
Abstract
Aim: The aim of this study was to examine whether health status (number of chronic diseases, health shock and use of tranquilizers/sleeping pills) is related to labour-market outcomes later in life. Methods: Twin data for Finnish men and women who were at least 33 years old in 1990 were linked to comprehensive register-based information on unemployment and the incidence of disability pension. We used the within-twin dimension of the data to account for shared family and genetic factors. Self-reported information on the number of diagnosed chronic diseases, health shock and drug use were obtained from the 1975 and 1981 twin surveys, when the twins were at least 18 years old. Unemployment months and the incidence of disability pension were measured during prime working age over the 1990–2004/2009 period. Results: Poor health status is significantly positively related to unemployment and the incidence of disability pension. The results are robust to controlling for shared family and genetic factors and the key measures of risky health behaviours (alcohol use, lifetime smoking and body mass index).
Introduction
The relationship between health and labour-market outcomes has been extensively studied in the literature. Early life measures such as birth weight are important determinants of outcomes in adulthood [1]. Furthermore, risky health behaviours have been linked to significantly worse labour-market success. These measures include the misuse of alcohol ([2]; see Table I for a review), smoking [3,4] and physical inactivity [5]. In addition, there are empirical studies demonstrating that chronic illnesses are negatively related to labour-force participation [6], employment and household income [7,8], as well as broader socio-economic outcomes, such as financial difficulties [9]. Studies have documented the significant economic burden of psychiatric disorders and mental distress [10,11].
Mean characteristics of the sample.
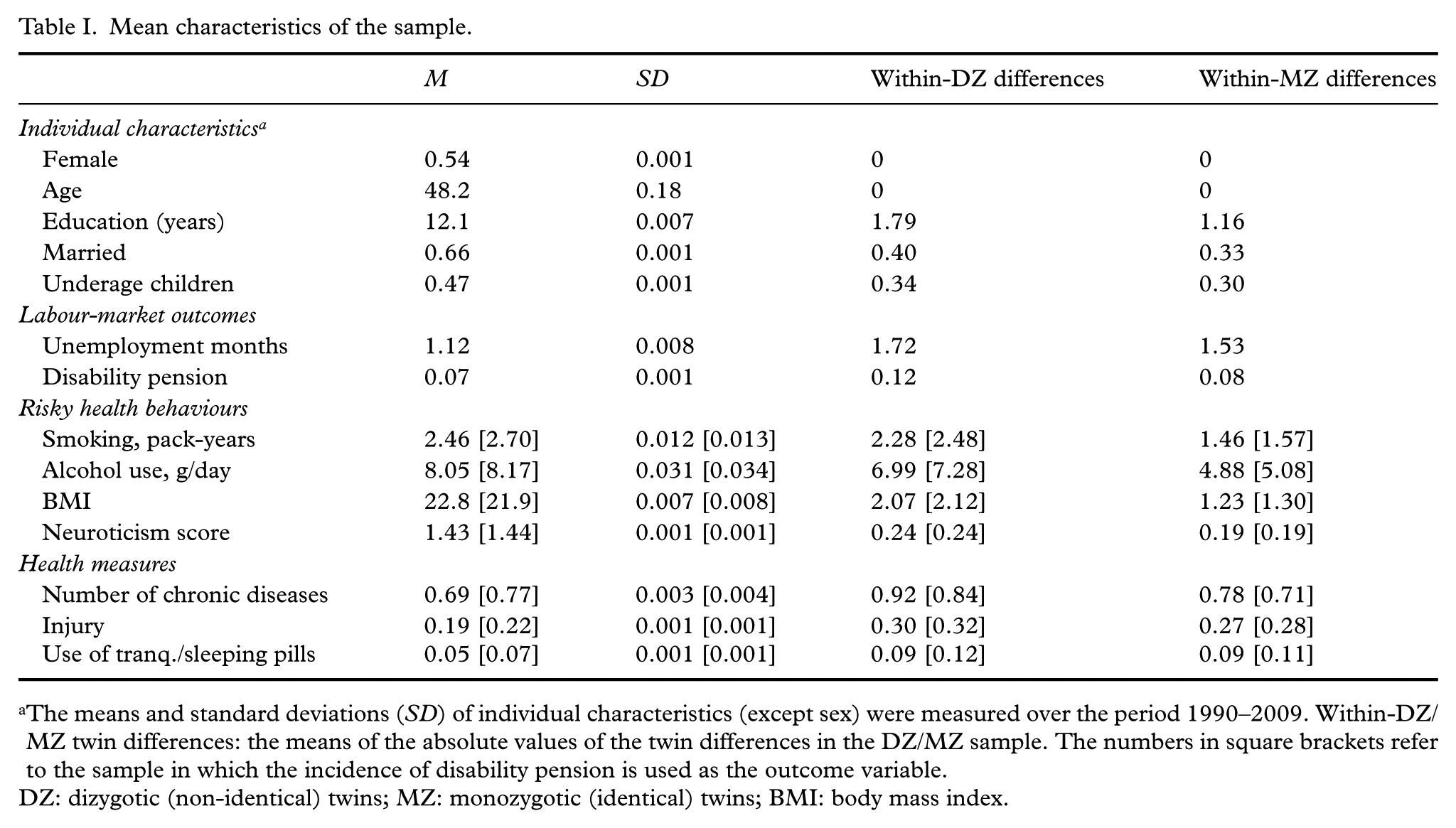
The means and standard deviations (SD) of individual characteristics (except sex) were measured over the period 1990–2009. Within-DZ/MZ twin differences: the means of the absolute values of the twin differences in the DZ/MZ sample. The numbers in square brackets refer to the sample in which the incidence of disability pension is used as the outcome variable.
DZ: dizygotic (non-identical) twins; MZ: monozygotic (identical) twins; BMI: body mass index.
There are three possible mechanisms through which worse health may lead to poor labour-market outcomes in the long run. First, health status is a determinant of a person’s productivity and stamina, which are the key ingredients of earnings capacity. Second, poor health may lead to discrimination in the labour market. Third, poor health may be related to a short-time preference that reduces investments to work-related skills. This mechanism can be interpreted two ways: either the employer is not interested in investing people who are chronically ill, or the people with poor health are unable to invest themselves.
