
Abstract
Aim: The first aim of this study was to explore the prevalence
of loneliness and subjective health complaints (SHCs) among school-aged children
in Finland. The second aim was to analyse to what extent perceived loneliness
explains any variance in SHCs among school-aged children.
Method: A representative sample of 5925 Finnish children
and adolescents from grades 5 (Mage=11.8 years), 7
(Mage=13.8) and 9
(Mage=15.8) completed the Health Behaviour in
School-aged Children (HBSC) survey. Descriptive statistics were used to examine
the prevalence of health complaints and loneliness. Structural equation
modelling was used to test how strongly loneliness was associated with SHCs.
Results: The prevalence of loneliness and SHCs was higher
among girls and increased with age. Loneliness was a significant predictor of
health complaints, especially of psychological symptoms among girls and among
ninth grade students.
Introduction
Adolescence is the period in human growth and development that occurs after childhood and before adulthood, which corresponds roughly to the period between 10 and 19 years of age [1]. It is a time when the risk of loneliness is greater compared to other periods of life, partly due to the many physiological and psychological changes young people go through, as well as their ever-changing social world [2]. In addition, adolescence is a vulnerable period for development of somatic and psychological symptoms [3,4].
Loneliness is a common human experience which affects most people at some point in their lives [5,6]. Excessive loneliness, however, can be painful and devastating. Research has shown that approximately one tenth of school-aged children experience social isolation, peer rejection and loneliness commonly [7,8]. This is especially concerning because we know that loneliness can have severe consequences for physical and mental health and well-being [9,10].
The current study sought to explore the prevalence of loneliness and subjective health complaints (SHCs) among adolescents in Finland and to analyse the association between loneliness and SHCs.
Loneliness as a risk to health and well-being
Loneliness is defined as a hurtful subjective experience of lacking desired social relationships [6], and it is characterised by a discrepancy between actual and desired social relationships [11]. Loneliness researchers often emphasise the important distinction between the experience of loneliness and of being alone [5,6–8,11]. Being alone refers to solitude and the reality of being without others, while being lonely is an emotional state of mind which involves a longing for human contact [5]. A distinctive feature of loneliness is that each person experiences it differently, and many factors, including genetics and the environment, impact upon these individual experiences [12]. There are also theories which hold that loneliness is associated with deficits in social skills [8] or certain personality traits [13].
Feelings of loneliness are common among school-aged children. A nationally representative study showed that nearly 60% of Finnish adolescents from grades 5, 7 and 9 experience loneliness occasionally, and for one tenth, those feelings are common [14]. These findings echo those of Junttila and Vauras [8] among 10-year-old Finnish children. Other countries have reported similar findings. Galanaki [7] studied Greek elementary school children, of which 70% experienced loneliness sometimes and 7% experienced loneliness often. The longitudinal US study of Ladd and Ettekal [15] among early to late adolescents found that 14% of participants experienced a high level of loneliness over a prolonged period. Similarly, a longitudinal study conducted in England showed that 22% of participants reported a high level of loneliness throughout the 10-year study period [16].
Loneliness, especially when experienced over a prolonged period, is associated with various health consequences, such as anxiety and depression [9,10]. Additionally, loneliness can negatively affect academic performance [17], alcohol consumption and poorer self-reported general health [16].
SHCs
SHCs are defined as symptoms of emotional distress, behavioural difficulties and health complaints unattributed to a clear medical or psychological diagnosis, for example headache, irritability and nervousness [18]. Research conducted among children and adolescents suggests that SHCs have a two-dimensional structure in which different symptoms cluster into two correlated factors: somatic (e.g. headache, stomach ache, backache) and psychological (e.g. feeling low, nervousness, anxiety) [3,4].
SHCs are more prevalent among girls and older adolescents, and the gender difference increases with age [3]. A trend study examining prevalence and stability of SHCs among adolescents from 2002 to 2010 in 34 countries indicated that health complaints are fairly stable over time in most countries, and no clear international trend can be observed between years 2002 and 2010 [19]. There is also evidence that clustering of recurrent SHCs is common among adolescents [18]. A study examining the prevalence of somatic symptoms (e.g. headache, stomach ache and backache) and their consequences for the daily lives of adolescents demonstrated that recurrent somatic symptoms can compromise the health of adolescents and have negative consequences for their every-day functioning, such as school attendance, sleep disturbances and ability to pursue hobbies [20]. In addition, recurrent psychosomatic symptoms such as headache, abdominal pain, backache, irritability and sleeping difficulties during adolescence may continue into adulthood and develop into more serious health problems [21].
