
Abstract
Keywords
Introduction
The prevalence of edentulism decreased from 51% to 12% among 70-year-olds in Gothenburg, Sweden between 1971 and 1992 [1] and decreased from 53.3 % to 35.7% in Umeå, Sweden, between 1981 and 1990 [2]. Similar decreases in edentulism prevalence have been found in other large population-based studies from Sweden [3, 4] and other countries [5, 6]. The prevalence of removable denture use has decreased over the years [1, 2, 7] but the prevalence of dental implants seems to be growing [1, 5, 8]. The trend towards decreasing edentulism has benefited older people by improving chewing ability, oral function and self-esteem [1, 4, 9]. The utilization of dental care among elderly people has increased over time as well [10, 11]. Despite the recent decrease in edentulism, a substantial number of people live with edentulism and are in need of dental care.
With increasing age, there is a corresponding increase in the factors that increase the risk of losing teeth due to periodontal disease and caries [5, 12, 13]. Thus, it is especially important to maintain good oral hygiene and oral health as people age. The correlation between edentulism and general health is complex. Diabetes may increase an adult’s risk of developing periodontal disease and dry mouth [14–16]. Cognitive impairment may increase the risk of losing teeth and chewing ability [16–18]. Conversely, edentulism may lead to cardiovascular disease or stroke, which, in turn, may aggravate cognitive impairment [17, 19, 20]. Edentulism is also associated with poor quality of life [21].
In addition to health factors, socioeconomic and demographic factors have been associated with edentulism and the use of dental care [11, 22]. Low educational level, low income and residence in a rural area are associated with not visiting a dental facility and with edentulism [11, 22–27]. Some older studies found that there were more edentulous women than men, but more recent studies do not show this difference based on sex [1, 2, 13, 28]. Prevalence of edentulism differs between countries [29] and probably by region within countries as well [1, 2].
The increasing number of people who retain their own teeth as they age means that more people will be at risk of developing periodontal disease and caries in the future [7]. The rapid increase in the elderly population as a result of medical advances and increased prosperity may make this change even more pronounced [30]. Elderly people have increased prevalence of several risk factors thought to lead to edentulism. Thus, a demographic shift towards a larger proportion of elderly people in the population might have extensive effects on oral health. Furthermore, many studies of edentulism are dated.
In light of this background, it is important to investigate which factors are associated with edentulism and the extent of edentulism in the current setting. This information would be useful for developing future strategies for dental care prevention.
The primary aim of this study was to describe the prevalence of edentulism and the uses of removable dentures, dental implants and dental services in a representative sample of people aged 65 years or older in northern Sweden and western Finland. The secondary aim was to investigate which socioeconomic and health risk factors are associated with edentulism and use of dental services in these populations.
Materials and methods
Setting
This study is based on the GERDA study [31], a population-based study of people aged 65, 70, 75 and 80 years old and living in one of 15 municipalities in Västerbotten, Sweden, or one of 17 municipalities in Österbotten, Finland. The study and data collection were carried out in 2010. The project was approved by the Regional Ethics Review Board of Umeå (Dnr 05-084Ö/2010-220-320).
Participants
Of the 10,696 people aged 65, 70, 75 and 80 years to whom the GERDA questionnaire was sent, 6838 responded (63.9% response rate). The response rate was 70.7% (3799/5426) in Sweden and 58.0% (3059/5270) in Finland. Those who answered ‘yes’ or ‘no’ to the question “Do you mainly have your own permanent teeth left?” were selected for inclusion in this study, giving a final sample size of 6099 people.
Procedures
The survey was randomly mailed to every third person in the urban municipalities of Skellefteå and Umeå, to every second person in the urban municipality of Vaasa, and to every person in the other municipalities, for the investigated age groups, based on records from the Swedish Tax Agency and the Finish Population Register Centre. A second copy of the questionnaire was sent 1 month after the first mailing as a reminder to those who had not responded. A returned survey from the participant was considered to indicate consent to participate in the study.
Definition of edentulism
The survey posed the following questions, which could be answered with ‘yes’ or ‘no’:
Do you mainly have your own permanent teeth left?”
Do you wear dentures?”
Do you have dental implants?”
Have you visited a dentist in the preceding year?”
Edentulism was defined as a ‘no’ response to the question about mainly having one’s own permanent teeth left.
Diagnosis and definitions
Sociodemographic information regarding sex, domicile, economy, education and living situation was collected from all participants. Educational level was categorized by number of years of school attended and dichotomized as a higher educational level (≥9 years) or a lower educational level (<9 years). Information about economy was elicited by the question “Do you make ends meet?” The answer options were ‘with no difficulties’, ‘some difficulties’, ‘rather difficult’ or ‘very difficult’, with the two latter answers being considered indicative of a low income level. A question of living situation was dichotomized as ‘living alone’ or ‘not living alone’. Participants answered ‘yes’ or ‘no’ to questions about their medical history (diabetes, stroke, myocardial infarction and high blood pressure). A question about self-experienced health from the Swedish version of the SF-36 was dichotomized as ‘good self-experienced health’ or ‘poor self-experienced health’.
