
Abstract
Background: The aim of the study was to investigate changes in self-rated health (SRH) between different age groups and sexes over a 20-year period. Methods: Data were retrieved from the large longitudinal Health Survey of North Trøndelag, Norway, which includes data collected from more than 190,000 participants aged 20–70+ years between the years 1984 and 2008. Data were analysed using logistic regression and adjusted for sex. Results: From 1984 to 2008, the odds of scoring higher on SRH decreased by 46% in the youngest age group (20–29 years) and increased by approximately 35% in the middle-aged and older age groups (40–70+ years). When considering sex differences, women in most age groups scored lower than the men on their SRH.
Introduction
Health status has been found to be one of the most important factors in an individual’s endeavours to have a ‘good life’. Not only is good health an asset in itself but it also influences many factors in people’s lives, such as their well-being, life expectancy, life satisfaction, work, income and social relationships, amongst other things [1–4]. Moreover, there is a large body of evidence indicating that ill health is associated with reduced well-being [2,5]. Today, it is also well known that good health contributes heavily to general social and economic growth [1,6]. For a society, a population’s general health status is therefor of great importance with respect to economic outcomes in terms of productivity, labour supply, human capital and public spending. Interest in having as healthy and happy population as possible is therefore of crucial importance in reducing the social and health-care costs of societies in the future. New data indicate that the overall health situation in many countries, including Norway, may have improved over recent decades [1,7,8]. An interesting question is whether and how this improvement has affected the health situation for different age groups over a longer timeframe. Few studies have looked at self-rated health (SRH) for different age groups over a longer time period [9]. Thus, the aim of this study was to evaluate a possible increase in the SRH for different age groups in Norway over a 20-year period using one of the largest health surveys in the world, the Health Survey of North Trøndelag (HUNT).
A range of different indicators can be used to measure a population’s health. SRH has become extensively used as an outcome measure in population health surveillance and can help in guiding politicians and governments to create a healthier and more equal society [10]. The SRH questionnaire has shown to be a reliable measure of subjective health, institutionalisation, hospitalisation, morbidity and mortality [11–16]. An important factor when evaluating people’s health is age, and data indicate that the increase in health problems of older people is primarily the result of chronic diseases [2,3]. In general, as one grows older, more health problems arise. Nevertheless, many of these problems may be prevented or delayed by engaging in healthy behaviours [3]. Data indicate that different age groups rate SRH differently and that SRH declines with age [1]. However, some studies using SRH have reported only small changes between cohorts and even better SRH ratings amongst the oldest groups [17]. Therefore, it has been stated that the way SRH evolves in a population over a longer time period for different age groups can be both limited and inconclusive [14]. The aim of this paper is to fill a gap in the ongoing discussion about changes in health over time by exploring changes in the SRH of different age groups over a period of more than 20 years. More specifically, we hypothesise that the SRH of all age groups has improved compared to that of the same age groups 10 and 20 years prior to our study period. Moreover, the Eurostat 2017 report suggests that women tend to report more negatively on their health than men [18]. Similarly, in a study looking at sex and the validity of SRH, the authors found that SRH was associated with more physical health problems in the previous 12 months amongst females than amongst males [16]. To the best of our knowledge, few studies have investigated sex and age-group differences in SRH over a period of more than 20 years with a large number of participants. Based on previous findings, we hypothesise that women in all age groups will score lower than men on their SRH.
Methods
The study samples were obtained from the long-running HUNT study in Norway. For all HUNT waves, a prospective, longitudinal study design was used. All the samples are population based and unselected, and are considered to be representative for the general Norwegian population [19]. An invitation with the health questionnaire was sent by mail to all citizens in the county of Nord-Trøndelag who were aged ⩾20 years. Details concerning the questionnaires and examinations have been described elsewhere [20]. The HUNT data were collected in three waves – HUNT 1 in 1984–1986, HUNT 2 in 1995–1997 and HUNT 3 in 2006–2008 – and included more than 190,000 participants [19,20]. The Nord Trøndelag county population size remained relatively stable throughout the study period (125,835 in 1981 vs. 128,694 in 2006), and in- and out-migration was low [19]. This study includes participants from 20 to 70+ years of age. In all three surveys, the proportion of women participating was slightly higher than that of men, and the highest overall participation was amongst those in the middle-aged group (40–49 years). The proportion of respondents answering the SRH question in all three HUNT waves was 32.3%. Of the respondents who answered the SRH question, 53.2% participated in both HUNT 1 and HUNT 2, and 41.5% participated in both HUNT 2 and HUNT 3. Table I shows the number of participants from the three different study periods used in this study, stratified by age group and sex. The HUNT 3 wave was used as the reference group due to its most recent assessment.
