
Abstract
The establishment and continuing development of a sufficient and competent public health workforce is fundamental for the planning, implementation, evaluation, effect and ethical validity of public health strategies and policies and, thus, for the development of the population’s health and the cost-effectiveness of health and public health systems and interventions. Professional public health strategy-making demands a background of a comprehensive multi-disciplinary curriculum including mutually, dynamically coherent competences – not least, competences in sociology and other behavioural sciences and their interaction with, for example, epidemiology, biostatistics, qualitative methods and health promotion and disease prevention. The size of schools and university departments of public health varies, and smaller entities may run into problems if seeking to meet the comprehensive curriculum challenge entirely by use of in-house resources. This commentary discusses the relevance and strength of establishing comprehensive curriculum development networks between schools and university departments of public health, as one means to meet the comprehensiveness challenge. This commentary attempts to consider a two-stage strategy to develop complete curricula at the bachelor and master’s as well as PhD levels.
Keywords
Considering the overwhelming health gap, also in our part of the world, caused by poor social conditions, as also demonstrated by Marmot in this issue of the Journal [1,2], there is in public health a huge need for professional competences in sociology and other behavioural sciences and their interaction with, for example, epidemiology, biostatistics, qualitative methods and health promotion and disease prevention. Being able to display health status by a monotone social stratification without further insight in living conditions only denotes a first step and does not, in itself, establish a sufficient basis for the public health professional to be able to identify the crucial health-demolishing processes in a defined population and, thus, to develop and lead well-targeted, systematic and effective public health strategies in that population. We need scientifically based, sincere insight also in social processes.
For instance, the three concepts of the social gradient in health, the ‘causes of the causes’ and the social determinants in health constitute important contributions by the social sciences, not least by Michael Marmot, as also pointed out by Westin [3]. So far, these and other sociological concepts have found too little relevance in public health teaching and research. Consequently, it is a relevant question for leads and staff of schools and university departments of public health, how well the need for providing public health students with such competences is actually met.
Such consideration is of vital importance for the professionally targeted development of population health. The establishment and continuing development of a sufficient and comprehensively competent public health workforce is fundamental for the planning, implementation, evaluation, effect and ethical validity of public health strategies and policies and, thus, for the development of the population’s health and the cost-effectiveness of health and public health systems and interventions [4,5]. Accordingly, the public health educational capacity in European countries actually increased markedly during the last decades and manifests itself in a growing membership (schools and university departments of public health) of the Association of Schools of Public Health in the European Region (ASPHER): during 2006–2016, from 69 to 112 institutional members situated all over Europe [6]. A multitude of programmes are offered across Europe [6–8]. The most frequent include bachelor and master’s programmes in comprehensive public health. Together with programmes for specialization in public health for physicians and nurses, they form a relevant background for shaping a generalist professional, accredited and authorized in comprehensive public health [9].
Like other continuous public functions in society, the future generalist public health profession shall be accountable to the population it serves, as well as to the elected leaders [10]. Accountability for the population’s health requires proficiency in the theory and practice of the development, implementation and evaluation of coherent public health strategies. They include: the systematic observation and analysis of population health and of health systems, public health and social systems and interventions; the identification of targets and target groups for intervention; choice of intervention based on scientific evidence; implementation, resource allocation and monitoring; and follow-up on the development of the health of the target population and the functioning of target health systems and public health systems (Figure 1) [11].
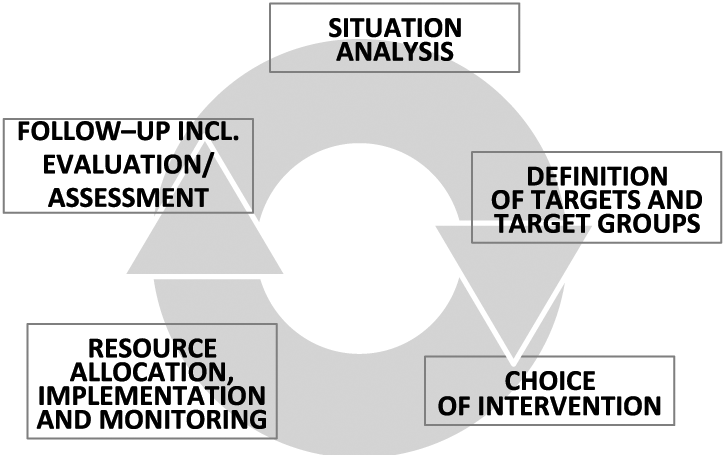
The strategic circle in public health.