This paper examines the relationship between chronic diseases and the use of mental-health drugs (tranquilizers/sleeping pills) and labour-market outcomes in adulthood. We use a large nationally representative twin data set. The identification of the effect of health status on labour-market prospects is not straightforward. There are unobservable confounders such as family background and peer effects that are significantly correlated with both health status and labour-market outcomes. Thus, cross-sectional estimates are likely to be biased.
We enhance the empirical knowledge on this important issue in three major ways. First, there is only scant evidence of the effects of health status on long-term labour-market outcomes in adulthood using a twin design. Using sibling data, Currie et al. [12] show that health problems in early childhood are important predictors of socio-economic status in adulthood. Bharadwaj et al. [13] take advantage of Swedish twin data to account for shared family effects. Bharadwaj et al. [13] emphasise that poor health is an important contributor to experiencing unemployment, especially during macroeconomic crises. Our research design is most closely related to a study by Lundborg et al. [14], who use twin data but labour-market outcomes from only a single year (2003). They examined the effects of health on adulthood outcomes such as earnings and found that the effects are strongest for mental-health conditions.
This paper focuses on the effects of health status on long-term labour-market prospects in adulthood. As outcomes, we use unemployment months and the incidence of disability pension. The labour force in Europe is aging rapidly. Preserving the effective labour supply at an adequate level implies the need for longer working careers. The incidence of disability pension is a relevant outcome for policy purposes because it is the most common way to retire before the official retirement age in the Finnish setting. Our outcomes are closely related because prolonged unemployment episodes may lead to disability pension, especially among the oldest cohorts. A key advantage of our approach from a policy perspective is that we examine the potential effect of chronic diseases on labour-market outcomes in a setting in which the population is ageing rapidly. Health policy provides a suitable tool to mitigate the adverse effects of chronic conditions that are closely related to health behaviours but cannot affect the exogenous sources of changes in health such as accidents. The twin data allow us to account both for unmeasured environmental factors and for genetic factors. Using information on non-identical (dizygotic [DZ]) twins is equivalent to controlling for sibling effects because DZ twins originate from the same family. DZ twins share ~50% of their genes. Using data on identical (monozygotic [MZ]) twins allows us to account further for inherited traits and characteristics. MZ twins are essentially genetically identical. The focus on non-nurture and non-nature predictors of poor labour-market outcomes provides policy-relevant information because health status net of shared family and genetic factors can be affected by policy tools.
Second, our sample consists of twin pairs for whom we observe accurate administrative information on labour-market success during the prime working age. As outcome variables of interest, we use the individual’s annual outcomes in adulthood over a 15- to 20-year follow-up period. Most of the earlier literature on health and labour-market outcomes has relied on self-reported short-term measures of labour-market outcomes.
Third, the earlier empirical literature that exploits plausibly exogenous variation in health to identify the effects on subsequent labour-market outcomes is very sparse [15,16] because it is difficult to find relevant variation in health that would otherwise be unrelated to labour-market outcomes. Our analysis, which is based on information on injuries and diseases that have caused weak employability, extends the literature in this respect. We are unaware of any earlier research using plausibly exogenous health shocks in the context of twin design.
Methods
Data
The analyses are based on the Older Finnish Twin Cohort Study of the Department of Public Health assembled at the University of Helsinki. Using personal identifiers, the twin survey has been linked to the Finnish Longitudinal Employer-Employee Data (FLEED). The initial twin candidates eligible for the study were same-sex twin pairs who were at least 18 years old in 1975 [17]. Three surveys were conducted in 1975, 1981 and 1990. FLEED is an annual panel of labour-market and broader economic outcomes for the years 1990–2009. FLEED is constructed from several administrative registers that are compiled by Statistics Finland. Previous studies have documented the representativeness of the twin data set by comparing it to a one-third random sample of all Finns using FLEED and covering the same age cohorts [18]. For example, men have completed 12.4 (12.6) years of formal education and 81% (83%) of them are married, as calculated from a sample of all Finns (twin data). The average years of completed education were 12.1 for women in both samples, and 72–73% of them were married.
Our analyses focus on twin pairs for whom we observe information regarding the number of chronic diseases, health shock, drug use and subsequent labour-market outcomes. The sample for the incidence of unemployment includes cohorts of non-retired twin pairs who were at least 33 years old in 1990. The sample size is 143,310 person-year observations. Standard errors are clustered by twin pair in all models. When the incidence of disability pension is used as the outcome variable, the sample consists of the working-age population who are 33–60 years old, including those individuals who are on a disability pension (or have the status of individual early retirement). Persons who have an old-age or unemployment pension are excluded from the sample. If an individual with a disability pension becomes entitled to an old-age or unemployment pension, his/her subsequent person-year observations are excluded from the estimation sample. The sample size is 130,606 person-year observations when the incidence of disability pension is used as the outcome variable.
Measures
Using FLEED, we focus on two key outcome variables that are designed to capture poor labour-market prospects. The first outcome variable is the number of an individual’s unemployment months at year t. The observation window for the outcome is the period 1990–2009. The second outcome variable captures an individual’s incidence of receiving a disability pension. The measure obtains the value of 1 if a 33- to 60-year-old individual was granted a disability pension at year t (or was on individual early retirement). Information on disability pension is not available in FLEED after 2004. Therefore, the outcome is measured over the period 1990–2004.
We focus on three measures of health status: the number of chronic diseases, an indicator for health shock (injury) and the use of tranquilizers/sleeping pills. Health status is measured using the twin surveys from 1981 and 1975 to avoid the so-called justification bias (i.e. reporting a worse subjective level of health to justify a person’s current labour-market status). Thus, the twins were on average 27 (33) years old at the time of the measurements in 1975 (1981).
The number of chronic diseases is measured as the self-reported sum of chronic diagnosed diseases. The twins were first asked how many chronic diseases they had in 1981. The 1981 survey included statements about the 18 most common chronic diseases, including emphysema, chronic obstructive pulmonary disease, high blood pressure, angina pectoris, peptic ulcer, diabetes and gout. Second, the twins were asked how many chronic diseases they had in 1981 other than those diseases already listed in the first question. The average number of the most common chronic diseases was approximately 0.70, according to the first question. The answers to the second question revealed that the average number of other chronic diseases was lower: approximately 0.15. The total number of chronic diseases was calculated as the number of the most common chronic diseases added to the number of other chronic diseases.