The four-item version of the Geriatric Depression Scale was used as a measure of depression. This scale has a high sensitivity and is useful in detecting depression among old people [32]. Questions about personal activities of daily living (P-ADLs), instrumental activities of daily living (I-ADLs), loneliness and social activity were asked. Participants who were unable to shower independently were considered as dependent in P-ADLs. Participants who were unable to clean their home, shop for food or cook independently were considered as dependent in I-ADLs.
A question about loneliness (‘Do you suffer from loneliness?’) was answered with either ‘yes’ or ‘no’. Participants were asked about outdoor activity; not having been outdoors for a week was classified as ‘no activity outdoors’. Participants were asked about social contact; if they never had any contact with neighbours or friends, they were classified as ‘socially isolated’.
Statistics
The IBM SPSS Statistics 22 package was used for statistical analyses. Univariate comparisons between proportions were analysed using the Pearson chi-square test. Comparisons between means were performed with Student’s t test. Participants with missing responses to the questions ‘Do you wear dentures?’ and ‘Do you have dental implants?’, who also answered ‘yes’ to the question ‘Do you have mainly your own permanent teeth left?’ were categorized as having answered ‘no’ to the questions about dental implants and dentures.
In the epidemiologic presentation (Table I), prevalence figures were weighted to make the data more representative in the selected age groups in Västerbotten, Sweden, and Österbotten, Finland. Weighting was performed by counting the number of participants in Umeå and Skellefteå (Sweden) thrice and the number of participants in Vasa (Finland) twice. Factors associated with the dependent variable in univariate analyses were tested in multivariate logistic regression analyses. Results from the logistic regression analyses were presented as odds ratios (ORs) and 95% confidence intervals (CIs). A significance level of p < 0.05 was used.
Prevalence of edentulism, denture use, dental implants and not having visited a dentist in the preceding year.
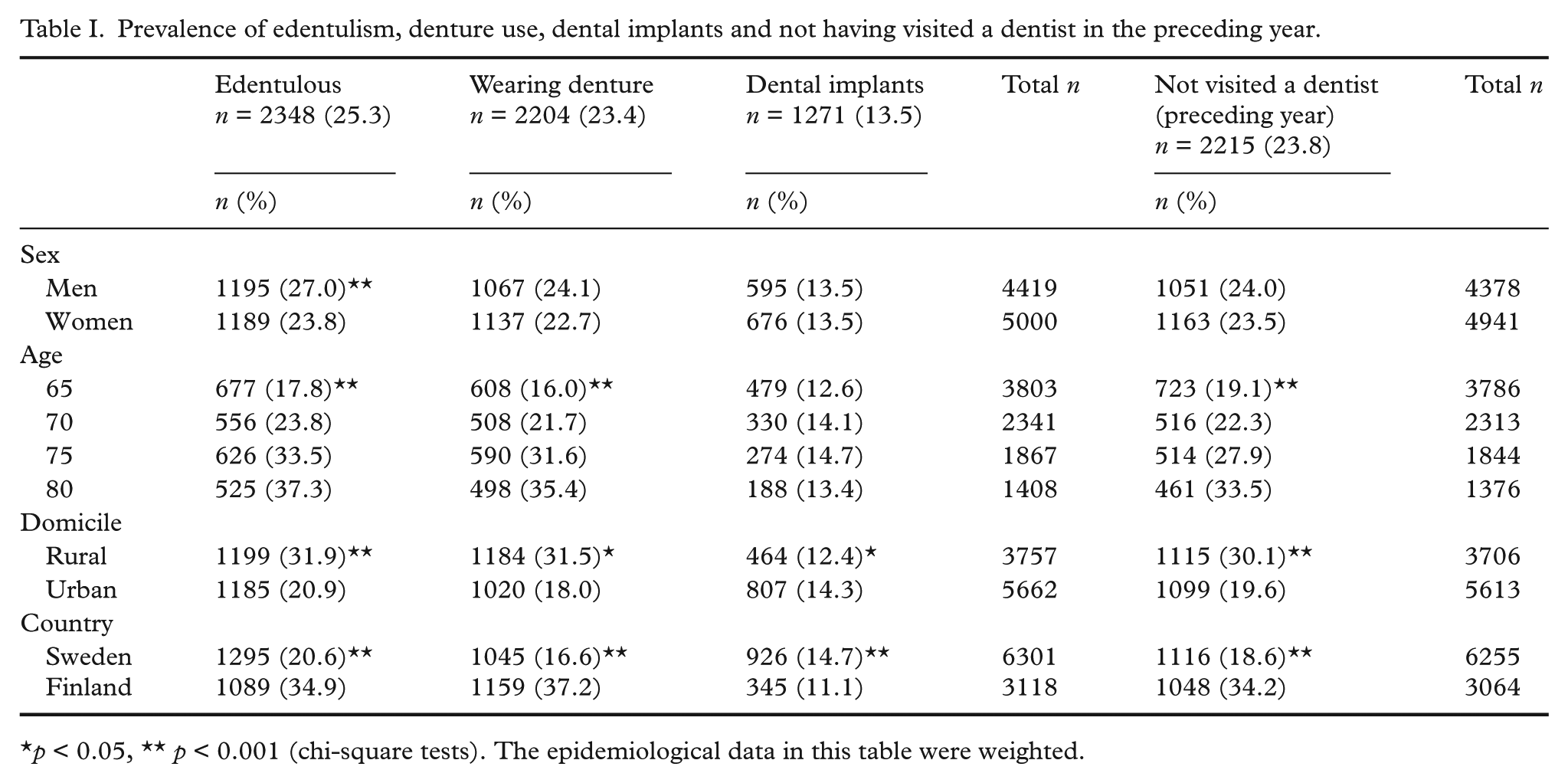
p < 0.05, ** p < 0.001 (chi-square tests). The epidemiological data in this table were weighted.
