
Abstract
Aims: To investigate if any differences in unmet healthcare needs between persons registered at public and private primary care providers exist in Skåne (southernmost Sweden). Methods: The 2012 public health survey in Skåne was conducted with a postal questionnaire and included 28,029 respondents aged between 18 and 80 years. The study was cross-sectional. If the responder in the last three months had perceived oneself to be in need of medical care by a physician but did not seek it, this was used as a measure of unmet healthcare needs. Differences in unmet healthcare needs in relation to the primary care provider were investigated while adjusting for socioeconomic status and self-rated health in a logistic regression. Results: Differences in unmet healthcare needs were small and non-significant when comparing public and private healthcare providers. Non-manual workers were to a somewhat higher extent using private providers while manual workers showed a reverse pattern. Unmet healthcare needs had decreased slightly since 2008, but so had the response rate.
Keywords
Introduction
Strong primary care (PC) is associated with better population health [1–3], improved quality of care [4], reduced socioeconomic inequality in health [1], higher self-rated health for people with chronic diseases [5] and better cost control [6]. Moreover, good health outcomes at a national level correlate to beneficial economic outcomes, such as productivity and output [7], and it is therefore not surprising that adequate access to healthcare services has been a major goal of many European policymakers.
PC offers services that do not require advanced medical equipment and is responsible for guiding the patient to the right level within the health system. The most common form of PC practice in Sweden is a facility with four to six general practitioners (GPs), complemented by other staff categories such as nurses, midwives, physiotherapists and psychologists [8].
During the last decade Swedish healthcare has undergone political reforms in an attempt to improve availability and quality. Until recently, the healthcare system was run by the public sector alone, largely the product of past national governments led by the Social Democrats. Sweden’s healthcare decision making is decentralized into 21 elected county councils, which own and operate almost all hospitals and a majority of PC facilities. In the 1990s the centre-right national government proposed changes to facilitate privatization of the PC, but it was not until 2007 that the first county councils implemented these changes [9].
In 2010 the centre-right national government enacted a change in the national Health Care Act, which made choice of provider and freedom of establishment for private PC providers mandatory with public payment [10]. The theory behind patient choice of provider is to improve efficiency, quality and responsiveness of the healthcare system through the threat of exit [11]. In Sweden, registration at PC practices is primarily passive on the grounds of prior use or proximity, but with an option to change provider actively [12].
Today, private providers account for over 40% of all PC practices. However the distribution of private providers varies with a higher prevalence in urban areas [13]. The national regulation of freedom of establishment for providers limits county councils’ influence over private providers’ decisions about where to set up their practices. The Swedish reimbursement system for PC varies among county councils but is largely determined by capitation (an annual sum per listed individual adjusted for age, illness and socioeconomic indicators), a fee-for-service (payment per visit) and a small portion of pay-for-performance according to certain set targets [14]. There is to date no evidence that the quality or efficiency of private providers differs systematically from those of public providers in Sweden, nor should such differences be expected as the responsibilities and reimbursements are the same irrespective of their ownership [9].
Although high-quality healthcare is universally accessible for all citizens to a reasonable expenditure, waiting time and poor continuity/lack of patient centredness as well as unequally distributed services are ongoing challenges in Swedish healthcare [8]. In a recent report Swedish healthcare features were for the most part evaluated as ‘medium’ on a scale weak–medium–strong. Access was evaluated as medium and continuity weak, while for comparison the neighbour Denmark was rated strong in both these features [15].
A study in Skåne, the southernmost part of Sweden, based on register data 2007–2011 showed that healthcare utilization in terms of both number of individuals that had visited a GP and number of GP-visits per capita had increased in all defined subgroups since the privatization and free choice reform, but that people above 64 belonging to a family with an income above median had more advantage of the reform [16]. National data indicate that the reform has had a negative impact on the provision of services for persons with complex needs [17].
Unmet need has been referred to as a measure of ‘the differences, if any, between those services judged necessary to deal appropriately with defined health problems and those services actually being received’ and ‘an unmet need is the absence of any, or of sufficient, or of appropriate care and services’ [18]. The most commonly used measure of access to healthcare is self-assessed unmet need (SUN) [19,20]. This subjective assessment of unmet healthcare need assumes the patient to be the best assessor of their health status and whether they have received the most appropriate healthcare. The relationship between SUN and utilization depends upon how SUN is defined, upon the framing of the questions and upon the possible reasons for unmet need that are included. Most existing studies of unmet need have been carried out in the United States and have measured unmet need with survey questions referring to the past 12-month period [20]. In this study we investigate unmet healthcare needs in the previous three months.
