
Abstract
Aim: The aim of this study was to examine the reported frequency of breakfast intake and selected food and beverages in the investigated group of Swedish children in comparison with recommended intakes. Furthermore, the study analyses these food habits and some demographic and lifestyle factors in relation to overweight and obesity. Methods: This cross-sectional study builds on data collected in 2008 and 2010. Measured anthropometric data and parent questionnaire data were collected. A total of 2620 Swedish children (52.1% boys) aged seven to nine years were included. Results: The majority of parents reported that their children (95.4%) had breakfast every day. The majority of children had fresh fruit (84.7%) and vegetables (83.9%) most days a week. Only 1.6% of the children were reported to have fast food and 6.0% to have sugar containing soft drinks, four days a week or more. The prevalence of overweight including obesity (OW/OB) was 17.8% for boys, 18.6% for girls. The odds of being OW/OB was higher among those not having breakfast every day (odds ratio (OR) 1.9, 95% confidence interval (CI) 1.20–2.96), drinking diet soft drink (OR 2.6, 95% CI 1.52–4.42) and skimmed/semi-skimmed milk (OR 1.8, 95% CI 1.37–2.36) four days a week or more. Parents being overweight and having low education levels were also related to a higher risk of their children being overweight.
Introduction
The development of child overweight including obesity (OW/OB) is complex and several factors interplay, such as child birth weight and if the child was breastfed [1], physical activity level [2], parental body mass index (BMI), education [2,3] and area of residence [4]. Dietary habits certainly also play a role in the development of child OW/OB [3,5], and studies have shown a positive relationship between breakfast skipping and OW/OB [6].
The breakfast habits of children/adolescents have been described as being of importance for OW/OB status, and having breakfast is recommended in the Nordic countries [5,7]. In 2010, 72% and 66% 11-, 13- and 15-year-old Swedish boys and girls, respectively, reported a daily breakfast intake [8]. However, children, and in particular adolescents, are more likely to skip breakfast than any other meal [6]. Regular breakfast consumption has been associated with positive health benefits [9]. Children who regularly have breakfast have in other studies been shown to be more likely to have a better diet quality and a higher intake of key food groups, such as fruit, dairy and dietary fibre. Furthermore, they are also more likely to meet the recommendations for micronutrients [10].
Children who skip breakfast tend to eat more energy-dense food such as fast food and consume a higher percentage of energy at subsequent meals. When children are skipping breakfast, it can lead to excess hunger, overeating and consequently eating larger portion sizes [9].
Fruit and vegetables (f&v) are an essential part of a healthy diet. A study from 10 European countries showed that Swedish 11-year-olds had the highest f&v intake (291 g/day) after Norway and Bulgaria [11]. Consumption of food such as processed food, French fries, sweets and sugar-containing soft drinks is considered unhealthy [7,12]. Studies have shown that consumption of these food items contributes to OW/OB among children [3,5,12]. A decreasing trend was observed for sweets and soft drink consumption for Swedish adolescents from 2001 to 2010 [13]. Even if milk is an important component of a child’s diet, there are few studies that explore the association between milk consumption and body mass among children [14].
World Health Organization Childhood Obesity Surveillance Initiative (WHO COSI) study
On the recommendation from the World Health Organization (WHO) [15], the World Health Organization Childhood Obesity Surveillance Initiative (WHO COSI) was developed in order to monitor the development of childhood OW/OB in Europe. In 2007/2008, the first data collection was launched and 13 European countries including Sweden participated, using a common standardized protocol for measurement as well as equipment [16].
Aims of this paper
The first aim of this paper was to explore parental reports of frequency of breakfast intake and selected food items in relation to current recommendations among a group of seven- to nine-year-old Swedish children. The second aim was to analyse these reported food habits, parental demographic and lifestyle factors in relation to the children’s overweight and obesity status.
Material and methods
Study population
The selection of schools and data collection procedure have been described previously [2,4]. The measured children were given a lifestyle questionnaire to be filled out by their parents or guardians. The recruitment process is described in Figure 1.
