participants with corresponding answers. Data presented with median (min–max) intake times a month for the main food groups. Percentage of median intake times a month of the main food groups, traditional (x) and imported (y), were calculated by summing the medians of the main food groups and the sum was divided by the total median intake of traditional and imported food (x + y).
Comparison of study participant characteristics, reproductive factors and lifestyle between age groups is presented in Table III. On the basis of median age at inclusion, participants were divided into two age groups for statistical analysis of possible differences between the groups: ≤28 and >28 years of age. A significant difference between age groups was found for BMI, ethnicity, educational level, personal income/year, previous pregnancies, planned breastfeeding period and hashish use before pregnancy: In general, BMI, educational level, personal income per year, previous pregnancies and planned breastfeeding period were significantly higher among participants in the age group >28 years of age, whereas hashish use during the last year before pregnancy was higher in the age group ≤28 years of age. A borderline significant difference was seen for dried fish between the age groups with participants in the age group ≤28 years of age having a more frequent intake of dried fish (p=0.078) (Supplementary V).
Study participant characteristics, reproductive factors and lifestyle: age comparisons.
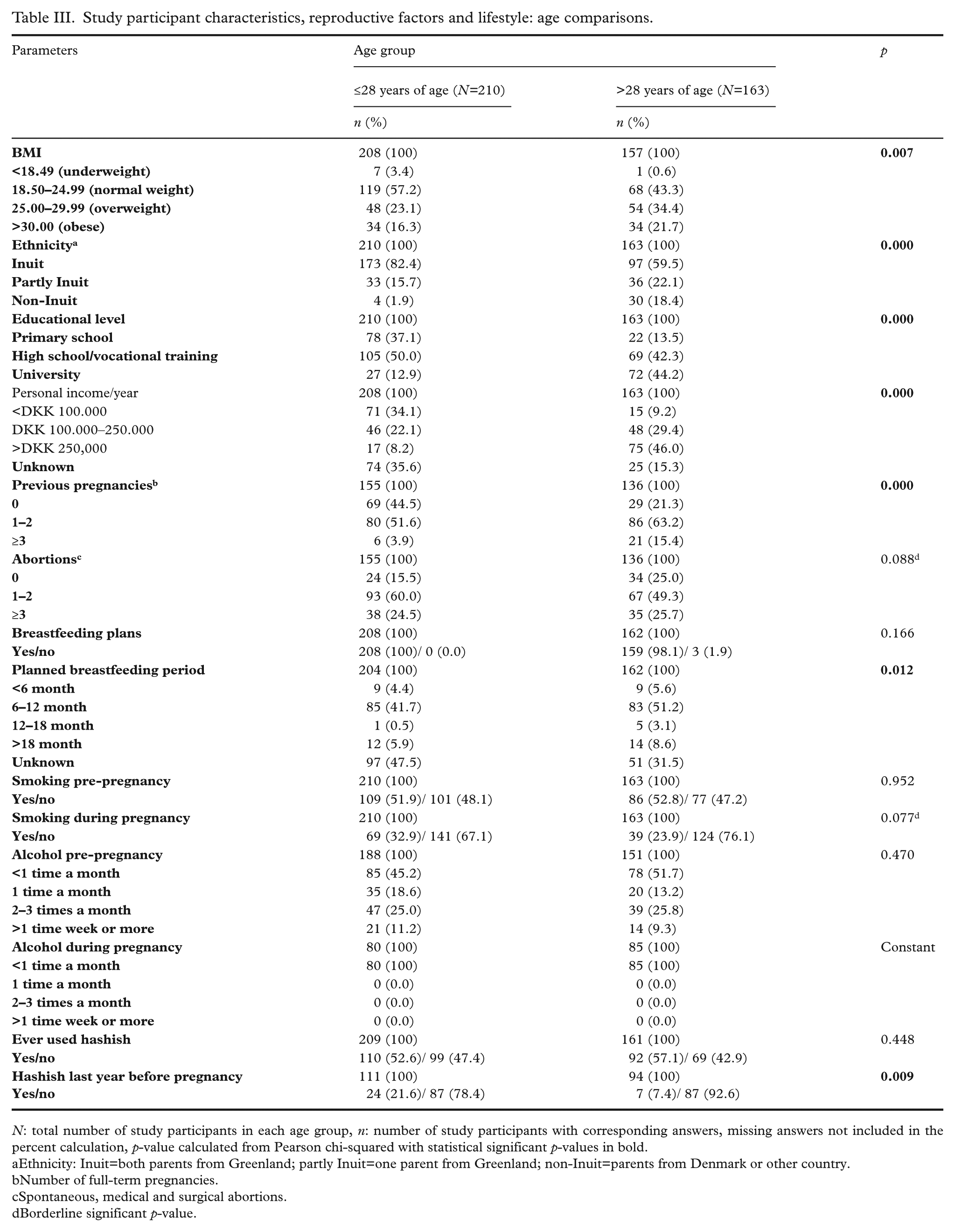
N: total number of study participants in each age group, n: number of study participants with corresponding answers, missing answers not included in the percent calculation, p-value calculated from Pearson chi-squared with statistical significant p-values in bold.