Results
Epidemiology
In the total sample, 27.0% of men were edentulous compared with 23.8 % of women (p < 0.001) (Table I), resulting in a 25.3% prevalence overall. Nearly one-quarter of 70-year-olds were edentulous. Among 70-year-olds, 20.1% of Swedes and 32.5% of Finns were edentulous (p < 0.001). Men and women had similar rates of edentulism in Sweden and Finland. Among 70-year-old Swedes, 21.9% of men and 18.5% of women were edentulous (p = 0.085). Among 70-year-old Finns, 35.6 % of men and 29.6 % of women were edentulous (p = 0.091). Among 70-year-olds in Umeå, Sweden, 15.0% of men and 16.3% of women were edentulous (p = 0.656). Among 75-year-old Swedes, 28.1 % were edentulous, compared with 44.0 % of Finns in the same age group (p < 0.001).
The prevalence of edentulism increased with age (p < 0.001), as did the rates of denture use (p < 0.001) and no dental visit in the preceding year (p < 0.001). The prevalence of edentulism (p < 0.001) and denture use (p < 0.05) was higher among people living in rural areas, who did not visit a dentist as often as people living in urban areas (p < 0.001). The prevalence of dental implants was higher among people living in urban areas than in people living in rural areas (p < 0.05) (Table I).
Prevalences of edentulism (p < 0.001) and denture use (p < 0.001) were higher in Finland than in Sweden, but dental implants were more common in Sweden (p < 0.001). Finnish respondents were less likely than Swedish respondents to have visited a dentist during the preceding year (p < 0.001) (Table I).
Factors associated with edentulism
In univariate analyses, edentulism was associated with living in a rural area (p < 0.001), male sex (p = 0.010), increasing age (p < 0.001), low income level (p < 0.001), lower educational level (p < 0.001), poor self-experienced health (p < 0.001), diabetes (p < 0.001), depression (p < 0.001), myocardial infarction (p < 0.001), high blood pressure (p = 0.044), stroke (p = 0.014) living alone (p < 0.001), social isolation (p = 0.002), loneliness (p < 0.001), dependence in I-ADLs (p < 0.001) and P-ADLs (p = 0.001) (Table II).
Factors associated with edentulism and denture use in univariate analyses.