Aim of this study
The existing research shows that loneliness associates with health complaints among school-aged children. However, we know less about the strength of the association between loneliness and health complaints, or how it varies by gender and grade level. The first aim of this study was to explore the prevalence of loneliness and SHCs among school-aged children in Finland. The second aim was to investigate the extent to which perceived loneliness predicts SHCs (somatic symptoms and psychological symptoms) both in general and between genders and grade levels.
Methods
Data-collection procedure
Data were collected among Finnish adolescents as part of the Health Behaviour in School-aged Children (HBSC) study in 2014. The HBSC study is an international World Health Organization collaborative study using cross-sectional surveys performed every fourth year among students in grades 5, 7 and 9. Samples were chosen from the Finnish school register using random cluster sampling. The HBSC study protocol ensures that the sample is nationally representative of the target population [22]. School principals gave approval for the survey. Participation was voluntary, and students completed a standardised questionnaire during a school lesson, following instruction from a teacher. The response rate of the participants was 85.2% in schools that took part in the survey. Students answered anonymously, and the completed questionnaires were returned via a provided sealed envelope.
Participants
Participants were 5925 students (2914 boys), of whom 2072 were from 5th grade (Mage=11.8 years), 1918 were from 7th grade (Mage=13.8 years) and 1935 were from 9th grade (Mage=15.8 years). Gender and grade level were not found to be associated in the data (χ2(2)=2.15; p=0.34), meaning that a similar proportion of boys and girls were in each grade level. The sample was mostly Caucasian with Finnish background (97%), and the majority of participants (87%) were living in urban areas.
Measures
Perceived loneliness was assessed using a single question on global loneliness: ‘Do you ever feel lonely?’ The response categories were: 1=‘yes, very often’; 2=‘yes, quite often’; 3=‘yes, sometimes’; 4=‘no’. This question was included in the Finnish national version of the HBSC questionnaire.
Subjective health complaints (psychological and somatic complaints) were assessed using the HBSC-SCL (symptom checklist), which is designed as a non-clinical measure of health complaints [4]. In addition to these symptoms, a question on anxiety was included in the Finnish national version of the HBSC questionnaire. The scale used in this study included four somatic symptoms (headache, neck and shoulder ache, stomachache, backache) and four psychological symptoms (feeling nervous, anxiety, difficulties in getting to sleep, feeling low). On a five-point response scale, the students reported the frequency of experiencing each symptom in the past six months by answering the question: ‘In the last six months, how often have you had the following?’ The response categories were: 1=‘about every day’, 2=‘more than once a week’, 3=‘about every week’, 4=‘about every month’, 5=‘rarely or never’. Cronbach’s alpha value for somatic symptoms was 0.76 and for psychological symptoms 0.80, indicating good internal consistency of the scales [23].
Demographics
Gender was recorded by asking the student to circle the correct alternative: 1=‘boy’, 2=‘girl’. The grade level was recorded by asking the student to circle the correct alternative: 1=‘5th grade’, 2=‘7th grade’, 3=‘9th grade’. Gender and grade level were used as grouping variables in the structural equation modelling.
Statistical analyses
Descriptive statistics were used to examine the prevalence of perceived loneliness and SHCs. Chi-square tests were used to analyse the bivariate associations between background variables (gender and grade level) and perceived loneliness and SHCs. The descriptive analyses were performed with the statistical package SPSS Statistics for Windows v22.0 (IBM Corp., Armonk, NY).
Structural equation modelling was used to analyse the extent to which loneliness explains the variance in somatic and psychological symptoms. Statistical analyses were performed using the statistical package Mplus v7.0 (Muthén and Muthén, Los Angeles, CA). The parameters were estimated using the maximum likelihood robust (MLR) estimation method, which is robust to non-normality of observed variables. The cases with a few missing values were included in the analyses and treated with the missing at random (MAR) data procedure in Mplus.
The analyses were performed as follows. As a first step, the structure of the HBSC-SCL (symptom checklist) was determined, and two alternative theoretical models were estimated separately and compared using scaled chi-square tests for difference, SB χ2 [24]. To analyse the extent to which perceived loneliness predicts SHCs, loneliness was added as a predictor to a two-factor model of SHCs, and paths (regression coefficients) from perceived loneliness to two latent factors, somatic and psychological symptoms, were estimated. The gender and grade-level differences were analysed by estimating models simultaneously for subgroups and by adding constraints first to factor loadings and second to regression coefficients. Nested models were then compared by scaled chi-square test.