Ethnicity: Inuit=both parents from Greenland; partly Inuit=one parent from Greenland; non-Inuit=parents from Denmark or other country.
Number of full-term pregnancies.
Spontaneous, medical and surgical abortions.
Borderline significant p-value.
Regional comparisons of study population characteristics, reproductive factors and lifestyle are presented in Tables IV and V. A significant difference between regions was found for ethnicity, educational level, previous pregnancies and smoking: 90.9% of the participants from region Disko Bay were Inuit while 13.8% were of non-Inuit descend in region West. A higher educational level (high school and university) was found among participants in the following order: Region South >West >Disko Bay >North and East. The highest number of previous pregnancies among participants was found in the order: Region East >South >Disko Bay >West and North. Smoking before pregnancy was most common among participants from region Disko Bay >North >West >South and East, while smoking during pregnancy was most common among participants from region East >South >North >Disko Bay and West.
Study participant characteristics, reproductive factors: region comparisons.
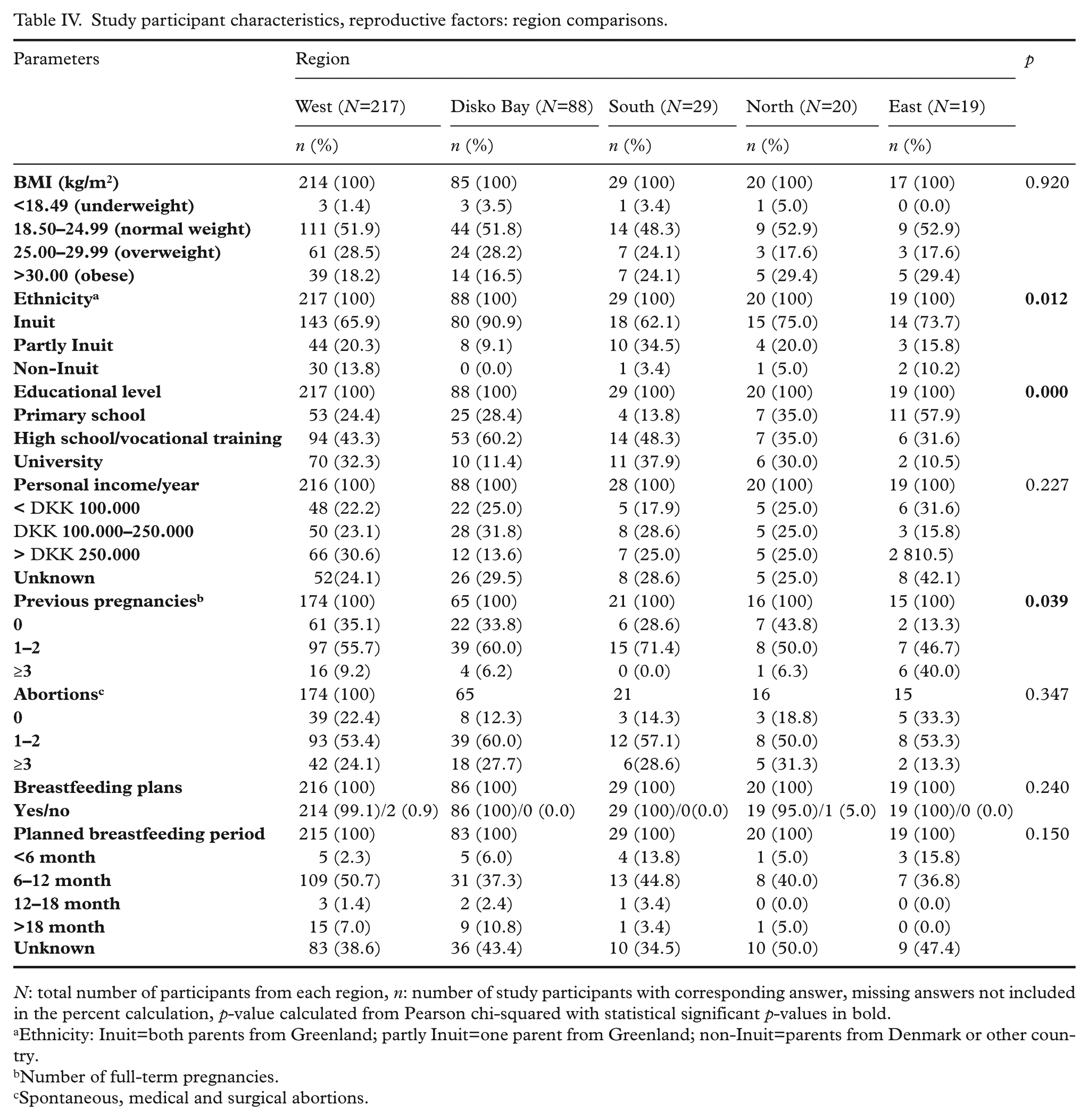
N: total number of participants from each region, n: number of study participants with corresponding answer, missing answers not included in the percent calculation, p-value calculated from Pearson chi-squared with statistical significant p-values in bold.
Ethnicity: Inuit=both parents from Greenland; partly Inuit=one parent from Greenland; non-Inuit=parents from Denmark or other country.
Number of full-term pregnancies.