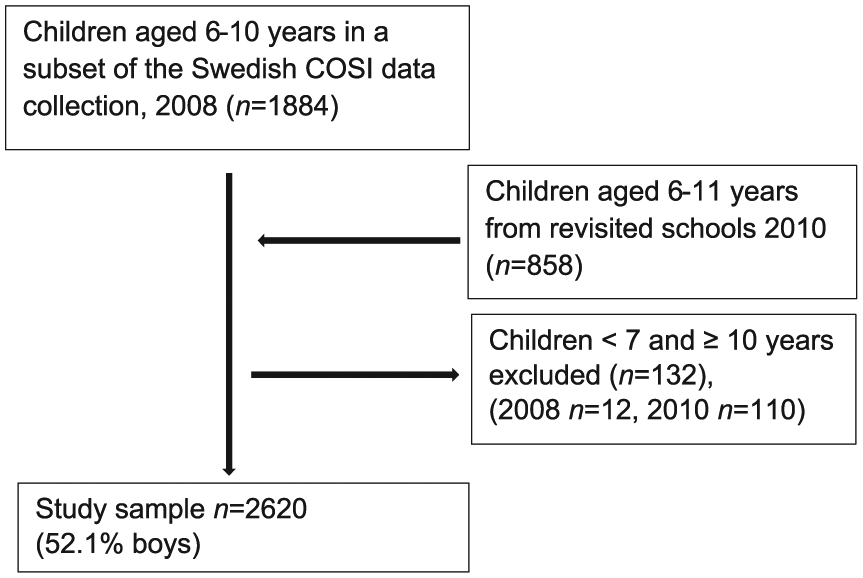
Overview of the inclusion and exclusion process in the subset of Swedish WHO COSI study 2008 and 2010 of seven- to nine-year-old children from the northern and eastern part of Sweden.
Lifestyle questionnaires
The lifestyle questionnaire contained information related to breakfast habits, as well as food and beverage intake. The question relating to breakfast habits was formulated as follows: over a typical week, how often does your child have breakfast? The food and beverage questionnaire contained 17 items, and the question was: how often does your child eat or drink the following kinds of foods or beverages? The options for breakfast, food items and beverages were ‘every day’, ‘most days (4–6 days)’, ‘some days (1–3 days)’ and ‘never’. For breakfast habits, the response was dichotomized to ‘every day’ and ‘less than seven days a week’. For the food items and beverages, the responses were dichotomized into less than four days a week and four or more days a week.
Anthropometric measurements
The height and weight of the children were measured by trained staff using the WHO COSI protocol [17]. Age and gender-specific BMI cut-off points for thinness (defined as BMI ≤ –1 standard deviation (SD)), normal weight (defined as > –1 SD < +1 SD), overweight (defined as ≥ +1 SD < +2 SD) and obesity (defined as ≥ +2 SD) are according to the Swedish national growth reference from Werner [18]. To facilitate the identification of factors of importance for OW/OB, children with different degrees of thinness, defined as BMI ≤ –1 SD according to the growth reference from Werner [18] (n = 425 cases) were excluded from the chi-square test and the regression analyses, leaving a total sample of n = 2195 children, 1129 boys (51.4%). Overweight and obesity were merged into OW/OB.
Demographic and lifestyle factors
The place of residence was categorized as ‘urban/semi-urban’ or ‘rural’ [17]. For both parents, the self-reported BMI were calculated and weight status was determined according to the international cut-off for adults, BMI ≥ 25 kg/m2 for overweight and BMI ≥ 30 kg/m2 for obesity [19], and dichotomized into ‘both parents normal weight’ and ‘one or both parents overweight (including obesity)’. The education level of parents was dichotomized into ‘at least one parent educated at university level’ or ‘both parents below university level’.
Statistical analysis
Body size characteristics of the children were described using the means (SD) of all anthropometric variables. The chi-square test was performed to identify significant independent variables followed by the binary logistic regression models to establish associations between all independent variables and the outcome variable (OW/OB). Odds ratios (ORs) with 95% confidence intervals (CIs) were computed to estimate the association between variables. All p-values reported were based on two-tailed comparisons and the level of significance set at 0.05. All statistical analyses were performed using Statistical Package of Social Sciences (SPSS), Version 23.0 (SPSS Inc., Chicago, IL, USA).
Ethical considerations
The regional Ethics Committee in Stockholm reviewed and approved this project (number 2008/5:4 and protocol 2010/5:5). For the 2008 data collection, a passive consent was used for parents. For the 2010 data collection, an active informed written consent was requested from the parents. Before both data collections, oral consent was obtained from the child.
Results
Breakfast frequency and food and beverage consumption
As shown in Table I, a majority of the children were having breakfast every day (95.4%).
Consumption frequency of breakfast, food and beverages for Swedish seven- to nine-year-old children during a regular week.