The measure for plausibly exogenous health shock is based on two questions from the twin surveys. The first question comes from the 1981 survey, indicating whether an individual has ever been disabled from work at least for three weeks due to an injury or a disease. The second question originates from the 1975 survey, revealing whether an individual has ever experienced weak employability caused by an accident. Thus, our measure for health shock obtains the value of 1 if either one event or both events has occurred.
Finally, we use a proxy for (poor) mental health by taking advantage of self-reported information on medication use in 1981. The use of tranquilizers and/or sleeping pills captures one aspect of mental health. The twins were asked how many days in total during the past year they had used tranquilizers or sleeping pills (or both). The alternatives were measured on a five-point scale (no use, <10 days, 10–59 days, 60–180 days, >180 days). The use of tranquilizers/sleeping pills was divided into three mutually exclusive categories based on previous medical literature: no use of medication; infrequent use (1–59 days) of either medication; and frequent use (≥60 days) of either medication (cf. [19]). Infrequent and frequent use of these medications arguably captures different aspects of mental stress. Exogenous negative life shocks and the incidence of environmental stress, such as divorce, widowhood or experiencing a layoff, may promote the use of psychoactive medications. However, the use of these medications is often only temporary and does not indicate the onset of serious mental-health problems for which the frequent use of medications is more common. The share of twins who have used either medication frequently is quite low (~1–2%) in the data. Thus, the sample size limits the opportunities to estimate the relationship between a categorical measure of medication and the outcomes using the within-MZ twin sample. Therefore, we constructed an indicator for poor mental health that obtains simply the value of 1 if an individual had used either medication. In robustness checks, we also consider an alternative proxy for mental health that obtains the value of 1 if an individual had used either medication infrequently.
Using register-based information from FLEED, the baseline models include demographic controls. These are age, sex, education years, marital status, the presence of underage children and the full set of year dummies. Age, sex and the year effects are automatically eliminated in within-twin models because there is no within-twin variation in these controls. We further assess the robustness of the baseline estimation results by accounting for risky health behaviours and a measure of mental stability. The controls obtained from the twin survey include measures for smoking, alcohol consumption, body mass index (BMI) and neuroticism. Smoking is measured as pack-years [4] and captures the lifetime consumption of cigarettes. Alcohol consumption is measured as consumption of pure alcohol by grams per day [2]. Neuroticism is assessed using 10 items in the short form of the Eysenck Personality Inventory. The controls originate from the 1975 survey and are used to account for pre-existing risk factors for chronic diseases and mental distress. These controls have also been found to be significantly related to labour-market outcomes in the prior empirical literature.
Descriptive statistics
Table I presents descriptive statistics for the sample of all individuals in our twin data. The demographic characteristics reveal that 66% are married and 47% have underage children. The average age is 48 years, and on average, the twins have completed 12 years of formal education. The average number of unemployment months per year is 1.12, and approximately 7% of the twins, measured using person-year observations, have received a disability pension.
The twins are of normal weight (mean BMI=22.8 kg/m2), consume on average 8 g of alcohol per day (i.e. approximately one unit of alcohol) and have smoked on average one pack of cigarettes daily for ~2.5 years. The average number of chronic diseases is ~0.7–0.8. Less than one-half (45%) of the twins report at least one diagnosed chronic disease (not reported in Table I). Approximately 20% of the twins report a health shock caused by an accident, injury or disease. Finally, the use of tranquilizers/sleeping pills is not common (~6%).
The means of the absolute values of twin differences show that compared to the DZ twins, the MZ twins are much more similar to each other with respect to labour-market outcomes, basic demographic characteristics and the number of chronic diseases. Important exceptions are the measure of health shock and the use of tranquilizers/sleeping pills, for which we find largely similar differences among the DZ and MZ twins. We further estimated a regression model to check the contributions of heritability and shared environment in the variation in each health measure using the standard DF method [20]. These results showed that the heritability component is statistically significant in explaining the variation in the number of chronic diseases but not in explaining the health shock (not reported in tables). The genetic component also marginally explains the variation in the use of medications, but not when we use solely infrequent use of tranquilizers/sleeping pills as the outcome variable. These results suggest that our measure for the health shock is likely independent of an individual’s own control. For comparison, Pedersen [21] finds that the variation in tranquilizer use is to some extent attributable to genetic factors but reports no evidence of heritable influences for the use of sleeping pills. Overall, there is sufficient within-twin pair variation in the data among the MZ twins, which is crucial for model identification.
Table II presents descriptive statistics on individual characteristics during the measurement in 1981. The means are calculated separately for those who have/do not have chronic diseases in 1981. Annual earnings in 1980 originate from the Longitudinal Population Census of Statistics Finland. Those who had reported at least one chronic disease in 1981 were two years older (32 vs. 34 years) and more likely married (63% vs. 67%) and less likely living together with their twin sibling (8% vs. 5%) compared to those who had no reported chronic diseases. Importantly, individuals were similar in their labour-market status (employment or unemployment) and skill level (education years and earnings level) during the measurements in 1981, regardless of their health status. We also calculated simple correlations between within-MZ differences in the number of chronic diseases and individual characteristics, and none of these correlations were statistically significant (not reported in tables). This means that the within-MZ variation in health status at the time of measurement is unlikely explained by the sibling differences in initial labour-market success.
Mean characteristics in 1981 by health status (number of chronic diseases).

Statistical methods
To address the research questions, we use four approaches in our empirical modelling [2]. First, we estimate an ordinary least squares (OLS) regression to quantify the relationships between the health measures and labour-market prospects for a combined sample of DZ and MZ twins, and we treat the data as if it were based on individuals.

