
Abstract
Introduction
Campylobacteriosis is the most frequently reported food- and waterborne infection in the Nordic countries (Denmark, Finland, Iceland, Norway and Sweden) and indeed throughout Europe where incidences have remained at constant high levels for the past decade [1]. In the Nordic countries, notification rates of campylobacteriosis are comparatively high; incidences including travel-related cases reported to the European Centre for Disease Control and Prevention (ECDC) in 2017 ranged between 73.9 and 106.1 cases/100.000 population [1], the highest being in Finland and Sweden. Although the continued high levels of Campylobacter infection in the Nordic countries may be influenced by changes in health care–seeking behaviour and recent improvements in surveillance systems and/or diagnostics, they are, however, somewhat worrying, as they have occurred despite national control efforts, primarily to reduce incidences in poultry flocks.
Campylobacteriosis is a zoonotic disease, with reservoirs including poultry, wild birds, livestock and domesticated dogs and cats [2]. The disease occurs in all age groups, but incidence rates are notably higher in persons younger than 30 years of age and particularly among small children [3,4]. For Europeans, travelling abroad is one of the most important risk factors for infection. Domestic risk factors primarily include handling or consumption of undercooked chicken, contaminated drinking water and contact with animal and environmental infection reservoirs [5–7]. The role of the latter remains relatively poorly understood. However, sand, soil, mud and water are all potentially important [7–9]. Although mainly sporadic in nature, outbreaks of campylobacteriosis do occur [10,11] and are often linked to drinking water, raw milk or accidental ingestion of mud, for example during obstacle races [8,12–15]. Waterborne outbreaks in particular have frequently been reported following heavy rainfall [3,16–18], highlighting a potential link with extreme weather and a concern for the impact of climate change on Campylobacter.
Aims
This study aimed to describe the epidemiology of campylobacteriosis in four Nordic countries (Denmark, Finland, Norway and Sweden) from 2000 to 2015 in order to provide an informed basis for future infection prevention measures and disease management guidelines.
Methods
Human Campylobacter infection is notifiable in Denmark, Finland, Norway and Sweden where clinicians or laboratories are obliged to notify a Campylobacter case to the national public-health authorities: Statens Serum Institut in Denmark (through the national microbiology database, MiBa), the National Institute for Health and Welfare in Finland, The Norwegian Institute of Public Health (through the Norwegian Surveillance System for Communicable Diseases, MSIS) and the Public Health Agency of Sweden (via the national surveillance system SmiNet). The laboratory criteria for a Campylobacter diagnosis are quite similar across the countries: isolation of Campylobacter spp. by culture from faeces or blood. Since 2013, the Swedish criteria have also included samples positive for Campylobacter spp. using direct polymerase chain reaction (PCR) on stool samples. During the study period, this was not routinely established in the other countries, although some diagnostic laboratories in Denmark used the method occasionally.
For this study, we used all Campylobacter infections notified in Denmark, Finland and Sweden from 1 January 2000 until 31 December 2015 and in Norway from 1 January 2000 until 31 December 2014. Each case notification included the patient’s age (grouped in five-year intervals), sex, geographical location (at municipality level), presumed origin of infection (domestic, foreign and unknown) and date of sample taken (Norway, Finland) or date of sample received in the laboratory (Denmark, Sweden). Infections reported to be acquired abroad were excluded from the analysis, while infections reported to be of domestic or unknown origin were included.
For every municipality in each country, the population density (persons per km2) was calculated, and the geographical location (north, south, east or west) with reference to central latitude and longitude was defined. Further, a measure of waterline was calculated, given as a percentage of the total estimated municipality outline size covered by inland and/or coastal water. Due to the approximate nature of this method, the final values for waterline coverage were not used as absolute measures but were divided into four categories: 0%, <10%, 10–50% and >50%.
Accumulated and age-specific population sizes per year were obtained from Statistics Denmark (www.statistikbanken.dk), Statistics Finland (www.pxnet2.stat.fi), Statistics Norway (www.ssb.no) and Statistics Sweden (www.statistikdatabasen.scb.se).