Number of responders for SRH for different HUNT study samples.
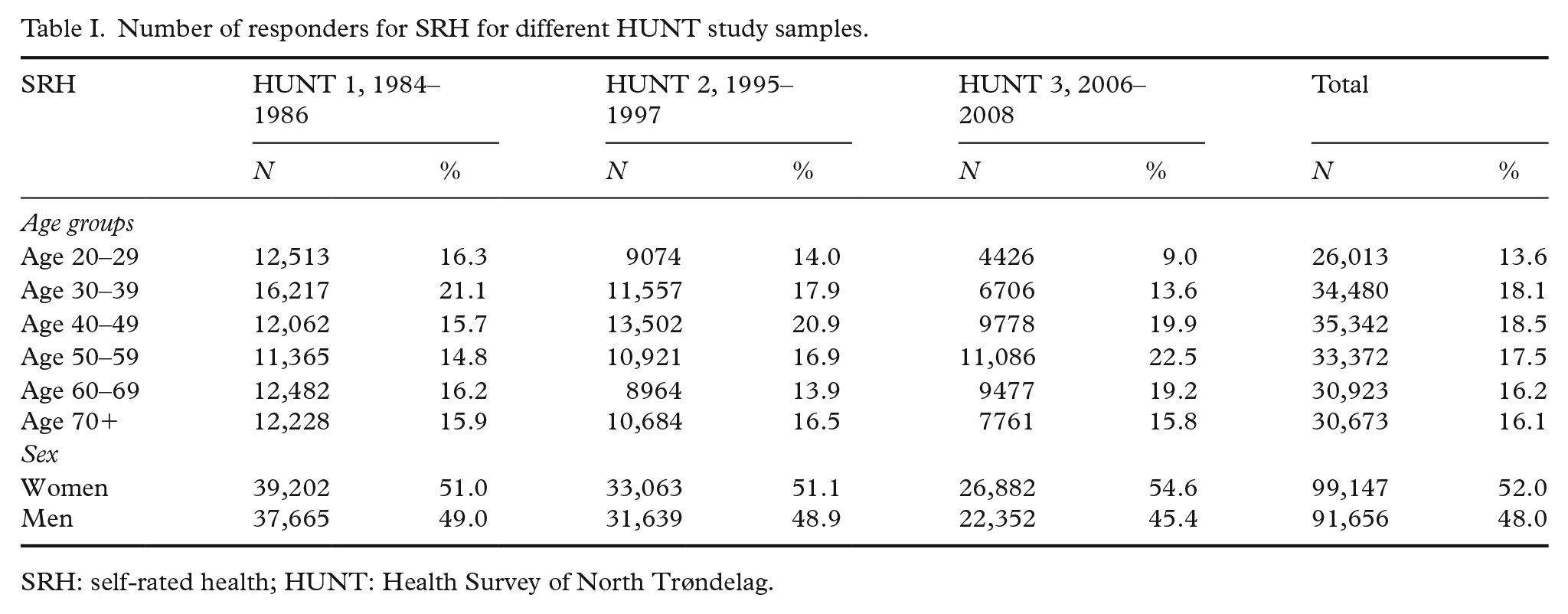
SRH: self-rated health; HUNT: Health Survey of North Trøndelag.
Measures
SRH was assessed by the single question ‘How is your health at the moment?’ in all waves, with a four-point rating scale ranging from 1=‘poor’ to 4=‘very good’. Table II show the number of responses given by all age groups for each level of SRH during the three HUNT waves. All responses were considered independent, regardless of whether the responder participated in one or more of the three HUNT waves.
OR of SRH across time and sex with 95% CI for different age groups.