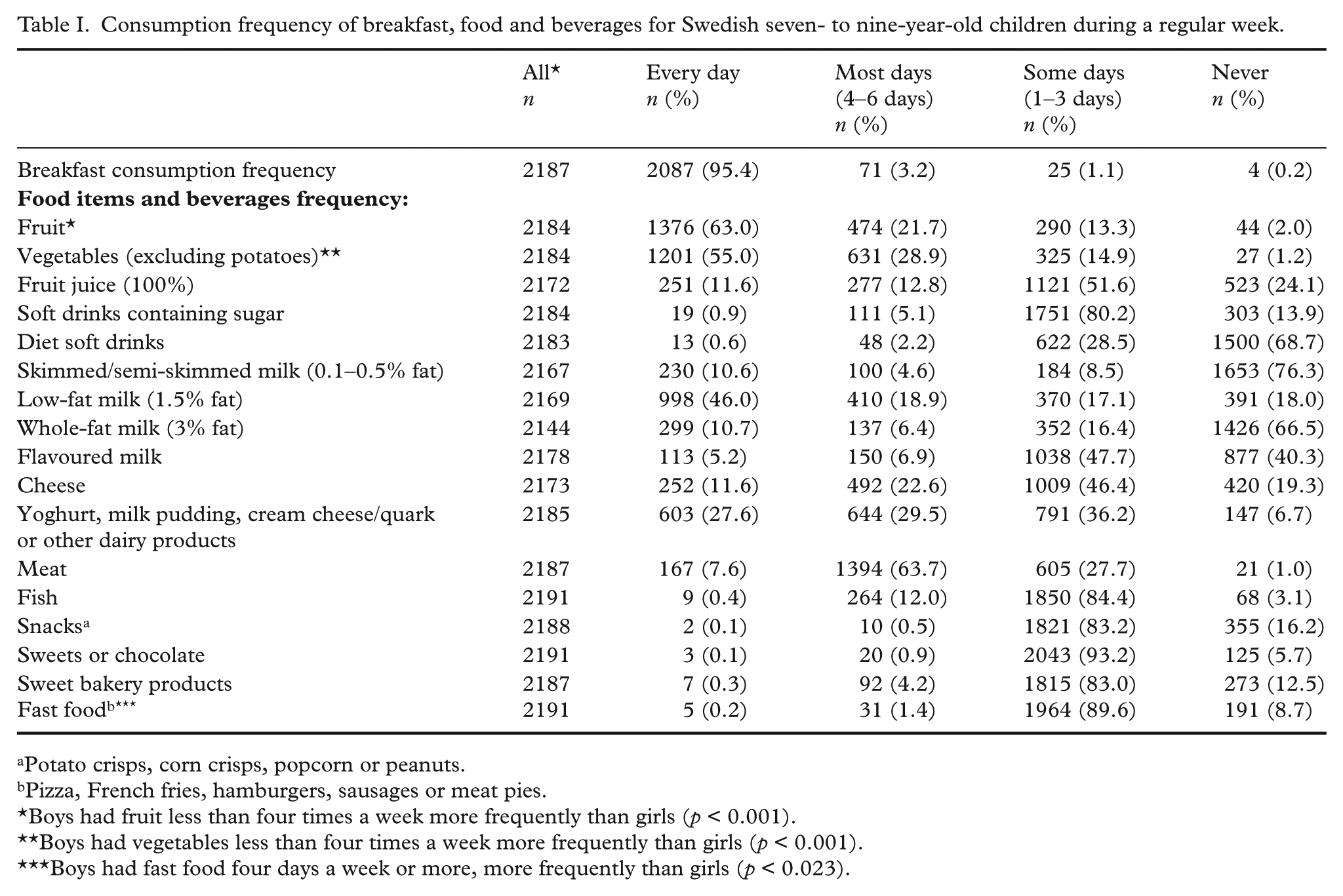
Potato crisps, corn crisps, popcorn or peanuts.
Pizza, French fries, hamburgers, sausages or meat pies.
Boys had fruit less than four times a week more frequently than girls (p < 0.001).
Boys had vegetables less than four times a week more frequently than girls (p < 0.001).
Boys had fast food four days a week or more, more frequently than girls (p < 0.023).
Fruit was reported to be eaten by 84.7% of the children, and vegetables, by 83.9% four days or more per week. For both f&v, we found a significant (p < 0.001) gender difference, whereas boys more commonly were reported as having f&v less than four days a week (data not shown).
The vast majority of the children (≥ 95.5%) had snacks, sweets or chocolate, sweet bakery products and fast food (pizza, French fries, hamburgers, sausages or meat pies) less than four days a week (Table I). We also found a significant gender difference (p = 0.023) for fast food; the boys were reporting having fast food items four days a week or more frequently than the girls (data not shown).
For beverages, the majority of children were reported having soft drinks containing sugar (94.0%), diet soft drinks (97.2%) and fruit juice (75.7%) less than four days a week. For skimmed/semi-skimmed milk and whole-fat milk, 84.8% and 82.9%, respectively, of the children were reported to consume these types of milk less than four days a week (Table I).