where
Second, we take twin differences for the variables and estimate the same regression using the combined DZ–MZ sample. Third, we estimate the within-twin pair regression using the DZ sample. The estimator is consistent if
Results
Descriptive evidence
Table III reports the average number of unemployment months and the average share of people who have received a disability pension, conditional on diagnosed chronic diseases (panel A), health shock (panel B) and the use of tranquilizers/sleeping pills (panel C). Individuals who have reported at least one chronic disease in 1981 have more unemployment months, and they are more likely to receive a disability pension or retire early than those who did not report any chronic diseases in 1981. These differences in labour-market outcomes become even more pronounced when the health shock (injury) or consumption of tranquilizers/sleeping pills is used as the measure for poor health. The t-test of the null hypothesis of equal group means is rejected for all measures of labour-market outcomes.
Health status and long-term labour-market outcomes.
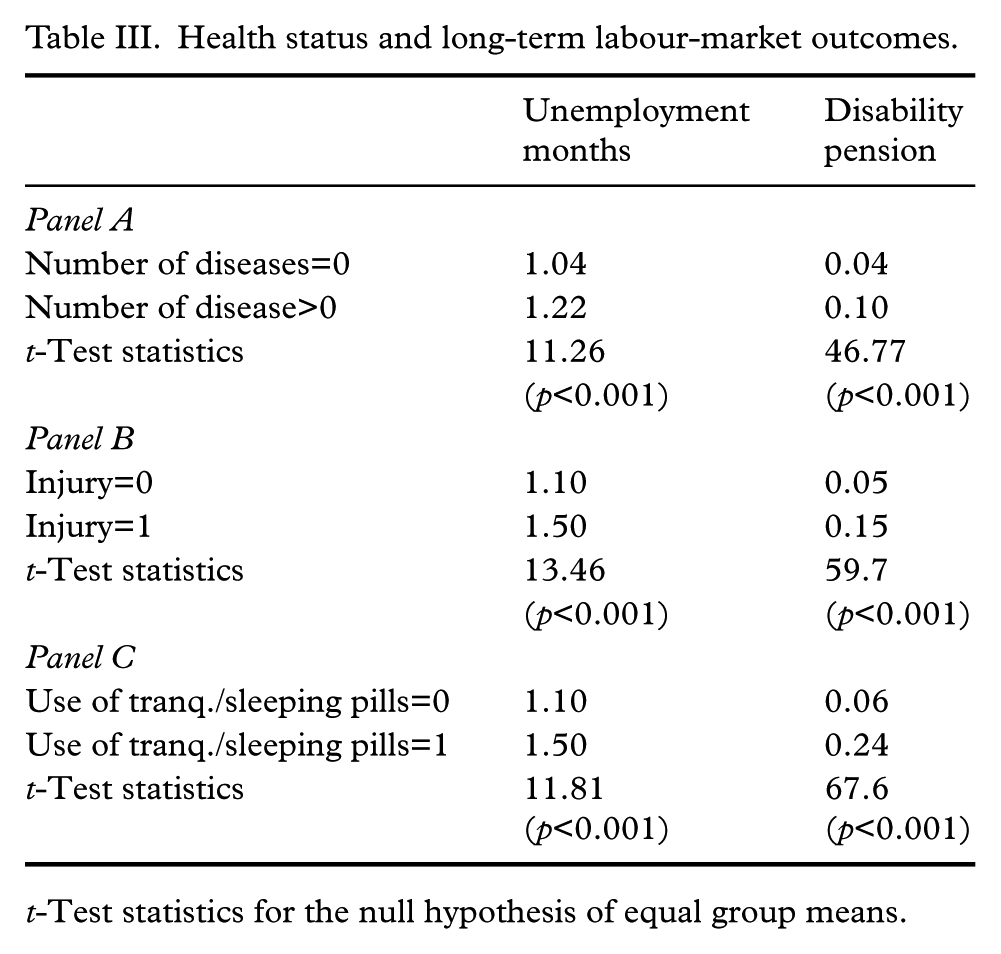
t-Test statistics for the null hypothesis of equal group means.
Figure 1 illustrates the evolution of unemployment months by health shock status over the period 1990–2009. The year 1990 was the peak of the economic upswing, with exceptionally low aggregate unemployment. In 1991–1994, Finland experienced a severe economic crisis, when the GDP dropped sharply and unemployment increased to a historically high level. After 1995, the economy recovered and developed favorably until the global financial crisis hit in 2008. As shown in Figure 1, unemployment is generally notably higher for those who have reported a negative health shock in the past (1975/1981). Importantly, in 1990, the number of unemployment months was at the same level as those who had not reported a health shock, supporting the assumption about the exogeneity of the health measure. The difference in unemployment became detectable during the recession, and the gap persisted even when the economy recovered from the depression of the early 1990s.
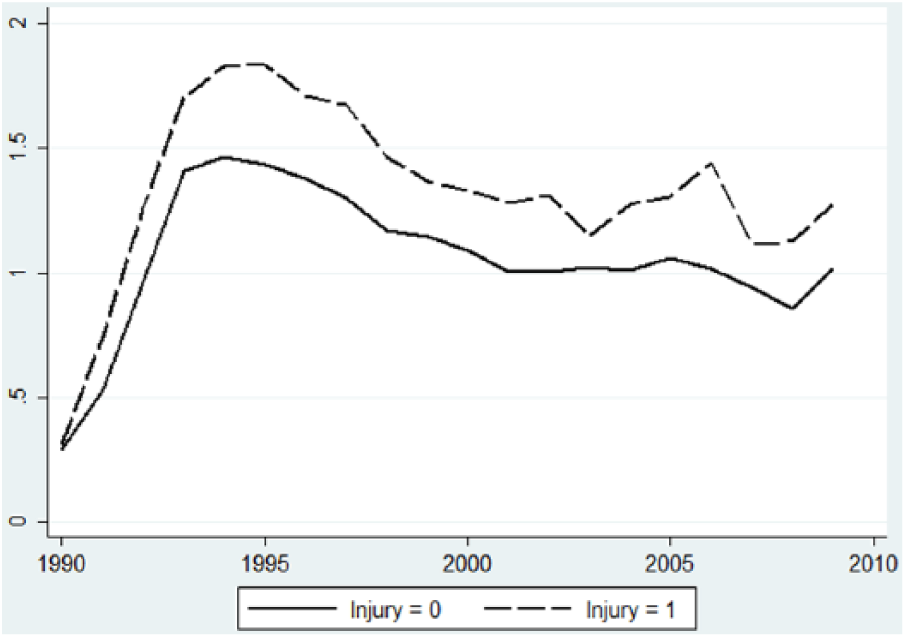
Mean unemployment months per year by health shock status over the period of 1990–2009.