The aim of this paper is to examine whether there are any differences in unmet healthcare needs between public and private PC providers in Skåne, and if unmet healthcare needs overall have decreased since the Healthcare Act reform. Also we examine if there are any differences in distribution of the socioeconomic status (SES) groups between the two types of PC providers.
Methods
Study population
Public health surveys have been conducted regularly in Skåne, the southernmost region of Sweden, by Region Skåne. In this study data from the 2012 public health questionnaire are used. The study is cross-sectional and based on a stratified random (weighted) sample of people living in Skåne according to the public register of residents. In the 2012 survey 28,029 people responded to the postal questionnaire, which accounts for a 51.7% response rate. Three reminding questionnaires were sent to the initial non-respondents, including a final shorter version. The study has been approved by the ethical committee at Lund University, Sweden.
Definitions
Dependent variable: Unmet healthcare needs during the past three months were assessed with the self-reported item: ‘Have you during the past 3 months considered yourself to be in need of healthcare by a physician, but not sought such care?’, with the options ‘No’ and ‘Yes’.
Self-reported causes of unmet healthcare use during the past three months were assessed with the question: ‘What was your reason for not seeking care?’ with the alternative responses: ‘could not afford’, ‘did not have time’, ‘the symptoms disappeared’, ‘too long waiting time’, ‘do not think I can get help’, ‘did not get in contact on the phone’, ‘did not get contact with doctor’, ‘did not know any doctor’, ‘wanted to wait for a while’ and ‘other’ (with the possibility to fill in the reason).
Independent variables: Private and public PC provider was attained from the questionnaire where the responders had answered the question ‘How is your primary care organized?’ and the alternatives were ‘Public’, ‘Private’ and ‘Don’t know’.
Age is analyzed in intervals of 18–24, 25–34, 35–44, 45–54, 55–64 and 65–80 years of age.
All analyses were stratified by sex.
Country of birth was divided into ‘Born in Sweden’ and ‘Born in other country than Sweden’.
Marital status was investigated with the question ‘What is your civil status?’, with the options ‘married, registered partnership, or cohabiting’, ‘unmarried’, ‘divorced’ and ‘widow/widower’.
SES by occupation includes 11 categories: Higher non-manual employees, medium level non-manual employees, low level non-manual employees, skilled manual workers, unskilled manual workers, self-employed/farmers, those on long-term sick leave, students, early retired before age 65 years (for health reasons or entitlement in the employment contract), old-age pensioners (older than 65 years), and unclassified.
Self-rated health was assessed with the item ‘How do you consider your general health status?’ and had five alternatives: ‘Very good’, ‘Good’, ‘Neither good nor poor’, ‘Poor’ and ‘Very poor’.