We used descriptive statistics and two-tailed t-tests to analyse demographic factors, analysis of variance to compare incidences between municipalities and linear regression to examine the trends in incidences over time and for different population densities. The graphical presentation of the seasonality of campylobacteriosis was made using simple three-week moving averages in which the number of cases in a given week was calculated by the average number of cases over the previous three weeks. The moving average was used to emphasise the seasonal cycles of infections, and the interval of three weeks was chosen with consideration of the strong seasonal fluctuation of Campylobacter infections. All statistical analyses were undertaken using the Stata v11.0 (StataCorp, College Station, TX). Maps and GIS calculations for the municipality waterline were generated using QGIS v2.14.11 (QuantumGIS, Open Source Geospatial Federation Project, www.qgis.org).
Results
Incidence and demography
During 2000–2015, a total of 164,001 Campylobacter cases, excluding known foreign travel-related cases, were notified in the four countries, ranging from 20,338 to 52,912 cases per country and 1356 to 3307 cases per year (Table I). For 84,372 (51%) of these cases, the country of infection was reported as not known, while the rest were specifically reported as domestic in origin. Finland and Denmark reported the highest proportion of cases with an unknown travel status (79% and 82%, respectively), while country of infection was known for most of the cases reported in Norway and Sweden (Table I).
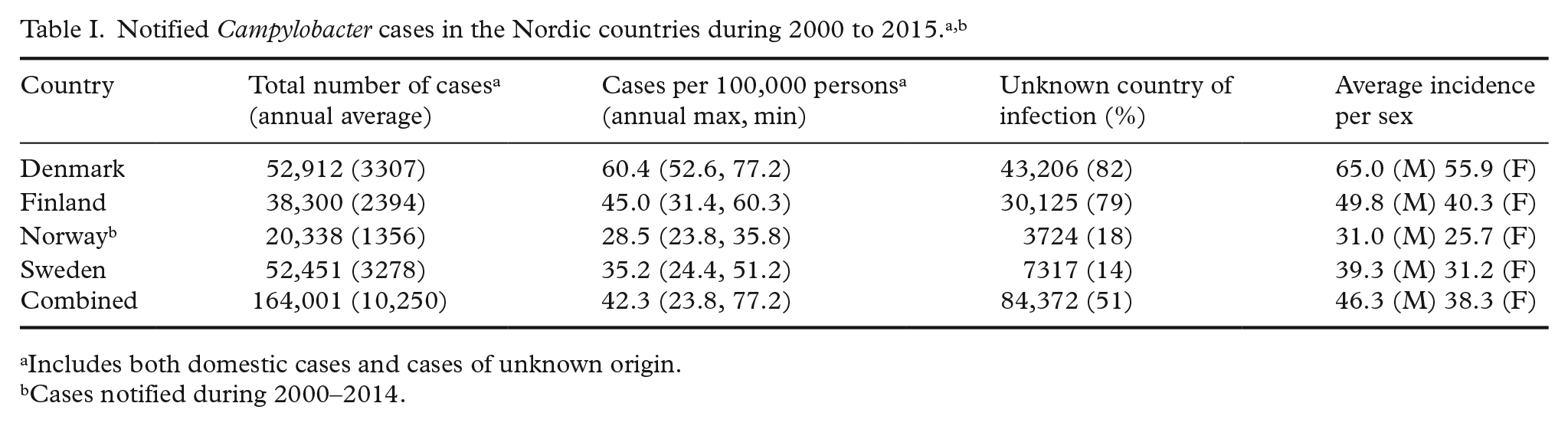
Includes both domestic cases and cases of unknown origin.
Cases notified during 2000–2014.
Overall, the average incidence of campylobacteriosis was 42.3 cases per 100,000 population, ranging from 28.5 in Norway to 60.4 in Denmark (Table I and Figure 1). Denmark reported a consistently higher incidence than the average, while in Norway the reported incidence remained low throughout the period (Figure 1). From 2004 onwards, the incidence of campylobacteriosis increased significantly in all countries (r2=0.31–0.54; p<0.05) apart from Denmark where an increase was only observed from 2014 to 2015 (Figure 1).