Main estimation results
The estimates for the number of chronic diseases and the indicators for health shock (injury) and the use of tranquilizers/sleeping pills on the labour-market outcomes are reported in Table IV. The cross-sectional OLS results show that poor health is statistically significantly correlated with weaker labour-market prospects later in life. The pattern is similar for the number of chronic diseases, the health shock and the use of tranquilizer/sleeping pills as the measures of health. For example, those persons who have experienced a health shock work approximately 0.15 months less than those who have not reported a health shock. This effect corresponds to three unemployment months over the 20-year follow-up period (0.15 months×20=3 months). Importantly, the effect of health shock is economically more significant when we use the incidence of disability pension as the outcome variable (β=0.078). We interpret this result in two ways. In Table II, we document that the average probability of a disability pension was 7%. Thus, the estimate can be interpreted as a ~100% increase in the incidence of a disability pension for those who had a health shock. This further corresponds to 1.2 years more of disability pension over the follow-up period (0.078 years×15=1.2 years).
OLS and within-twin estimates of health status on unemployment and disability pension: bivariate regressions.
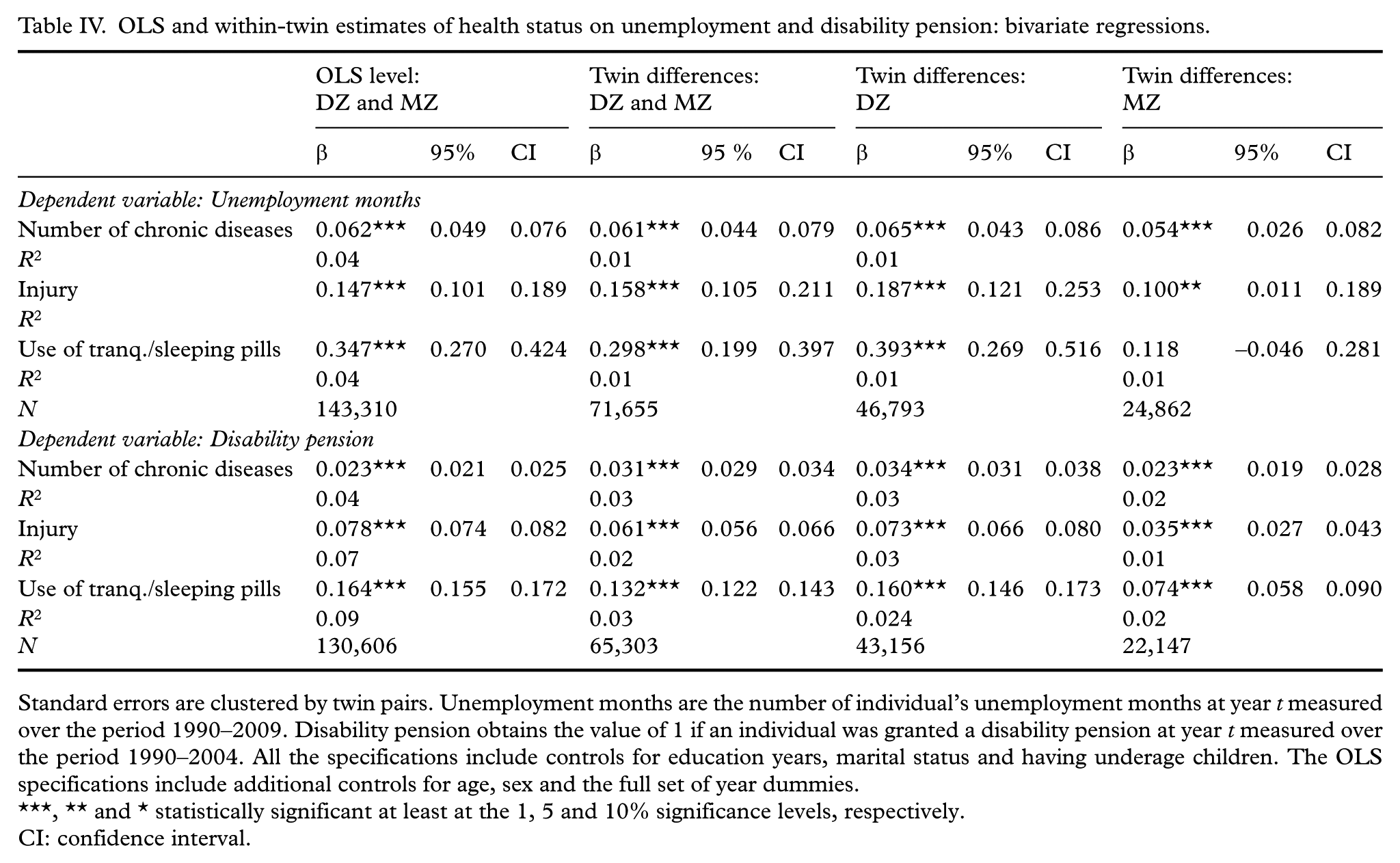
Standard errors are clustered by twin pairs. Unemployment months are the number of individual’s unemployment months at year t measured over the period 1990–2009. Disability pension obtains the value of 1 if an individual was granted a disability pension at year t measured over the period 1990–2004. All the specifications include controls for education years, marital status and having underage children. The OLS specifications include additional controls for age, sex and the full set of year dummies.
** and * statistically significant at least at the 1, 5 and 10% significance levels, respectively.
CI: confidence interval.
The estimates for drug use reveal that the individuals who consume tranquilizers/sleeping pills work approximately four months less over the 20-year period than those who do not use either of these medications. Again, the economic significance of the associations is more pronounced when we use the incidence of disability pension as the outcome variable. The use of tranquilizers/sleeping pills is associated with 2.5 more years of disability pension compared to those who do not use either of these medications.