Statistical analysis
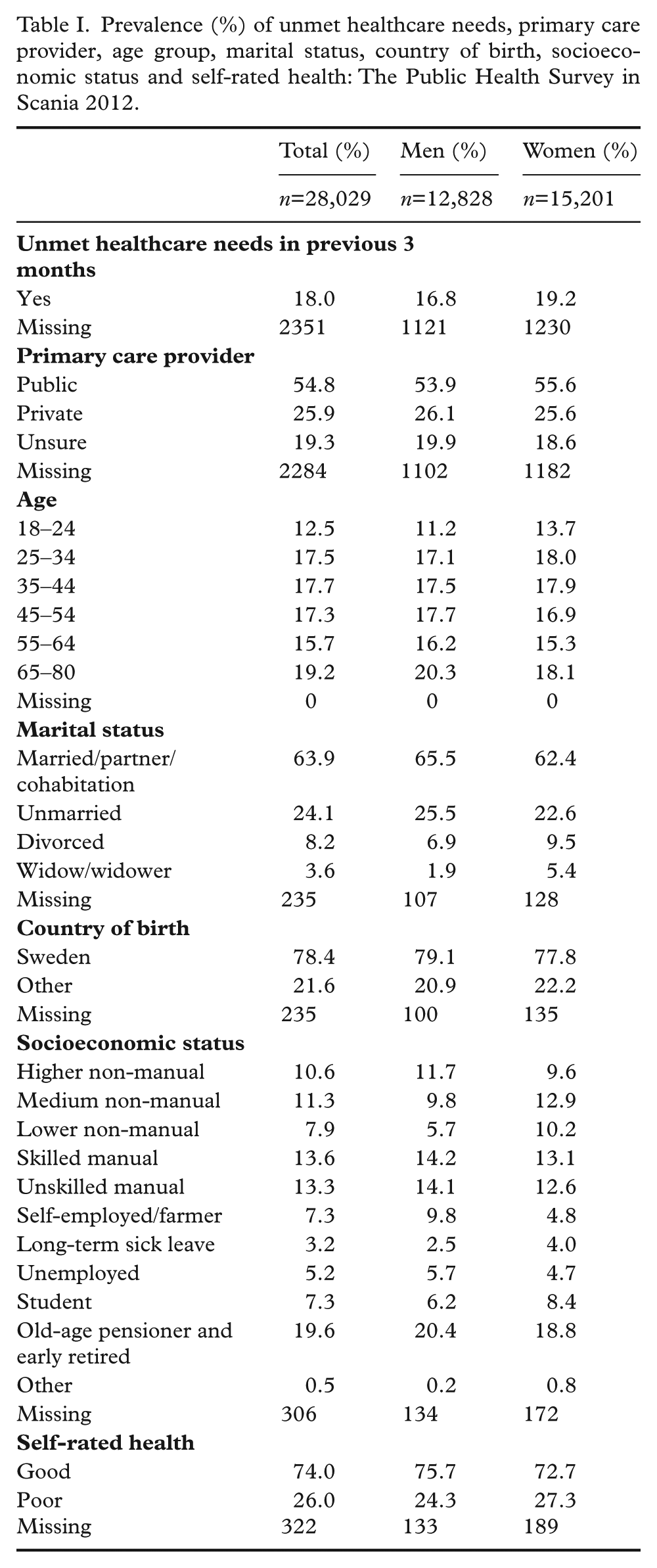
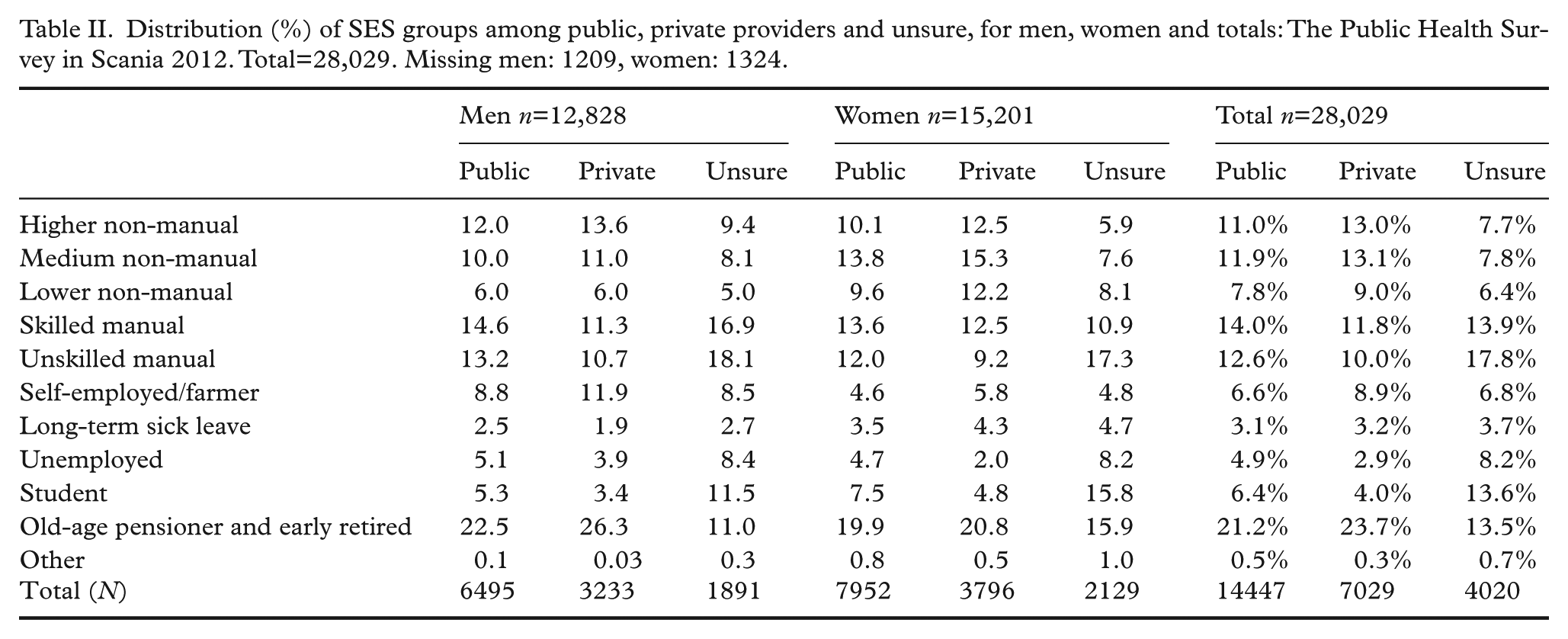
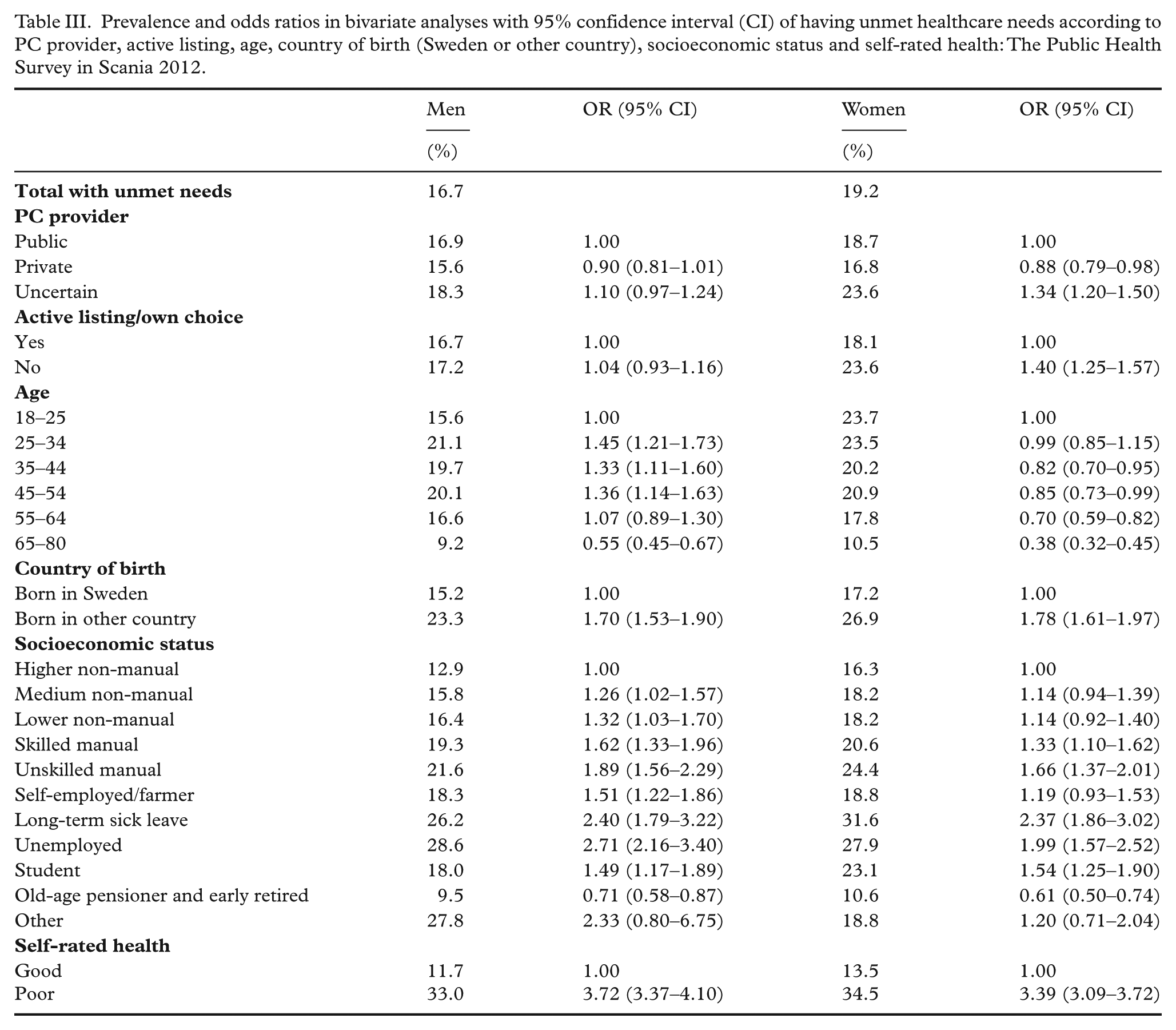
The prevalence (%) of unmet healthcare needs during the past three months, country of birth, marital status, self-rated health, SES according to occupation and persons listed at private and public primary care providers were calculated (Table I). The distribution (%) of each SES class among public and private PC providers as well as unsure was calculated (Table II). The prevalence (%) within strata of each variable and odds ratios (ORs) with 95% confidence intervals (95% CIs) of unmet healthcare needs during the past three months were calculated using bivariate logistic regression analyses (Table III). Age-adjusted and multiple adjusted ORs and 95% CIs of unmet healthcare needs according to PC provider were calculated in multivariate logistic regression analyses (Table IV). All analyses were stratified by sex. The statistical analyses were performed using the SPSS PASW software package version 22.0.
Prevalence (%) of unmet healthcare needs, primary care provider, age group, marital status, country of birth, socioeconomic status and self-rated health: The Public Health Survey in Scania 2012.
Distribution (%) of SES groups among public, private providers and unsure, for men, women and totals: The Public Health Survey in Scania 2012. Total=28,029. Missing men: 1209, women: 1324.