The model fit was evaluated using the chi-square test, the root mean square error of approximation (RMSEA), the comparative fit index (CFI), the Tucker–Lewis index (TLI) and the standardised root mean square residual (SRMR). As the chi-square test is highly sensitive to large sample size, Bentler and Bonnett [25] recommend using the relative goodness of fit indices in addition to the chi-square test. According to Hu and Bentler [26], a cut-off value <0.06 for the RMSEA and value <0.08 for SRMR indicate good fit. For CFI and TLI, values >0.95 indicate a good fit.
Results
Prevalence of SHCs and loneliness
The prevalence of SHCs experienced weekly or more often and that of loneliness experienced very or quite often are presented in Table I. Results show that girls experience somatic and psychological symptoms more often than boys (p<0.001 for all symptoms). Nearly half of girls reported having headache weekly or more often, 51% reported feeling nervous at least weekly and 41% reported having difficulties getting to sleep weekly or more often. For boys, the most common somatic symptom was headache (32%), and the most common psychological symptoms were feeling nervous (39%) and difficulties in getting to sleep (32%). The biggest difference between boys and girls was in feeling low, which was two times more common among girls than among boys (30% compared to 15%).
Percentage of students experiencing health complaints weekly or more often, and percentage of students experiencing loneliness quite or very often.
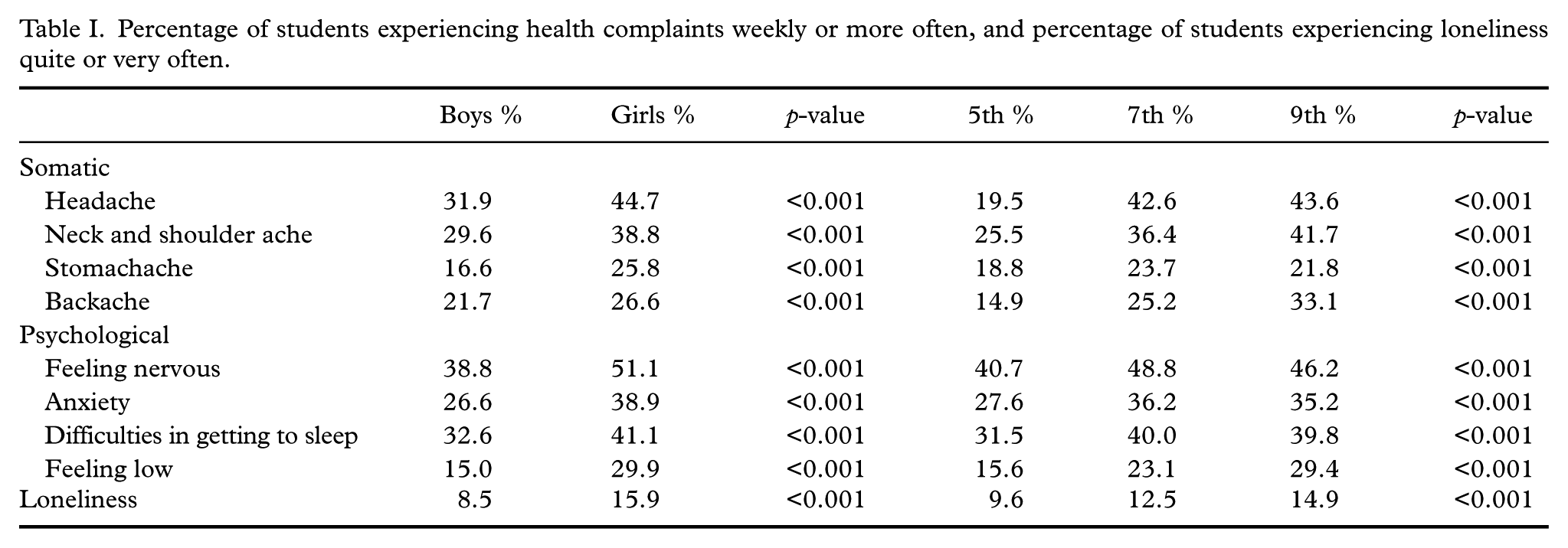
All SHCs were more common among the upper grades of basic education (p<0.001 for all symptoms). Prevalence of weekly headache was 23% more common in 7th grade compared to 5th grade. Neck and shoulder pain and backache were also >10% more common among 7th grade students compared to 5th graders. For psychological symptoms, the prevalence of anxiety and difficulties getting to sleep were 9% more common among 7th graders compared to 5th graders.