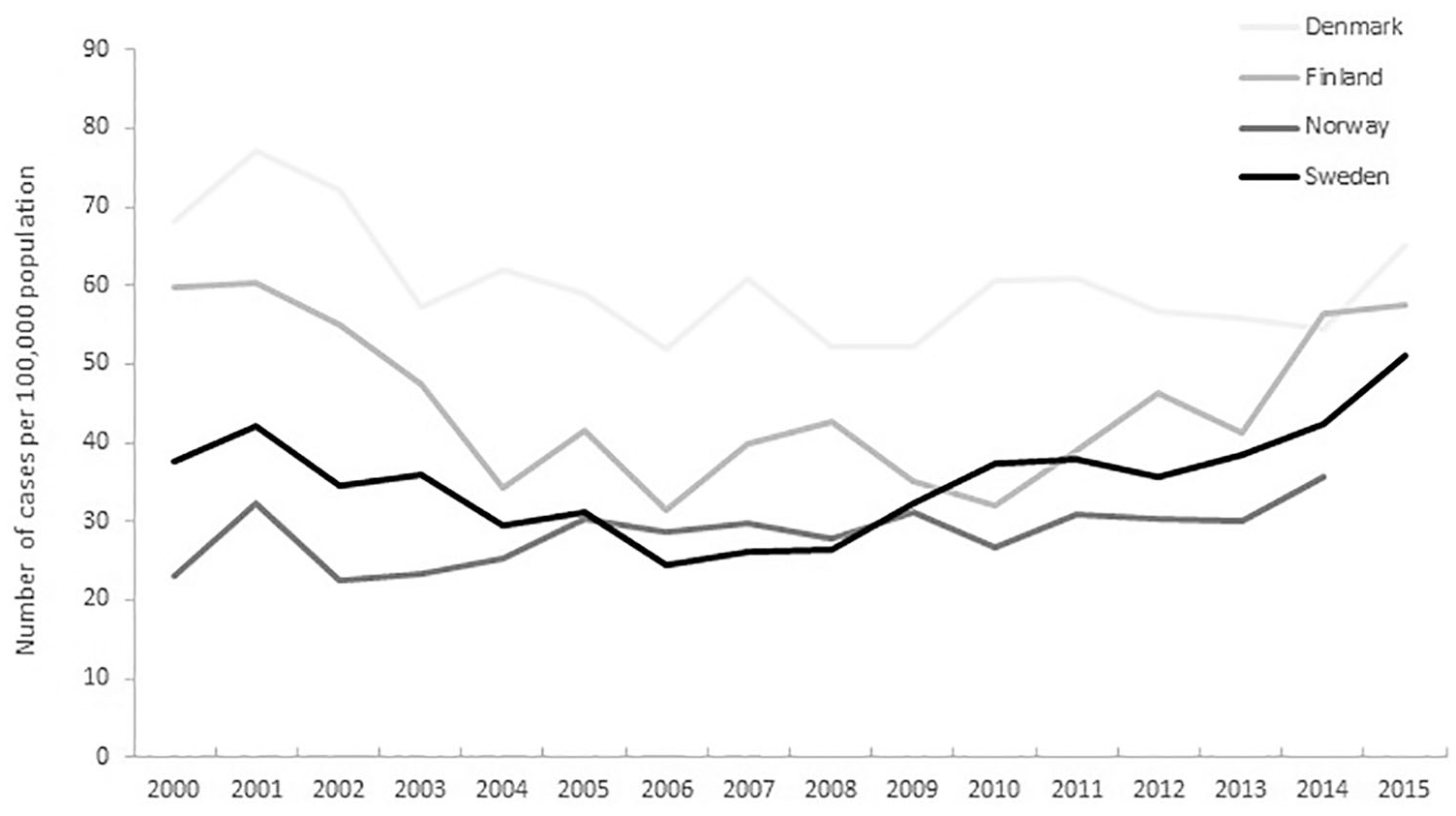
Incidence of non-travel acquired Campylobacter in the Nordic countries, 2000–2015.