Prevalence and odds ratios in bivariate analyses with 95% confidence interval (CI) of having unmet healthcare needs according to PC provider, active listing, age, country of birth (Sweden or other country), socioeconomic status and self-rated health: The Public Health Survey in Scania 2012.
Age-adjusted and multivariate odds ratios (OR) and 95% confidence interval (CI) of unmet healthcare needs in relation to PC provider: the Public Health Survey in Scania 2012.
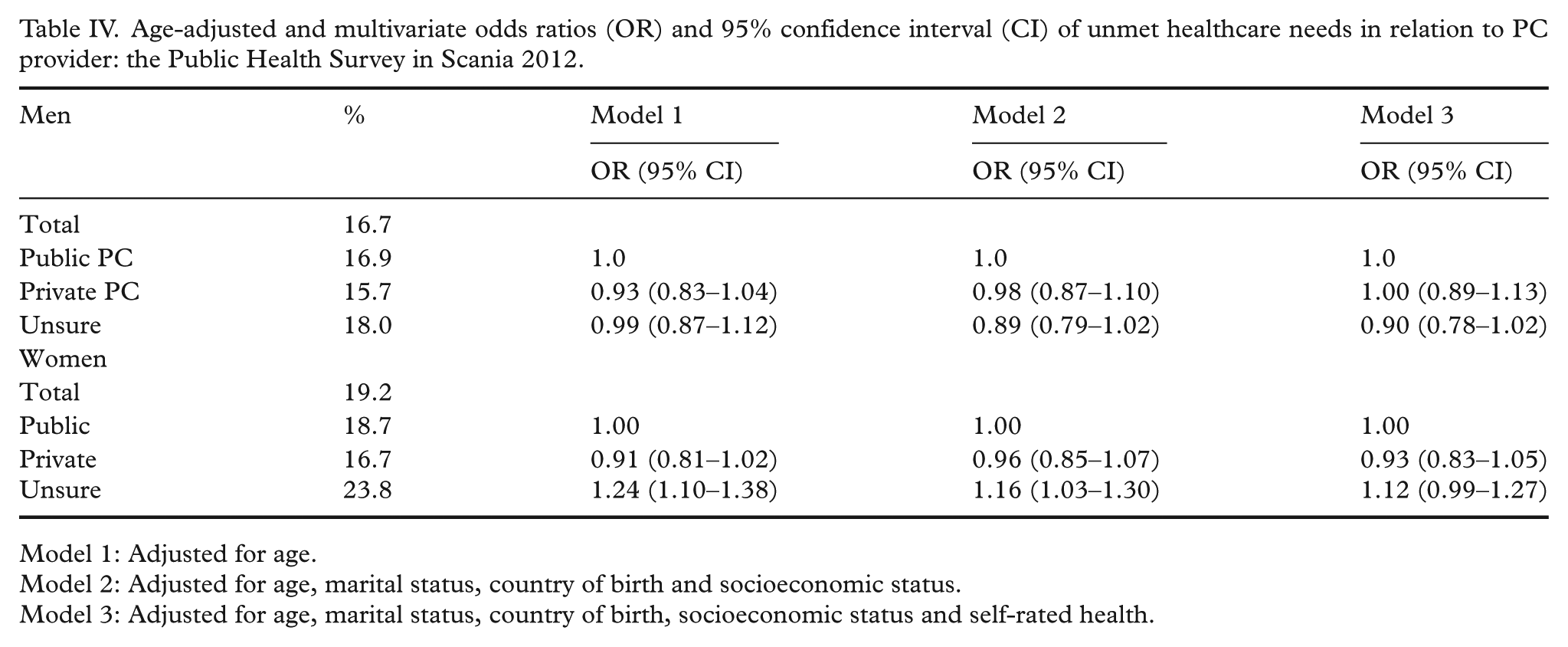
Model 1: Adjusted for age.
Model 2: Adjusted for age, marital status, country of birth and socioeconomic status.
Model 3: Adjusted for age, marital status, country of birth, socioeconomic status and self-rated health.
Results
Table I shows the prevalence (%) of unmet healthcare needs, marital status, country of birth, SES, self-rated health and listed PC provider. Table II demonstrates that the private providers had a somewhat higher prevalence of non-manual workers for both men and women, while they had a somewhat lower prevalence of unemployed and manual workers compared with the public providers. The distribution of people on long-term sick leave was similar between the providers. Table III shows that factors such as being born outside Sweden, manual work, being on long-term sick leave or unemployed or having poor self-rated health