Prevalence of perceived loneliness followed the trend of health complaints. Loneliness was more common among girls than among boys (p<0.001), and participants tended to be lonely more often in higher grade levels (p<0.001).
Similar gender and grade-level differences were observed when analysing the daily SHCs and loneliness being experienced very often. The prevalence of each was higher among girls compared to boys (e.g. headache: boys 2.8%, girls 6.8%; difficulties getting to sleep: boys 5.3%, girls 8.7%; loneliness: boys 3.3%, girls 5.3%) and incidence of daily SHCs and loneliness being experienced very often also increased with age (e.g. headache: 3.0% in 5th grade, 5.7% in 7th grade and 5.9% in 9th grade; difficulties getting to sleep: 6.3% in 5th grade, 7.7% in 7th grade and 7.2% in 9th grade; loneliness: 2.9% in 5th grade, 5.1% in 7th grade and 5.2% in 9th grade).
Relationship between experienced loneliness and SHCs
The correlations, means and standard deviations for the reported SHCs and loneliness are presented in Table II. All correlations were statistically significant. The highest correlations were between backache and neck and shoulder pain (r=0.62) and between anxiety and feeling nervous (r=0.59). Loneliness correlated highest with feeling low (r=0.50) and lowest with neck and shoulder pain (r=0.22) and backache (r=0.22).
Pearson correlations between the subjective health complaints and loneliness.
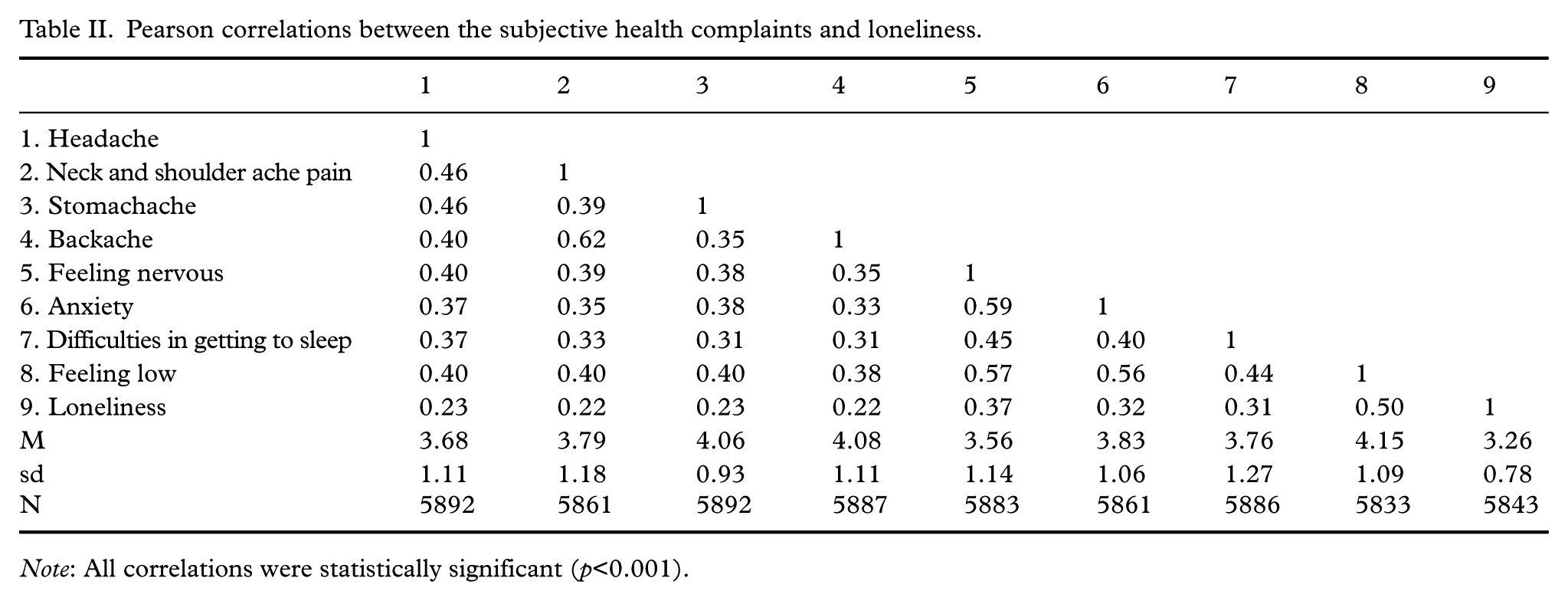
Note: All correlations were statistically significant (p<0.001).