Children’s characteristics
Table II shows the mean and SD for age, weight, height and BMI for three different age groups and by gender. We found no significant gender difference in height, weight and BMI, except for the eight-year-old boys that were significantly taller (p < 0.001). The boys were thinner and more obese than the girls. The prevalence of weight categories according to the growth reference by Werner [18] were calculated and presented (Table II).
Anthropometric data according to age groups, prevalence of thinness, normal weight, overweight and obesity for the Swedish seven- to nine-year-old children.
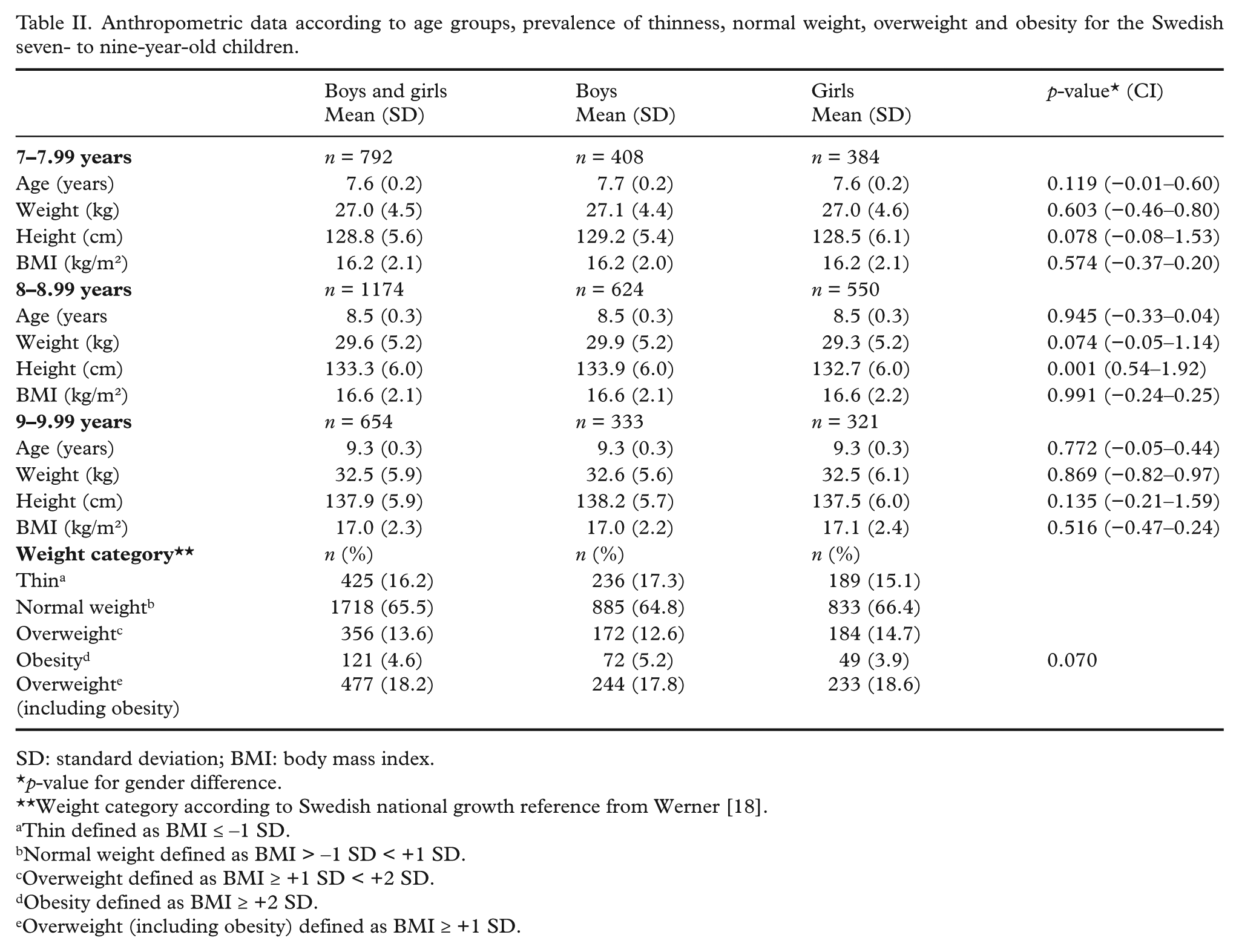
SD: standard deviation; BMI: body mass index.
p-value for gender difference.
Weight category according to Swedish national growth reference from Werner [18].
Thin defined as BMI ≤ –1 SD.
Normal weight defined as BMI > –1 SD < +1 SD.