were associated with significantly higher unmet healthcare needs. Men and women on private PC provider patient lists reported somewhat lower unmet healthcare needs (OR 0.90 and 0.88, respectively) but this was only significant for women. Table IV demonstrates that when adjusted for age, marital status, country of birth, socioeconomic status and self-rated health the differences in unmet healthcare needs attenuated and became non-significant also for women.
Discussion
Unmet healthcare needs did not differ significantly between public and private providers when adjusted for age, marital status, country of birth and SES. However, the number of persons reporting not knowing how their PC provider was organized was fairly high (16.8%). A disparity in SES distribution between the PC providers was seen, which has also been reported in previous studies [16,17]. People in the work force reported to a significantly higher extent lack of time as a reason for not seeking care, while people on sick leave and the unemployed had a higher prevalence of reporting that they could not afford to seek care [21].
Unmet healthcare needs had overall decreased slightly compared with the 2008 survey for both men and women, when unmet needs were 17.4% for men (16.7%, 2012) and 20.4% for women (19.2%, 2012). Whether this is due to the reform or other factors is unclear. There has been a small downward trend of unmet healthcare needs in Skåne since they first were assessed in 2000. However, the response rate has also decreased somewhat over time. In the years 2000 and 2004 the overall response rate was 59%, in 2008 54.1% and in the questionnaire used in this study 51.7%.
Swedish PC organization stands out compared with most other European countries for several reasons. The GPs in Sweden are employed and salaried by the county council or healthcare companies in contrast to most European GPs who are self-employed [9,22]. Although Sweden uses financial incentives to encourage patients to register with a GP and obtain referral to specialist care, it is one of only a few European countries without a national system of gatekeeping function (where referral is needed for secondary care) [8,22]. When compared internationally, the average number of outpatient visits (to a GP as well as to specialist outpatient services) is considerably lower in Sweden than in other countries, being three per person a year, compared with six on average for Organization for Economic Cooperation and Development countries [23]. This may be due to the organization of healthcare in Sweden, where a greater number of visits are done by nurses, and to the fact that Swedish healthcare is dominated by hospital-based care. Access to outpatient care is also considered to be lower in Sweden than in other countries [17].