In all four countries, males had higher infection rates than females (t=3.2–5.1; p<0.05; Table I). Age-specific incidences were similar in Denmark, Norway and Sweden, where small children (0–4 years) and young adults (20–29 years) had the highest incidences (t=4.8–5.8; p<0.001) of both domestic and unknown cases (Figure 2). In Finland, 20–29 year olds (t=3.4; p<0.01) also had high incidences, but no peak of infections in small children was observed (Figure 2).
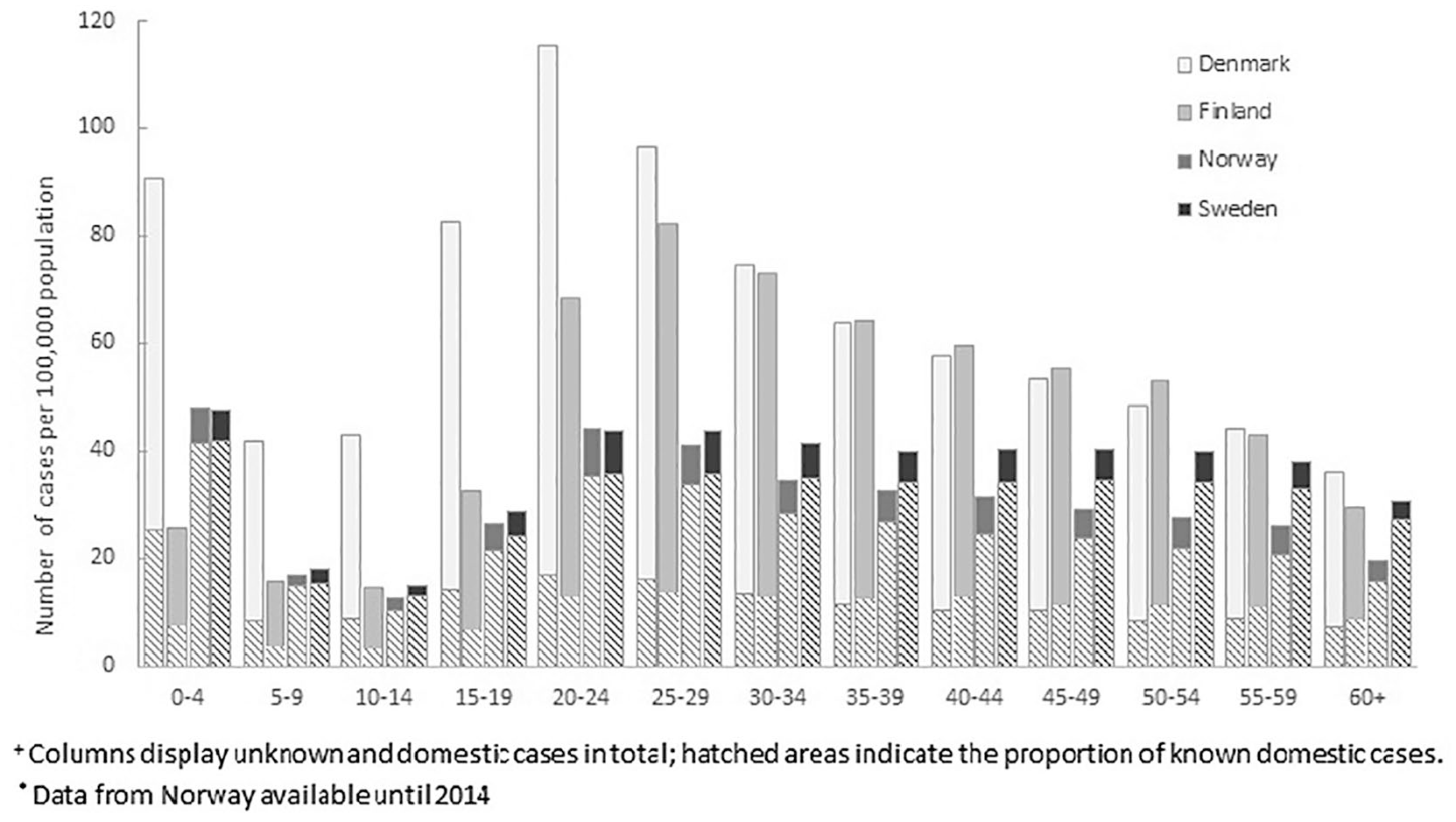
Age-specific incidence of Campylobacter in the Nordic countries, 2000–2015.+,*
Seasonality
Campylobacteriosis exhibited a distinct seasonal pattern in the four countries, with an increase in incidence from the middle of May (week 19), peaking in mid-July to the beginning of August (weeks 29–32; Figure 3). The timing of the increase in onset was similar for all countries, but peaks occurred at slightly different times, the earliest in Finland (July) and the latest in Denmark (early August). The seasonality of disease was independent of year of notification (Figure 3).