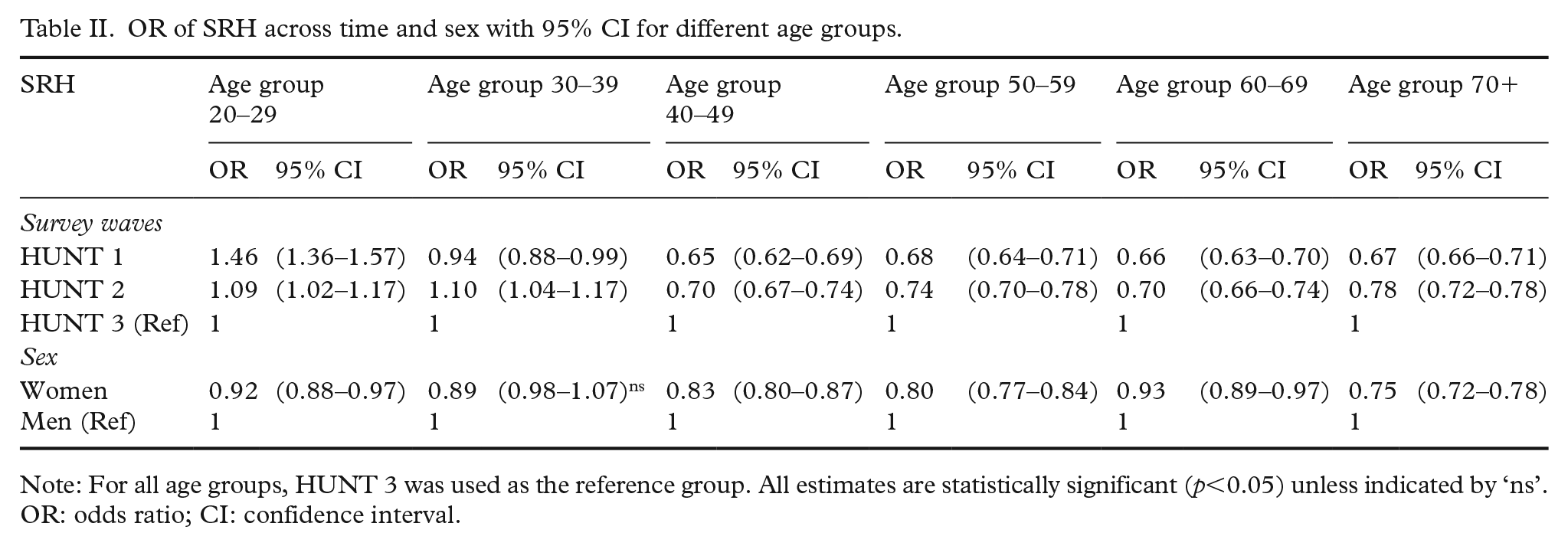
Note: For all age groups, HUNT 3 was used as the reference group. All estimates are statistically significant (p<0.05) unless indicated by ‘ns’.
OR: odds ratio; CI: confidence interval.
Statistical analyses
The associations between levels of SRH, age groups and time periods (the three HUNT waves) were modelled using ordinal logistic regression models, with SRH being the dependent variable. The level of SRH was reported as a categorical ordinal variable. The results are expressed as odds ratios with 95% confidence intervals. In the present model, we stratified by age groups and modelled the odds for achieving a higher level of SRH in HUNT 1 and HUNT 2, using HUNT 3 as a reference group. All analyses were adjusted for sex, and men were used as a reference group. The fit of ordinal regression models was tested with the test of parallel lines to verify that using ordinal models was the right approach, as opposed to using multinomial models. As the analyses are considered exploratory, no adjustments for multiple testing were performed. p-Values of <0.05 were considered statistically significant. All analyses were performed using IBM SPSS Statistics for Windows v22 (IBM Corp., Armonk, NY).
Ethics
The HUNT studies are approved by the Regional Committee for Medical and Health Research Ethics of Norway and the Norwegian Data Protection Authority.
Results
As can be seen in Table II and Figure 1, SRH decreased significantly (46%) from 1984 to 2008 in the youngest age group (20–29 years), indicating a shift towards lower levels of SRH in 2008 for this age group. In contrast, the proportion of middle-aged and older individuals (40–70+ years) reporting high levels of SRH increased significantly (~34%) from 1984 to 2008, indicating a shift towards higher levels of SRH. When stratified by age group, the largest shift in the odds of scoring higher on SRH was seen in the middle-aged and older age groups (40–70+ years).