Overweight defined as BMI ≥ +1 SD < +2 SD.
Obesity defined as BMI ≥ +2 SD.
Overweight (including obesity) defined as BMI ≥ +1 SD.
Table III shows the association between OW/OB and reported breakfast consumption as well as selected foods and beverages. We found a significant positive association between OW/OB and reports of not having breakfast every day, drinking diet soft drinks and drinking skimmed/semi-skimmed milk four days or more.
Consumption frequency of breakfast, food and beverage for normal weight and OW/OB in Swedish seven- to nine-year-old children.
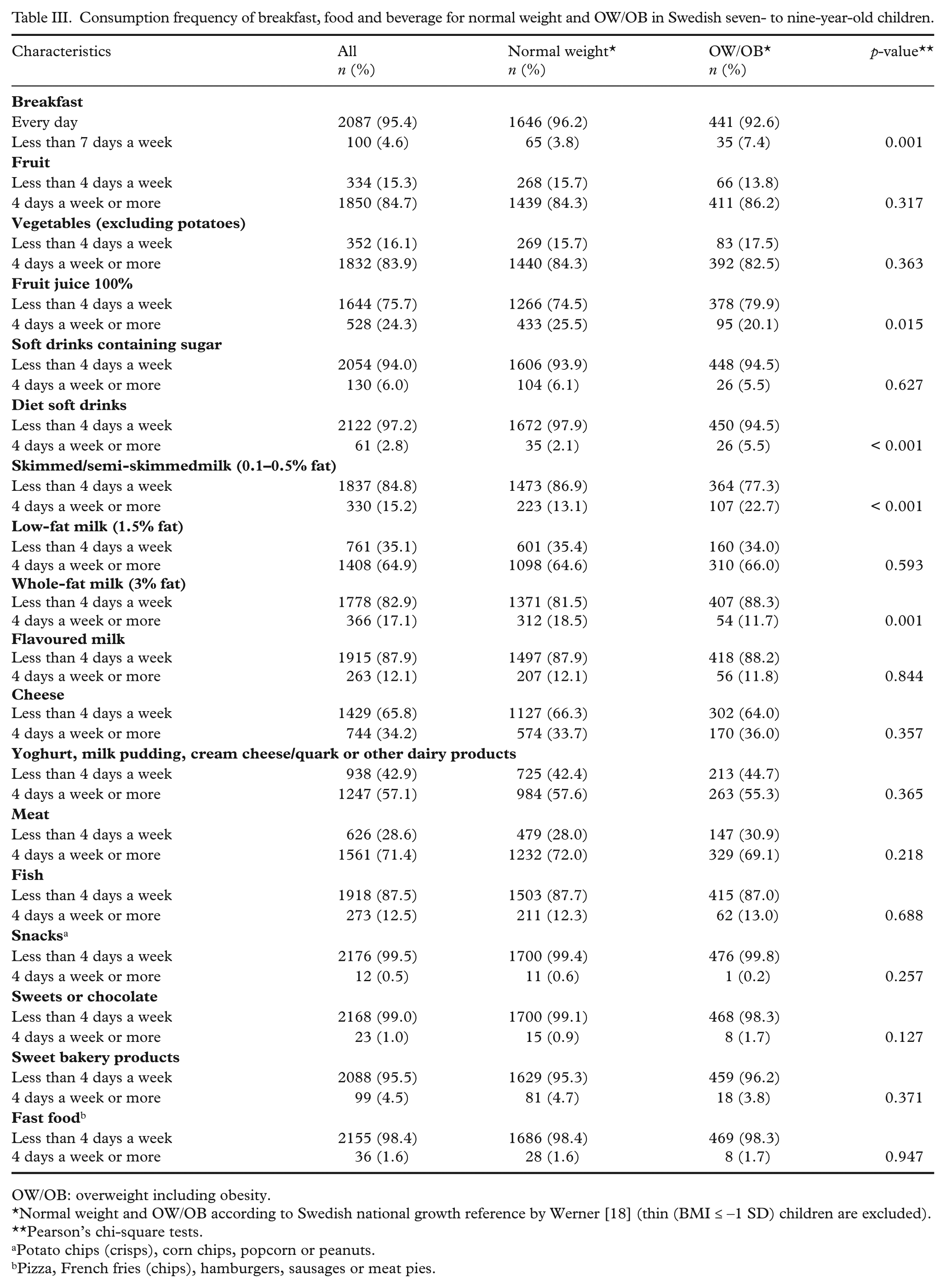
OW/OB: overweight including obesity.
Normal weight and OW/OB according to Swedish national growth reference by Werner [18] (thin (BMI ≤ –1 SD) children are excluded).