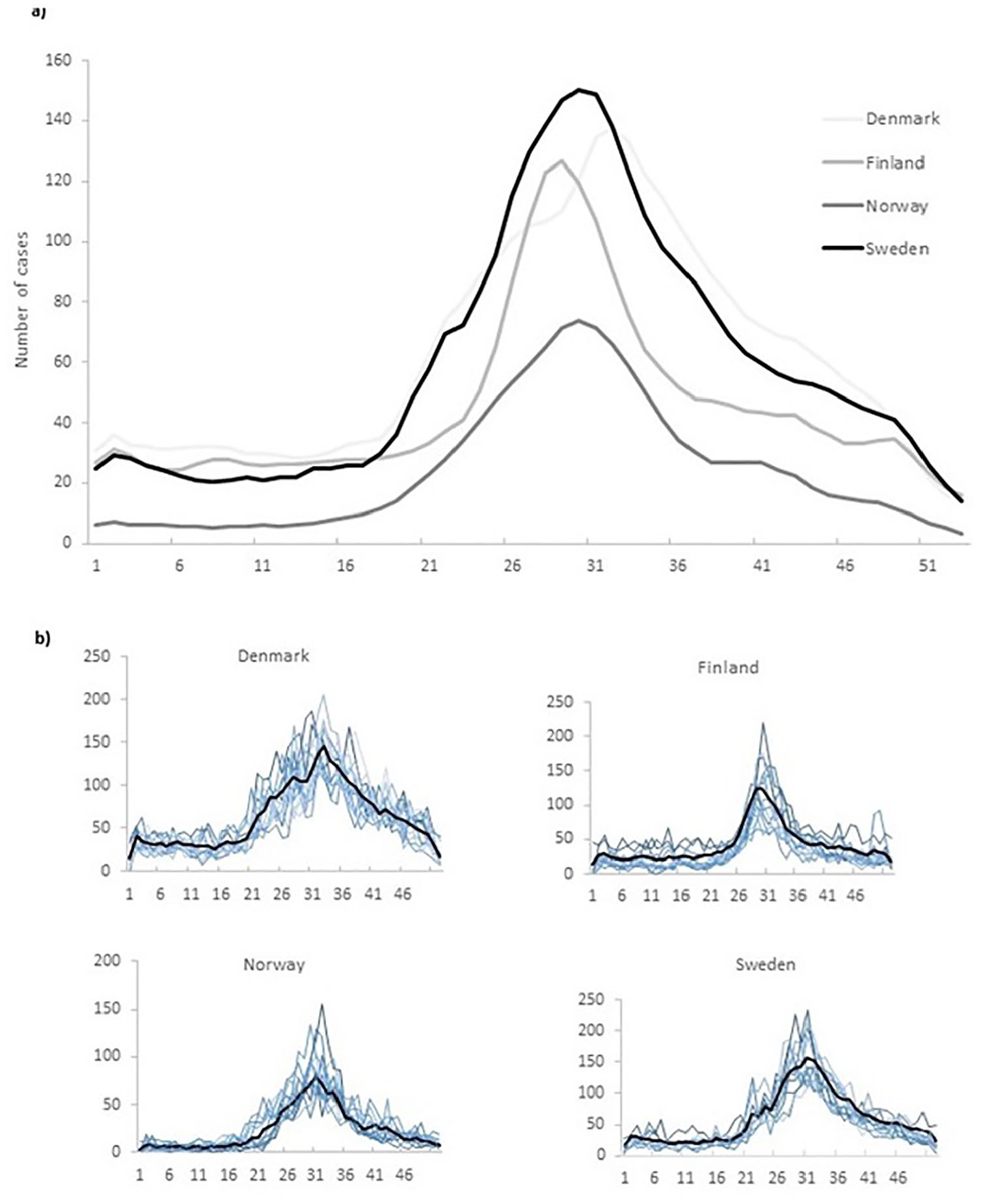
(a) Weekly average number of Campylobacter cases in the Nordic countries (three-week moving averages), 2000–2015.+,* (b) Weekly number of Campylobacter cases per year in Denmark, Finland, Norway and Sweden, 2000–2015+,* (average over the study period shown in black).