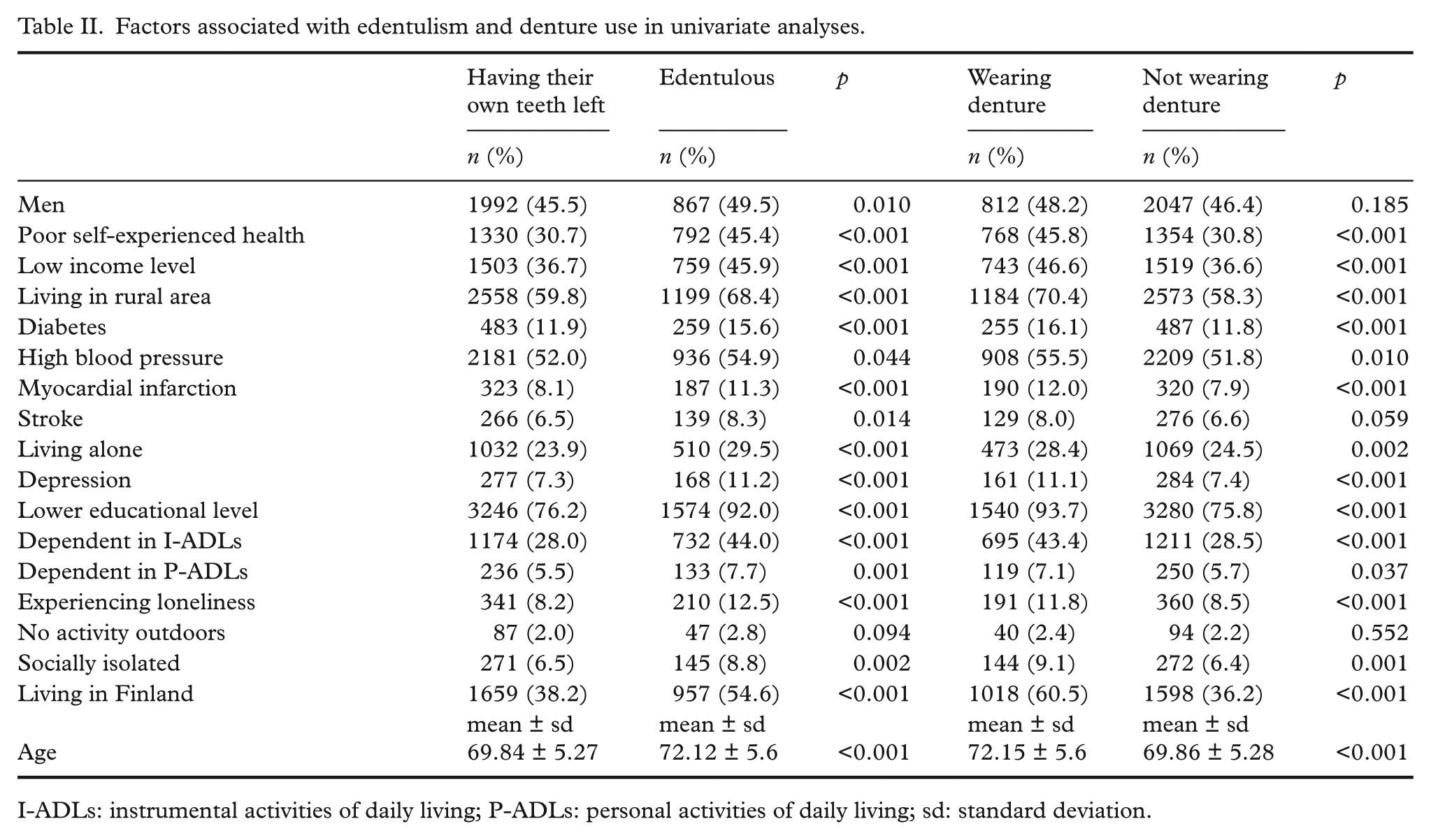
I-ADLs: instrumental activities of daily living; P-ADLs: personal activities of daily living; sd: standard deviation.
Denture use was associated with living in a rural area (p < 0.001), increasing age (p < 0.001), low income level (p < 0.001), lower educational level (p < 0.001), poor self-experienced health (p < 0.001), diabetes (p < 0.001), depression (p < 0.001), myocardial infarction (p < 0.001), high blood pressure (p = 0.010), living alone (p = 0.002), social isolation (p = 0.001), loneliness (p < 0.001) and dependence in I-ADLs (p < 0.001) and P-ADLs (p = 0.037) (Table II).
Not having visited a dentist during the preceding year was associated with edentulism (p < 0.001), denture use (p < 0.001), lower dental implant use (p < 0.001), living in a rural area (p < 0.001), increasing age (p < 0.001), low income level (p < 0.001), lower educational level (p < 0.001), poor self-experienced health (p < 0.001), diabetes (p < 0.001), depression (p = 0.014), myocardial infarction (p < 0.001), high blood pressure (p < 0.001), living alone (p < 0.001), social isolation (p < 0.001), loneliness (p < 0.001), dependence in I-ADLs (p < 0.001) and in P-ADLs (p = 0.006) and lack of outdoor activity (p = 0.020). (Table III).
Factors associated with not having visited a dentist in the preceding year in univariate analyses.