Despite the reforms in 2007–2010, Swedish PC continues to suffer with poor doctor continuity and accessibility. To help get an understanding of the issues in Swedish healthcare and how to improve it, it is convenient to compare Sweden’s performance in a global perspective and especially to other countries with a universal healthcare. The comparison with Denmark is particularly interesting as Danish PC scores higher in most characteristics including accessibility and continuity [15] with a lower healthcare expenditure than Sweden’s: US$6463/capita compared with Sweden’s US$6808/capita[24]. The cost does not correlate to the number of visits to a physician as Denmark has a higher number, 4.4 visits per year and person, while Sweden has 2.9 [25], despite Sweden having a higher physician density (Sweden has 4.1 physicians per 1000 while Denmark has 3.6) [26]. The majority of Danish GPs are self-employed, work on contract for the public funder and work in small units of one to two GPs [27]. Swedish GPs, despite privatization, continue for the most part to be employees of public or private providers and typically work in larger settings of 4–10 GPs [8,17]. A stronger autonomy over the work situation as well as a different reimbursement system (a pay for service and capita instead of a fixed salary) may partly explain why Danish GPs statistically perform better than Swedish GPs. Since the fee-for-service was introduced in addition to the capitation-based payment, Denmark has seen fewer referrals to specialists while the volume of fee-for-service has increased [27], hence economic incentives seem to stimulate productivity.
There is an increasing number of patients who visit emergency departments in Sweden [28] while the number of hospital beds is steadily decreasing[29]. Sweden has the lowest number of hospital beds per capita in Europe after Lichtenstein [30]. A stronger PC with improved availability and doctor continuity could prevent unnecessary visits to the emergency rooms as well as delayed treatments. Several studies have shown that continuity of care is associated with lower mortality for all causes, better access to care, less re-hospitalization, less need for specialist care, less use of emergency care and better detection of medical adverse effects [22].
Strengths and limitations
The study population was large with a large number of participants. The study involved a random, weighted sample of the population, which gives a representative view of the general population. The total participation rate was 51.7% after reminders. The non-response analysis showed that women, older people, people born in Sweden, married people and those with a higher income and higher level of education responded to a somewhat greater extent. The risk of selection bias is still limited.
The measure of unmet healthcare needs in this study was assessed by the question whether in the last 3 months one had ‘considered oneself to be in need of medical care by a physician but decided not to seek’. Although this item investigates healthcare availability indirectly it does not provide any details about the person’s health status or healthcare utilization. When adjusting for self-rated health, differences in ORs of unmet healthcare needs are alleviated hinting at a connection between health status and unmet healthcare needs. Neither does it specify the objective need of the responder as the item ranges from minor symptoms that most likely would subside with time to acute and serious disorders or a known malignant condition with delayed follow up. Someone with poorer health is assumed to use healthcare more often, and higher healthcare utilization is more likely to generate unmet needs.
Specific questions about satisfaction with their current healthcare provider have not been assessed and may have shed a different light on the current PC organization. The time window of perceived need for healthcare is also small and perhaps a longer interval such as a year would have included more people with unmet needs. The time interval is shorter than most international measures of unmet healthcare needs, and therefore it is difficult to compare the data with other countries and regions. The same question was however included in the public health surveys carried out in Skåne in 2000, 2004, 2008 and 2012, which makes it a valid item to compare unmet healthcare needs in different population groups in Skåne and over time.
It should be taken into consideration that the questionnaire was carried out 3 years after the reform was implemented in Skåne, and differences between the two types of PC organizations may have developed later. A study comparing data on unmet healthcare needs/patient satisfaction among the Nordic countries has been considered, although comparable data of unmet healthcare needs have been difficult to retrieve.
Conclusions
This study shows non-significant differences in unmet healthcare needs when comparing private providers and public healthcare providers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Scientific Research Council (Vetenskapsrådet) Grant Dnr 521-2013-2674 (K2014-69X-22427-01-4) and the Swedish Avtal om utbildning av läkare och forskning (ALF) Government Grant Dnr M 2014/354.