Pearson’s chi-square tests.
Potato chips (crisps), corn chips, popcorn or peanuts.
Pizza, French fries (chips), hamburgers, sausages or meat pies.
In the unadjusted regression model (Table IV), the risk of being OW/OB was higher if the child was reported not to have breakfast every day, if the child had diet soft drinks or skimmed/semi-skimmed milk. For whole-fat milk, we found an inverse association with OW/OB. Adjusting for gender, parental weight status, parents’ education level and area of living attenuated the model only slightly. Breakfast, diet soft drinks, skimmed/semi-skimmed milk remained significant. The risk of being OW/OB was higher if one of both parents was OW/OB and if the parental education level was below university degree.
Binary logistic regression for unadjusted and adjusted odds ratios (ORs) of OW/OB for Swedish seven- to nine-year-old children.
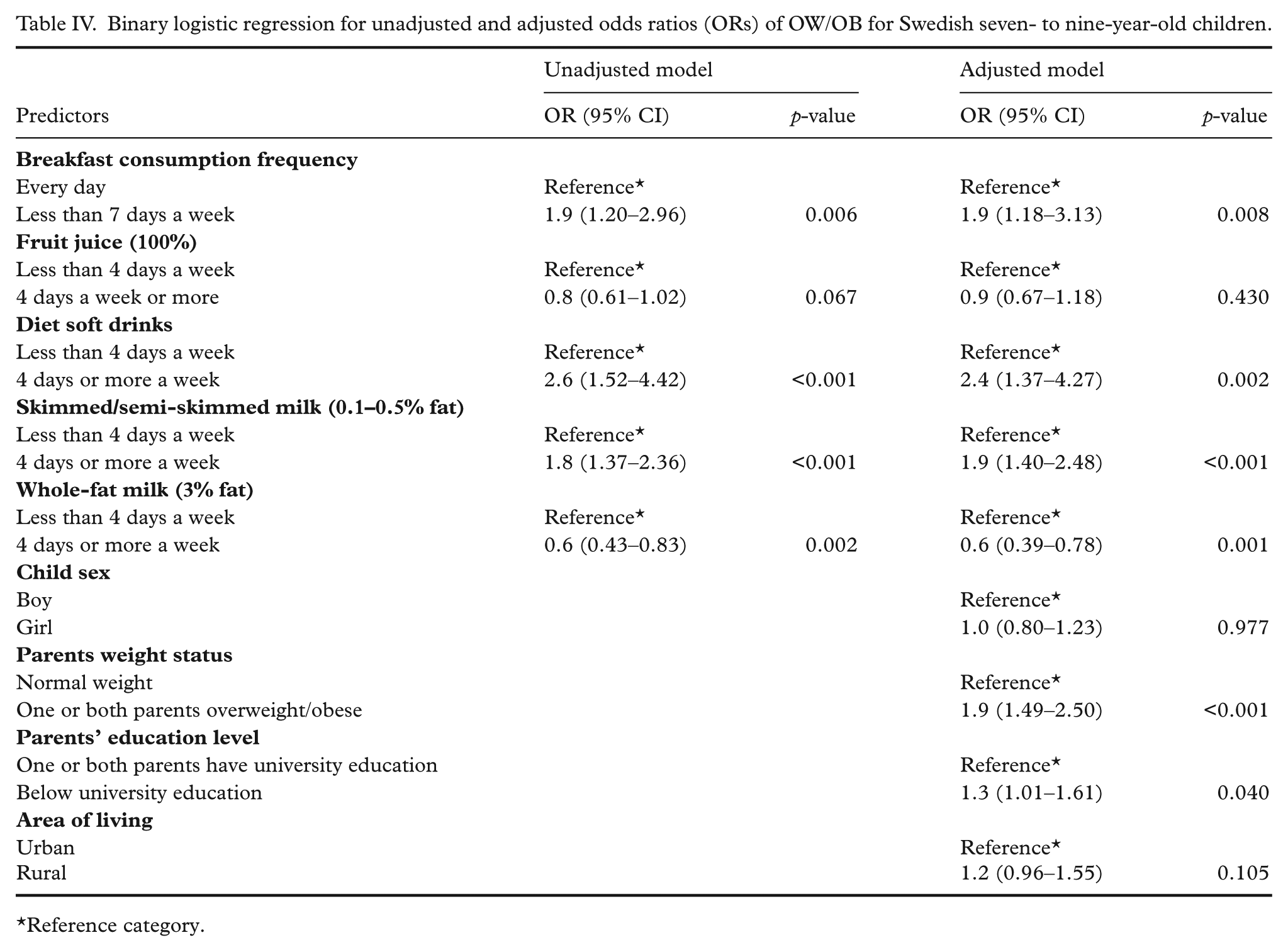
*Reference category.