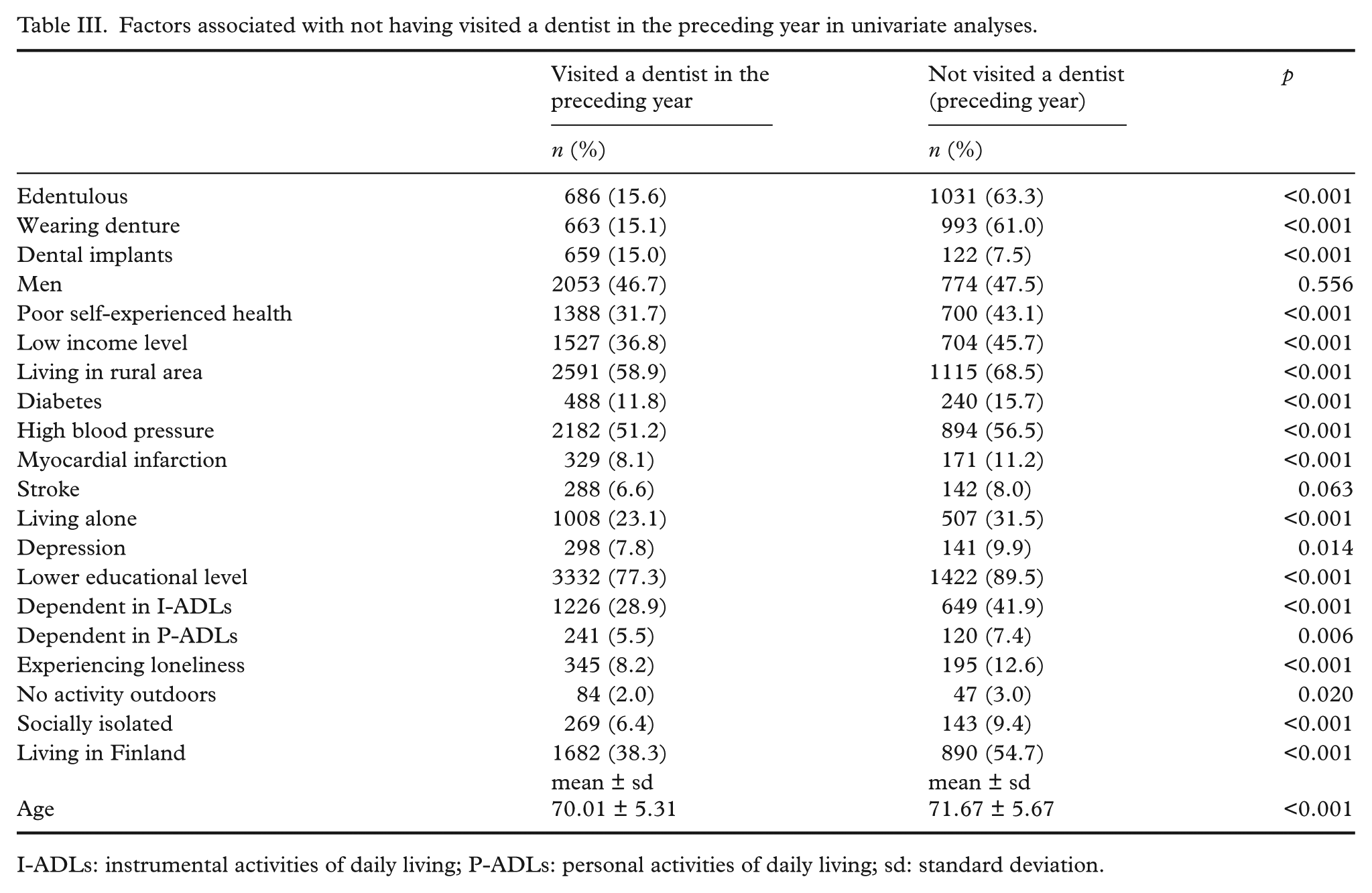
I-ADLs: instrumental activities of daily living; P-ADLs: personal activities of daily living; sd: standard deviation.
In multivariate analyses (Table IV), edentulism was independently associated with male sex, having poor self-experienced health, low income level, living in a rural area, lower educational level, dependence in I-ADLs, social isolation and increasing age. Denture use was independently associated with poor self-experienced health, low income level, living in a rural area, lower educational level, dependence in I-ADLs, social isolation and increasing age. Not having visited a dentist during the preceding year was independently associated with edentulism, denture use, living in a rural area, living alone and social isolation. Having dental implants was also associated with more frequent dental visits (p < 0.001).
Factors associated with edentulism, denture use and not having visited a dentist in the preceding year in multivariate analyses.