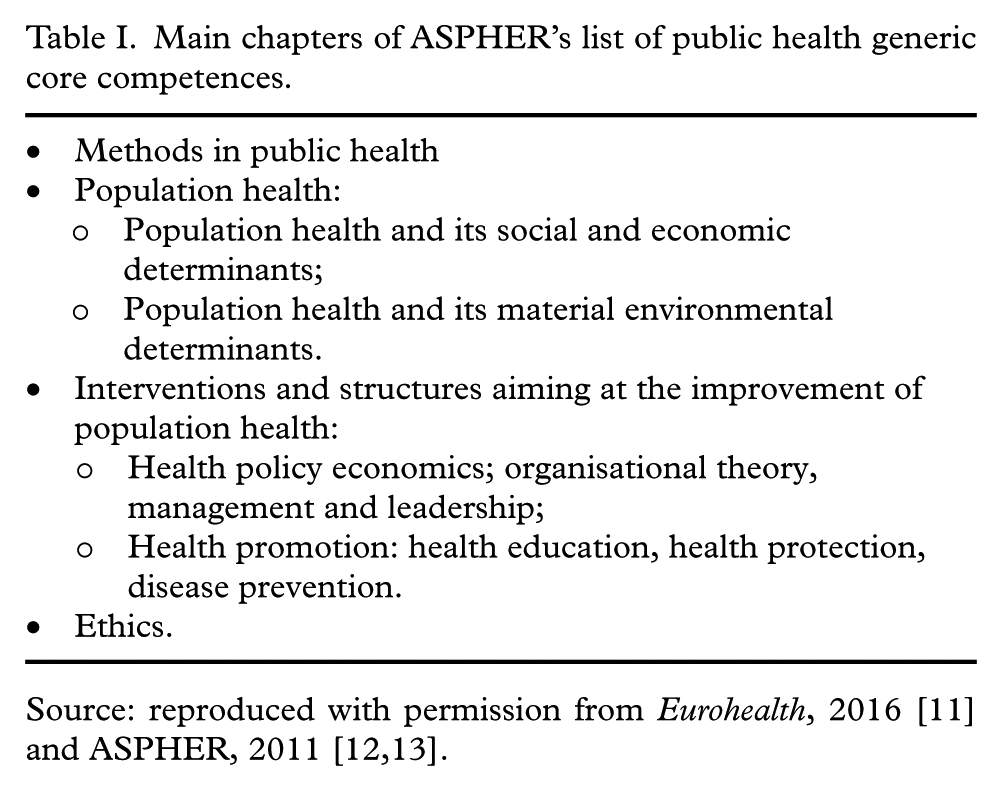
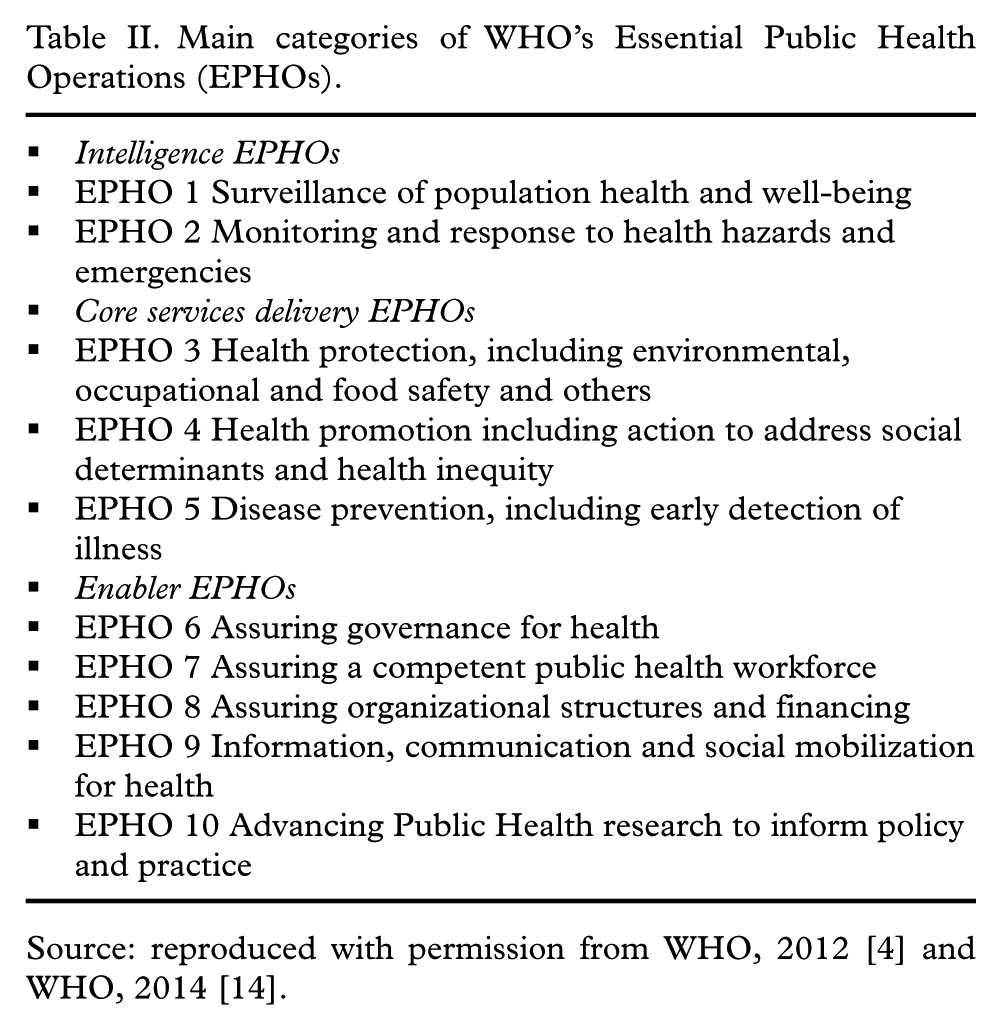
Professional public health strategy-making thus demands a background of multidisciplinary and – in the strategic perspective – mutually coherent competences. The competences profile needed – knowledge and skills – presents itself in the chapter structure of ASPHER’s lists of generic core competences for public health professionals (Table I) [12,13], endorsed by World Health Organization (WHO) Europe’s member states and included in WHO’s European Action Plan for Strengthening Public Health Capacities and Services in 2012 [4]. Moreover, as competences indicate potential to act, WHO Europe’s Essential Public Health Operations (EPHOs) [14] can represent action itself, in a likewise coherent and dynamic combined structure (Table II) [15], at the core of a generalist profession in comprehensive public health. No part of this comprehensive spectrum of competences and EPHOs should be missed in the education programmes offered by the schools and university departments – this, of course, does not only include the social and behavioural sciences, but all parts of the curriculum.
Main chapters of ASPHER’s list of public health generic core competences.
Main categories of WHO’s Essential Public Health Operations (EPHOs).
The size and structure of the staffing of schools and departments of public health, however, include substantial variation. While the larger institutions [6] are sized to be able to cover the comprehensive spectre of sub-disciplines, it is evident that smaller entities may run into problems if seeking to meet this challenge entirely by use of in-house resources. Accordingly, in a study [16] covering selected schools of public health in four countries – Poland, UK, France, Portugal – we found that the self-reported strength of competences as well as EPHOs offered by the departments and schools varied considerably.