Discussion
We found that the vast majority of the children were reported to have breakfast daily and f&v four days a week or more. For food items like snacks, sweets or chocolate, sweet bakery products, fast food and soft drinks containing sugar, the majority of children had these food items less than four days a week. The children were more likely to be OW/OB if the children did not have breakfast every day, had diet soft drinks and skimmed/semi-skimmed milk four days a week or more, if one or both parents was overweight/obese or if their education level was below university.
Breakfast habits
We found that the vast majority, 95.4% of the children, had breakfast daily. In a study from Norway, 91% of the children age 9–10 years were reported to have breakfast every day [20] which is in agreement with our study. In another a study on breakfast consumption among 11-, 13- and 15-year-old children and adolescents from 31 European countries, 69.4% of the Swedish children reported having breakfast daily [8], which was lower than our findings. A possible explanation to the high breakfast frequency in our study is the children’s age, since breakfast skipping has been identified as a problem more related to older children [6,8,9].
Breakfast can be defined as the first meal of the day, eaten before or at the start of daily activities within two hours of waking, typically no later than 10:00 am and containing a calorie level between 20% and 35% of daily energy need [21]. Even if we did not have information on what food items the children had for breakfast, a traditional Swedish breakfast usually contains food items such as bread or cereal, fruit (fruit juice) and low-fat milk products or other calcium sources [22], food items that are included in National dietary guidelines [22] as a part of a healthy breakfast for children [21]. In a study of Swedish 11–12-year-old children on dietary patterns reported that the reason for skipping breakfast was not enough time in the morning or that they were too tired [23].
Among the children not having breakfast every day, we also found a lower consumption frequency of f&v, a higher consumption frequency of soft drinks containing sugar, sweet bakery products, sweets and chocolate and slightly more fast food compared with the children having breakfast every day (data not shown).
In the Nordic nutrition recommendations for a healthy dietary pattern for children [7], a regular intake of breakfast is recommended [8].
Even if only 4.6% of the children did not have breakfast every day, findings from the current study indicated an increased risk of OW/OB among children who were reported not to have breakfast daily (OR 1.9, 95% CI 1.20–2.96), and also when adjusting for gender, parents’ weight status education and area of residence. These results are consistent with previous findings [2,5,9]. In a previous study from the US (2010), the prevalence of breakfast skipping for 9–13-year-old children was 20.6% for boys and 19.7% for girls. The prevalence of obesity was also higher among the breakfast skippers compared with those who had breakfast [9].
Reported frequency of intake of fruit and vegetables (f&v)
The parents reported that 84.7% and 83.9% of the children had f&v four days a week or more (Table I). In a food survey based on a four-day food registration by parents of Swedish children (Riksmaten Barn) [24], the fruit consumption for eight-year-olds was reported as 5.5 times a week for boys and girls, and the vegetable consumption frequency was 5.6 times a week for boys and six times a week for girls [24]. In another study on f&v consumption among 11-year-old children in 10 European countries, about 40% and 60% of the Swedish children reported having f&v every day, respectively [11]. For comparison, in our study, the parents reported a higher daily consumption of fruit among their children (63%), while the daily vegetable consumption in our study (55.0%) corresponded reasonably well (Table I). We also found a significant (p < 0.001) gender difference in f&v consumption, with boys more frequently having f&v less than four days a week. The same gender difference in consumption of f&v was also observed in a study of Swedish 11-year-old children [11]. The recommended intake of f&v for children in Sweden is 400 g per day, with no reference to frequency of intake [22]. It is not possible to determine if the children in our study meet the recommended intake of f&v due to limitations in our data.
Even if we did not find any association between intake of f&v and overweight and obesity (Table III), other studies have indicated that overweight children consume less f&v than normal-weight children [3].
Consumption of beverages
The majority of children (≤ 82.9%) had the different types of milk less than four days a week, except for low-fat milk where 64.9% of the children consumed low-fat milk four days a week or more (Table I). In Riksmaten Barn [20], the eight-year-old children’s consumption frequency of whole-fat milk (3% fat) was 2.7 times a week, low-fat milk (1.5% fat) 7.4 times and semi-skimmed milk (0.5% fat) 2.8 times a week. The Swedish National Food Agency recommend children in all ages to consume low-fat milk daily [22]; however, only 64.9% of the children in our study meet this recommendation.
We found that the majority of children, 94% and 97.2%, had sugar containing soft drinks and diet soft drinks, respectively, less than four days a week. A low consumption frequency of soft drinks was also found in the Riksmaten study; children aged eight had sugar containing soft drinks 2.7 times per week and diet soft drinks 0.21 times a week [24].