Spontaneous, medical and surgical abortions.
Study participant lifestyle: region comparisons.
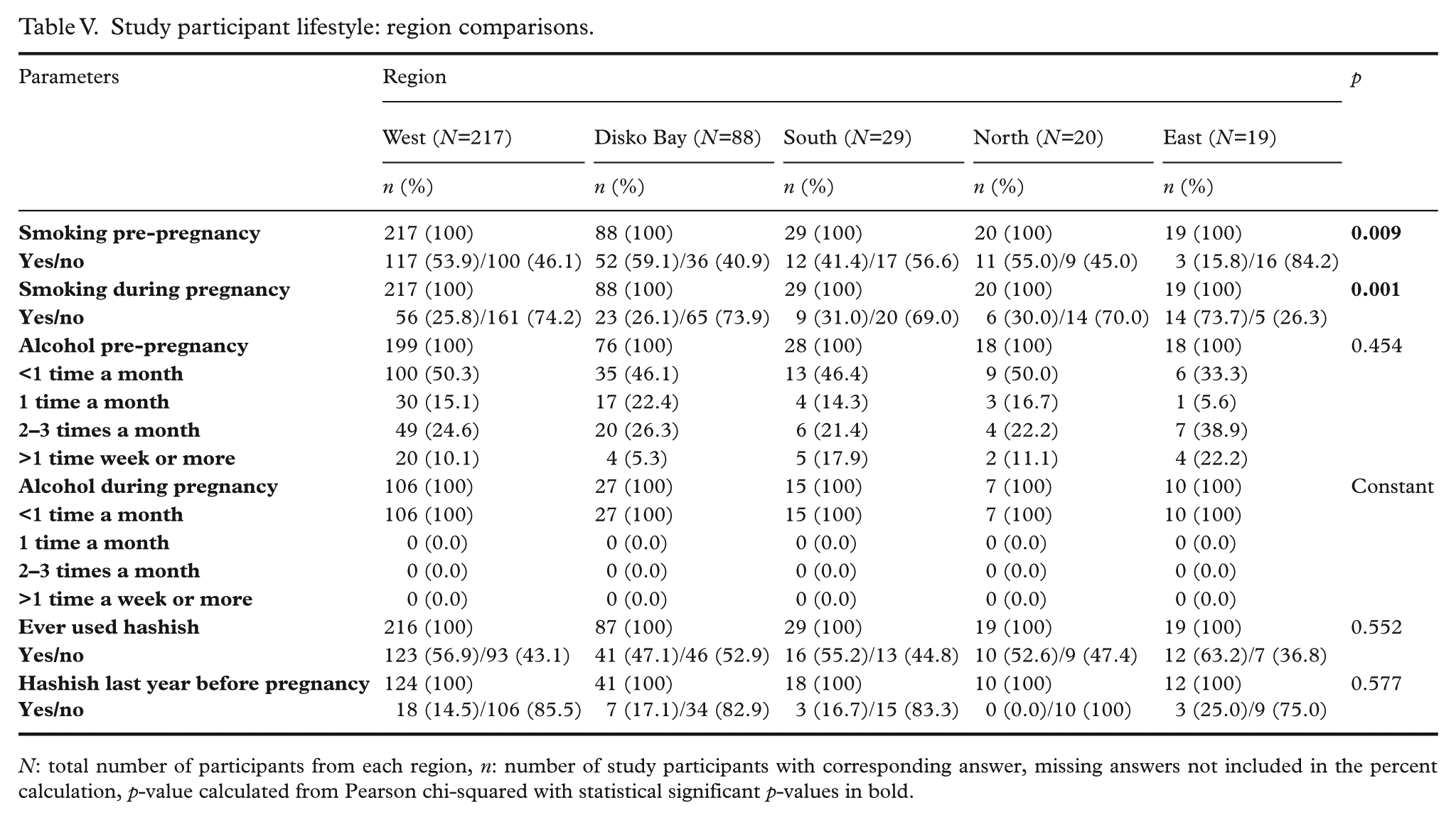
N: total number of participants from each region, n: number of study participants with corresponding answer, missing answers not included in the percent calculation, p-value calculated from Pearson chi-squared with statistical significant p-values in bold.
Regional comparisons of dietary habits are presented in Table VI. A statistically significant difference was observed for sauce with hot meals (p=0.047) and fast-food (p=0.017) with participants from region East having higher intake of both. A borderline significant difference (p=0.053) was observed for carbohydrate food with participants from region Disko Bay, South and East having the highest intake.
Median traditional and imported food intake times a month: region comparisons.
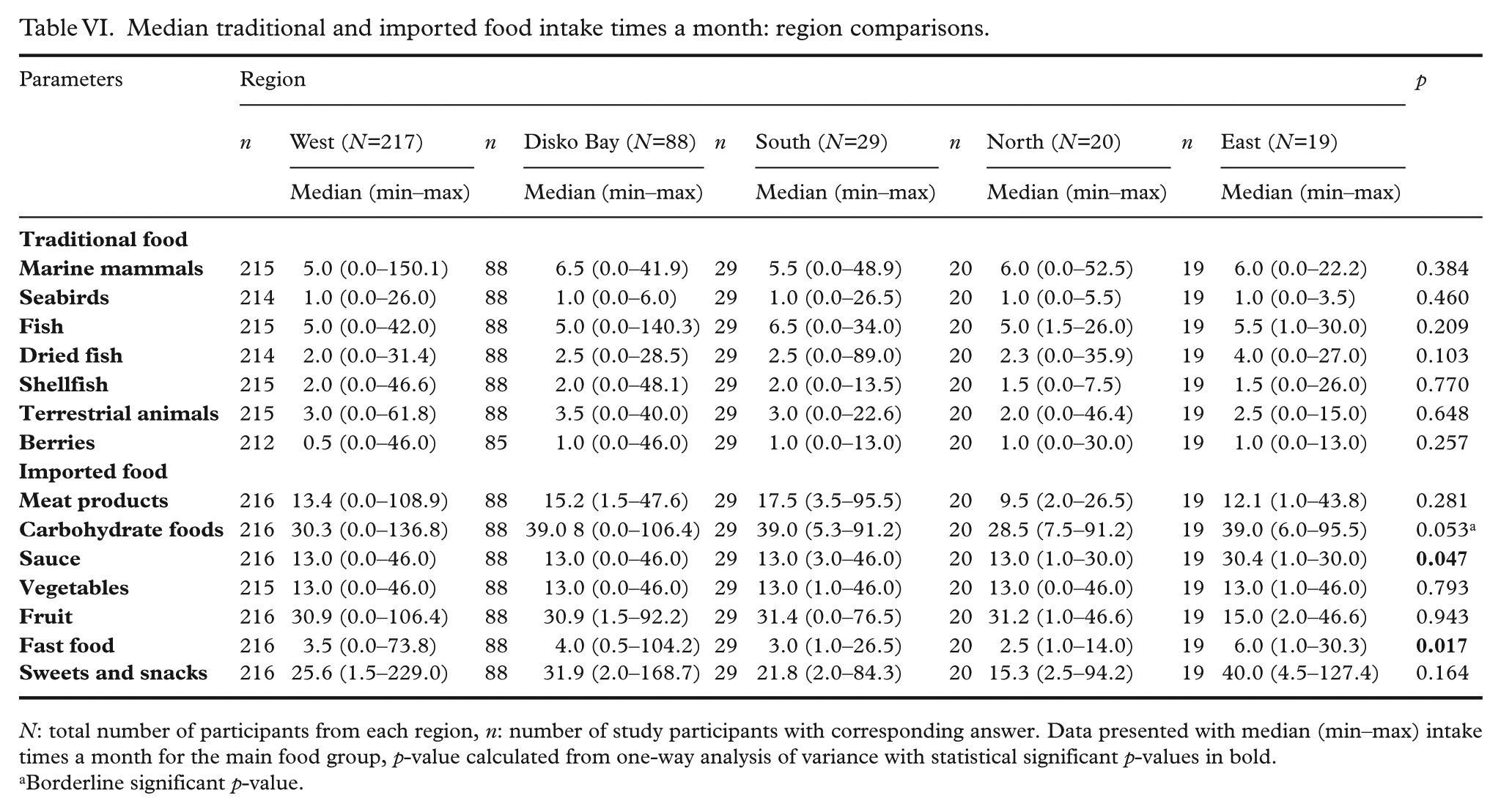
N: total number of participants from each region, n: number of study participants with corresponding answer. Data presented with median (min–max) intake times a month for the main food group, p-value calculated from one-way analysis of variance with statistical significant p-values in bold.
Borderline significant p-value.
Discussion
In total, 46.6% of the participants had a BMI >25.0 kg/m2 (median 24.2 kg/m2, range 17.1–47.5) at inclusion. High BMI levels during pregnancy have been associated with various adverse pregnancy outcomes such as preterm birth, fetal defects and congenital anomalies [17, 18]. Of the 374 participants, 89.4% were recruited in the first trimester of pregnancy, and we do not think that a