There are, of course, various ways to meet relatively unmet curriculum needs; for example, by inviting visiting professors for short stays and by implementing IT-based solutions. Comparing competences and EPHO profiles, within as well as between countries, in our Four Country Study, showed to be complementary to some degree [16]. Thus, in a situation of scarce resources, collaboration in national as well as between country networks seems attainable as an attractive strategy for the development of comprehensive programmes.
Two educational strategies should be considered in this context. In the European Region, we generally have focussed on meeting the needs of education at the bachelor and master’s levels, without quite an identical strength of consideration at the PhD level and, furthermore, public health specialization on a bachelor and master’s basis. In the Nordic Countries, the Nordic School of Public Health NHV (NHV), over many years, formed a centre that was inspiring for the broad establishment of MPH programmes in all the Nordic Countries. Thus, NHV fulfilled its institutional mission, before it was closed in 2015 [17]. Here, one could pose the question, whether the Nordic Countries – with a combined population of 25 million and, if Baltic schools would participate, about 6 million more – would form a sufficient basis for a network-based, competitive centre of higher research education in public health.
Moreover, between-country networking can be further extended geographically, and it seems that similar considerations – on network collaboration among national and regional European schools and departments of public health – should be discussed also in other parts of Europe. Such a ‘network thinking’ aiming at strengthening the basis for comprehensive, interdisciplinary, dynamic and coherent public health education and training could constitute a massive shift towards achieving excellence, knowledge brokering and the exchange of experience concerning best practice in public health. Networking between schools of public health is a relevant theme to be considered at public health conferences at various levels – global, European, regional and national.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.