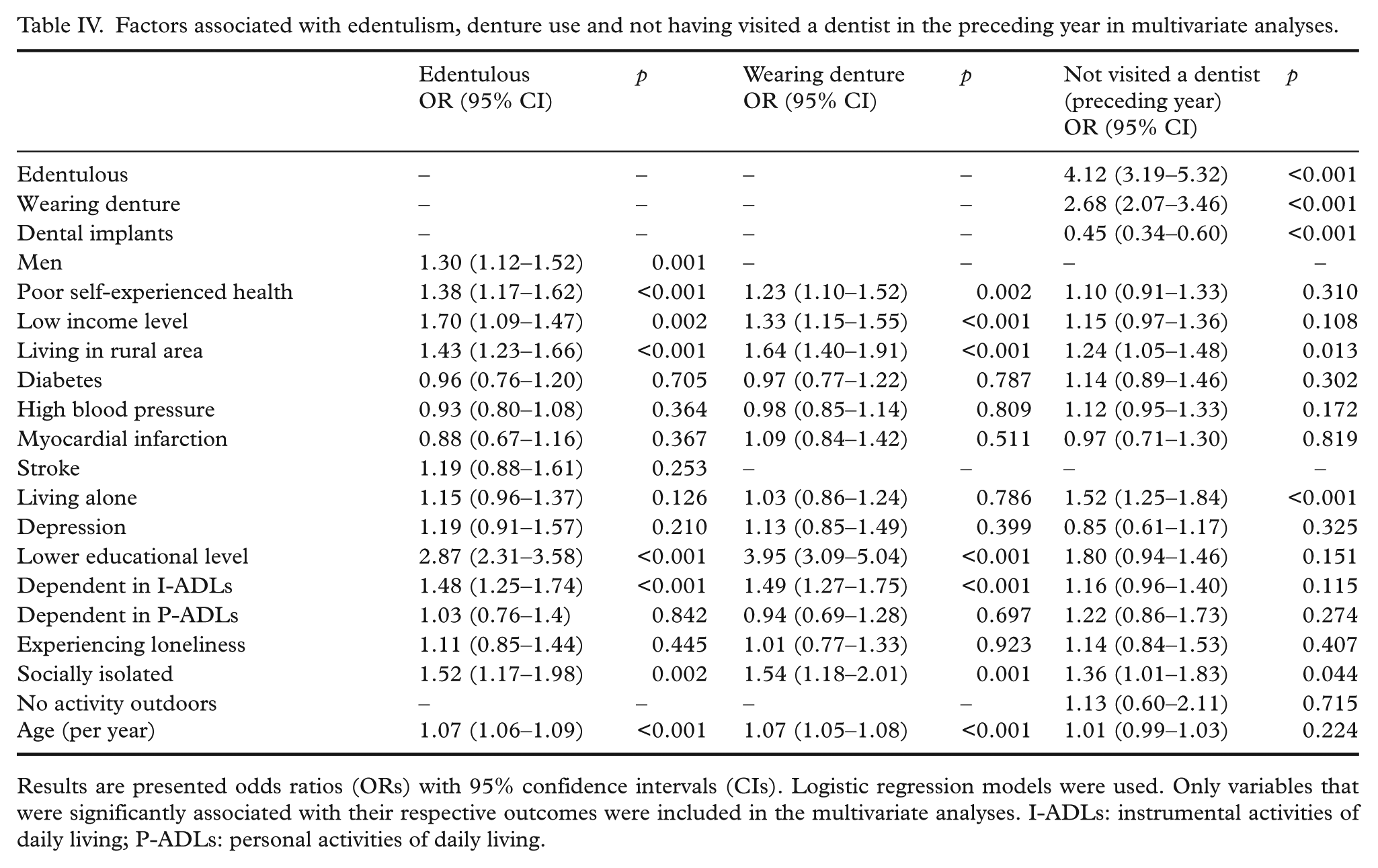
Results are presented odds ratios (ORs) with 95% confidence intervals (CIs). Logistic regression models were used. Only variables that were significantly associated with their respective outcomes were included in the multivariate analyses. I-ADLs: instrumental activities of daily living; P-ADLs: personal activities of daily living.
There was a higher prevalence of dental implant use in Sweden (14.8%) than in Finland (10.4%) (p < 0.001) (Table V). Among people with dental implants, 76.6% had a lower educational level, compared with 81.4% of people without implants (p < 0.001).
Characteristics of the study sample in total, in women compared with men, and in Sweden compared with Finland.