Confirmatory factor analysis (CFA) was used to confirm the two-dimensional structure of the HBSC-SCL-scale. One- and two-factor models were compared, and a scaled chi-square difference test showed that the goodness-of-fit of the two-factor model was significantly better than that of the one-factor model: SBχ2(1)=447.22, p<0.001. To answer our research question, to what extent loneliness explains variance in SHCs, we estimated the model in which perceived loneliness was added as a predictor for the two-factor model of somatic and psychological symptoms by estimating the regression coefficients from loneliness to the two latent factors. Based on the modification indices, the errors between the items ‘backache’ and ‘neck and shoulder pain’ were allowed to correlate, as research shows that concomitant neck and low back pain has constantly increased among adolescents [27].
After modifications, the fit indices showed good fit for the model in which the regression coefficients were added from loneliness to somatic and psychological symptoms: χ2(24)=299.18, p<0.001; RMSEA=0.04, SRMR=0.02, CFI=0.98, TLI=0.97. All variables measuring somatic and psychological symptoms had high factor loadings varying from 0.57 to 0.76. The regression coefficient between loneliness and somatic symptoms was 0.33 (p<0.001), and between loneliness and psychological symptoms it was 0.51 (p<0.001), indicating that loneliness is a significant predictor of both somatic and psychological