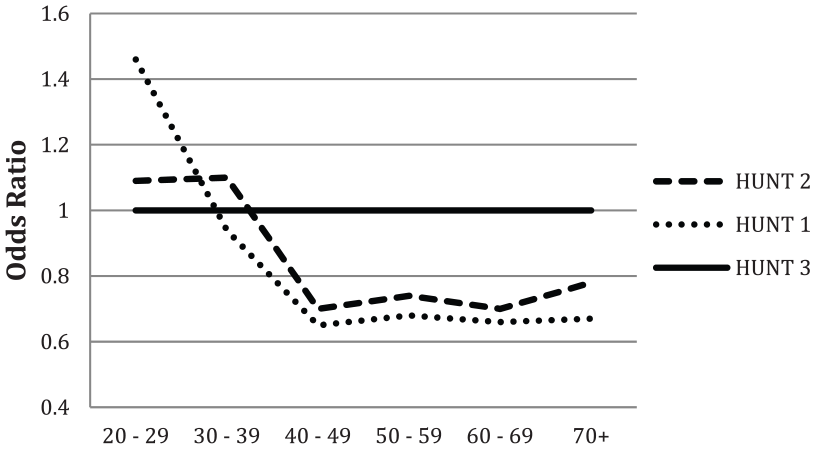
Point estimates of odds ratio for self-rated health (SRH) and age groups across time using the Health Survey of North Trøndelag wave 3 (HUNT 3) as the reference group. All estimates are statistically significant (p<0.05).
With regard to sex, women in all age groups were more likely to score lower than men on SRH, as can be seen in Table II and Figure 2. In general, the odds of reporting a higher score on SRH were about 15% higher for males compared to females for all age groups. However, the differences in odds between the sexes were relatively modest (Table II and Figure 2).
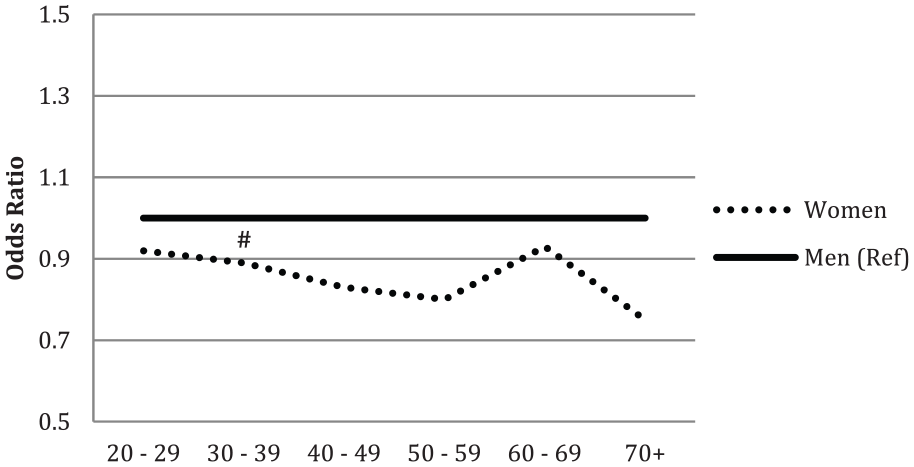
Point estimates of odds ratio for SRH and sex using men as the reference. If indicated with (#), the estimates are not statistically significant (p<0.05) and are marked as (#=ns).
Discussion
The main finding of this study was that SRH has increased for the 40–70+ year-old age groups and decreased for the 20–39 year-old age groups in the period from 1984 to 2008. These findings are in line with the findings of Johanessen et al. and the Eurostat data, indicating a decrease in SRH for younger age groups and an increase in SRH for middle-aged and older age groups [13,18]. Thus, our findings strengthen the assumption of a trend that middle-aged and older people have increased their SRH and that younger adults have had a negative trend for a period of more than 20 years. To see if this trend continues, this should be explored further with the new HUNT data set (HUNT 4) available in 2020. The middle-aged and older age groups in Norway have objectively seen nearly continuous improvement in different factors important for SRH and life satisfaction [7,21,22]. Many factors such as health care, nutrition, GDP, income, welfare, the labour market, education, social support and so on could be contributing to this change [1]. For instance, GDP increased continuously in Norway from 1984 to 2008, overall health status has improved over recent decades and life expectancy also increased during the HUNT investigation period [7,21,23]. Education affects SRH, both directly and indirectly [24]. In Norway, the population’s educational level has risen considerably in recent decades, with about 37.4% of women and 29.6% of men having higher educations as of 2017 [25]. Regarding the labour force, unemployment rates were generally low between the 1980s and 2010.