pregnancy-associated weight gain can explain the generally higher BMI levels among the participants. Similar high BMI levels (43.3% > 25.0 kg/m2) were also observed for the 189 participants in the ACCEPT sub-study recruited during 2010–2011 [12]. To avoid an overestimation of overweight and obesity it has, however, been suggested that Inuit body proportions should be evaluated with regard to abdominal circumference, muscle mass, fat distribution and torso proportion, as it differs from Caucasian body proportions [19]. A review investigating BMI among Inuit in Greenland during 1963–1998 suggested a 10% raised BMI cut-off point for the Inuit population [20].
Almost all (99.2%) participants planned to breastfeed their child, and 54.7% planned to breastfeed for the recommended ≥ 6 months, but 40.4% were in doubt about the duration of the planned breastfeeding period. As several studies have reported the benefits of breastfeeding such as better cognitive development in the offspring and lower risk of obesity and diabetes in mother and child [21], an effort should be made to reach the group of women who are unsure about the duration of the planned breastfeeding and communicate the benefits of breastfeeding for the recommended ≥6 months [22].
In the present study, 29% reported to be smoking during pregnancy. This is a significant decrease compared to previous studies, where 45–60% of the Greenlandic pregnant women were smoking during pregnancy [12, 23]. As both short- and long-term adverse health effects of maternal smoking have been reported, the number of women who smoke during pregnancy is still too high and efforts should be made to reduce the number of smokers [24].