symptoms among school-aged children. Loneliness explained 11% of the variance in somatic symptoms and 26% of the variance in psychological symptoms. All estimated parameters were statistically significant and are presented in Figure 1.
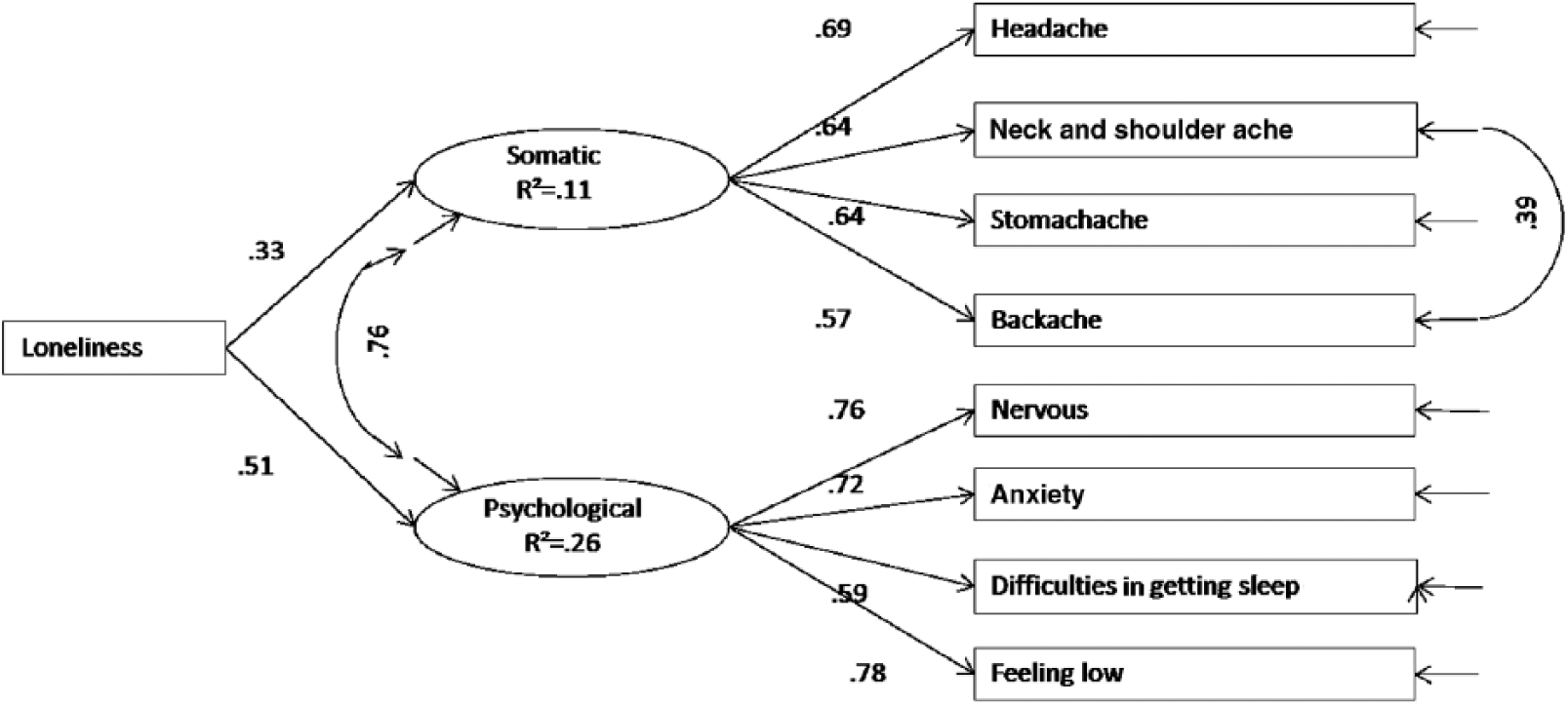
Perceived loneliness as a predictor for subjective somatic and psychological symptoms (n=5796). Standardised estimates.
Gender and grade-level differences
Multi-group comparisons were used to analyse how strongly loneliness predicts somatic and psychological symptoms according to gender and grade level. Using a multi-group model, we estimated the model simultaneously for boys and girls and for 5th, 7th and 9th grade students. The fit indices showed good fit for the model estimated for boys and girls: χ2(54)=374.11, p<0.001; RMSEA=0.05, SRMR=0.03, CFI=0.97, TLI=0.97. The fit indices also showed good fit in the model which estimated simultaneously for different grade levels: χ2(84)=405.89, p<0.001; RMSEA=0.04, SRMR=0.03, CFI=0.97, TLI=0.97. Loneliness explained higher amount of variance in somatic and psychological symptoms among girls and students in higher grades. All estimated parameters were statistically significant and are presented in Figure 2.
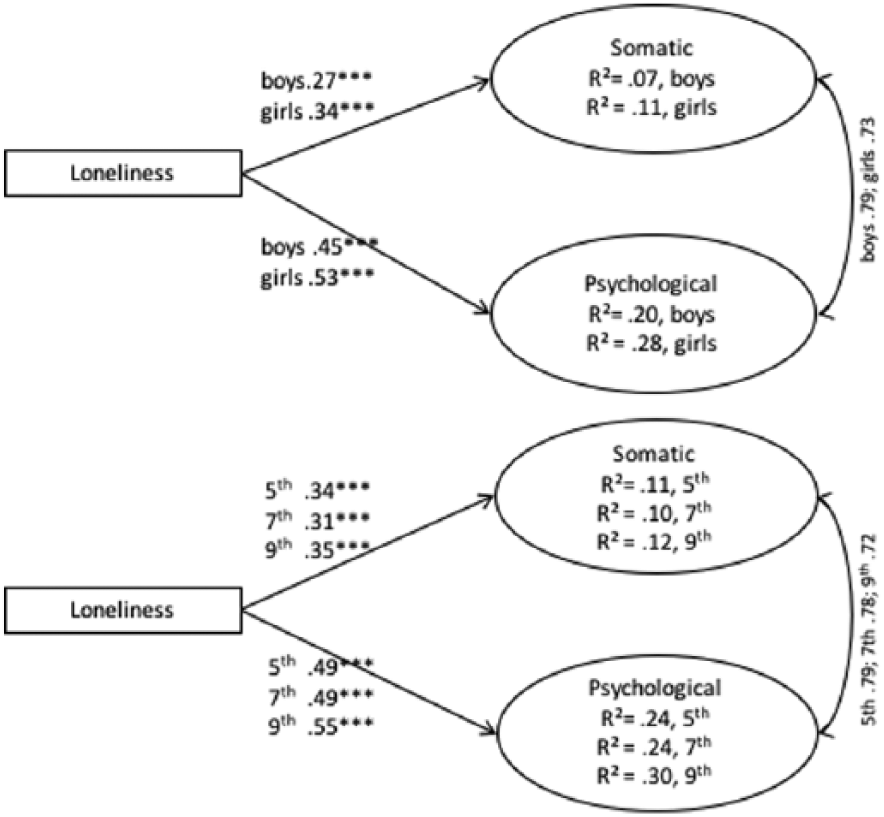
Regression coefficients of loneliness predicting somatic and psychological symptoms in subgroups formed by gender and grade level, separate models. Factor loadings set equal, standardised estimates.