Reported beverage intake and overweight/obesity
We found that children who were reported having diet soft drinks and skimmed/semi-skimmed milk four days a week were 2.6 (95% CI 1.52–4.42) and 1.8 times (95% CI 1.37–2.36) more likely to be overweight (including obesity). When we adjusted for gender, parent’s weight status, education and area of residence, the results only attenuated slightly (Table IV). A possible explanation is that parents of overweight children report that their child is drinking diet soft drinks as a weight-controlling measure. Foreyt et al. [25] found a similar association between the consumption of low-calorie sweeteners and overweight and obesity among children and adolescents.
In regards to our findings concerning the increased risk of being overweight (including obesity) among children having skimmed/semi-skimmed milk four days a week, a study by Berkey et al. (2005) indicated that consumption of skimmed and low-fat milk (1% fat) may provide some children with excess energy that results in excess weight gain [26]. On the other hand, as for diet soft drinks, the parents of overweight children may have reported that their child was drinking skimmed/semi-skimmed milk as a weight controlling measurement or maybe as a more socially desirable response.
For whole-fat milk, we found an inverse association with overweight and obesity; children having whole-fat milk four days a week or more were less likely to be overweight and obese. Studies on milk consumption and association with overweight and obesity are inconclusive. A study on children from Italy (2005) also found an inverse association between whole-fat milk consumption and overweight and obesity [14], while the opposite effect was observed in a study on seven-, nine- and 13-year-old children, where a three-year excess weight gain was also associated with the intake of whole-fat milk [12].
In our study, 94.0% of the children had sugar containing soft drinks less than four days a week, but we found no significant association between sugar-containing soft drinks and OW/OB. However, other studies have identified a relationship between soft-drink consumption and OW/OB development among children [12,27].
Fast food and snacks, sweets and sweet bakery products
The parents reported that the vast majority (≥ 95.5%) of the children had fast food items, snacks, sweets and sweet bakery products less than four days a week, while avoidance is recommended [22].
Even if we did not find any association between OW/OB and consumption of fast food items, snacks, sweets and sweet bakery products, a study of seven-, nine- and 13-year-old children from the UK found that excess weight gain over a three-year period was associated with the consumption of food items such as potato crisps, French fries, sweets, desserts, full- and low-fat milk and sugar containing beverages [12].
Children’s overweight status and socio-demographic factors
In the adjusted regression model we found that if one or both parents was overweight or obese and if the parents’ education level was below university level, the children’s risk of being OW/OB increased; this has previously been reported from the full Swedish WHO COSI material from 2008 [2].
Strengths and limitations
One of the major strengths of this study was the thorough collection of height and weight data, using the WHO COSI protocol [4]. We could also see that the prevalence of normal weight, overweight and obesity was in line with previous findings from 2008 when the total Swedish WHO COSI sample was included [28]. Also, the food intake frequencies were consistent with previous findings from a National food survey [24]. Another strength of this study was that the findings were adjusted for a selection of potential confounders, which allowed for confidence in the study results.
There are several limitations to be noted. As this is a cross-sectional study, it is not possible to infer a causal relation. The self-reported questionnaire answered by parents may have been affected by limitations related to memory or misreporting of exposure. Parents who were concerned about their child’s weight status might have been more likely to over-report more favourable behaviours, for example breakfast habits and f&v consumption, and to under-report less favourable behaviours such as consumption of sugar-containing soft drinks, cookies and sweets [29] and more likely to take steps to improve their child’s diet [30]. In this material, we had no information on portion size or what food items the children had for breakfast. Bread and cereal products were not included in the questionnaire. It would have been an advantage to have one or more open-ended questions regarding other foods. This was not included due to the international data collection and the need to simplify all data collection methods.
Conclusion
The majority of the children in this study were reported to have a rather favourable food intake pattern. However, the children were more likely to be OW/OB when reported to skip breakfast and if the children consumed diet soft drinks and skimmed milk/semi-skimmed milk more than four days a week, which could be interpreted as an effect rather than a cause.
Footnotes
Acknowledgements
The authors are grateful to Eric Poortvliet, Usama Al-Ansari and Manzur Kader at Karolinska Institutet for their contribution to the data collection and handling. We are also grateful to all the staff and students, children, parents and teachers who helped out with the data collection and Trudy Wijnhoven and Joao Breda at the WHO European Region for coordinating the COSI study.
Declaration of conflicting interests
None declared.
Funding
This work was supported by funds from The Swedish Council for Working Life and Social Research and Karolinska Institutet.