Alcohol consumption decreased to <1 time a month during pregnancy for all participants who had reported their alcohol consumption (44%). In the remaining 56% of the pregnant women, alcohol consumption during pregnancy is unknown. The LQ lacked an option to answer, ‘0 times a month’ and thus the result might be skewed. The result is, however, consistent with the previous ACCEPT sub-study 2010–2011 in which 96.8% of the participants consumed alcohol < 1 time a month during pregnancy and the IVAAQ Greenlandic child cohort 1999–2005, where 92.4% refrained from drinking alcohol during pregnancy [12, 23]. We therefore assume that the majority of participants significantly reduced or stopped their alcohol intake during pregnancy. The intake of traditional food among all participants constituted 12%. Compared to earlier studies investigating dietary habits in Greenland, there is a clearly decreasing intake of traditional food over time [6, 12, 25]. Despite the decreasing trend, the frequent intake of marine mammals is of concern, as this food group has some of the highest levels of POPs [7]. POPs can cross the placenta barrier during pregnancy and be passed on to the infant through breastfeeding [26]. The Greenlandic Nutritional Council recommends that pregnant and breastfeeding women decrease their intake of specific marine mammals and replace these with e.g. fish [27] – high in omega 3 fatty acids and vitamin D and low in POPs [28]. Receiving dietary advice after becoming pregnant may not be timely to avoid the adverse health effects; recommendations should thus be given long before pregnancy [29].