The estimates remain statistically significant in smaller DZ–MZ and DZ specifications in which shared family factors are accounted for. The preferred within-MZ estimates fully account for both shared family and genetic factors (column 4). These coefficients are more imprecisely estimated but nevertheless remain statistically significant. The only estimate that is no longer statistically significant is the use of tranquilizers/sleeping pills when unemployment months is applied as the outcome variable.
The preferred within-MZ estimates show that the effect of poor health status on the labour-market outcomes is economically more significant at the exit margin of adjustment. Over a long period, one chronic disease is associated with an increase in unemployment of one month. For disability, the magnitude is four months. A plausibly exogenous health shock is associated with an increase in unemployment of approximately two months but an increase in disability from work of six months. Furthermore, the proxy for poor mental health is statistically significant in explaining disability retirement but not unemployment.
The within-DZ estimates tend to be larger compared to the within-MZ estimates. This suggests that there are unobserved genetic factors positively correlated with poor health status in our twin setting, which may lead to upwardly biased estimates when only shared family background is controlled for. For example, risk-prone behaviour may be positively correlated with the exposure of chronic diseases, while anxiety is arguably positively correlated with the use of tranquilizers. Because risk preferences and anxiety are at least partially genetically inherited [23], they are more completely accounted for in the MZ sample than in the DZ sample. The exposure to exogenous health shocks is not genetically inherited, but not everyone copes with these negative events in the same way. Some people recover more quickly from stress and have better ability to function at work. Therefore, the smaller estimated coefficient of health shock in the MZ sample could be explained by the differences in human resilience to stress and adversity, which are partly genetically inherited [24].
Extensions
To explore the robustness of the baseline estimates, we have estimated several additional specifications. First, we estimated the preferred within-MZ model separately for men and women to examine the potential heterogeneity of the associations. However, the use of tranquilizer/sleeping pills is relatively uncommon in the data. Thus, the sample size (evaluated by the number of persons, not by using annual outcomes) is insufficient, and there is not enough variation in the MZ cells for men and women separately. For this reason, in Table V, we present the results by sex using only the number of chronic diseases and health shock. The baseline results remained intact when we used the incidence of disability pension as the outcome variable. Thus, having chronic diseases or experiencing a health shock is positively correlated with the incidence of disability for both sexes. The number of chronic diseases is also positively related to unemployment months for both sexes. However, the effect of health shock on unemployment months prevails only for women. Because men are usually the main breadwinners in Finnish families, they may be more likely to avoid unemployment, even after experiencing negative health shocks.
Within-MZ twin estimates of poor health status on unemployment and disability pension by sex.
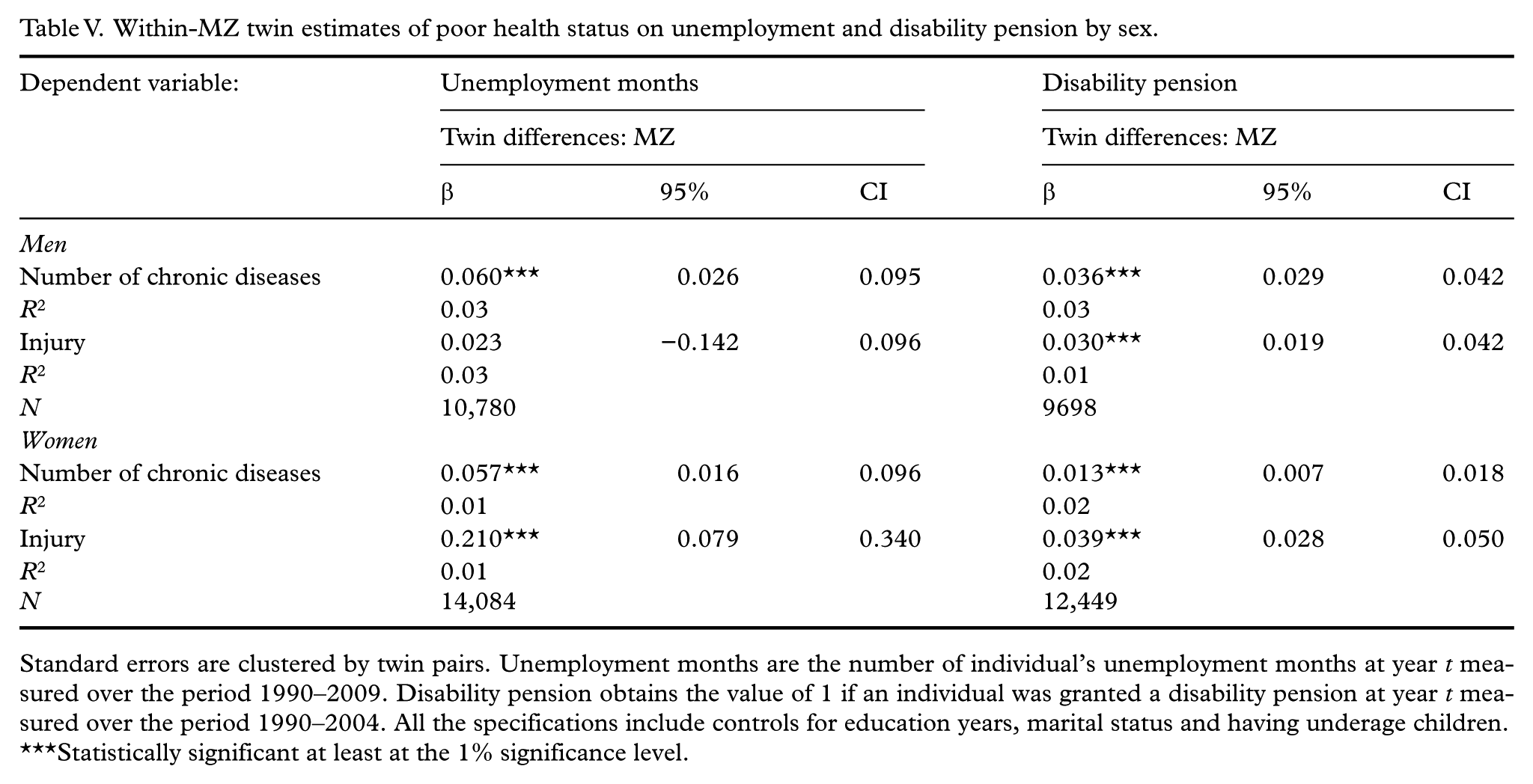
Standard errors are clustered by twin pairs. Unemployment months are the number of individual’s unemployment months at year t measured over the period 1990–2009. Disability pension obtains the value of 1 if an individual was granted a disability pension at year t measured over the period 1990–2004. All the specifications include controls for education years, marital status and having underage children.