Geography
In all four countries, Campylobacter incidences at municipality level increased with increasing population density (r2=0.7–0.8; p<0.001). However, the incidence in children younger than 10 years of age was significantly higher (r2=0.6–0.7; p<0.01) in less densely populated municipalities in Denmark, Norway and Sweden. In Norway and Sweden, a north–south divide was observed, with higher incidences in southernmost municipalities and lower incidences in the northern municipalities, after adjusting for population density and municipality-specific age structure (Figure 4; F=4.9–6.2; p<0.001). Further, incidences of campylobacteriosis were significantly higher in Norwegian and Swedish municipalities, with more than a 50% ‘water perimeter’ (Figure 4).

Average incidence of Campylobacter (number of cases per 100,000 population) at geographical level in (a) Denmark, (b) Finland, (c) Norway and (d) Sweden, 2000–2015.+
Discussion
This paper analyses campylobacteriosis data from four Nordic countries over a 16-year period. Our results indicate three important findings related to seasonality, infection in different age groups and geographical patterns of infection.
First, we demonstrate that the seasonality of Campylobacter infections has remained strikingly constant, peaking during the same period each year from 2000 to 2015. The seasonal peaks reflect changes in human behaviour during the warmer months, such as different eating habits and hygiene practices, as well as more frequent contact with environmental risk factors combined with seasonally fluctuating infection rates in broiler flocks [3,19]. Provided that these factors impact campylobacteriosis in Nordic countries, our results confirm that they have remained relatively constant during the study period. The peak of infection varied slightly between countries (earliest in Finland and latest in Denmark), potentially indicating different holiday patterns, behavioural risk factors (e.g. spending more time outdoors during the onset of the light nights) or as yet unexplained differences among poultry infection rates in the four countries. The early peak in Finland in particular may be explained by foreign travel, as the school holiday begins earlier than the other Nordic countries, and a high proportion of the data included from Finland have an unknown place of origin.
Second, we show that Campylobacter incidences were higher among children younger than 10 years of age living in rural areas, which supports the hypothesis that this population group is more frequently infected via exposure to environmental and animal factors such as contact with farm animals, unpasteurised milk, contaminated water and wildfowl [6,7,20]. A north–south divide of infection was demonstrated for Sweden and Norway, with higher Campylobacter incidences in southern municipalities. This may be an indirect effect of climate, as warmer weather facilitates exposure to outdoor risk factors such as barbecueing, outdoor bathing and animals. A non-climatic explanation for this may be differences in access to general practitioners, and even diagnostic laboratories, ultimately affecting health care–seeking behaviour and diagnostic patterns.
The third important observation was that rates of campylobacteriosis were significantly higher in Swedish and Norwegian municipalities with a high degree of water coverage (inland or coastline), suggesting that direct water contact or factors indirectly related to water (sand, mud, etc.) may increase the risk of infection. Given previous findings of Campylobacter in beach sands and bathing water [21,22] and indeed outbreaks of campylobacteriosis associated with outdoor sports such as swimming and bicycle races [8,9,15,23], it is likely that such exposures also lead to sporadic cases.