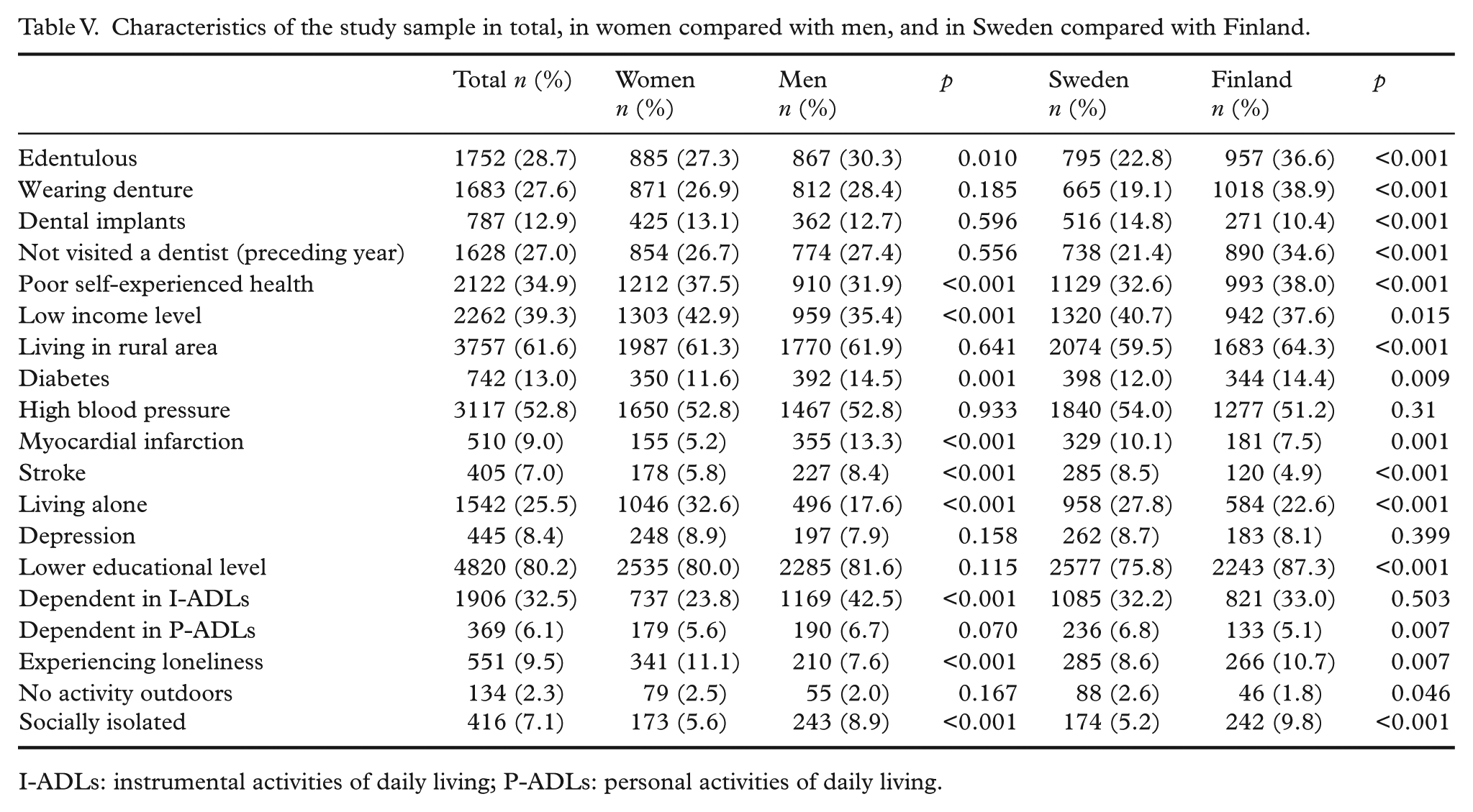
I-ADLs: instrumental activities of daily living; P-ADLs: personal activities of daily living.
Compared with men, women more often reported low income level (p < 0.001) and poor self-experienced health (p < 0.001); however, fewer women were edentulous (p < 0.01). Men reported more dependence in I-ADLs than did women (Table V).
Compared with Swedes, more Finns were edentulous (p < 0.001), living in rural areas (p < 0.001), had a low educational level (p < 0.001) or diabetes (p = 0.009), were socially isolated (p < 0.001) and experienced loneliness (p = 0.007) (Table V).
Discussion
We found a low prevalence of edentulism in Sweden compared with the prevalence reported from previous studies in the same Swedish geographical areas [2]. There were large geographical differences in edentulism prevalence between urban and rural areas, and between Sweden and Finland. Edentulism was independently associated with lower educational level, low income level, living in a rural area, male sex, dependence in I-ADLs, social isolation and poor self-experienced health.
In 2000, a study in Gothenburg reported a 7% prevalence of edentulism in 70-year-olds [1]. We found a 20.1% prevalence of edentulism in Västerbotten 10 years later in the same age group. However, results from a study using a representative sample of Swedes in 2000 showed a prevalence of edentulism ranging from 25% to 30% in people aged 65 to 76 years [3]. Our finding that 31.9% of people living in rural areas and 20.9% of people living in urban areas had edentulism is consistent with findings from earlier studies [22, 33]. There appear to be vast geographical differences in edentulism in Sweden; however, differences in study timeframes, definitions of edentulism and presentations of age-specific results complicate such comparisons. Additionally, we found no overrepresentation of women, but actually a slightly higher prevalence of edentulism among men overall, consistent with the diminished sexual divide in edentulism that has previously been reported [26, 27]. Among 70-year-olds in Västerbotten, there were 21.4% edentulous men and 35.7% edentulous women in the city of Umeå in 1990 [2], compared with our results from 2010 study data showing 15.0% edentulous men and 16.3% edentulous women in the same city and age group.