Statistically significant at least at the 1% significance level.
Second, we included the measures of risky health behaviours (i.e. alcohol use, smoking and BMI) and the neuroticism score measured in 1975 as additional controls in the MZ-differenced model. The estimates show that education, marital status, alcohol use and neuroticism are important predictors of the incidence of disability pension and unemployment (Table VI). These results accord well with previous research [3,25]. Importantly, the earlier findings reported in Table IV for chronic diseases, health shock and the use of tranquilizers/sleeping pills remained intact. Using the number of chronic diseases, the estimate obtains the value of 0.044 (0.022) in the model in which we use unemployment months (disability retirement) as the outcome variable. For brevity, we present the estimates of the full models only for the specifications in which we use an exogenous health shock as the measure for poor health status. Interestingly, the relative importance of the health shock as a predictor of unemployment months is comparable to education years (Table VI). Accordingly, the negative effect of an exogenous health shock on the incidence of a disability retirement is equivalent to a ‘loss’ of three education years, which corresponds to a vocational or polytechnic degree in length. To illustrate a rough monetary (shadow) value of the exogenous health shock, we use a simple back-of-the-envelope calculation and the fact that the estimated return to one additional year of education in terms of earnings in Finland is about 10% [26]. Using the average level of earnings in the twin data (approximately €25,660 in 2009) our estimate implies that the monerary value of exogenous health shock is approximately €7700 per year.
Within-MZ twin estimates of health shock (injury) on unemployment and disability pension with additional controls.
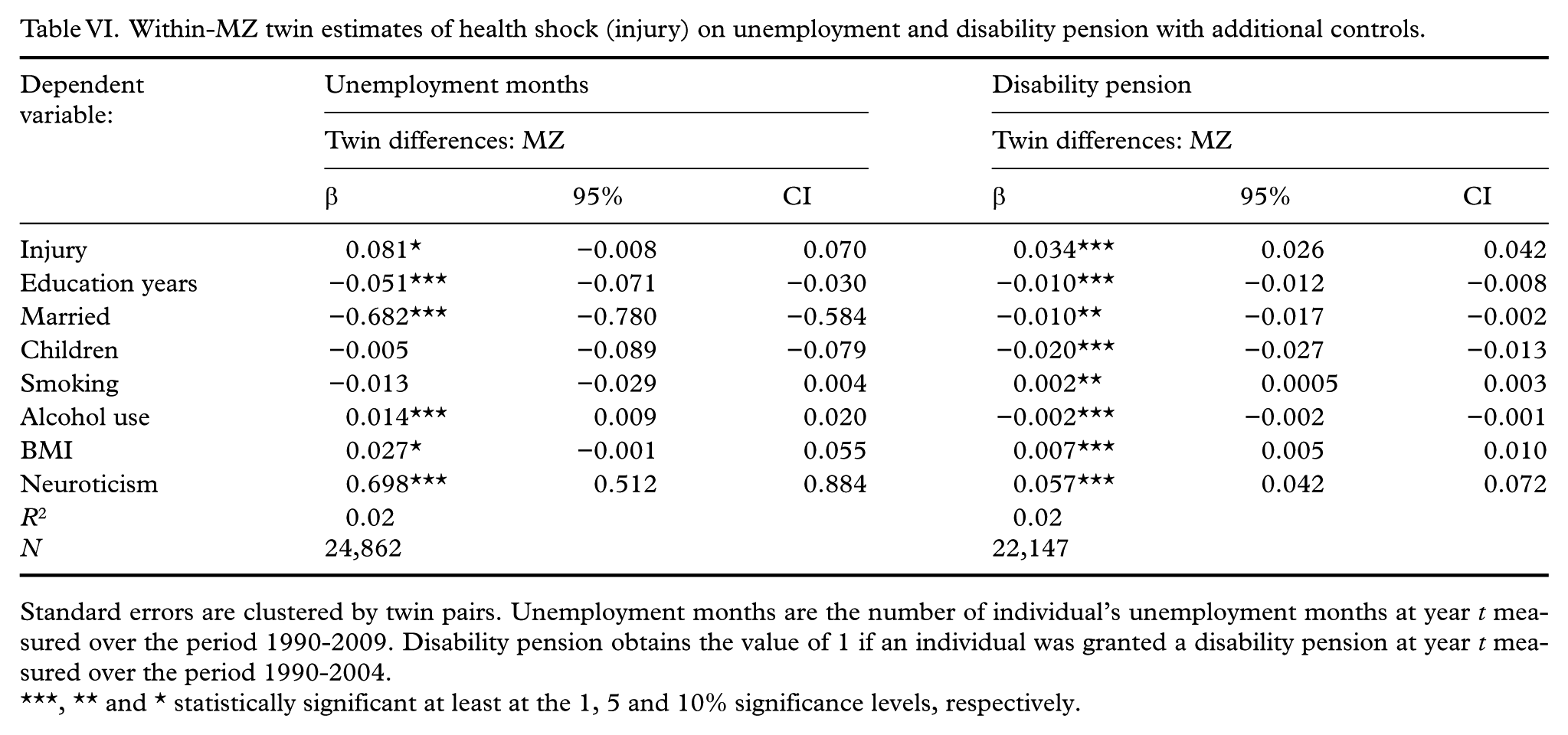
Standard errors are clustered by twin pairs. Unemployment months are the number of individual’s unemployment months at year t measured over the period 1990-2009. Disability pension obtains the value of 1 if an individual was granted a disability pension at year t measured over the period 1990-2004.