Our results from this study shed new light to the transmission patterns of Campylobacter in the Nordic countries. However, they need to be interpreted considering the limitations of the data used. The increase in campylobacteriosis over time in Finland, Norway and Sweden and suddenly from 2014 to 2015 in Denmark may reflect a combination of factors. In Denmark, a notification artefact may be at play influenced by the increased shift towards direct electronic notification together with the introduction of direct PCR diagnosis on faecal matter towards the end of the study period [3]. Differences in surveillance and diagnostic methods may also explain the variation in notification rates between the countries. At the same time, awareness of new control strategies for zoonotic diseases is another key point. For instance, the 2003 Danish strategy to control Campylobacter in broilers and retail food resulted in a 16% reduction of positive broiler flocks [24], likely contributing to the decrease in human campylobacteriosis from 2004 onwards. In Sweden, control campaigns were initiated in the 1990s, decreasing the incidence in broiler flocks but not in humans [25]. From 2013 onwards, the incidence of Campylobacter in Swedish domestic broiler flocks and humans increased notably, prompting more intense control measures at the farm and slaughterhouse level. In Finland, the regulation of Campylobacter in poultry started in 2004, requiring mandatory self-checking at the slaughterhouse level. During 2004–2012, potentially as a result of the regulation, the prevalence of Campylobacter-positive slaughter batches in Finland remained relatively low at 2.1–7.0% [26]. Lastly, the Norwegian national action plan on Campylobacter in broilers has been running since 2001, and while the proportion of positive flocks has varied substantially since the launch of the action plan, the overall prevalence in broilers remains low compared to other European countries [27].
Another important limitation of the data presented is the impact of international travel. The Campylobacter infection rates reported in this study are lower than described in European annual reports [1], as we excluded travel-related cases. Instead, we chose to include both confirmed domestic cases and cases of unknown origin. The true origin of domestic-labelled cases is likely domestic [28]. However, the unknown cases are a source of error, as a proportion of these are likely to be travel associated, particularly in Denmark and Finland where around 80% of cases were of unknown origin. Generally, 30–60% of all Campylobacter cases notified in the Nordic countries are estimated to be acquired domestically [1,3,29]. We encourage a more thorough collection of the variable ‘place of infection’ (domestic/abroad) by reporting clinicians, which ultimately will facilitate better analysis of this issue in future research. Unintentionally including travel-related cases in our analysis could have caused bias with respect to the age-specific, geographical and seasonal distribution of disease. The Finnish data showed a deviation from the observed ‘norm’ of high infection rates in children younger than five years of age. Children in particular may be more susceptible to developing symptomatic infection due to a combination of immunological factors and increased exposure to environmental reservoirs. The absence of high infection rates among this age group in Finland could be due to the high proportion of infections with unknown country of infection (see below). If many of the infections of unknown origin were in fact acquired abroad (which is likely), this may have clouded the age distributions. Lastly, children in Finland may also be exposed differently (e.g. more likely to live in urban areas or have less contact with animals), be better trained in hygiene or exhibit different health care–seeking behaviour than in other Nordic countries.
Finally, considering the geographical variation of campylobacteriosis within countries, differences in health care–seeking behaviour and deviations in diagnostic laboratory activity levels (i.e. disproportion between the number of samples analysed and the population served) represented potential sources of error. However, considering that an rural–urban divide among adults and children has previously been demonstrated [3,20], these activity levels do not appear to have impacted on the results presented.
Conclusions
For more than a decade, campylobacteriosis has been the most prevalent bacterial gastrointestinal illness in the Nordic countries. The results from this study demonstrate that the disease in Denmark, Finland, Norway and Sweden over 16 years mostly followed known patterns with respect to demography, seasonality and geography. It confirms that males, young adults and children living in rural areas are at significantly higher risk of infection, highlighting these population groups as suitable targets for future information campaigns. A noteworthy finding is the increased Campylobacter rates in municipalities with a high degree of coastline or inland water, suggesting higher risks for populations with frequent contact with natural water sources possibly via environmental transmission. In this respect, new tools such as next-generation sequencing for determining clonal variation and clustering [30] in combination with electronic data storage and transfer can ultimately shed better light on the poorly understood aspects of Campylobacter epidemiology with respect to temporal and geographical shifts, sources of transmission and infection control.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: this work was part of KLIMAFORSK, a large-scale Nordic programme on climate research, supported by the Research Council of Norway.