Our findings of 28.1% edentulism in Sweden and 44.0% edentulism in Finland among 75-year-olds differs from a 1989 report showing a 23% prevalence of edentulism in Gothenburg, Sweden, and a 58% prevalence in Jyväskylä, Finland [29]. Although the prevalence of edentulism may have decreased in Finland, and the regional difference may have decreased, earlier studies comparing Finland and Sweden were made in the different geographical areas.
Our study showed that edentulism and denture use were more common in Finland, whereas dental implant use and dental visits were more common in Sweden. These findings may reflect differences in health insurance and reimbursement systems for dental treatments between the two countries [34]. Public funding of dental care significantly decreases inequity in dental health [35]. Sweden introduced partial public coverage of dental care expenses in 1974, which was reduced somewhat in 1999, but still probably had a large effect on edentulism. Meanwhile, Finland introduced partial public coverage as late as 2002, which is not likely to have produced major positive cohort effects in a survey collected in 2010.
Some previous study results indicated that women visit the dentist more frequently than men [23, 24], although another study found no differences between men and women with respect to dental visits [11]. We did not see a difference in dental visit frequency between men and women. The prevalence of edentulism in women may have decreased compared with previous results [1, 2], possibly as a result of increased sexual equality in access to and quality of health care. However, women reported worse self-experienced health and lower income levels than men in our study.
Consistent with previous findings, we found strong multivariate correlations between edentulism and educational level, income level and residence in a rural area [4, 16, 22–27], as well as an association between social isolation and edentulism [36]. The same risk factors were found to be associated with denture use. Dental implant use was mainly associated with educational level. However, dental implant prevalence was lower compared with the other primary study variables, suggesting that a larger sample may have been needed to find the same associations.
The factors associated with not visiting a dentist were partly different, with no apparent associations with income level or educational level, but rural living was associated with fewer dental visits. A previous Swedish study showed the decreasing effect of socioeconomic status on dental visits over time in repeated surveys, but a significant association remained at the last measurement point in 2000 [37]. Another Swedish study showed educational level to be consistently associated with dental visits from 1992 to 2011, with no apparent attenuation of the association over time [11]. The association between rural living and fewer dental visits in this study may be explained by the differences in availability of dental clinics near participants’ homes, travel distances to the nearest dental clinic, and difficulty in accessing dental care for those with impaired health. Edentulism, denture use, living alone and social isolation were also associated with not visiting a dentist. Edentulous people may not prioritize dental visits or, alternatively, may not need regular dental care. Conversely, not visiting the dentist may lead to worse oral health and edentulism.
Previous studies have found that poor oral hygiene and oral health are associated with cardiovascular disease and stroke [16, 19–20]. However, our results do not show any significant association between edentulism or denture use and cardiovascular disease. We found a correlation between dependence in I-ADLs and edentulism. People who are dependent in I-ADLs have a greater need for mobility services, which may limit contact with dental care professionals. However, we did not find an association between I-ADL dependency and not visiting a dentist. Diabetes was not strongly associated with being edentulous, despite previous reports that diabetes increases adults’ risk of developing periodontal disease [14, 15].
One limitation of this study is that we used non-specific questions to inquire about edentulism, denture use and implants. People who answered ‘yes’ to the question about having dental implants could have a single implant or an implant-supported denture; these constructions differ markedly. Respondents may have had difficulty in understanding the question about denture use to include both partial and full dentures. Questions about degree of edentulism would be instructive in providing information about chewing abilities. A previous analysis of survey non-responders showed higher non-response rates among older people than younger people, and slightly higher non-response rates in rural than urban areas. The non-response rate was higher in Finland than Sweden overall, but the distribution of non-responders was similar based on age groups and urban versus rural areas [38]. These demographic features of non-responders may have led to a slight underestimation of the overall prevalence of edentulism. Strengths of the study are the large number of participants, coverage of both urban and rural areas, and inclusion of Swedes and Finns. Thus, comparisons could be made for these demographic parameters.
In conclusion, this study shows that edentulism is more prevalent in Finland than in Sweden, and more common in rural than in urban areas. The prevalence of edentulism is likely to decrease with time, as advances in dental care and health care may increase the need for dental care among large numbers of older people who keep their teeth and remain at risk of developing periodontal disease. We found edentulism in people aged 65 years and older to be associated with low educational level, low income level, male sex, not visiting a dentist, residence in rural areas and dependence in ADLs, social isolation and experiencing poor health. These results identify important factors associated with edentulism that could be used to identify at-risk people who should be offered preventive services, and to identify factors important for intervention.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Interreg IIIA Kvarken-MittSkandia Program (2005–2007) and the Bothnia-Atlantica Program, which were both funded by the European Union, the European Regional Development Fund and the Swedish Research Council (grant number K2014-99X-22610-01-6).