** and * statistically significant at least at the 1, 5 and 10% significance levels, respectively.
Third, we used alternative measures for poor health status as the independent variable. Because the effect of the number of chronic diseases is likely to be non-linear, we constructed an indicator for poor mental health that obtains the value of 1 if an individual had at least one chronic disease. The estimate for the preferred within-MZ model was 0.131 when we used unemployment months as the outcome variable (not reported in tables). This shows that individuals who had at least one chronic disease work approximately 2.6 months less in the long run (0.131 years×20) compared to those who have no chronic diseases. The estimate for an indicator of chronic diseases was 0.032 when we used an incidence of a disability retirement as the outcome variable. This corresponds to 0.5 years (6 months) more of disability pension over a 15-year period. Interestingly, this effect is equivalent to that of a plausibly exogenous health shock (cf. Table IV, column 4). We also constructed an indicator for poor mental health that obtained the value of 1 if an individual had used tranquilizers/sleeping pills infrequently. This measure captures the incidence of temporary stress and does not necessarily indicate the onset of serious mental-health problems. The estimate in our preferred within-MZ model was statistically insignificant when we used unemployment months or an incidence of a disability pension as the outcome variables (not reported in tables). Thus, the positive relationship found in Table III (column 4) is driven by the frequent use of tranquilizers/sleeping pills.
Measurement error
A potential problem with twin design is that it may exacerbate the measurement error problem compared to the baseline cross-sectional estimation at the individual level. Classical measurement error in an independent variable could result in conservative estimates [27]. Thus, the attenuation bias caused by random measurement error in our health measures would bias the estimates towards zero. For this reason, we have also estimated within-twin models in which we use the difference in chronic conditions in 1975 as an instrument for the difference in chronic conditions in 1981. Instrumental variable (IV) estimation alleviates the measurement error bias if the measurement error is classical. The IV estimation does not mitigate potential omitted-variable bias unless the omitted variable is correlated only with the 1981 measure. The IV model is estimated using the standard two-stage least squares. Consistent with attenuation bias, we find that the IV point estimates using the within-MZ sample are significantly larger than the baseline point estimates (0.023 vs. 0.051 for a disability retirement and 0.054 vs. 0.283 for the unemployment months). The first-stage estimates also exceed the standard threshold of 10 (F-test is 2087.7 for a disability pension and 977.8 for unemployment months). These results should nevertheless be treated with some caution. First, people may have reported more chronic health conditions in 1981 than in 1975 because they are simply older. Second, the 1981 survey included statements about the 18 most common chronic diseases, while the 1975 survey included statements about 16 diseases.
The measurement error in health status may also be mean reverting. This could cause the self-reported health status to be biased towards the mean. For example, those who have several chronic diseases may underreport, while those who do not have any chronic diseases may over-report. This implies that the measured twin-difference in the number of chronic diseases would be smaller than the true difference, which may also lead to estimates that are closer to zero.
Discussion
There is a well-established two-way relationship between health and labour-market prospects [28,29]. Chronic conditions are potentially important but are relatively neglected determinants of outcomes in the labour market. Taking a life course perspective is important for appropriate analyses of these relationships because the negative effects accumulate over time. We used nationally representative twin data linked to register-based administrative information on individuals’ unemployment and the incidence of disability pension to examine the relationship between health status and the measures of poor labour-market outcomes in the long term.
Extending previous empirical research, we established three important links. First, chronic diseases and the use of tranquilizers/sleeping pills are significantly positively associated with unemployment in adulthood. These results remained intact after accounting for shared family and genetic factors. Second, we found that poor health status is a strong predictor of disability pension. Third, we used plausibly exogenous variation in health based on injuries and diseases that have caused more than three weeks’ disability from work. Our basic findings remained intact, suggesting that there is most likely a causal link between health status and labour-market prospects.
The current results support policies that promote health to improve labour-market outcomes in the long run. Preventive measures are particularly important in this respect. Improved health delivers high social returns in terms of lower unemployment and fewer incidences of disability pension. The results should be considered in the comprehensive evaluations of benefits and costs of investments that improve access to health care. Because unemployment leads to multiple socio-economic problems, such as deprivation, promoting health entrenches the social fabric more broadly. Early labour-market exit and disability pension also constitute a substantial burden to public finances.
There are issues related to our data and research design that are relevant for the interpretation of the results. First, attrition is a potential worry in all follow-up studies. Significant attrition that would be concentrated to those who have the poorest health may lead to conservative estimates. However, the response rate to the 1981 twin survey was 84%, and prior analyses of the twin data have not reported significant attrition [30]. Second, classical measurement error in an independent variable would result in conservative (OLS) estimates, as discussed earlier. Third, our data originate from Finland, where specific chronic conditions related to cardiovascular diseases are more important than elsewhere. Relationships between health status and long-term labour-market success may therefore be country specific. Importantly, the estimated effects are economically significant, despite the fact that the Nordic welfare states, including Finland, provide extensive programmes and universal access to health care to mitigate the negative effects of health status on long-term labour-market outcomes. Therefore, our estimates likely constitute the lower bound for the size of the effects that prevail in other countries.
Our linked data have key strengths. First, our analyses were based on a 20-year follow-up period and a relatively large sample size. Second, the outcome variables originated from register-based data containing a minimum amount of measurement error. The earlier literature has typically used self-reported information on labour-market outcomes that is prone to systematic measurement error. Third, we used a twin design that allowed us to account for shared family and genetic factors. The use of twin data constitutes a promising approach to examine the increasingly policy-relevant topics that examine the links among health status, risky health behaviours and labour-market outcomes.
Our study also has some important limitations. First, the analysis of twin data does not exclude non-causal explanations for the association between health status and labour-market outcomes in adulthood. A confounding factor such as a serious negative life event may influence health status in 1981, and this unmeasured characteristic may also be related to labour-market prospects over the follow-up period. Second, the analyses were based on self-reported information on the use of tranquilizers/sleeping pills that is prone to measurement error. Future studies would benefit from using administrative prescription data.
Footnotes
Acknowledgements
We would like to thank Jaakko Kaprio for access to the twin data. We are grateful to the editor (Lauri Sääksvuori) and three anonymous reviewers for helpful comments. All the data analyses for this paper were carried out at Statistics Finland, following its terms and conditions of confidentiality.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
The research has been financially supported by the Jenny and Antti Wihuri Foundation, Palkansaajasäätiö and the Academy of Finland Strategic Research Council project Work, Inequality and Public Policy (number 293120).