Age groups
Participants in the age group >28 years of age had a higher BMI, higher parity, and fewer were in doubt regarding the duration of planned breastfeeding period. Similar patterns were observed in the ACCEPT sub-study 2010–2011[12]. As BMI seems to increase with age, interventions should focus on maintaining normal weight throughout pregnancy and adulthood. The experience with breastfeeding and associated knowledge of benefits in the older age group should be communicated to younger women in the childbearing age to reduce their uncertainty about the duration of breastfeeding.
In the age group ≤28 years of age the use of hashish during the last year before pregnancy was higher than in the age group >28 years of age (21.6% vs. 7.4%). As the lifestyle questionnaire did not contain questions regarding the use of hashish during pregnancy, the extent of this problem is unknown. Hashish use during pregnancy has been associated with adverse birth outcomes such as lower birth weight and small for gestational age [30, 31]. The latest population survey in Greenland report a decrease in hashish use among young women from 2005–2014 [1], but as hashish use before and during pregnancy still seems high, it should be further investigated to make suitable interventions.
Regions
The percentage of participants living for the longest time in each particular region was considered representative of the population in the respective regions. Participants from region East had the lowest educational level, and the highest prevalence of smokers during pregnancy (73.7%). This is in agreement with the latest population survey in Greenland where the prevalence of daily smokers was higher among people living in region East, who had no further education than primary school [1]. To reduce the number of smokers, interventions should be targeted specifically at women in the childbearing age in region East.
As shown in the present study, a frequent intake of sauce with hot meals and fast-food among participants from region East was also observed in the ACCEPT sub-study 2010–2011 (12). This may be due to ingrained habits of consuming sauces, often high in fat and salt, with every meal and limited availability of healthy alternatives. These tendencies are worrying and efforts should be made to promote the intake of more healthy food items.
Method limitations
In the FFQ, participants were asked about their dietary habits before pregnancy as these were believed to optimally describe normal dietary pattern unaffected by pregnancy. Recall bias may, however, occur, as the time before pregnancy is an indefinite period to remember. A 24-hour dietary recall scheme as a supplement to the FFQ may reduce potential recall bias [32].
As participants were interviewed at different times of the year, the reporting of dietary intake might be affected by seasonal variation. Many traditional food items are only available from the natural environment during certain periods of the year. Also, the imported food items are affected by seasonal variation in remote areas, as the supply of fresh food is limited during the winter.
Summary and conclusions
The pregnant women in the present study had a relatively high BMI and a high smoking frequency, together with a high intake of imported food items. Women >28 years of age had a higher BMI and planned to breastfeed for a longer time than women ≤28 years of age. Pregnant women in region East had a higher smoking frequency and consumed sauce with hot meals and fast-food more often than women in the other regions. Interventions aimed at pregnant women in the future should focus even more on the risk of smoking during pregnancy, the benefits of breastfeeding, and promote healthy eating habits including non-fat healthy traditional food items.
Supplemental Material
Supplemental Material for Reproductive factors, lifestyle and dietary habits among pregnant women in Greenland: The ACCEPT sub-study 2013–2015
Supplemental material, supp_mat_714188 for Reproductive factors, lifestyle and dietary habits among pregnant women in Greenland: The ACCEPT sub-study 2013–2015 by Anne Seneca Terkelsen, Manhai Long, Lise Hounsgaard and Eva Cecilie Bonefeld-Jørgensen in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
We would like to thank all members of Centre of Arctic Health & Molecular Epidemiology, Department of Public Health, Aarhus University for scientific support. The authors would also wish to thank all the participating pregnant women; the involved staff at the hospitals in Greenland, especially midwives helping to enroll the pregnant women and supervising in questionnaires. A special thanks to Head of the Institute (now substitute rector of University of Greenland) Suzanne Moeller, Institute for Nursing and Health Science, University of Greenland, Nuuk, Greenland for coordination support in Greenland.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
ACCEPT is financially supported by the Danish Environmental Protection Agency (MST-112-00225), the Danish Council for Strategic Research (grant No. 10-092818) and the cross-faculty Arctic Research Centre at Aarhus University.
References
{kind=link}
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.