Finally, we analysed if loneliness was an equally strong predictor of SHCs in subgroups formed by gender and grade level. We estimated a model in which regression coefficients were set as equal between groups and tested the model fit of the constrained model using a scaled chi-square test. The test showed that regression coefficients cannot be set equal between boys and girls (SBχ2(2)=21.80, p<0.001) or between different grade levels (SBχ2(4)=14.89, p=0.005), indicating that the strength in which loneliness predicts health complaints varies among subgroups.
Discussion
The aims of this study were (1) to explore the prevalence of SHCs and feelings of loneliness among school-aged children and (2) to analyse to what extent loneliness explained the variance in subjective somatic and psychological symptoms among children and adolescence. The results show that the prevalence of somatic and psychological symptoms is high among Finnish school-aged children, a finding reflected in the increasing trend evident in the literature over recent decades towards such high levels of symptoms [14,19]. In this study, students’ gender and grade level were associated with prevalence of symptoms. Girls and students in upper grades of basic education reported more common health complaints, which is in line with comparative studies internationally [19,28]. In addition, the prevalence of SHCs among adolescents has been stable over past two decades [3].
The prevalence of frequent feelings of loneliness was 9% among boys and 15% among girls, and the feeling of loneliness was significantly more common among girls than among boys. Galanaki [7] has reported similar gender differences and suggested that such gender differences might originate from different socialisation practices; girls are encouraged to place a higher emphasis on human relationships and to express their emotional experiences more openly than boys.
The second aim of this study was to analyse to what extent loneliness associates with SHCs. The CFA gave a clear indication that there are two dimensions underlying the phenomenon of SHCs, as shown in previous research [3,4]. The main finding was that perceived loneliness was a significant predictor of both somatic and psychological symptoms, especially among girls and among 9th grade students, among whom loneliness explained 28% and 30% of variance in psychological symptoms, respectively. Although much research exists showing the relationship between loneliness and physiological and mental problems [9,10,15,16], less is known regarding the extent to which loneliness explains such symptoms or regarding the difference in strength of association between genders and between grade levels. We know from the literature that health complaints are more common among girls, but this study elucidates this finding further by demonstrating that loneliness is a stronger predictor of health complaints among girls than among boys. Similarly, health complaints are known to be more common in upper grades, but this study further shows that loneliness is a stronger predictor of such symptoms among students aged 15 than among younger students.
Strengths and limitations
The strength of the HBSC study is that it is a nationally representative study conducted every four years [22], which affords the possibility of following trends in adolescent health behaviours over time. However, due to the cross-sectional nature of the data, causal interpretations are not possible in this study design. The data are self-reported by nature, which in this case can been seen as strength. Studies indicate that children and adolescents are capable of reporting health symptoms adequately and understand the concepts of health complaints [29]. Loneliness is by definition a subjective feeling, which only the one experiencing it can report. Previous research of Galanaki [7] indicates that >80% of a sample of 12-year-old children understood loneliness as different from being alone. In the HBSC study, loneliness is measured by just one open question: ‘How often do you feel lonely?’ Although research has shown that one loneliness question is strongly correlated with the widely used UCLA measure of loneliness [30], differing conceptions of loneliness between participants and researchers may be seen as a limitation in such a question.
Conclusions
Given the increased capacity for intimacy, loneliness in general is expected to decrease from mid- to late adolescence. However, not all adolescents succeed in establishing intimate and satisfying peer relationships [2,13,15,16]. The strength of association between loneliness and SHCs is significant and worthy of attention. While much political and civic focus is often concentrated on the mental and physical health levels of young people, the strength of loneliness as a predictor of such health levels is informative in identifying one area where efforts might be concentrated in order to prevent ill-health among today’s youth. Future research might benefit from a focus on exploring further this association between loneliness and SHCs and the complexity of each, with a view to suggesting what actions might best be taken to support adolescents’ physical, social and emotional well-being.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.