There is considerable concern about the behaviour of younger age groups today and the peer pressure they undergo to achieve a ‘successful life’ [26,27]. In a study looking at life satisfaction, the 20–29 year-old age group had a stable life satisfaction level for the time period 1984–2008, while the older age groups (40+ years) showed a significant increase [22]. In addition to increased competition to obtain a suitable education, high expectations to perform well in college and universities and a tougher labour market for young and poorly educated people, there is pressure to be included in the ‘right’ social groups, have a ‘perfect’ body and so forth [1,26,28,29]. These pressures have been shown to increase stress and depression – symptoms that have certainly increased in younger generations [26,28,29]. A report on living conditions in Norway states that young girls in particular report psychological problems [4]. The differences in overall SRH between the younger and middle-aged and older age groups might be further explained by variables other than age, and future studies should try to include other variables, as described previously in this paper.
As hypothesised, our study also suggests that there are sex differences in SRH that favour men. Women in the 40–59 and 70+ year-old age groups scored 20% lower on SRH in comparison to men, while women in the 60–69 year-old age group scored 7% lower. Nevertheless, the sex differences were relatively small. This is in line with previous findings, and in the Norwegian part of EU–SILC 2013, women scored higher (21%) on health problems than men (14%) [4]. Also the Eurostat Quality of Life report of 2015 indicates that in most age groups, women tended to report less positively than men on their health [1]. On average, 70.7% of men and 65% of women reported good or very good health, and 10.5% of women and 8.4% of men reported their health to be bad or very bad. Furthermore, in the study by Baćak and Olafsdottir [16] which looked at sex differences for SRH in 19 European countries, it was found that women reported significantly more physical health problems than males. The findings from the present study have implication for both practitioners and public-health politics. Given the decrease of 46% in SRH for the 20–29 year-old age group, practitioners should pay extra attention to their young patients’ assessment of decreased health. This is especially true for women, as the data from this paper indicate that females generally report lower SRH than males. The results presented in this paper should lead to more research to understand the mechanism behind this negative trend amongst the young and women in particular.
The strength of the present study is the longitudinal design, with data covering more than 20 years, the very large sample size with more than 190,000 participants and the use of the same methodology at each wave, ensuring good data quality in the presented results. Nevertheless, the findings presented in this paper need to be carefully interpreted, and some limitations must be kept in mind. First, the study is based on data from Norway, a country that ranks very high on most surveys of SRH, and this may preclude our findings from being generalised to other countries. However, the results presented in this study are in accordance with a large body of published data [1,11,13,14,27]. Second, a limited number of variables were included, and therefore the data cannot indicate the influence of different variables on the changes in SRH. A third limitation is that this study used a single variable for overall SRH. Although single-item variables on health have proven to be valid and reliable, future studies should strive for more objective health measures [10,14,30]. Fourth, the overall response rate was lower for the HUNT 3 wave than it was for the previous two HUNT waves, and this could have resulted in selection bias. Analyses of the HUNT waves have revealed a higher prevalence of cardiovascular disease, diabetes and mental distress amongst non-participants [20]. An underestimation of disorders due to the non-participation of individuals with such diagnoses could have led to bias. However, though studies thus far suggest there is no reason to be concerned about the introduction of bias, our results must be interpreted with caution [19,20].
Conclusions
This study describes a decrease of 46% in SRH for the 20–29 age group, a decrease of 10% for the 30–39 age group and an increase in SRH of 34% for the 40–70+ age groups in Norway from 1984–86 to 2006–8. This study also suggests sex differences in SRH for most age groups in favour of men. However, the sex differences were relatively modest.
Footnotes
Acknowledgements
The Nord-Trøndelag Health Study (The HUNT Study) is a collaboration between the HUNT Research Centre (Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology), Nord-Trøndelag County Council, Central Norway Regional Health Authority and the Norwegian Institute of Public Health.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.